A Cardiac Force Index Applied to the G Tolerance Test and Surveillance among Male Military Aircrew

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Mobile Monitoring Device for Cardiac Function
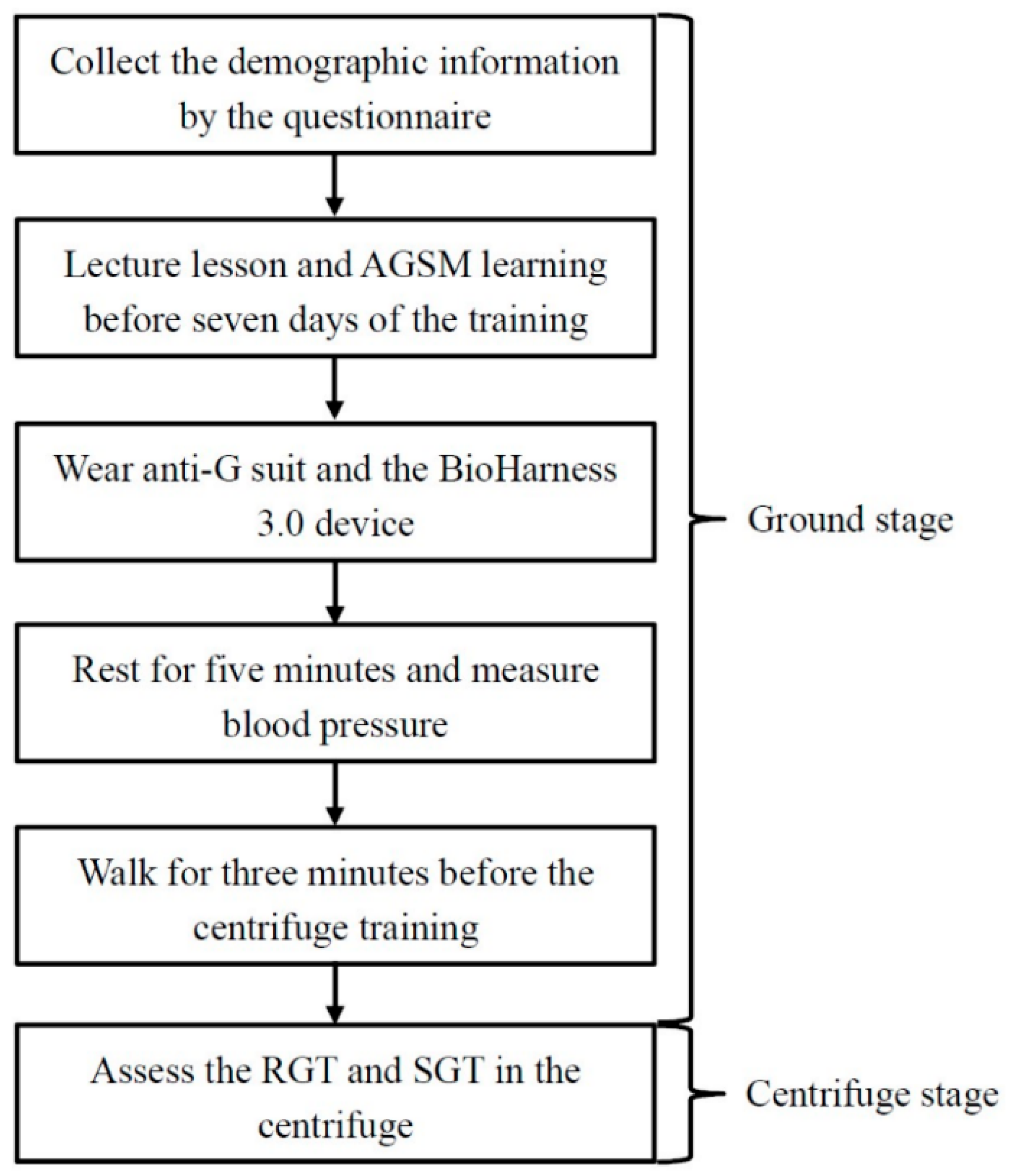
2.3. Study Protocol and Data Collection
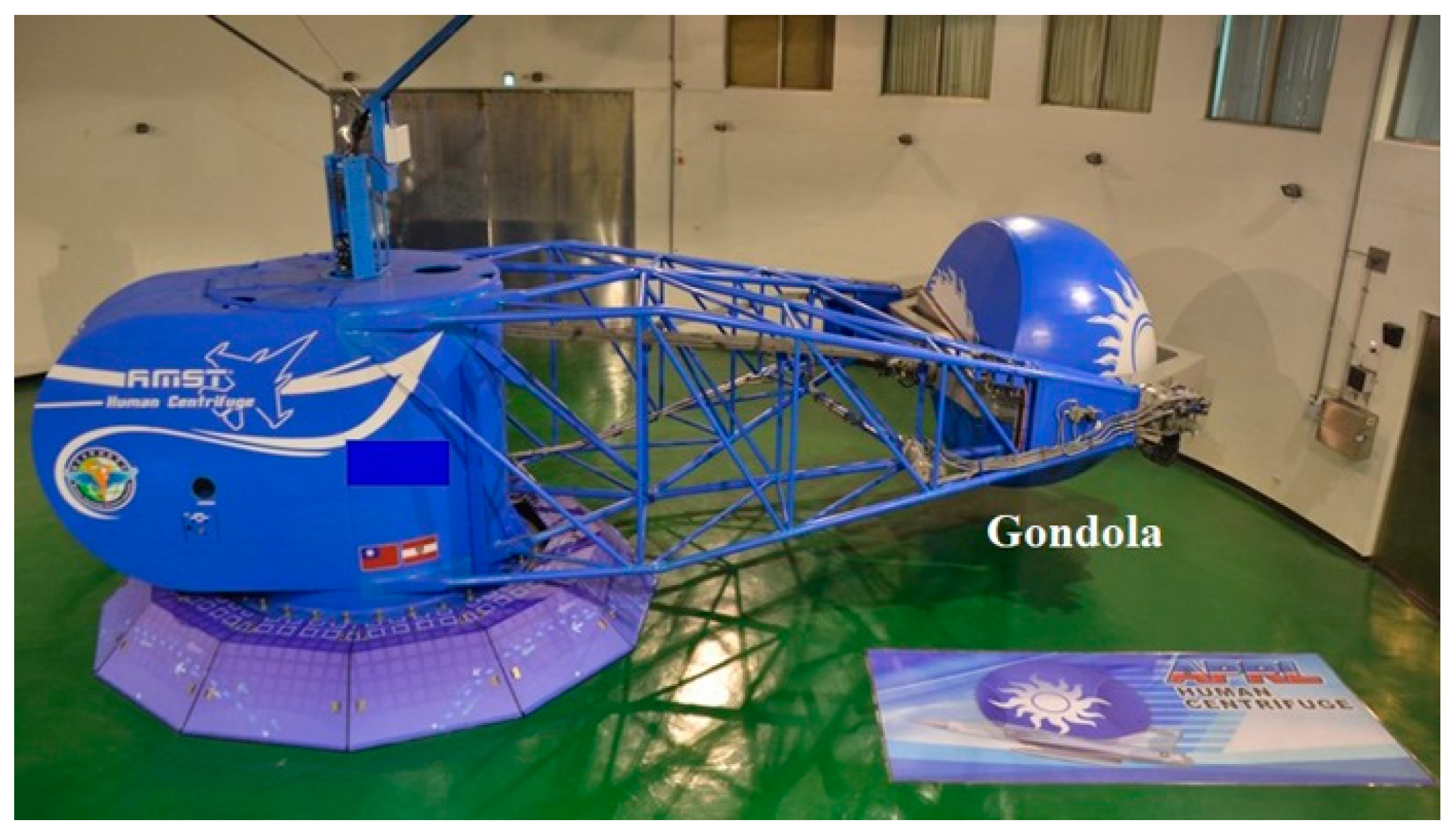
2.4. Centrifuge Stage
2.5. Data Processing of Cardiac Function
- Activity: Level and amount of activity represents the movement of the participants recorded every second by the accelerometer sensors inside the BioHarness 3.0.
- HR: The number of beats per minute (bpm) while resting or walking was also measured by the sensor and provided as an average at the time span of one second on the BioHarness 3.0 Summary Excel file report.
