
Do Alcohol Prevention Programs Influence Adolescents’ Drinking Behaviors? A Systematic Review and Meta-Analysis



Abstract
:1. Introduction
2. Methods
2.1. Research Design
2.2. Inclusion Criteria
2.3. Search Strategy
2.4. Quality Assessment
2.5. Data Collection
2.6. Data Analysis
3. Results
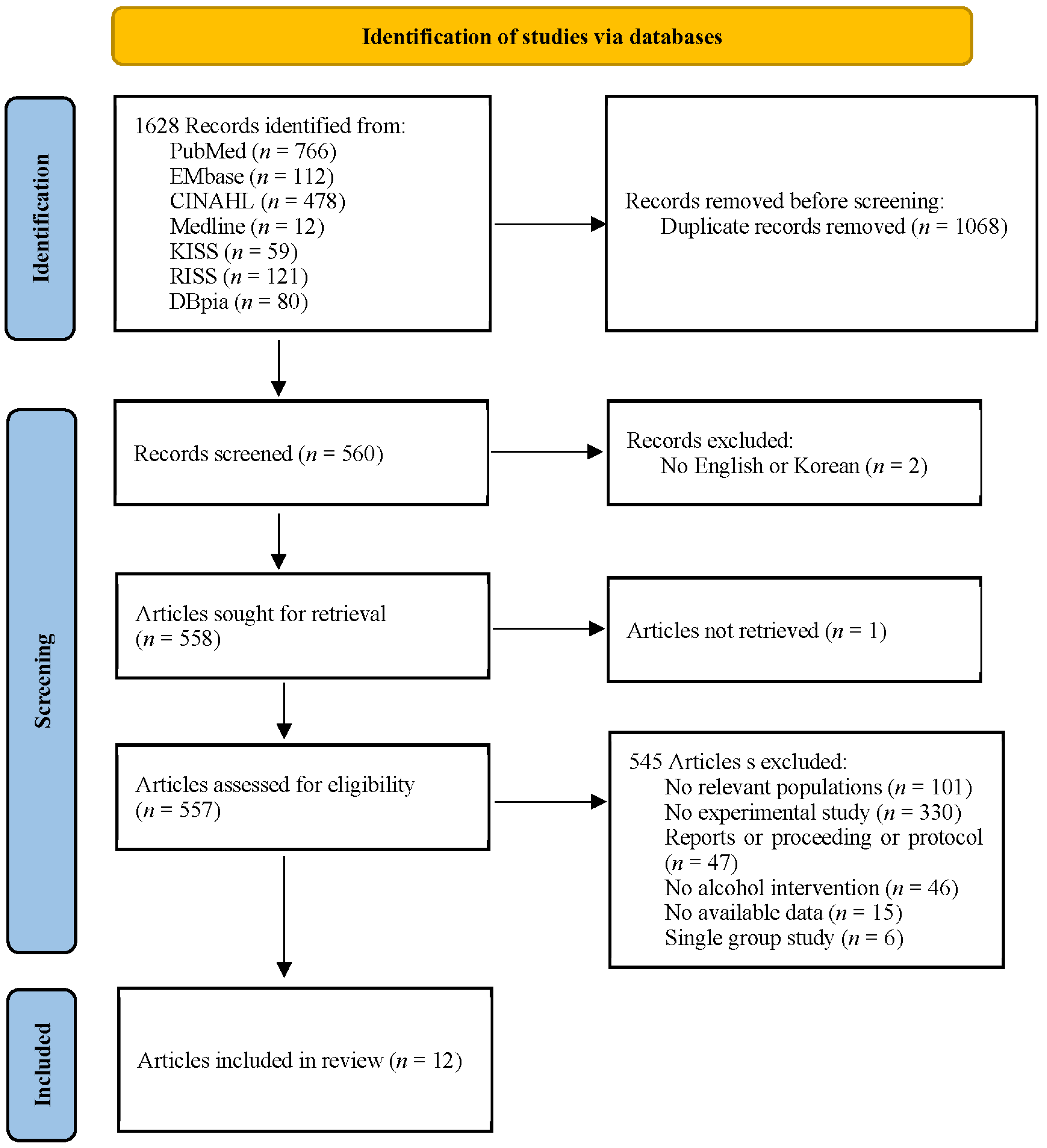
3.1. Data Extraction
3.2. Characteristics of the Study
3.3. Methodological Quality
3.4. Effects of Alcohol Prevention Intervention on Drinking Behaviors
3.5. Effects of Alcohol Prevention Intervention on Secondary Outcomes
3.6. Publication Bias Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Health Topics-Alcohol. 2020. Available online: https://www.who.int/health-topics/alcohol#tab=tab_1 (accessed on 2 March 2020).
