Effectiveness of a Novel HIV Self-Testing Service with Online Real-Time Counseling Support (HIVST-Online) in Increasing HIV Testing Rate and Repeated HIV Testing among Men Who Have Sex with Men in Hong Kong: Results of a Pilot Implementation Project


 and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Recruitment Process
2.4. Training of CBO Staff
2.5. Baseline Telephone Survey and Health Promotion
- (1)
- An online video promoting HIVST-online: The video was used in the previous RCT [24]. In the video, a local MSM narratively discussed the benefits and barriers of HIVST-online, demonstrated its procedures, and emphasized that HIVST was easy to use, as well as the availability of immediate online support.
- (2)
- A new online video promoting regular HIV testing. The video was based on the maintenance theories [27]. In the video, a peer MSM shared his positive experience of using HIVST-online, and emphasized the importance of regular HIV testing.
- (3)
- An online demonstration video on how to use oral fluid-based HIVST kits.
- (4)
- Other health promotion components, including: (i) description of the project, (ii) knowledge and benefit of the HIVST, (iii) information about HIV epidemic among MSM in Hong Kong, (iv) a discussion forum containing positive feedbacks of HIVST-online users, and (v) contact of the program staff (phone, social media, and email).
2.6. Implementation of HIVST-Online
2.7. Month 6 Follow-Up Telephone Survey
2.8. Measurements
2.8.1. Primary Outcome
2.8.2. Baseline Background Characteristics
2.8.3. Perceptions Related to HIVST Measured at the Baseline
2.8.4. Process Evaluation
2.9. Ethics Statement
2.10. Statistical Analysis
3. Results
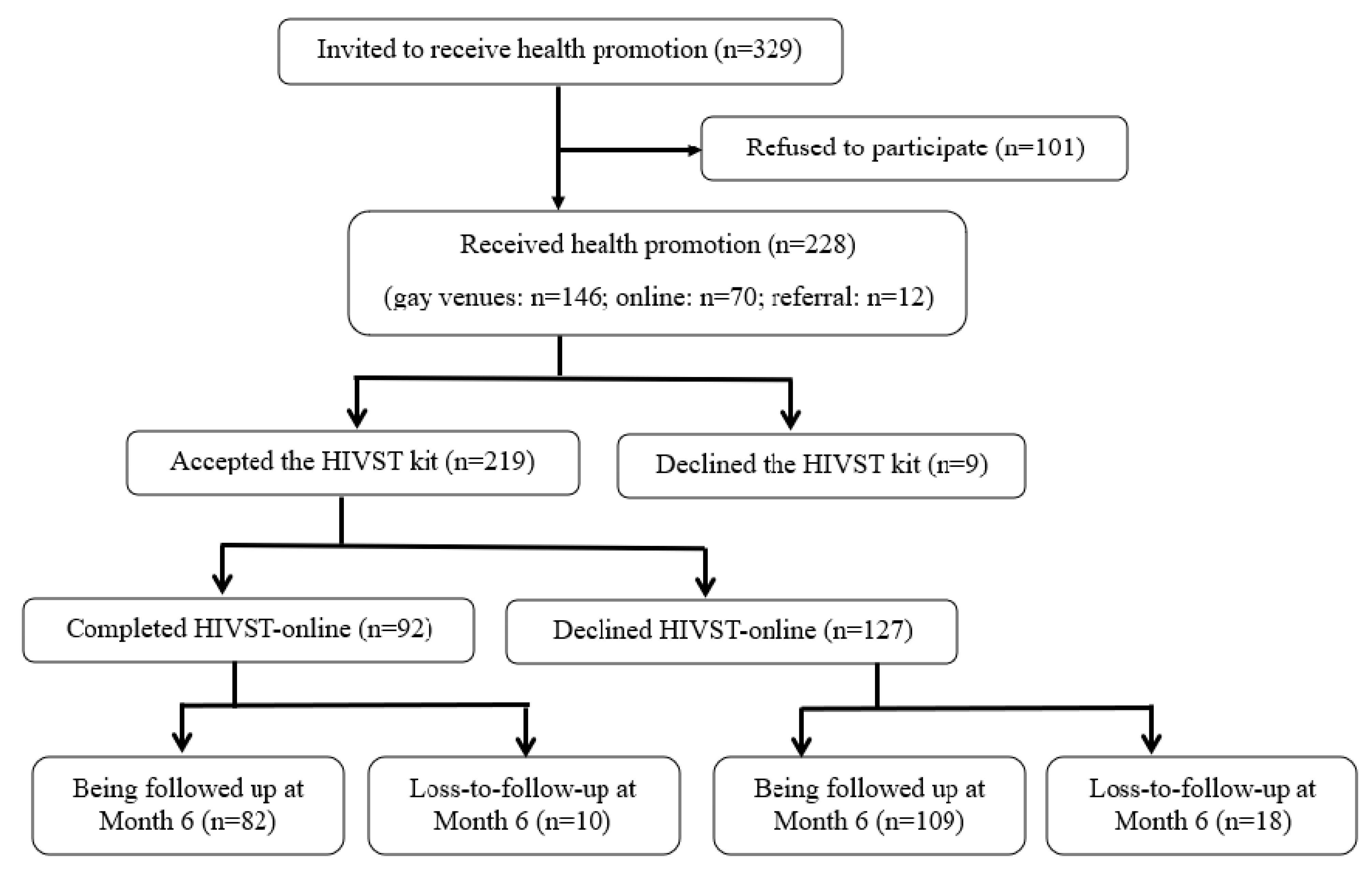
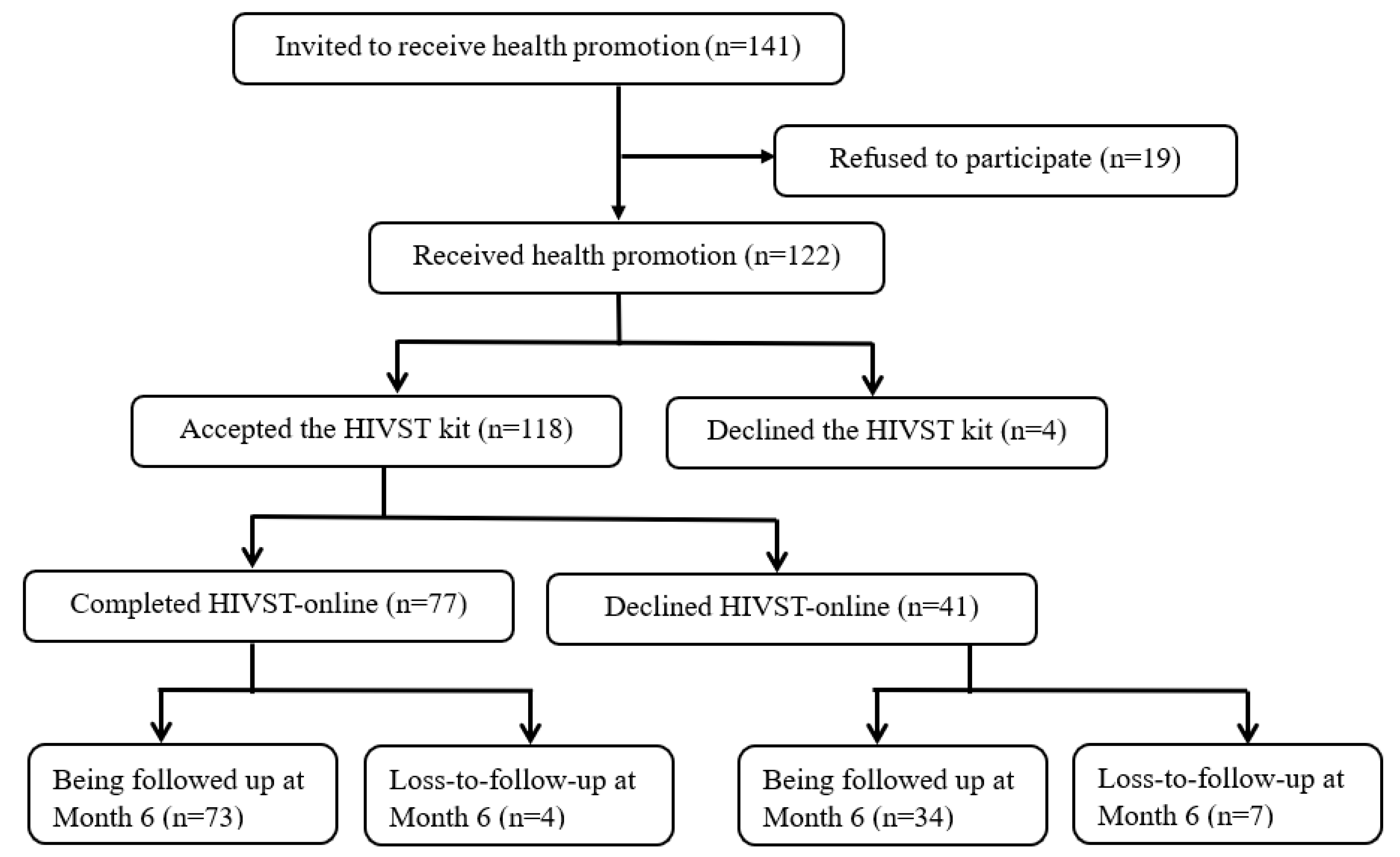
3.1. Baseline Characteristics
3.2. HIV Testing Uptake during the Follow-Up Period
