
Obstetricians’ Attitude towards Childbirth

 ,
,  ,
, 

Abstract
:1. Introduction
2. Materials and Methods
2.1. The Survey
2.2. Instrument
2.3. Statistical Analysis
3. Results
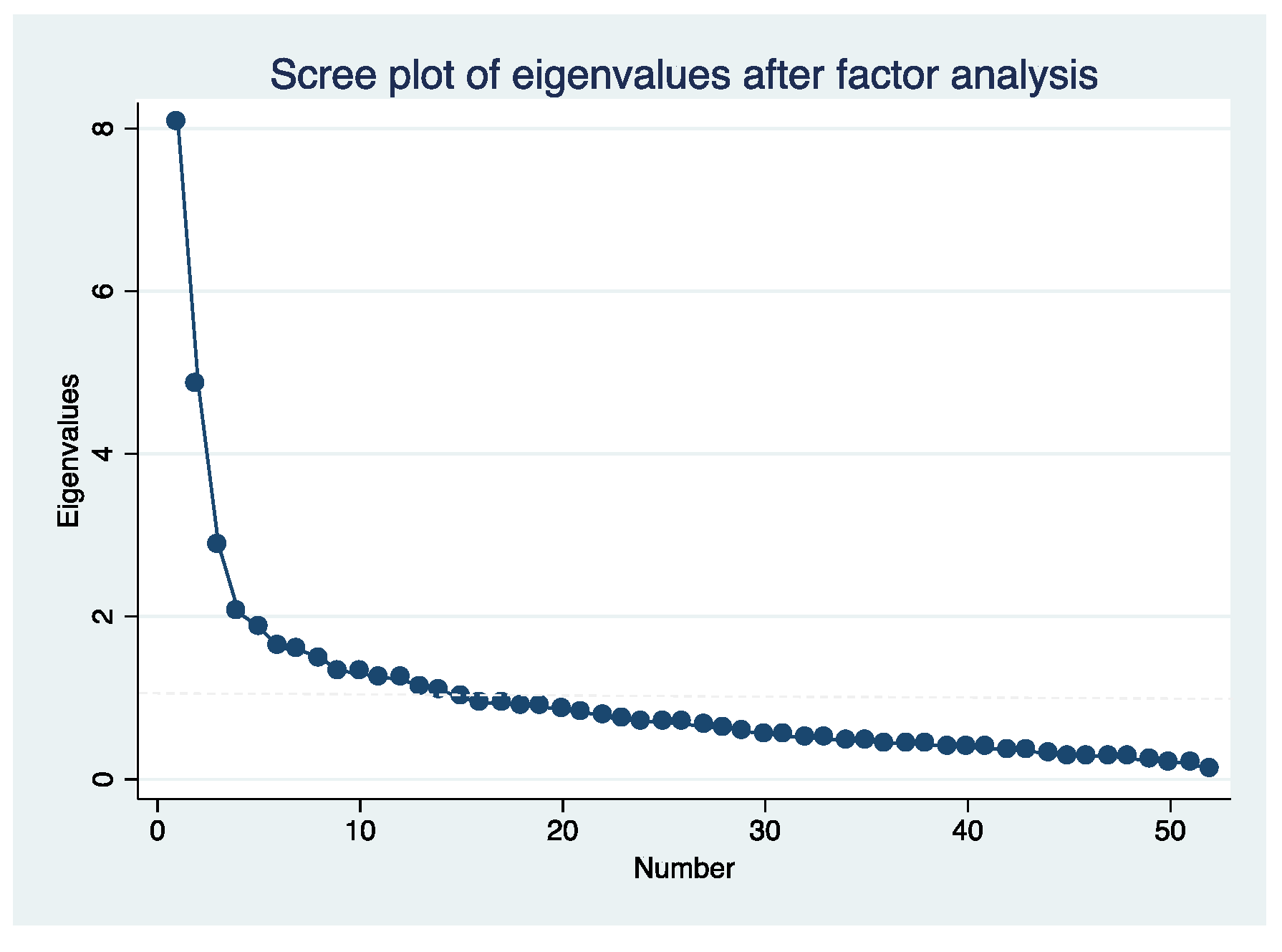
3.1. Exploratory Factor Analysis
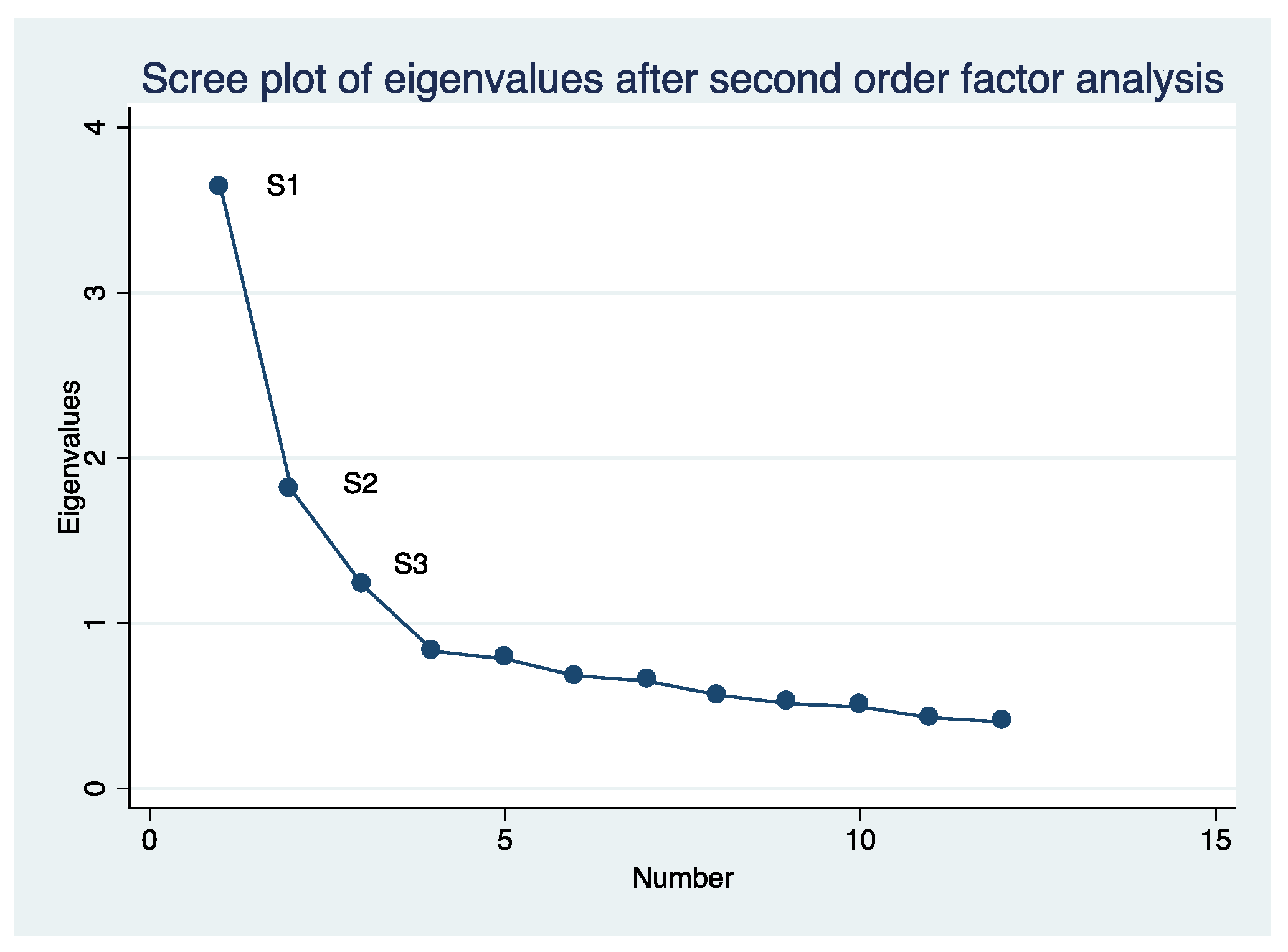
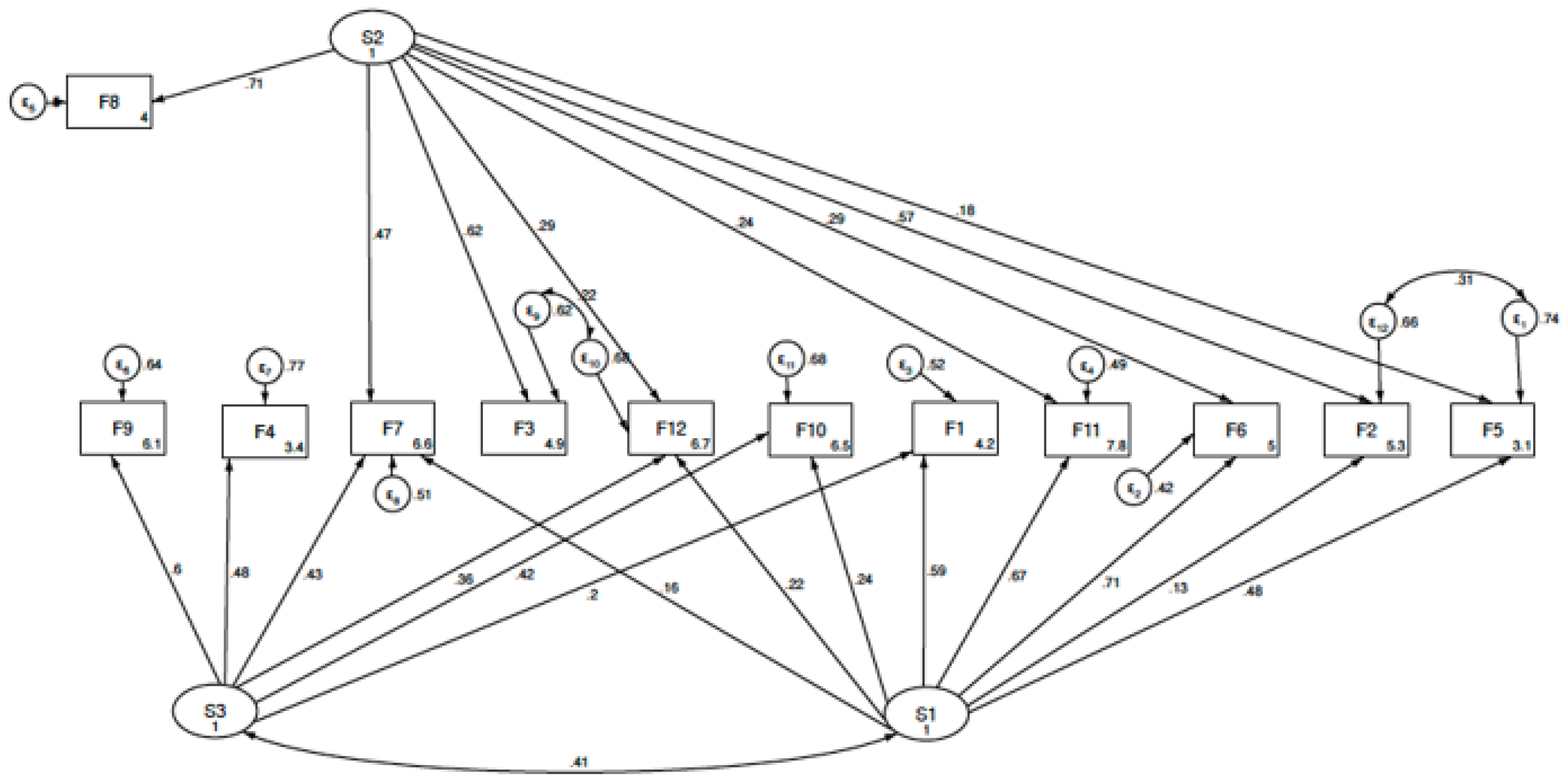
3.2. Confirmatory Analysis
3.3. Scores
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ayers, S.; Wright, D.B.; Thornton, A. Development of a measure of postpartum PTSD: The city birth trauma scale. Front. Psychiatry 2018, 9, 409. [Google Scholar] [CrossRef] [Green Version]
- Ertan, D.; Hingray, C.; Burlacu, E.; Sterlé, A.; El-Hage, W. Post-traumatic stress disorder following childbirth. BMC Psychiatry 2021, 21, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Yildiz, P.D.; Ayers, S.; Phillips, L. The prevalence of posttraumatic stress disorder in pregnancy and after birth: A systematic review and meta-analysis. J. Affect. Disord. 