- Griswold, M.G.; Fullman, N.; Hawley, C.; Arian, N.; Zimsen, S.R.M.; Tymeson, H.D.; Venkateswaran, V.; Tapp, A.D.; Forouzanfar, M.H.; Salama, J.S.; et al. Alcohol use and burden for 195 countries and territories, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2018, 392, 1015–1035. [Google Scholar] [CrossRef] [Green Version]
- Spear, L.P. Adolescent alcohol exposure: Are there separable vulnerable periods within adolescence? Physiol. Behav. 2015, 148, 122–130. [Google Scholar] [CrossRef] [Green Version]
- Korea Ministry of Education; Korea Ministry of Health and Welfare; Korea Disease Control and Prevention Agency. The Statistics Report of the Fifteenth Korea Youth Risk Behavior Web-Based Survey; KDCA: Cheongju, Korea, 2019.
- Korea Disease Control and Prevention Agency. Korea Health Statistics 2018: Korea National Health and Nutrition Examination Survey (KNHANES VII-3); KDCA: Cheongju, Korea, 2019.
- Gruber, E.; DiClemente, R.J.; Anderson, M.M.; Lodico, M. Early Drinking Onset and Its Association with Alcohol Use and Problem Behavior in Late Adolescence. Prev. Med. 1996, 25, 293–300. [Google Scholar] [CrossRef]
- Cho, H.C. A meta-analysis on the factors related to adolescents’ alcohol use: From 1990 to 2012. Korean J. Youth Stud. 2014, 21, 191–221. Available online: https://www.kci.go.kr/kciportal/ci/sereArticleSearch/ciSereArtiView.kci?sereArticleSearchBean.artiId=ART001896130 (accessed on 9 August 2021).
- Dir, A.L.; Bell, R.L.; Adams, Z.W.; Hulvershorn, L.A. Gender Differences in Risk Factors for Adolescent Binge Drinking and Implications for Intervention and Prevention. Front. Psychiatry 2017, 8, 289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jackson, N.; Denny, S.; Ameratunga, S. Social and socio-demographic neighborhood effects on adolescent alcohol use: A systematic review of multi-level studies. Soc. Sci. Med. 2014, 115, 10–20. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.K.; Kim, G.H. Factors Affecting Drinking and Drinking Frequency among Korean Youth. Korean J. Youth Stud. 2013, 20, 317–346. Available online: https://www.dbpia.co.kr/journal/articleDetail?nodeId=NODE06662030 (accessed on 9 August 2021).
- Champion, K.E.; Newton, N.; Barrett, E.; Teesson, M.R. A systematic review of school-based alcohol and other drug prevention programs facilitated by computers or the Internet. Drug Alcohol Rev. 2012, 32, 115–123. [Google Scholar] [CrossRef] [PubMed]
- Das, J.K.; Salam, R.A.; Arshad, A.; Finkelstein, Y.; Bhutta, Z.A. Interventions for Adolescent Substance Abuse: An Overview of Systematic Reviews. J. Adolesc. Health 2016, 59, S61–S75. [Google Scholar] [CrossRef] [Green Version]
- Newton, N.C.; Champion, K.E.; Slade, T.; Chapman, C.; Stapinski, L.; Koning, I.; Tonks, Z.; Teesson, M. A systematic review of combined student- and parent-based programs to prevent alcohol and other drug use among adolescents. Drug Alcohol Rev. 2017, 36, 337–351. [Google Scholar] [CrossRef]
- Hale, D.R.; Fitzgerald-Yau, N.; Viner, R.M. A Systematic Review of Effective Interventions for Reducing Multiple Health Risk Behaviors in Adolescence. Am. J. Public Health 2014, 104, e19–e41. [Google Scholar] [CrossRef]
- Bo, A.; Hai, A.H.; Jaccard, J. Parent-based interventions on adolescent alcohol use outcomes: A systematic review and me-ta-analysis. Drug Alcohol Depend. 2018, 171, 98–109. [Google Scholar] [CrossRef] [PubMed]
- Hurley, E.; Dietrich, T.; Rundle-Thiele, S. A systematic review of parent based programs to prevent or reduce alcohol consumption in adolescents. BMC Public Health 2019, 19, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Ivaniushina, V.; Titkova, V.; Alexandrov, D. Peer influence in adolescent drinking behaviour: A protocol for systematic review and meta-analysis of stochastic actor-based modeling studies. BMJ Open 2019, 9, e028709. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanner-Smith, E.E.; Lipsey, M.W. Brief Alcohol Interventions for Adolescents and Young Adults: A Systematic Review and Meta-Analysis. J. Subst. Abus. Treat. 2015, 51, 1–18. [Google Scholar] [CrossRef] [Green Version]
- Cochrane Handbook of Systematic Reviews of Interventions. Version 5.1.0 [updated March 2011]. Available online: http://handbook.cochrane.org/ (accessed on 11 November 2012).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, 332–336. [Google Scholar] [CrossRef] [Green Version]
- JBI. Checklist for Case Control Studies. Available online: https://jbi.global/critical-appraisal-tools (accessed on 1 May 2021).