3.3. Factors Predicting HIVST-Online Uptake
3.4. Process Evaluation of HIVST-Online Users
3.5. Baseline Characteristics between Those Who Declined and Received HIVST-Online
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Beyrer, C.; Baral, S.D.; Walker, D.; Wirtz, A.L.; Johns, B.; Sifakis, F. The expanding epidemics of HIV type 1 among men who have sex with men in low- and middle-income countries: Diversity and consistency. Epidemiol. Rev. 2010, 32, 137–151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, X.; Lu, H.; Cox, C.; Zhao, Y.; Xia, D.; Sun, Y.; He, X.; Xiao, Y.; Ruan, Y.; Jia, Y.; et al. Changing the landscape of the HIV epidemic among MSM in China: Results from three consecutive respondent-driven sampling surveys from 2009 to 2011. Biomed Res. Int. 2014, 2014, 563517. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sullivan, P.S.; Jones, J.S.; Baral, S.D. The global north: HIV epidemiology in high-income countries. Curr. Opin. HIV AIDS 2014, 9, 199–205. [Google Scholar] [CrossRef] [PubMed]
- National Health and Family Planning Commission of the People’s Republic of China. China AIDS Response Progress Report. 2015. Available online: https://www.unaids.org/sites/default/files/country/documents/CHN_narrative_report_2015.pdf (accessed on 20 February 2020).
- Hong Kong Department of Health. PRiSM—HIV Prevalence and Risk Behavioural Survey of Men Who Have Sex with Men in Hong Kong 2017. Available online: https://www.aids.gov.hk/english/surveillance/sur_report/prism2017e.pdf (accessed on 15 February 2020).
- Hong Kong Department of Health. HIV Surveillance Report—2018 Update. Available online: https://www.aids.gov.hk/english/surveillance/sur_report/hiv18.pdf (accessed on 10 February 2020).
- Anglemyer, A.; Rutherford, G.W.; Horvath, T.; Baggaley, R.C.; Egger, M.; Siegfried, N. Antiretroviral therapy for prevention of HIV transmission in HIV-discordant couples. Cochrane Database Syst. Rev. 2013, 4, CD009153. [Google Scholar]