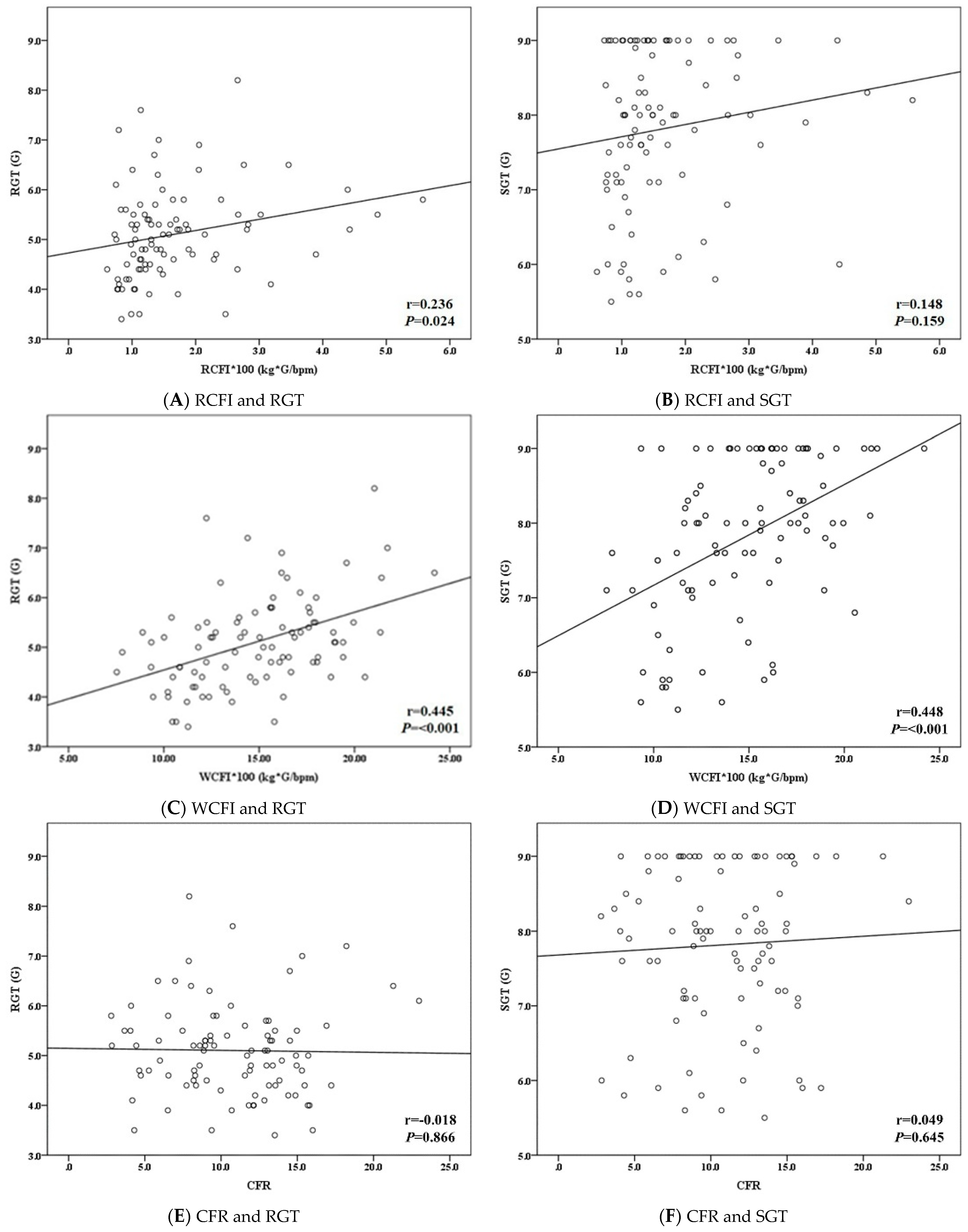
- CFI: There are two different types of CFI, resting CFI (RCFI) and walking CFI (WCFI), illustrated in this study. The average value of the RCFI was calculated by the two-minute data before the end of sit-resting status. For the WCFI, the mean value was identified by the two-minute data before the end of walking status on the ground.
- Cardiac force ratio (CFR): The average value of the CFR was calculated using the two-minute WCFI divided by the two-minute RCFI.