- Bax, L. MIX 2.0. Professional Software for Meta-Analysis in Excel. Version 2.0.1.6. BiostatXL. Available online: https://www.meta-analysis-made-easy.com (accessed on 18 November 2018).
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.T.; Rothstein, H.R. Introduction to Meta-Analysis; John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 2009; p. 452. [Google Scholar]
- Mavridis, D.; Salanti, G. How to assess publication bias: Funnel plot, trim-and-fill method and selection models. Evid. Based Ment. Health 2014, 17, 30. [Google Scholar] [CrossRef]
- Koning, I.M.; Lugtig, P.; Vollebergh, W.A. Differential effects of baseline drinking status: Effects of an alcohol prevention program targeting students and/or parents (PAS) among weekly drinking students. J. Subst. Abus. Treat. 2014, 46, 522–527. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Komro, K.A.; Livingston, M.D.; Wagenaar, A.C.; Kominsky, T.K.; Pettigrew, D.W.; Garrett, B.A.; Cherokee Nation Prevention Trial Team. Multilevel Prevention Trial of Alcohol Use among American Indian and White High School Students in the Cherokee Nation. Am. J. Public Health 2017, 107, 453–459. [Google Scholar] [CrossRef]
- McKay, M.T.; McBride, N.T.; Sumnall, H.R.; Cole, J.C. Reducing the harm from adolescent alcohol consumption: Results from an adapted version of SHAHRP in Northern Ireland. J. Subst. Use 2012, 17, 98–121. [Google Scholar] [CrossRef] [Green Version]
- Zebregs, S.; Putte, B.V.D.; De Graaf, A.; Lammers, J.; Neijens, P. The effects of narrative versus non-narrative information in school health education about alcohol drinking for low educated adolescents. BMC Public Health 2015, 15, 1085. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Armitage, C.J.; Rowe, R.; Arden, M.A.; Harris, P.R. A brief psychological intervention that reduces adolescent alcohol consumption. J. Consult. Clin. Psychol. 2014, 82, 546–550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doumas, D.M.; Esp, S.; Flay, B.; Bond, L. A Randomized Controlled Trial Testing the Efficacy of a Brief Online Alcohol Intervention for High School Seniors. J. Stud. Alcohol Drugs 2017, 78, 706–715. [Google Scholar] [CrossRef] [PubMed]
- D’Amico, E.J.; Tucker, J.S.; Miles, J.N.V.; Zhou, A.J.; Shih, R.A.; Green, H.D. Preventing Alcohol Use with a Voluntary After-School Program for Middle School Students: Results from a Cluster Randomized Controlled Trial of CHOICE. Prev. Sci. 2012, 13, 415–425. [Google Scholar] [CrossRef] [PubMed]
- Spirito, A.; Sindelar-Manning, H.; Colby, S.M.; Barnett, N.P.; Lewander, W.; Rohsenow, D.J.; Monti, P.M. Individual and Family Motivational Interventions for Alcohol-Positive Adolescents Treated in an Emergency Department. Arch. Pediatr. Adolesc. Med. 2011, 165, 269–274. [Google Scholar] [CrossRef] [Green Version]
- Werch, C.E.; Bian, H.; Carlson, J.M.; Moore, M.J.; DiClemente, C.C.; Huang, I.-C.; Ames, S.C.; Thombs, D.; Weiler, R.M.; Pokorny, S.B. Brief integrative multiple behavior intervention effects and mediators for adolescents. J. Behav. Med. 2010, 34, 3–12. [Google Scholar] [CrossRef] [Green Version]
- Gmel, G.; Venzin, V.; Marmet, K.; Danko, G.; Labhart, F. A quasi-randomized group trial of a brief alcohol intervention on risky single occasion drinking among secondary school students. Int. J. Public Health 2012, 57, 935–944. [Google Scholar] [CrossRef] [PubMed]