- Tanser, F.; Barnighausen, T.; Grapsa, E.; Zaidi, J.; Newell, M.L. High coverage of ART associated with decline in risk of HIV acquisition in rural KwaZulu-Natal, South Africa. Science 2013, 339, 966–971. [Google Scholar] [CrossRef] [Green Version]
- Baeten, J.M.; Donnell, D.; Ndase, P.; Mugo, N.R.; Campbell, J.D.; Wangisi, J.; Tappero, J.W.; Bukusi, E.A.; Cohen, C.R.; Katabira, E.; et al. Antiretroviral prophylaxis for HIV prevention in heterosexual men and women. N. Engl. J. Med. 2012, 367, 399–410. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization (WHO). Guideline on When to Start Antiretroviral Therapy and on Pre-Exposure Prophylaxis for HIV. 2015. Available online: https://www.who.int/hiv/pub/guidelines/earlyrelease-arv/en/ (accessed on 20 February 2020).
- UNAIDS. An Ambitious Treatment Target to Help End the AIDS Epidemic. 2014. Available online: http://www.unaids.org/sites/default/files/media_asset/90-90-90_en_0.pdf (accessed on 16 February 2020).
- Hao, C.; Huan, X.; Yan, H.; Yang, H.; Guan, W.; Xu, X.; Zhang, M.; Wang, N.; Tang, W.; Gu, J.; et al. A randomized controlled trial to evaluate the relative efficacy of enhanced versus standard voluntary counseling and testing on promoting condom use among men who have sex with men in China. AIDS Behave. 2012, 16, 1138–1147. [Google Scholar] [CrossRef]
- Rotheram-Borus, M.J.; Newman, P.A.; Etzel, M.A. Effective detection of HIV. J. Acquir. Immune Defic. Syndr. 2000, 25, S105–S114. [Google Scholar] [CrossRef]
- World Health Organization (WHO); UNAIDS. Guidance on Provider-Initiated HIV Testing and Counselling in Health Facilities (Strengthening Health Services for Fight HIV/AIDS). 2007. Available online: http://www.who.int/hiv/pub/guidelines/9789241595568_en.pdf (accessed on 10 February 2020).