2.6. Statistical Analysis
3. Results
3.1. Characteristics of Study Participants
3.2. Physiological Responses on the Ground and during the G Tolerance Test
3.3. Relationship between CFI and G Tolerance Examined by Multivariate Regression
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Burton, R.; Whinnery, J. Biodynamics: Sustained acceleration In Fundamentals of Aerospace Medicine, 3rd ed.; DeHart, R.L., Davis, J.R., Eds.; Lippincott Williams and Wilkins: Baltimore, MD, USA, 2002; pp. 122–153. [Google Scholar]
- Lalande, S.; Buick, F. Physiologic +Gz tolerance responses over successive +Gz exposures in simulated air combat maneuvers. Aviat. Space Environ. Med. 2009, 80, 1032–1038. [Google Scholar] [CrossRef]
- Ueda, K.; Ogawa, Y.; Yanagida, R.; Aoki, K.; Iwasaki, K. Dose-effect relationship between mild levels of hypergravity and autonomic circulatory regulation. Aerosp. Med. Hum. Perform. 2015, 86, 535–540. [Google Scholar] [CrossRef]
- Manen, O.; Dussault, C.; Sauvet, F.; Montmerle-Borgdorff, S. Limitations of stroke volume estimation by non-invasive blood pressure monitoring in hypergravity. PLoS ONE 2015, 10, e0121936. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoffmann, U.; Koschate, J.; Appell Coriolano, H.J.; Drescher, U.; Thieschäfer, L.; Dumitrescu, D.; Werner, A. Adaptation of systemic and pulmonary circulation to acute changes in gravity and body position. Aerosp. Med. Hum. Perform. 2019, 90, 688–695. [Google Scholar] [CrossRef] [PubMed]
- Yilmaz, U.; Cetinguc, M.; Akin, A. Visual symptoms and G-LOC in the operational environment and during centrifuge training of Turkish jet pilots. Aviat. Space Environ. Med. 1999, 70, 709–712. [Google Scholar] [PubMed]
- Cao, X.S.; Wang, Y.C.; Xu, L.; Yang, C.B.; Wang, B.; Geng, J.; Gao, Y.; Wu, Y.H.; Wang, X.Y.; Zhang, S.; et al. Visual symptoms and G-induced loss of consciousness in 594 Chinese Air Force aircrew—A questionnaire survey. Mil. Med. 2012, 177, 163–168. [Google Scholar] [CrossRef] [Green Version]
- Slungaard, E.; McLeod, J.; Green, N.D.C.; Kiran, A.; Newham, D.J.; Harridge, S.D.R. Incidence of G-induced loss of consciousness and almost loss of consciousness in the Royal Air Force. Aerosp. Med. Hum. Perform. 2017, 88, 550–555. [Google Scholar] [CrossRef]
- Stevenson, A.T.; Scott, J.P.; Chiesa, S.; Sin, D.; Coates, G.; Bagshaw, M.; Harridge, S. Blood pressure, vascular resistance, and +Gz tolerance during repeated +Gz exposures. Aviat. Space Environ. Med. 2014, 85, 536–542. [Google Scholar] [CrossRef]
- Tu, M.Y.; Chu, H.; Chen, H.H.; Chiang, K.T.; Hu, J.M.; Li, F.L.; Yang, C.S.; Cheng, C.C.; Lai, C.Y. Roles of physiological responses and anthropometric factors on the gravitational force tolerance for occupational hypergravity exposure. Int. J. Environ. Res. Public Health 2020, 17, 8061. [Google Scholar] [CrossRef]
- Tu, M.Y.; Chu, H.; Lin, Y.J.; Chiang, K.T.; Chen, C.M.; Chen, H.H.; Yang, C.S.; Lai, C.Y. Combined effect of heart rate responses and the anti-G straining manoeuvre effectiveness on G tolerance in a human centrifuge. Sci. Rep. 2020, 10, 21611. [Google Scholar] [CrossRef]
- Eiken, O.; Kölegärd, R.; Bergsten, E.; Grönkvist, M. G protection: Interaction of straining maneuvers and positive pressure breathing. Aviat. Space Environ. Med. 2007, 78, 392–398. [Google Scholar]
- Sundblad, P.; Kölegård, R.; Eiken, O. G tolerance and the vasoconstrictor reserve. Eur. J. Appl. Physiol. 2014, 114, 2521–2528. [Google Scholar] [CrossRef] [PubMed]
- Pipraiya, M.; Tripathi, K.; Dogra, M. Effects of +Gz acceleration on indices of heart rate variability. Ind. J. Aerosp. Med. 2005, 49, 37–47. [Google Scholar]
- Newman, D.G.; White, S.W.; Callister, R. Evidence of baroreflex adaptation to repetitive +Gz in fighter pilots. Aviat. Space Environ. Med. 1998, 69, 446–451. [Google Scholar] [PubMed]
- Lai, C.; Tu, M.; Chu, H.; Liu, C. Cardiac performance of cadets during the centrifuge training with rapid onset rate. Aerosp. Med. Hum. Perform. 2019, 90, 225. [Google Scholar]
- Hsiao, P.J.; Chiu, C.C.; Lin, K.H.; Hu, F.K.; Tsai, P.J.; Wu, C.T.; Pang, Y.K.; Lin, Y.; Kuo, M.H.; Chen, K.H.; et al. Usability of wearable devices with a novel cardiac force index for estimating the dynamic cardiac function: Observational study. JMIR Mhealth Uhealth 2020, 8, e15331. [Google Scholar] [CrossRef] [PubMed]
- United States Patent Office. Method for Detecting Cardiac Status, Method for Monitoring Cardiac Status during Exercise, and Apparatus for Monitoring Cardiac Status. Available online: https://patents.google.com/patent/US20160058314 (accessed on 1 July 2021).