2017, 208, 634–645. [Google Scholar] [CrossRef] [PubMed]
- Grekin, R.; O’Hara, M.W. Prevalence and risk factors of postpartum posttraumatic stress disorder: A meta-analysis. Clin. Psychol. Rev. 2014, 34, 389–401. [Google Scholar] [CrossRef] [PubMed]
- Ayers, S.; Bond, R.; Bertullies, S.; Wijma, K. The aetiology of post-traumatic stress following childbirth: A meta-analysis and theoretical framework. Psychol. Med. 2016, 46, 1121–1134. [Google Scholar] [CrossRef]
- Mazza, M.; Caroppo, E.; Marano, G.; Chieffo, D.; Moccia, L.; Janiri, D.; Rinaldi, L.; Janiri, L.; Sani, G. Caring for mothers: A narrative review on interpersonal violence and peripartum mental health. Int. J. Environ. Res. Public Health 2021, 18, 5281. [Google Scholar] [CrossRef]
- Martín-Arribas, A.; Vila-Candel, R.; O’connell, R.; Dillon, M.; Vila-Bellido, I.; Beneyto, M.Á.; De Molina-Fernández, I.; Rodríguez-Conesa, N.; González-Blázquez, C.; Escuriet, R. Transfers of care between healthcare professionals in obstetric units of different sizes across spain and in a hospital in Ireland: The midconbirth study. Int. J. Environ. Res. Public Health 2020, 17, 8394. [Google Scholar] [CrossRef]
- McKelvin, G.; Thomson, G.; Downe, S. The childbirth experience: A systematic review of predictors and outcomes. Women Birth 2020, 34, 407–416. [Google Scholar] [CrossRef]
- World Health Organization. Intrapartum Care for a Positive Childbirth Experience. 2018. Available online: https://www.ncbi.nlm.nih.gov/books/NBK513809/ (accessed on 10 August 2021).
- Lee, S.; Holden, D.; Webb, R.; Ayers, S. Pregnancy related risk perception in pregnant women, midwives & doctors: A cross-sectional survey. BMC Pregnancy Childbirth 2019, 19, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Possati, A.B.; Prates, L.A.; Cremonese, L.; Scarton, J.; Alves, C.N.; Ressel, L.B. Humanization of childbirth: Meanings and perceptions of nurses. Esc. Anna Nery 2017, 21, 20160366. [Google Scholar] [CrossRef] [Green Version]
- Bretin, H.; Gómez Bueno, C. Amabilidad, Respeto y Dignidad. Hacia la Humanización del Parto y del Nacimiento. Junta de Andalucía: Sevilla, Spain, 2010. Available online: https://digibug.ugr.es/handle/10481/17828 (accessed on 10 August 2021).
- Beltrán-Calvo, C.; Martín-López, J.E.; Solà-Arnau, I.; Aceituno-Velasco, L.; Alomar-Castell, M.; Barona-Vilar, C.; Corona-Páez, I.; Costa-Sampere, D.; Crespo, M.F.; Espiga-López, I.; et al. Guía de práctica clínica de atención en el embarazo y puerperio. Available online: https://www.mscbs.gob.es/organizacion/sns/planCalidadSNS/0Guiaatembarazo.htm (accessed on 10 August 2021).