- Haug, S.; Castro, R.P.; Kowatsch, T.; Filler, A.; Dey, M.; Schaub, M.P. Efficacy of a web- and text messaging-based intervention to reduce problem drinking in adolescents: Results of a cluster-randomized controlled trial. J. Consult. Clin. Psychol. 2017, 85, 147–159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doumas, D.M.; Esp, S.; Turrisi, R.; Bond, L.; Flay, B. Efficacy of the eCHECKUP TO GO for High School Seniors: Sex Differences in Risk Factors, Protective Behavioral Strategies, and Alcohol Use. J. Stud. Alcohol Drugs 2020, 81, 135–143. [Google Scholar] [CrossRef]
- Melsen, W.G.; Bootsma, M.C.J.; Rovers, M.M.; Bonten, M.J.M. The effects of clinical and statistical heterogeneity on the predictive values of results from meta-analyses. Clin. Microbiol. Infect. 2014, 20, 123–129. [Google Scholar] [CrossRef] [Green Version]
- Lin, L.; Chu, H.; Murad, M.H.; Hong, C.; Qu, Z.; Cole, S.R.; Chen, Y. Empirical Comparison of Publication Bias Tests in Meta-Analysis. J. Gen. Intern. Med. 2018, 33, 1260–1267. [Google Scholar] [CrossRef] [Green Version]
- Chung, T.; Creswell, K.G.; Bachrach, R.; Clark, D.B.; Martin, C.S. Adolescent Binge Drinking. Alcohol Res. Curr. Rev. 2018, 39, 5–15. [Google Scholar]
- Foxcroft, D.R.; Tsertsvadze, A. Universal alcohol misuse prevention programmes for children and adolescents: Cochrane systematic reviews. Perspect. Public Health 2012, 132, 128–134. [Google Scholar] [CrossRef]
- Foxcroft, D.R.; Ireland, D.; Lister-Sharp, D.J.; Lowe, G.; Breen, R. Longer-term primary prevention for alcohol misuse in young people: A systematic review. Addiction 2003, 98, 397–411. [Google Scholar] [CrossRef] [PubMed]
- Faggiano, F.; Vigna-Taglianti, F.; Versino, E.; Zambon, A.; Borraccino, A.; Lemma, P. School-based prevention for illicit drugs’ use. Cochrane Database Syst. Rev. 2005, CD003020. [Google Scholar] [CrossRef]
- Caria, M.P.; Faggiano, F.; Bellocco, R.; Galanti, M.R. Effects of a School-Based Prevention Program on European Adolescents’ Patterns of Alcohol Use. J. Adolesc. Health 2011, 48, 182–188. [Google Scholar] [CrossRef]
- Faggiano, F.; Galanti, M.R.; Bohrn, K.; Burkhart, G.; Vigna-Taglianti, F.; Cuomo, L.; Fabiani, L.; Panella, M.; Perez, T.; Siliquini, R.; et al. The effectiveness of a school-based substance abuse prevention program: EU-Dap cluster randomised controlled trial. Prev. Med. 2008, 47, 537–543. [Google Scholar] [CrossRef] [PubMed]
- Cuijpers, P.; Jonkers, R.; De Weerdt, I.; De Jong, A. The effects of drug abuse prevention at school: The ‘Healthy School and Drugs’ project. Addiction 2002, 97, 67–73. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.; Bang, S.A.; Seo, E. A Study on Factors Influencing Youth Drinking Using Binomial Logistic Regression. J. Korean Soc. Comput. Info. 2019, 24, 167–174. [Google Scholar] [CrossRef]
- Holmila, M.; Karlsson, T.; Warpenius, K. Controlling teenagers’ drinking: Effects of a community-based prevention project. J. Subst. Use 2010, 15, 201–214. [Google Scholar] [CrossRef]
- Rodgers, M.A.; Pustejovsky, J.E. Evaluating meta-analytic methods to detect selective reporting in the presence of dependent effect sizes. Psychol. Methods 2021, 26, 141–160. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Inclusion | Exclusion | |
|---|---|---|
| Participants | Adolescents (13~18 years) | Studies of subjects participate in other studies that simultaneously affect drinking behavior Those who are diagnosed with alcoholism and are being treated |