- Chu, C. Method for Detecting Cardiac Status, Method for Monitoring Cardiac Status during Exercise and Apparatus for Monitoring Cardiac Status. Taiwan Patent No. 408 I546051, 16 March 2016. [Google Scholar]
- Webb, J.T.; Oakley, C.J.; Meeker, L.J. Unpredictability of fighter pilot G tolerance using anthropometric and physiologic variables. Aviat. Space Environ. Med. 1991, 62, 128–135. [Google Scholar]
- Zephyr Technology Corporation. Zephyr™ BioHarness 3.0 User Manual. Available online: https://www.zephyranywhere.com/media/download/bioharness3-user-manual.pdf (accessed on 1 July 2021).
- Rice, G.M.; VanBrunt, T.B.; Snider, D.H.; Hoyt, R.E. Wearable accelerometers in high performance jet aircraft. Aerosp. Med. Hum. Perform. 2016, 87, 102–107. [Google Scholar] [CrossRef] [PubMed]
- United States Air Force. G Awareness for Aircrew. Available online: https://static.e-publishing.af.mil/production/1/af_a3_5/publication/afpam11-419/afpam11-419.pdf (accessed on 23 March 2021).
- Whinnery, J.E. +Gz tolerance correlation with clinical parameters. Aviat. Space Environ. Med. 1979, 50, 736–741. [Google Scholar]
- Yun, C.; Oh, S.; Shin, Y.H. AGSM proficiency and depression are associated with success of high-G training in trainee pilots. Aerosp. Med. Hum. Perform. 2019, 90, 613–617. [Google Scholar] [CrossRef]
- Scott, J.P.; Jungius, J.; Connolly, D.; Stevenson, A.T. Subjective and objective measures of relaxed +Gz tolerance following repeated +Gz exposure. Aviat. Space Environ. Med. 2013, 84, 684–691. [Google Scholar] [CrossRef]
- Park, M.; Yoo, S.; Seol, H.; Kim, C.; Hong, Y. Unpredictability of fighter pilots’ g duration tolerance by anthropometric and physiological characteristics. Aerosp. Med. Hum. Perform. 2015, 86, 397–401. [Google Scholar] [CrossRef]
- Bulbulian, R.; Crisman, R.P.; Thomas, M.L.; Meyer, L.G. The effects of strength training and centrifuge exposure on +Gz tolerance. Aviat. Space Environ. Med. 1994, 65, 1097–1104. [Google Scholar]
- Epperson, W.L.; Burton, R.R.; Bernauer, E.M. The influence of differential physical conditioning regimens on simulated aerial combat maneuvering tolerance. Aviat. Space Environ. Med. 1982, 53, 1091–1097. [Google Scholar]
- Epperson, W.L.; Burton, R.R.; Bernauer, E.M. The effectiveness of specific weight training regimens on simulated aerial combat maneuvering G tolerance. Aviat. Space Environ. Med. 1985, 56, 534–539. [Google Scholar]
- Tesch, P.A.; Hjort, H.; Balldin, U.I. Effects of strength training on G tolerance. Aviat. Space Environ. Med. 1983, 54, 691–695. [Google Scholar]
- Whinnery, J.E.; Parnell, M.J. The effects of long-term aerobic conditioning on +Gz tolerance. Aviat. Space Environ. Med. 1987, 58, 199–204. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Mean ± SD/n (%) | Min | Max |
|---|---|---|---|
| Age (years) | 26.17 ± 4.52 | 22 | 47 |
| Male | 92 (100%) | ||
| Height (cm) | 174.63 ± 5.69 | 162 | 188 |