- Plan de Calidad para el Sistema Nacional de Salud (Espanya); País Basc. Departamento de Sanidad.; Espanya. Ministerio de Ciencia e Innovación.; Espanya. Ministerio de Sanidad y Política Social. Guía de Práctica Clínica Sobre la Atención al Parto Normal: Versión Resumida; Eusko Jaurlaritzaren Argitalpen Zerbitzu Nagusia, Servicio Central de Publicaciones del Gobierno Vasco: Madrid, Spain, 2010; ISBN 9788445730904. [Google Scholar]
- Fernández, F.; Vera Ferrer, L.T.; Mercedes Novo, M.; Rodríguez Gómez, J.; Aguirre Jaime, A. El empoderamiento de la gestante y su satisfacción durante el parto. Dilemata 2018, 26, 207–215. [Google Scholar]
- United Nations. Committee on the Elimination of Discrimination against Women Seventy-fifth Session Decision Adopted by the Committee under Article 4 (2) (c) of the Optional Protocol, Concerning Communication No. 138/2018; United Nations: New York, NY, USA, 2020. [Google Scholar]
- González-Mesa, E.; Rengel-Díaz, C.; Riklikiene, O.; Thomson, G.; Cazorla-Granados, O.; Abreu, W.; Morgado-Neves, D.; Isbir, G.G.; Jonsdottir, S.S.; Karlsdóttir, S.I.; et al. Assessment of the attitude towards childbirth in health sciences students-development and validation of the questionnaire Cave-St. Curr. Psychol. 2021, 1–10. [Google Scholar] [CrossRef]
- González-Mesa, E.; Cazorla-Granados, O.; Blasco-Alonso, M.; Sabonet, L.; Jiménez-López, J.S.; Rengel-Díaz, C. Educating future professionals in perinatal medicine: The attitude of medical and nursing students towards childbirth. J. Perinat. Med. 2021, 49, 485–495. [Google Scholar] [CrossRef] [PubMed]
- Gustafsson, J.E.; Balke, G. General and specific abilities as predictors of school achievement. Multivariate Behav. Res. 1993, 28, 407–434. [Google Scholar] [CrossRef] [PubMed]
- Bentler, P.M. Comparative fit indexes in structural models. Psychol. Bull. 1990, 107, 238–246. [Google Scholar] [CrossRef]
- Hu, L.T.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Dumit, J. Illnesses you have to fight to get: Facts as forces in uncertain, emergent illnesses. In Proceedings of the Social Science and Medicine. Soc. Sci. Med. 2006, 62, 577–590. [Google Scholar] [CrossRef] [PubMed]
- Werner, A.; Malterud, K. It is hard work behaving as a credible patient: Encounters between women with chronic pain and their doctors. Soc. Sci. Med. 2003, 57, 1409–1419. [Google Scholar] [CrossRef] [Green Version]
- Greenhalgh, T.; Snow, R.; Ryan, S.; Rees, S.; Salisbury, H. Six “biases” against patients and carers in evidence-based medicine. BMC Med. 2015, 13, 200. [Google Scholar] [CrossRef] [Green Version]
- Sheen, K.; Spiby, H.; Slade, P. Exposure to traumatic perinatal experiences and posttraumatic stress symptoms in midwives: Prevalence and association with burnout. Int. J. Nurs. Stud. 2015, 52, 578–587. [Google Scholar] [CrossRef]