| Interventions | Studies published from 1 January 2010 to 30 April 2021 Studies published in English or Korean Studies with mean, standard deviation, concrete sample size | Studies of subject is unable to voluntarily answer the questionnaire Studies in which the main effect of intervention is drug therapy Studies in which mean, standard deviation, and sample size of each group not accurately presented |
| Control | Usual care, comparative experiment | Participating in other interventions |
| Outcomes | Primary outcome is drinking behaviors (frequency of alcohol drinking, amount of alcohol drinking, frequency of binge drinking) Secondary outcomes are knowledge, attitudes, alcohol harm, intention to drinking, self-efficacy When serial interventions were performed, only the effect of the first intervention was coded for analysis | Studies that did not measure primary or secondary outcomes as an outcome variable |
| Study design | Quasi-experimental studies or RCT | Not quasi-experimental studies or RCT In the quasi-experimental study, a single group comparative study |
| No. | Author (Year) | Country | Research Design | Target | Participants | Program | Duration | Outcome Variables | Quality Scores |
|---|---|---|---|---|---|---|---|---|---|
| 1 | Koning et al., (2014) [25] | Netherlands | cluster RCT | 19 schools, individual or/and family | 795 weekly drinking students (mean age: 12.66, SD = 0.49), E a: 158, E b: 251, E c: 151, C: 235 | PAS E a: parent intervention, E b: student intervention, E c: combined intervention | ≥6 month | drinking behavior (amount, frequency) | 8 |
| 2 | Mckay et al., (2012) [27] | Northern Ireland | non-randomized control longitudinal design | 29 schools, individual | 2187 (mean age: 13.84), E a: 847, E b: 574, C: 766 | revised SHAHRP E a: from teachers, E b: from external facilitators (local drug and alcohol educators) | ≥6 month | knowledge, attitudes, alcohol consumption, context of use, harm associated with own alcohol use and the alcohol use of other people | 8 |
| 3 | Zebregs et al., (2015) [28] | Netherlands | cluster RCT | 12 school, individual | 296 low educated adolescents 187 (age: 11–14), E: 161, C: 135 | information about alcohol of narrative versus non-narrative form E: narrative information, C: non-narrative information | <6 month | knowledge, attitude towards alcohol, and intention to drink alcohol | 10 |
| 4 | Komro et al., (2017) [26] | Cherokee Nation | cluster RCT | 6 communities (each with 1 high school), community/individual | 1623 high school students (mean age: 14.9–15.2), E a: 208, E b: 224, E3: 603, C: 588 | CMCA (community-organizing intervention targeting alcohol access), CONNECT (school-based universal screening and brief intervention) E a: CMCA, E b: CONNECT, E c: combined intervention | ≥6 month | current alcohol use, heavy episodic drinking | 9 |
| 5 | Armitage et al., (2014) [29] | North of England | RCT | 1 school, individual | 67 adolescents (mean age: 17.09, SD = 0.38), E: 32, C: 35 | Brief Psychological Intervention (self-affirming implementation intention) | <6 month | alcohol intake, behavioral intention, self-efficacy | 10 |
| 6 | Doumas et al., (2017) [30] | USA | RCT | 1 school, individual | 221 high school seniors (mean age: 17.16, SD = 0.45), E: 116, C: 105 | the eCHECKUP TO GO (brief, web-based personalized feedback intervention) | <6 month | drinking quantity, peak drinking quantity, frequency of drinking, problem drinking | 11 |