- Centers for Disease Control and Prevention (CDC). HIV testing among men who have sex with men–21 cities, United States. Morb. Mortal. Wkly. Rep. 2011, 60, 694. [Google Scholar]
- Hong Kong Advisory Council on AIDS. Recommended HIV/AIDS Strategies for Hong Kong (2017–2021). Available online: http://www.aca.gov.hk/english/strategies/pdf/strategies17-21.pdf.2017 (accessed on 13 April 2020).
- Gu, J.; Lau, J.T.; Wang, Z.; Wu, A.M.; Tan, X. Perceived empathy of service providers mediates the association between perceived discrimination and behavioral intention to take up HIV antibody testing again among men who have sex with men. PLoS ONE 2015, 10, e0117376. [Google Scholar] [CrossRef] [Green Version]
- Johnson, C.; Kennedy, C.; Fonner, V.; Siegfried, N.; Figueroa, C.; Dalal, S.; Sands, A.; Baggaley, R. Examining the effects of HIV self-testing compared to standard HIV testing services: A systematic review and meta-analysis. J. Int. AIDS Soc. 2017, 20, 21594. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. The WHO Guideline on HIV Self-Testing and Partner Notification. 2016. Available online: http://www.who.int/hiv/pub/vct/hiv-self-testing-guidelines/en/ (accessed on 15 April 2020).
- World Health Organization. HIV Self-Testing. 2019. Available online: https://www.who.int/hiv/topics/self-testing/en/ (accessed on 11 February 2020).
- Department of Health. HIV Self-Testing. Available online: https://dh-hivst.com.hk/en (accessed on 11 February 2020).
- World Health Organization. HIV Testing and Counselling: The Gateway to Treatment, Care and Support. 2003. Available online: https://www.who.int/3by5/publications/briefs/hiv_testing_counselling/en/ (accessed on 6 August 2020).
- Katz, D.A.; Cassels, S.L.; Stekler, J.D. Response to the modeling analysis by Katz et al. on the impact of replacing clinic-based HIV tests with home testing among men who have sex with men in Seattle: Authors’ reply. Sex Transm. Dis. 2014, 41, 320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Z.; Lau, J.; Ip, M.; Ho, S.P.Y.; Mo, P.K.H.; Latkin, C.; Ma, Y.L.; Kim, Y. A randomized controlled trial evaluating efficacy of promoting a home-based HIV self-testing with online counseling on increasing HIV testing among men who have sex with men. AIDS Behave. 2018, 22, 190–201. [Google Scholar] [CrossRef] [PubMed]
- Center for Disease Control and Prevention. Home-Based HIV Self-Testing with Online Instruction and Counseling (HIVST-OIC). Available online: https://www.cdc.gov/hiv/pdf/research/interventionresearch/compendium/si/cdc-hiv-Home_Based_HIV_Self_Testing_Online_SI_EBI.pdf (accessed on 23 July 2020).
- The Chinese University of Hong Kong. Guidelines for Survey and Behavioral Research Ethics. Available online: https://www.orkts.cuhk.edu.hk/images/Research_Funding/SBRE_appguide_Aug_2018.pdf (accessed on 23 November 2020).
- Prochaska, J.O.; Redding, C.A.; Harlow, L.L.; Rossi, J.S.; Velicer, W.F. The transtheoretical model of change and HIV prevention: A review. Health Educ. Q. 1994, 21, 471–486. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Yang, X.; Mo, P.K.H.; Fang, Y.; Ip, T.K.M.; Lau, J.T.F. Influence of Social Media on Sexualized Drug Use and Chemsex Among Chinese Men Who Have Sex With Men: Observational Prospective Cohort Study. J. Med. Internet Res. 2020, 22, e17894. [Google Scholar] [CrossRef]
- Janz, N.K.; Becker, M.H. The Health Belief Model: A decade later. Health Educ. Q. 1984, 11, 1–47. [Google Scholar] [CrossRef] [Green Version]