- Fuglenes, D.; Øian, P.; Kristiansen, I.S. Obstetricians’ choice of cesarean delivery in ambiguous cases: Is it influenced by risk attitude or fear of complaints and litigation? Am. J. Obstet. Gynecol. 2009, 200, 48.e1–48.e8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Slade, P.; Balling, K.; Sheen, K.; Goodfellow, L.; Rymer, J.; Spiby, H.; Weeks, A. Work-related post-traumatic stress symptoms in obstetricians and gynaecologists: Findings from INDIGO, a mixed-methods study with a cross-sectional survey and in-depth interviews. BJOG An. Int. J. Obstet. Gynaecol. 2020, 127, 600–608. [Google Scholar] [CrossRef] [PubMed]
- Pintado-Cucarella, S.; Penagos-Corzo, J.C.; Casas-Arellano, M.A. Burnout syndrome in medical and obstetric perception of violence [Síndrome de desgaste profesional en médicos y percepción de la violencia obstétrica]. Ginecol. Obstet. Mex. 2015, 83, 173–178. [Google Scholar]
- Olza Fernández, I.; Fernández, I.O.; Olza Fernández, I. PTSD and obstetric violence. Midwifery Today Int. Midwife 2013, 105, 48–49. [Google Scholar]
- Koster, D.; Romijn, C.; Sakko, E.; Stam, C.; Steenhuis, N.; de Vries, D.; van Willigen, I.; Fontein-Kuipers, Y. Traumatic childbirth experiences: Practice-based implications for maternity care professionals from the woman’s perspective. Scand. J. Caring Sci. 2020, 34, 792–799. [Google Scholar] [CrossRef]
- Abenhaim, H.A.; Benjamin, A.; Koby, R.D.; Kinch, R.A.; Kramer, M.S. Comparison of obstetric outcomes between on-call and patients’ own obstetricians. CMAJ 2007, 177, 352–356. [Google Scholar] [CrossRef] [Green Version]
- Fontein-Kuipers, Y.; Koster, D.; Romijn, C.; Sakko, E.; Stam, C.; Steenhuis, N.; de Vries, D.; van Willigen, I. I-POEMS Listening to the voices of women with a traumatic birth experience. J. Psychol. Cogn. 2018, 3, 29–36. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| N (%) | |
|---|---|
| Age | |
| <35 years | 104 (29.4) |
| 35–50 years | 128 (36.2) |
| >50 years | 122 (34.5) |
| Gender | |
| Male | 94 (26.6) |
| Female | 260 (73.4) |
| Children | |
| No | 105(29.7) |
| Yes | 249 (70.3) |
| Practice | |
| Private | 75 (21.2) |
| Public | 181 (51.1) |
| Both | 98 (27.7) |
| Community | |
| Andalucía | 81 (22.9) |
| Aragón | 16 (4.5) |
| Canarias | 15 (4.2) |
| Cantabria | 2 (0.6) |
| Castilla y León | 12 (3.4) |
| Castilla-La Mancha | 16 (4.5) |
| Cataluña | 47 (13.3) |
| Comunidad de Madrid | 59 (16.7) |
| Comunidad Valenciana | 25 (7.1) |
| Extremadura | 12 (3.4) |
| Galicia | 25 (7.1) |
| Islas Baleares | 9 (2.5) |
| La Rioja | 1 (0.3) |
| Navarra | 5 (1.4) |
| País Vasco | 17 (4.8) |
| Principado de Asturias | 4 (1.1) |
| Región de Murcia | 8 (2.3) |
| F1 | F2 | F3 | F4 | F5 | F6 | F7 | F8 | F9 | F10 | F11 | F12 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| It 11 0.768 | It 31 0.565 | It 37 0.823 | It 1 0.845 | It 5 0.366 | It 24 0.429 | It 19 0.553 | It 40 0.772 | It 6 0.679 | It 10 0.480 | It 9 0.350 | It 18 0.551 |
| It 12 0.812 | It 32 0.701 | It 38 0.847 | It 2 0.830 | It 28 0.792 | It 25 0.427 | It 22 0.803 | It 41 0.691 | It 7 0.598 | It 15 0.666 | It 51 0.710 | It 36 0.384 |