| 7 | D’Amico et al., (2012) [31] | USA | cluster RCT | 16 middle schools, individual | 8932 middle school students (mean age: 12.6), E: 4243, C: 4689 | CHOICE (a voluntary after school program for younger adolescents) | <6 month | alcohol use, heavy drinking, perceived alcohol use, alcohol intentions, self-efficacy | 10 |
| 8 | Spirito et al., (2011) [32] | USA | RCT | PED, individual and family | 97 students (mean age: 15.42–15.48), E: 41, C: 56 | IMI + FCU E: IMI + FCU, C: IMI | ≥6 month | drinking frequency, drinking quantity, frequency of high-volume drinking | 9 |
| 9 | Werch et al., (2011) [33] | USA | RCT | 2 high schools, individual | 451 public high school students (mean age: 17.08, SD = 0.82), E: 227, C: 224 | brief integrative multiple behavior intervention | ≥6 month | quantity x frequency of alcohol use | 9 |
| 10 | Gmel et al., (2012) [34] | Swiss | cluster quasi-randomized control trial | 9 school, individual | 668 secondary school students (age: 16–18), E: 338, C: 330) | brief group alcohol motivational intervention | <6 month | individual’s RSOD frequency, maximum number of drinks on a single occasion, and overall weekly consumption | 10 |
| 11 | Haug et al., (2017) [35] | Swiss | cluster RCT | 11 schools, individual | 1041 students (mean age: 16.8, SD = 1.6), E: 547, C: 494) | Mobile Coach Alcohol program | <6 month | frequency of RSOD, peak blood alcohol concentration, Overestimation of peer group drinking norms | 11 |
| 12 | Doumas et al., (2020) [36] | USA | RCT | 2 schools, individual | 283 students (mean age: 17.15, SD = 0.47), E: 159, C: 124 | eCHECKUP TO GO | <6 month | frequency of alcohol use, peak drinking quantity, Normative beliefs about peer alcohol use, positive alcohol expectancies, Protective behavioral strategies | 11 |
| Frequency of Drinking | Simple Forest Plot (Random Effect Model) | ||||||||
| Study ID | Author (Year) | N | Hg | CI− | CI+ | Z | p | w |  |
| 4a | Komro et al., (2017) | 796 | 0.53 | 0.37 | 0.69 | 6.48 | <0.001 | 14.4% | |
| 4b | Komro et al., (2017) | 812 | 1.05 | 0.89 | 1.21 | 12.68 | <0.001 | 14.4% | |
| 4c | Komro et al., (2017) | 1191 | −1.29 | −1.41 | −1.16 | −20.24 | <0.001 | 14.4% | |
| 8 | Spirito et al., (2011) | 97 | −0.25 | −0.65 | 0.16 | −1.20 | 0.231 | 13.7% | |
| 10 | Gmel et al., (2012) | 668 | −0.01 | −0.16 | 0.15 | −0.07 | 0.945 | 14.4% | |
| 11 | Haug et al., (2017) | 1041 | 0.02 | −0.10 | 0.14 | 0.32 | 0.749 | 14.4% | |
| 12 | Doumas et al., (2020) | 283 | 0.35 | 0.12 | 0.59 | 2.92 | 0.003 | 14.2% | |
| Overall | 3712 | 0.06 | −0.57 | 0.69 | 0.19 | 0.853 | 100.0% | ||
| Amount of Drinking | Simple Forest Plot (Random Effect Model) | ||||||||
| Study ID | Author (Year) | N | Hg | CI− | CI+ | Z | p | w |  |
| 1 a | Koning et al., (2014) | 393 | −0.35 | −0.56 | −0.15 | −3.41 | 0.001 | 9.3% | |
| 1 b | Koning et al., (2014) | 486 | −0.19 | −0.37 | −0.02 | −2.13 | 0.033 | 9.3% | |
| 1 c | Koning et al., (2014) | 386 | −0.34 | −0.55 | −0.14 | −3.27 | 0.001 | 9.2% | |
| 5 | Armitage et al., (2014) | 67 | −0.19 | −0.67 | 0.29 | −0.78 | 0.437 | 8.2% | |
| 6 | Doumas et al., (2017) | 221 | −0.29 | −0.55 | −0.02 | −2.12 | 0.034 | 9.1% | |
| 7 | D’Amico et al., (2012) | 567 | 0.11 | −0.05 | 0.28 | 1.32 | 0.186 | 9.3% | |
| 8 | Spirito et al., (2011) | 8932 | −0.06 | −0.10 | −0.02 | −2.77 | 0.006 | 9.5% | |