- Kwan, N.; Wong, A.; Fang, Y.; Wang, Z. ‘Get an early check—Chrysanthemum tea’: An outcome evaluation of a multimedia campaign promoting HIV testing among men who have sex with men in Hong Kong. HIV Med. 2018, 19, 347–354. [Google Scholar] [CrossRef]
- Zhong, F.; Tang, W.; Cheng, W.; Lin, P.; Wu, Q.; Cai, Y.; Tang, S.; Fan, L.; Zhao, Y.; Chen, X.; et al. Acceptability and feasibility of a social entrepreneurship testing model to promote HIV self-testing and linkage to care among men who have sex with men. HIV Med. 2017, 18, 376–382. [Google Scholar] [CrossRef]
- Noar, S.M.; Benac, C.N.; Harris, M.S. Does tailoring matter? Meta-analytic review of tailored print health behavior change interventions. Psychol. Bull. 2007, 133, 673–693. [Google Scholar] [CrossRef] [Green Version]
- Lach, H.W.; Everard, K.M.; Highstein, G.; Brownson, C.A. Application of the transtheoretical model to health education for older adults. Health Promot. Pract. 2004, 5, 88–93. [Google Scholar] [CrossRef]
- Paiva, A.L.; Lipschitz, J.M.; Fernandez, A.C.; Redding, C.A.; Prochaska, J.O. Evaluation of the acceptability and feasibility of a computer-tailored intervention to increase human papillomavirus vaccination among young adult women. J. Am. Coll. Health 2014, 62, 32–38. [Google Scholar] [CrossRef] [PubMed]
- Bustamante, M.J.; A Konda, K.; Davey, D.L.J.; León, S.R.; Calvo, G.M.; Salvatierra, J.; Brown, B.; Caceres, C.F.; Klausner, J.D. HIV self-testing in Peru: Questionable availability, high acceptability but potential low linkage to care among men who have sex with men and transgender women. Int. J. Std. AIDS 2017, 28, 133–137. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| All (n = 350) | New-Users of HIVST-Online (n = 228) | Ever-Users of HIVST-Online (n = 122) | p-Value | |
|---|---|---|---|---|
| % | % | % | ||
| Socio-demographic characteristics | ||||
| Age group (years) | ||||
| 18–30 | 57.1 | 54.4 | 62.3 | |
| 31–40 | 31.4 | 34.6 | 25.4 | |
| >40 | 11.4 | 11.0 | 12.3 | 0.21 |
| Marital/cohabitation status | ||||
| Currently single | 83.1 | 79.4 | 90.2 | |
| Cohabitate/married with a man | 16.6 | 20.6 | 9.0 | |
| Cohabited/married with a woman | 0.3 | 0 | 0.8 | 0.01 |
| Highest education level attained | ||||
| Secondary or below | 13.4 | 12.7 | 14.8 | |
| College or above | 86.6 | 87.3 | 85.2 | 0.60 |
| Current employment status | ||||
| Full-time | 84.3 | 86.0 | 81.1 | |
| Part-time/unemployed/retired/student | 15.7 | 14.0 | 18.9 | 0.24 |
| Sexual orientation | ||||
| Gay | 93.1 | 93.4 | 92.6 | |
| Bisexual | 6.3 | 5.7 | 7.4 | |
| Heterosexual | 0.6 | 0.9 | 0 | 0.49 |
| History of sexually transmitted infection | ||||
| No | 79.1 | 74.1 | 87.7 | |
| Yes | 20.9 | 25.4 | 12.3 | 0.004 |
| HIV testing history | ||||
| No. of HIV testing in the past 3 years in addition to HIVST-online | ||||
| 0 | 17.4 | 16.2 | 19.7 | |
| 1–3 | 44.0 | 38.6 | 54.1 | |
| >3 | 38.6 | 45.2 | 26.2 | 0.002 |
| Sexual behaviors in the last 3 months | ||||
| Anal intercourse with regular male sex partner(s) (RP) | ||||
| No | 30.0 | 25.9 | 36.9 | |
| Yes | 70.0 | 74.1 | 62.3 | 0.02 |
| Anal intercourse with non-regular male sex partner(s) (NRP) | ||||
| No | 54.6 | 57.0 | 50.0 | |
| Yes | 45.1 | 43.0 | 49.2 | 0.24 |
| Condomless anal intercourse (CAI) with men | ||||
| No | 54.9 | 57.0 | 50.8 | |
| Yes | 35.1 | 34.6 | 36.1 | 0.52 |
| Multiple male sex partnerships | ||||
| No | 56.3 | 59.2 | 50.8 | |
| Yes | 43.7 | 40.8 | 49.2 | 0.13 |
| Illicit drug use before/during anal intercourse with men | ||||
| No | 96.6 | 96.5 | 96.7 | |
| Yes | 3.4 | 3.5 | 3.3 | 0.91 |
| Perceptions related to HIV testing | ||||