| It 13 0.738 | It 33 0.825 | It 39 0.764 | It 3 0.663 | It 29 0.780 | It 26 0.715 | It 23 0.796 | It 42 0.483 | It 8 0.552 | It 47 0.582 | It 52 0.701 | It 45 0.662 |
| It 14 0.668 | It 34 0.582 | It 30 0.469 | It 27 0.739 | It 43 0.481 | It 48 0.423 | It 4 0.343 | |||||
| It 50 0.468 | It 35 0.747 | It 44 0.576 | It 49 0.719 | ||||||||
| It 16 0.448 | It 20 0.653 | ||||||||||
| It 17 0.446 | It 21 0.630 | ||||||||||
| It 46 0.401 |
| F1 | F2 | F3 | F4 | F5 | F6 | F7 | F8 | F9 | F10 | F11 | F12 | |
| F1 | 1.00 | |||||||||||
| F2 | 0.100 | 1.00 | ||||||||||
| F3 | 0.052 | 0.348 | 1.00 | |||||||||
| F4 | 0.218 | 0.032 | 0.028 | 1.00 | ||||||||
| F5 | 0.343 ** | 0.327 ** | 0.066 | 0.037 | 1.00 | |||||||
| F6 | 0.452 ** | 0.233 ** | 0.164 ** | 0.170 ** | 0.372 ** | 1.000 | ||||||
| F7 | 0.307 ** | 0.308 ** | 0.336 ** | 0.266 ** | 0.224 ** | 0.402 ** | 1.000 | |||||
| F8 | 0.066 | 0.399** | 0.431 ** | 0.009 | 0.100 | 0.198 ** | 0.320 ** | 1.000 | ||||
| F9 | 0.267 ** | 0.035 | 0.004 | 0.254 ** | 0.173 ** | 0.197 ** | 0.295 ** | 0.051 | 1.000 | |||
| F10 | 0.380 ** | 0.096 | 0.051 | 0.295 ** | 0.204 ** | 0.315 ** | 0.315 ** | 0.027 | 0.338 ** | 1.000 | ||
| F11 | 0.459 ** | 0.233 ** | 0.151 ** | 0.141 ** | 0.347 ** | 0.534 ** | 0.374 ** | 0.190 ** | 0.191 ** | 0.298 ** | 1.000 | |
| F12 | 0.234 ** | 0.203 ** | 0.314 ** | 0.231 ** | 0.204 ** | 0.330 ** | 0.389 ** | 0.179 ** | 0.303 ** | 0.265 ** | 0.274 ** | 1.000 |
| S1 Empathy | S2 BRT Risk Management | S3 Obstetric Performance |
|---|---|---|
| F1 | F2 | F4 |
| 0.713 | 0.635 | 0.698 |
| F5 | F3 | F9 |
| 0.717 | 0.801 | 0.706 |
| F6 | F7 | F10 |
| 0.719 | 0.482 | 0.570 |
| F11 | F8 | F12 |
| 0.723 | 0.770 | 0.509 |
| Chi-Square | df | RMSEA | CFI | AIC | BIC | SRMR | CD | |
|---|---|---|---|---|---|---|---|---|
| Model 1 (four factors) | 338.10 | 71 | 0.10 (0.09–0.11) | 0.80 | 21,868.0 | 22,053.82 | 0.11 | 0.98 |
| Model 2 (three factors) | 370.42 | 41 | 0.00 (0.00–0.03) | 1.00 | 204,520.9 | 206,420.58 | 0.02 | 0.97 |
| Scale | 25 th Percentile | 50 th Percentile | 75 th Percentile | Scale Rank | Mean | Std. Deviation | Scores Rank | Minimum | Maximum |
|---|---|---|---|---|---|---|---|---|---|
| CAVE | 183 | 196 | 211 | (52–260) | 193.21 | 21.19 | (52–260) | 119.00 | 260.00 |
| F1 | 24 | 29 | 34 | (8–40) | 28.64 | 6.81 | (8–40) | 8.00 | 40.00 |
| F2 | 18 | 20 | 22 | (5–25) | 19.44 | 3.66 | (5–25) | 5.00 | 25.00 |
| F3 | 10 | 12 | 14 | (3–15) | 11.79 | 2.42 | (3–15) | 3.00 | 15.00 |
| F4 | 8 | 10 | 12 | (3–15) | 9.84 | 2.88 | (3–15) | 3.00 | 15.00 |
| F5 | 7 | 9 | 11 | (4–20) | 9.39 | 3.07 | (4–20) | 4.00 | 20.00 |
| F6 | 13 | 15 | 18 | (4–20) | 15.14 | 3.03 | (4–20) | 4.00 | 20.00 |
| F7 | 19 | 22 | 23 | (5–25) | 20.96 | 3.19 | (5–25) | 7.00 | 25.00 |
| F8 | 9 | 11 | 12 | (3–15) | 10.50 | 2.60 | (3–15) | 3.00 | 15.00 |
| F9 | 12 | 14 | 15 | (3–15) | 12.95 | 2.11 | (3–15) | 3.00 | 15.00 |
| F10 | 16 | 18 | 20 | (4–20) | 17.31 | 2.67 | (4–20) | 7.00 | 20.00 |