| 9 | Werch et al., (2011) | 97 | −0.28 | −0.69 | 0.12 | −1.36 | 0.175 | 8.5% | |
| 10 | Gmel et al., (2012) | 451 | −3.24 | −3.52 | −2.96 | −22.59 | <0.001 | 9.0% | |
| 12 | Doumas et al., (2020) | 668 | 0.03 | −0.12 | 0.18 | 0.36 | 0.720 | 9.4% | |
| Overall | 11,514 | −0.46 | −0.87 | −0.05 | −2.20 | 0.028 | 100.0% | ||
| Frequency of Binge Drinking | Simple Forest Plot (Random Effect Model) | ||||||||
| Study ID | Author (year) | N | Hg | CI− | CI+ | Z | p | w |  |
| 4 a | Komro et al., (2017) | 796 | 1.92 | 1.73 | 2.10 | 20.43 | <0.001 | 12.6% | |
| 4 b | Komro et al., (2017) | 812 | 1.90 | 1.72 | 2.08 | 20.72 | <0.001 | 12.6% | |
| 4 c | Komro et al., (2017) | 221 | −0.11 | −0.38 | 0.15 | −0.82 | 0.410 | 12.4% | |
| 6 | Doumas et al., (2017) | 567 | 0.05 | −0.12 | 0.21 | 0.54 | 0.588 | 12.6% | |
| 8 | Spirito et al., (2011) | 97 | −0.19 | −0.59 | 0.22 | −0.91 | 0.363 | 12.1% | |
| 10 | Gmel et al., (2012) | 668 | −0.06 | −0.21 | 0.09 | −0.75 | 0.454 | 12.6% | |
| 11 | Haug et al., (2017) | 1041 | −0.04 | −0.16 | 0.08 | −0.63 | 0.527 | 12.6% | |
| 12 | Doumas et al., (2020) | 283 | −0.31 | −0.54 | −0.07 | −2.55 | 0.011 | 12.5% | |
| Overall | 3933 | 0.29 | −0.46 | 1.03 | 0.76 | 0.450 | 100.0% | ||
| Variables | Characteristics | Subgroup | K | Study ID | N | Hg | 95% CI | Z (p) | I2 (%) | |
|---|---|---|---|---|---|---|---|---|---|---|
| Lower Limit | Upper Limit | |||||||||
| Frequency of drinking | Age | <16 | 1 | 8 | 97 | −0.25 | −0.65 | 0.16 | 0.28 (0.231) | 0.0 |
| ≥16 | 4 | 4,10,11,12 | 3615 | 0.11 | −0.58 | 0.79 | 0.31 (0.758) | 99.2 | ||
| Number of participants | <500 | 2 | 8,12 | 380 | 0.08 | −0.51 | 0.66 | 0.25 (0.799) | 84.1 | |
| ≥500 | 3 | 4,10,11 | 3332 | 0.06 | −0.72 | 0.84 | 0.15 (0.881) | 99.4 | ||
| Number of schools | <10 | 4 | 4,8,10,12 | 2671 | 0.07 | −0.73 | 0.86 | 0.16 (0.871) | 99.2 | |
| ≥10 | 1 | 11 | 1041 | 0.02 | −0.10 | 0.14 | 0.32 (0.749) | 0.0 | ||
| Research design | RCT | 5 | 4,8,10,11,12 | 3712 | 0.06 | −0.57 | 0.69 | 0.19 (0.853) | 99.0 | |
| Type of program | Motivation | 5 | 4,8,10,11,12 | 3712 | 0.06 | −0.57 | 0.69 | 0.19 (0.853) | 99.0 | |
| Target population | Individual | 4 | 4,10,11,12 | 3615 | 0.11 | −0.58 | 0.79 | 0.31 (0.758) | 99.2 | |
| Family and community | 1 | 8 | 97 | −0.25 | −0.65 | 0.16 | 0.28 (0.231) | 0.0 | ||
| Measurement | repeated | 2 | 4,8 | 1720 | 0.01 | −1.22 | 1.24 | 0.02 (0.986) | 99.5 | |
| post | 3 | 10,11,12 | 1992 | 0.10 | −0.08 | 0.27 | 1.07 (0.284) | 71.5 | ||
| Quality assessment scores | <10 | 2 | 4,8 | 1720 | 0.01 | −1.22 | 1.24 | 0.02 (0.986) | 99.5 | |
| ≥10 | 3 | 10,11,12 | 1992 | 0.10 | −0.08 | 0.27 | 1.07 (0.284) | 71.5 | ||
| Amount of drinking | Age | <16 | 3 | 1,7,8 | 9824 | −0.22 | −0.38 | −0.07 | −2.82 (0.005) | 76.0 |
| ≥16 | 5 | 5,6,9,10,12 | 1690 | −0.68 | −1.87 | 0.50 | −1.13 (0.259) | 99.1 | ||
| Number of participants | <500 | 5 | 5,6,8,9,12 | 1119 | −0.75 | −2.12 | 0.63 | −1.07 (0.286) | 99.0 | |
| ≥500 | 3 | 1,7,10 | 10,395 | −0.16 | −0.30 | −0.03 | −2.41 (0.016) | 77.5 | ||
| Number of schools | <10 | 6 | 5,6,8,9,10,12 | 1787 | −0.62 | −1.65 | 0.41 | −1.18 (0.239) | 98.9 | |
| ≥10 | 2 | 1,7 | 9727 | −0.22 | −0.39 | −0.05 | −2.54 (0.011) | 81.0 | ||
| Research design | RCT | 8 | 1,5,6,7,8,9,10,12 | 11,514 | −0.46 | −0.87 | −0.05 | −2.20 (0.028) | 98.2 | |
| Type of program | Skill acquisition | 1 | 1 | 795 | −0.29 | −0.40 | −0.18 | −5.01 (<0.001) | 0.0 | |