| Behavioral intention to use free HIVST with real-time counseling services in the coming 6 months | ||||
| Unlikely/neutral | 25.7 | 26.3 | 24.6 | |
| Likely | 74.3 | 73.7 | 75.4 | 0.73 |
| Perceived logistical benefits of HIVST (% agree/strongly agree) | ||||
| HIVST is easy for you to use | 76.0 | 74.1 | 79.5 | |
| HIVST is convenient for you | 82.3 | 81.6 | 83.6 | |
| Perceived Logistical Benefit Scale 1 (Mean/SD) | 8.1/1.6 | 7.9/1.5 | 8.4/1.8 | 0.01 |
| Perceived psychological benefits of HIVST (% agree/strongly agree) | ||||
| Using HIVST could reduce embarrassment | 79.1 | 77.6 | 82.0 | |
| Using HIVST could avoid being stigmatized by service providers | 50.0 | 42.5 | 63.9 | |
| Using HIVST could protect your privacy | 84.0 | 82.0 | 87.7 | |
| Perceived Psychological Benefit Scale 2 (Mean/SD) | 11.5/2.6 | 10.9/2.6 | 12.4/2.4 | <0.001 |
| Perceived logistical barriers of HIVST (% agree/strongly agree) | ||||
| HIVST is expensive for you | 57.1 | 59.6 | 52.5 | |
| It is difficult for you to buy a HIVST kit | 54.0 | 51.8 | 58.2 | |
| You do not know how to choose a reliable HIVST kit | 70.0 | 69.3 | 71.3 | |
| You are concerned about the accuracy of HIVST | 53.4 | 57.9 | 45.1 | |
| Perceived Logistical Barrier Scale 3 (Mean/SD) | 14.0/3.2 | 13.9/3.2 | 14.2/3.2 | 0.33 |
| Perceived psychological barrier of HIVST (% agree/strongly agree) | ||||
| You are not psychologically prepared to perform HIVST | 19.4 | 17.1 | 23.8 | |
| You are concerned about not understanding the HIVST results | 13.1 | 13.2 | 13.1 | |
| You cannot receive immediate psychological support if you have a positive HIVST result | 40.3 | 35.1 | 50.0 | |
| You cannot access the HIV treatment and care services if you have a positive HIVST result | 27.1 | 24.6 | 32.0 | |
| Perceived Psychological Barrier Scale 4 (Mean/SD) | 10.6/3.1 | 10.0/3.1 | 11.6/2.7 | <0.001 |
| Cue to action related to HIVST (% agree/strongly agree) | ||||
| Significant others will support you to do HIVST | 70.3 | 68.4 | 73.8 | |
| Male sex partner will support you to do HIVST | 78.9 | 79.4 | 77.9 | |
| Cue to Action Scale 5 (Mean/SD) | 7.9/1.6 | 7.8/1.5 | 8.1/1.9 | 0.05 |
| Perceived self-efficacy related to HIVST (% agree/strongly agree) | ||||
| You are confident to obtain a high-quality HIVST kit | 38.0 | 39.9 | 34.4 | |
| You are confident to use HIVST kits properly | 74.0 | 73.7 | 74.6 | |
| You are confident to understand the HIVST results | 78.6 | 79.4 | 77.0 | |
| You are confident to receive confirmatory testing after obtaining a positive HIVST result | 78.3 | 80.7 | 73.8 | |
| Perceived Self-efficacy Scale 6 (Mean/SD) | 14.8/2.4 | 14.8/2.4 | 14.9/2.4 | 0.63 |
| Perceived importance of real-time counseling service supporting HIVST users | ||||
| Very unimportant/ unimportant/neutral | 36.0 | 38.6 | 31.1 | |
| Important/very important | 64.0 | 61.4 | 68.9 | 0.17 |
| All | New-Users of HIVST-Online | Ever-Users of HIVST-Online | Ever-Users vs. New-Users | ||||
|---|---|---|---|---|---|---|---|
| % | % | % | |||||
| Among All Participants (n = 350) | n = 350 | n = 228 | n = 122 | OR (95%CI) | p-Value | AOR (95%CI) | p-Value |
| HIVST-online uptake as documented by the HIVST-administrators (% Yes) | 48.3 | 40.4 | 63.1 | 2.53 (1.61–3.98) | <0.001 | 3.01 (1.80–5.05) | <0.001 |
| Among participants who completed the month 6 post-test survey (n = 298) | n = 298 | n = 191 | n = 107 | OR (95%CI) | p-value | AOR (95%CI) | p-value |
| Uptake of other types of HIV testing reported by the participants at the post-test survey (% Yes) | |||||||