| Weight (kg) | 74.39 ± 11.89 | 53 | 104 |
| BMI (kg/m2) | 24.35 ± 3.38 | 15.34 | 34.28 |
| Smoking status | |||
| No | 72 (78.3%) | ||
| Yes | 20 (21.7%) | ||
| Drinking status | |||
| No | 78 (84.8%) | ||
| Yes | 14 (15.2%) | ||
| Exercise habits | |||
| No | 47 (51.1%) | ||
| Yes | 45 (48.9%) |
| Variables | Mean ± SD | Min | Max |
|---|---|---|---|
| SBP (mmHg) | 141.80 ± 13.75 | 108 | 177 |
| DBP (mmHg) | 80.78 ± 7.03 | 65 | 104 |
| HR (bpm) | 84.07 ± 11.15 | 66 | 122 |
| RCFI (kg × G/bpm) | 0.02 ± 0.01 | 0.01 | 0.06 |
| WCFI (kg × G/bpm) | 0.15 ± 0.04 | 0.08 | 0.24 |
| CFR | 10.77 ± 4.11 | 2.80 | 22.98 |
| RGT (G) | 5.1 ± 0.9 | 3.4 | 8.2 |
| <5 G | 42 (45.7%) | ||
| ≥5 G | 50 (54.3%) | ||
| SGT (G) | 7.8 ± 1.1 | 5.5 | 9.0 |
| <8 G | 42 (45.7%) | ||
| ≥8 G | 50 (54.3%) |
| Model/Variables | β | SE | p | 95% CI |
|---|---|---|---|---|
| RGT Model | ||||
| Height (cm) | −0.06 | 0.02 | <0.001 | −0.08 to −0.03 |
| WCFI × 100 (kg × G/bpm) | 0.14 | 0.02 | <0.001 | 0.09 to 0.19 |
| SGT Model | ||||
| Height (cm) | −0.08 | 0.02 | <0.001 | −0.11 to −0.05 |
| WCFI × 100 (kg × G/bpm) | 0.17 | 0.03 | <0.001 | 0.11 to 0.22 |
| Model/Variables | Group | β | SE | p | OR | 95% CI |
|---|---|---|---|---|---|---|
| RGT Model (≥5 G vs. <5 G) | ||||||
| Exercise habits | yes vs. no | 1.10 | 0.47 | 0.019 | 3.01 | 1.20 to 7.52 |
| WCFI × 100 (kg × G/bpm) | 0.23 | 0.07 | 0.001 | 1.26 | 1.10 to 1.46 | |
| SGT Model (≥8 G vs. <8 G) | ||||||
| Height (cm) | −0.21 | 0.06 | 0.001 | 0.81 | 0.72 to 0.91 | |
| WCFI × 100 (kg × G/bpm) | 0.41 | 0.10 | <0.001 | 1.50 | 1.24 to 1.82 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chiang, K.-T.; Tu, M.-Y.; Lin, Y.-J.; Hsin, Y.-H.; Chiu, Y.-L.; Li, F.-L.; Chen, H.-H.; Lai, C.-Y. A Cardiac Force Index Applied to the G Tolerance Test and Surveillance among Male Military Aircrew. Int. J. Environ. Res. Public Health 2021, 18, 8832. https://doi.org/10.3390/ijerph18168832
Chiang K-T, Tu M-Y, Lin Y-J, Hsin Y-H, Chiu Y-L, Li F-L, Chen H-H, Lai C-Y. A Cardiac Force Index Applied to the G Tolerance Test and Surveillance among Male Military Aircrew. International Journal of Environmental Research and Public Health. 2021; 18(16):8832. https://doi.org/10.3390/ijerph18168832
Chicago/Turabian StyleChiang, Kwo-Tsao, Min-Yu Tu, You-Jin Lin, Yi-Hsiang Hsin, Yu-Lung Chiu, Fang-Ling Li, Hsin-Hui Chen, and Chung-Yu Lai. 2021. "A Cardiac Force Index Applied to the G Tolerance Test and Surveillance among Male Military Aircrew" International Journal of Environmental Research and Public Health 18, no. 16: 8832. https://doi.org/10.3390/ijerph18168832
APA StyleChiang, K. -T., Tu, M. -Y., Lin, Y. -J., Hsin, Y. -H., Chiu, Y. -L., Li, F. -L., Chen, H. -H., & Lai, C. -Y. (2021). A Cardiac Force Index Applied to the G Tolerance Test and Surveillance among Male Military Aircrew. International Journal of Environmental Research and Public Health, 18(16), 8832. https://doi.org/10.3390/ijerph18168832