| Motivation | 7 | 5,6,7,8,9,10,12 | 10,719 | −0.54 | −1.17 | 0.10 | −1.65 (0.098) | 98.8 | ||
| Target population | Individual | 6 | 5,6,7,9,10,12 | 10,622 | −0.58 | −1.28 | 0.13 | −1.60 (0.109) | 99.0 | |
| Family and community | 2 | 1,8 | 892 | −0.29 | −0.40 | −0.18 | −5.20 (<0.001) | 0.0 | ||
| Measurement | repeated | 3 | 1,8,9 | 1343 | −0.88 | −1.88 | 0.12 | −1.72 (0.085) | 98.9 | |
| post | 5 | 5,6,7,10,12 | 10,171 | −0.02 | −0.16 | 0.11 | −0.35 (0.729) | 64.9 | ||
| Quality assessment scores | <10 | 3 | 1,8,9 | 1343 | −0.88 | −1.88 | 0.12 | −1.72 (0.085) | 98.9 | |
| ≥10 | 5 | 5,6,7,10,12 | 10,171 | −0.02 | −0.16 | 0.11 | −0.35 (0.729) | 64.9 | ||
| Frequency of Binge drinking | Age | <16 | 1 | 8 | 97 | −0.19 | −0.59 | 0.22 | −0.91 (0.363) | 0.0 |
| ≥16 | 5 | 4,6,10,11,12 | 3836 | 0.35 | −0.45 | 1.16 | 0.86 (0.391) | 99.4 | ||
| Number of participants | <500 | 3 | 6,8,12 | 601 | −0.21 | −0.38 | −0.05 | −2.61 (0.009) | 0.0 | |
| ≥500 | 3 | 4,10,11 | 3332 | 0.58 | −0.45 | 1.61 | 1.09 (0.274) | 99.6 | ||
| Number of schools | <10 | 5 | 4,6,8,10,12 | 2892 | 0.33 | −0.59 | 1.26 | 0.71 (0.479) | 99.4 | |
| ≥10 | 1 | 11 | 1041 | −0.04 | −0.16 | 0.08 | −0.63 (0.527) | 0.0 | ||
| Research design | RCT | 6 | 4,6,8,10,11,12 | 3933 | 0.29 | −0.46 | 1.03 | 0.76 (0.450) | 99.3 | |
| Type of program | Motivation | 6 | 4,6,8,10,11,12 | 3933 | 0.29 | −0.46 | 1.03 | 0.76 (0.450) | 99.3 | |
| Target population | Individual | 5 | 4,6,10,11,12 | 3836 | 0.35 | −0.45 | 1.16 | 0.86 (0.391) | 99.4 | |
| Family and community | 1 | 8 | 97 | −0.19 | −0.59 | 0.22 | −0.91 (0.363) | 0.0 | ||
| Measurement | repeated | 2 | 4,8 | 1720 | 0.70 | −0.95 | 2.35 | 0.83 (0.406) | 99.7 | |
| post | 4 | 6,10,11,12 | 2213 | −0.10 | −0.20 | 0.01 | −1.84 (0.066) | 26.8 | ||
| Quality assessment scores | <10 | 2 | 4,8 | 1720 | 0.70 | −0.95 | 2.35 | 0.83 (0.406) | 99.7 | |
| ≥10 | 4 | 6,10,11,12 | 2213 | −0.10 | −0.20 | 0.01 | −1.84 (0.066) | 26.8 | ||
| Variable | K | Study No. | N | Hg | 95% CI | Z (p) | I2 (%) | |
|---|---|---|---|---|---|---|---|---|
| Lower Limit | Upper Limit | |||||||
| Knowledge | 2 | 2,3 | 2483 | 0.54 | 0.03 | 1.06 | 2.06 (0.039) | 97.7 |
| Attitudes | 2 | 2,3 | 2483 | −0.01 | −0.10 | 0.08 | −0.21 (0.835) | 35.9 |
| Harm associated with alcohol use | 2 | 2,6 | 3174 | 0.01 | −0.06 | 0.08 | 0.41 (0.683) | 0.0 |
| Intention to drink alcohol | 3 | 3,5,12 | 646 | 0.07 | −0.08 | 0.23 | 0.90 (0.366) | 0.0 |
| Self-efficacy | 2 | 5,7 | 8999 | 0.02 | −0.02 | 0.07 | 1.12 (0.263) | 0.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cho, M.-K.; Cho, Y.-H. Do Alcohol Prevention Programs Influence Adolescents’ Drinking Behaviors? A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 8524. https://doi.org/10.3390/ijerph18168524
Cho M-K, Cho Y-H. Do Alcohol Prevention Programs Influence Adolescents’ Drinking Behaviors? A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2021; 18(16):8524. https://doi.org/10.3390/ijerph18168524
Chicago/Turabian StyleCho, Mi-Kyoung, and Yoon-Hee Cho. 2021. "Do Alcohol Prevention Programs Influence Adolescents’ Drinking Behaviors? A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 18, no. 16: 8524. https://doi.org/10.3390/ijerph18168524
APA StyleCho, M. -K., & Cho, Y. -H. (2021). Do Alcohol Prevention Programs Influence Adolescents’ Drinking Behaviors? A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health, 18(16), 8524. https://doi.org/10.3390/ijerph18168524