| Using HIVST kits obtained in the project without receiving online real-time counseling services | 1.0 | 0.5 | 1.9 | 3.62 (0.32–40.39) | 0.30 | 13.99 (0.86–226.91) | 0.06 |
| Self-purchased HIVST kits and used by themselves | 0.7 | 1.0 | 0 | N.A. | N.A. | N.A. | N.A. |
| HIV testing at governmental hospitals or clinics | 5.0 | 4.7 | 5.6 | 1.20 (0.42–3.47) | 0.74 | 1.54 (0.46–5.19) | 0.48 |
| HIV testing at non-governmental organizations (NGO) | 21.1 | 20.9 | 21.5 | 1.03 (0.58–1.84) | 0.91 | 2.43 (1.16–5.07) | 0.02 |
| HIV testing at private clinics/laboratories | 1.3 | 0.5 | 2.8 | 5.48 (0.56–53.36) | 0.14 | 4.47 (0.40–50.16) | 0.23 |
| Any type of HIV testing | 66.1 | 58.6 | 79.4 | 2.73 (1.57–4.73) | <0.001 | 4.82 (2.51–9.28) | <0.001 |
| OR (95% CI) | p-Value | |
|---|---|---|
| Socio-demographic characteristics | ||
| Age group (years) | ||
| 18–30 | 1.0 | |
| 31–40 | 1.31 (0.84–2.12) | 0.23 |
| >40 | 0.85 (0.43–1.69) | 0.64 |
| Marital/cohabitation status | ||
| Currently single | 1.0 | |
| Cohabitate/married with a man | 0.60 (0.34–1.07) | 0.08 |
| Cohabited/married with a woman | N.A. | N.A. |
| Highest education level attained | ||
| Secondary or below | 1.0 | |
| College or above | 0.80 (0.43–1.48) | 0.47 |
| Current employment status | ||
| Full-time | 1.0 | |
| Part-time/unemployed/retired/student | 0.67 (0.37–1.21) | 0.18 |
| Sexual orientation | ||
| Gay | 1.0 | |
| Bisexual | 0.48 (0.19–1.20) | 0.12 |
| Heterosexual | 1.03 (0.06–16.52) | 0.99 |
| History of sexually transmitted infection | ||
| No | 1.0 | |
| Yes | 0.79 (0.47–1.33) | 0.38 |
| HIV testing history | ||
| Number of HIV testing in the past 3 years | ||
| 0 | 1.0 | |
| 1–3 | 0.99 (0.55–1.80) | 0.99 |
| >3 | 1.07 (0.58–1.96) | 0.82 |
| Being new-users or ever-users of HIVST-online | ||
| New-users | 1.0 | |
| Ever-users | 2.53 (1.61–3.98) | <0.001 |
| Sexual behaviors in the last 3 months | ||
| Anal intercourse with regular male sex partner(s) (RP) | ||
| No | 1.0 | |
| Yes | 0.71 (0.45–1.12) | 0.14 |
| Anal intercourse with non-regular male sex partner(s) (NRP) | ||
| No | 1.0 | |
| Yes | 1.42 (0.93–2.16) | 0.11 |
| Condomless anal intercourse (CAI) with men | ||
| No | 1.0 | |
| Yes | 1.28 (0.82–2.02) | 0.28 |
| Multiple male sex partnerships | ||
| No | 1.0 | |
| Yes | 1.27 (0.83–1.94) | 0.27 |
| Illicit drug use before/during anal intercourse with men (sexualized drug use) | ||
| No | 1.0 | |
| Yes | 1.52 (0.47–4.89) | 0.48 |
| OR (95% CI) | p-Value | AOR (95% CI) | p-Value | |
|---|---|---|---|---|
| Perceived Logistical Benefit Scale | 1.00 (0.88–1.14) | 0.95 | 0.98 (0.84–1.15) | 0.82 |
| Perceived Psychological Benefit Scale | 1.01 (0.93–1.09) | 0.91 | 0.99 (0.91–1.09) | 0.91 |
| Perceived Logistical Barrier Scale | 1.03 (0.96–1.10) | 0.39 | 1.03 (0.96–1.11) | 0.39 |
| Perceived Psychological Barrier Scale | 1.00 (0.93–1.07) | 0.96 | 0.99 (0.91–1.07) | 0.74 |
| Cue to Action Scale | 0.98 (0.86–1.12) | 0.78 | 0.98 (0.84–1.13) | 0.74 |
| Perceived Self-efficacy Scale | 1.01 (0.92–1.10) | 0.91 | 1.01 (0.91–1.11) | 0.89 |
| Perceived importance of real-time counseling supporting HIVST users | ||||
| Very unimportant/unimportant/neutral | 1.0 | 1.0 | ||
| Important /very important | 1.48 (0.95–2.30) | 0.08 | 1.40 (0.88–2.21) | 0.15 |
| Behavioral Intention to take up free HIVST in the coming 6 months | ||||
| Unlikely/neutral | 1.0 | 1.0 | ||
| Likely | 1.67 (1.03–2.72) | 0.04 | 1.60 (0.95–2.69) | 0.08 |
| All (n = 125) | New-Users of HIVST-online (n = 58) | Ever-Users of HIVST-online (n = 67) | p-Value | |
|---|---|---|---|---|
| % | % | % | ||
| Level of satisfaction of different procedures of HIVST-online (% satisfied/very satisfied) | ||||
| Receiving HIVST kits | 92.0 | 89.7 | 94.0 | 0.37 |
| Making appointment of HIVST-online | 96.0 | 98.3 | 94.0 | 0.23 |
| Visual and sound quality of online counseling | 92.8 | 96.6 | 89.6 | 0.13 |
| Clarity of instruction | 96.8 | 98.3 | 95.5 | 0.38 |
| Professionalism of HIVST-administrators | 96.8 | 100.0 | 94.0 | 0.06 |
| Credibility of HIVST-administrators | 96.8 | 98.3 | 95.5 | 0.38 |
| Support from HIVST-online administrators | 92.8 | 96.6 | 89.6 | 0.13 |
| Recommendations made by HIVST-online administrators on reducing high-risk behaviors | 88.8 | 89.7 | 88.1 | 0.99 |
| How helpful is online real-time counseling in the following aspects | ||||
| Understanding your current risk of HIV infection | 85.6 | 82.8 | 88.1 | 0.40 |
| Reducing your fear of HIV testing | 72.0 | 65.5 | 77.6 | 0.13 |
| Preparing you to do HIV testing | 78.4 | 72.2 | 83.6 | 0.13 |
| Mastering the methods and procedures of HIVST | 96.0 | 94.8 | 97.0 | 0.53 |
| Understanding testing results | 97.6 | 98.3 | 97.0 | 0.65 |
| Understanding the concept of window period | 88.8 | 87.9 | 89.6 | 0.77 |
| Acquiring knowledge to prevent HIV infection | 85.6 | 87.9 | 83.6 | 0.49 |
| Reducing high-risk behaviors | 80.0 | 81.0 | 79.1 | 0.79 |
| Behavioral intention to use HIVST-online again | ||||
| Very unlikely/unlikely/neutral | 21.6 | 24.1 | 19.4 | |
| Likely/very likely | 78.4 | 75.9 | 80.6 | 0.52 |
| Behavioral intention to recommend MSM friends to use HIVST-online | ||||
| Very unlikely/unlikely/neutral | 23.2 | 27.6 | 19.4 | |
| Likely/very likely | 76.8 | 72.4 | 80.6 | 0.28 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chan, P.S.-f.; Chidgey, A.; Lau, J.; Ip, M.; Lau, J.T.F.; Wang, Z. Effectiveness of a Novel HIV Self-Testing Service with Online Real-Time Counseling Support (HIVST-Online) in Increasing HIV Testing Rate and Repeated HIV Testing among Men Who Have Sex with Men in Hong Kong: Results of a Pilot Implementation Project. Int. J. Environ. Res. Public Health 2021, 18, 729. https://doi.org/10.3390/ijerph18020729
Chan PS-f, Chidgey A, Lau J, Ip M, Lau JTF, Wang Z. Effectiveness of a Novel HIV Self-Testing Service with Online Real-Time Counseling Support (HIVST-Online) in Increasing HIV Testing Rate and Repeated HIV Testing among Men Who Have Sex with Men in Hong Kong: Results of a Pilot Implementation Project. International Journal of Environmental Research and Public Health. 2021; 18(2):729. https://doi.org/10.3390/ijerph18020729
Chicago/Turabian StyleChan, Paul Shing-fong, Andrew Chidgey, Jason Lau, Mary Ip, Joseph T.F. Lau, and Zixin Wang. 2021. "Effectiveness of a Novel HIV Self-Testing Service with Online Real-Time Counseling Support (HIVST-Online) in Increasing HIV Testing Rate and Repeated HIV Testing among Men Who Have Sex with Men in Hong Kong: Results of a Pilot Implementation Project" International Journal of Environmental Research and Public Health 18, no. 2: 729. https://doi.org/10.3390/ijerph18020729
APA StyleChan, P. S. -f., Chidgey, A., Lau, J., Ip, M., Lau, J. T. F., & Wang, Z. (2021). Effectiveness of a Novel HIV Self-Testing Service with Online Real-Time Counseling Support (HIVST-Online) in Increasing HIV Testing Rate and Repeated HIV Testing among Men Who Have Sex with Men in Hong Kong: Results of a Pilot Implementation Project. International Journal of Environmental Research and Public Health, 18(2), 729. https://doi.org/10.3390/ijerph18020729