| F11 | 26 | 29 | 31 | (7–35) | 28.55 | 3.68 | (7–35) | 12.00 | 35.00 |
| F12 | 11 | 12 | 13 | (3–15) | 11.93 | 1.77 | (3–15) | 5.00 | 15.00 |
| Second order factors | |||||||||
| S1 | 71 | 89 | 87 | (23–115) | 78.47 | 12.23 | (23–115) | 34.00 | 110.00 |
| S2 | 57 | 63 | 69 | (16–80) | 62.69 | 8.54 | (16–80) | 34.00 | 80.00 |
| S3 | 48 | 53 | 57 | (13–65) | 52.04 | 6.38 | (13–65) | 31.00 | 65.00 |
| CAVE | F1 | F2 | F3 | F4 | F5 | F6 | F7 | F8 | F9 | F10 | F11 | F12 | S1 | S2 | S3 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Practice | ||||||||||||||||
| Private | 200.52 | 28.04 | 19.40 | 11.10 | 9.08 | 8.97 | 14.86 | 19.92 | 10.20 | 12.49 | 16.17 | 28.41 | 11.56 | 77.10 | 60.62 | 49.30 |
| Public | 193.76 | 29.43 | 19.55 | 12.17 | 10.17 | 9.51 | 15.29 | 21.49 | 10.62 | 13.24 | 18.09 | 28.73 | 12.17 | 79.74 | 63.85 | 53.68 |
| Both | 196.47 | 27.63 | 19.25 | 11.62 | 9.81 | 9.48 | 15.06 | 20.77 | 10.48 | 12.75 | 16.75 | 28.31 | 11.79 | 77.18 | 62.14 | 51.12 |
| F value | 7.64 | 2.61 | 0.22 | 5.64 | 3.84 | 0.88 | 0.58 | 6.88 | 0.72 | 4.04 | 18.35 | 0.47 | 3.61 | 1.99 | 4.14 | 14.98 |
| p | p ≤ 0.001 | NS | NS | p ≤ 0.004 | p ≤ 0.022 | NS | NS | p ≤ 0.001 | NS | p ≤ 0.018 | p ≤ 0.001 | NS | p ≤ 0.028 | NS | p ≤ 0.017 | p ≤ 0.001 |
| Age | ||||||||||||||||
| <35 years | 28.75 | 28.75 | 20.06 | 12.27 | 11.14 | 9.53 | 15.77 | 22.30 | 10.79 | 13.19 | 18.09 | 28.94 | 12.47 | 79.44 | 65.45 | 65.45 |
| 35–50 years | 28.35 | 28.35 | 19.73 | 11.90 | 9.95 | 9.50 | 15.00 | 21.25 | 10.37 | 13.15 | 17.50 | 28.26 | 11.92 | 78.05 | 63.27 | 63.27 |
| >50 years | 28.84 | 28.84 | 18.59 | 11.27 | 8.61 | 9.14 | 14.74 | 19.50 | 10.37 | 12.53 | 16.45 | 28.51 | 11.50 | 78.09 | 59.74 | 59.74 |
| F value | 11.70 | 0.83 | 5.26 | 5.16 | 24.50 | 0.59 | 3.53 | 25.70 | 0.96 | 3.72 | 11.80 | 0.97 | 8.74 | 0.45 | 13.90 | 27.30 |
| p | p ≤ 0.001 | NS | p ≤ 0.006 | p ≤ 0.006 | p ≤ 0.001 | NS | p ≤ 0.03 | p ≤ 0.001 | NS | p ≤ 0.025 | p ≤ 0.001 | NS | p ≤ 0.001 | NS | p ≤ 0.001 | p ≤ 0.001 |
| Gender | ||||||||||||||||
| Male | 28.10 | 28.10 | 19.11 | 11.51 | 8.77 | 9.56 | 14.60 | 20.00 | 10.76 | 12.61 | 16.39 | 28.25 | 77.40 | 77.40 | 61.39 | 49.17 |
| Female | 28.83 | 28.83 | 19.55 | 11.90 | 10.22 | 9.33 | 15.33 | 21.30 | 10.40 | 13.07 | 17.65 | 28.65 | 78.86 | 78.86 | 63.16 | 53.08 |
| t value | −2.89 | −0.88 | −0.99 | −1.48 | −4.27 | 0.63 | −2.00 | −3.45 | 1.15 | −1.79 | −3.57 | −0.90 | −3.58 | −0.99 | −1.73 | −5.28 |
| p | p ≤ 0.004 | NS | NS | NS | p ≤ 0.001 | NS | p ≤ 0.046 | p ≤ 0.001 | NS | NS | p ≤ 0.001 | NS | p ≤ 0.001 | NS | NS | p ≤ 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
González-Mesa, E.; Jiménez-López, J.; Blasco-Alonso, M.; Lubián-López, D. Obstetricians’ Attitude towards Childbirth. Int. J. Environ. Res. Public Health 2021, 18, 10650. https://doi.org/10.3390/ijerph182010650
González-Mesa E, Jiménez-López J, Blasco-Alonso M, Lubián-López D. Obstetricians’ Attitude towards Childbirth. International Journal of Environmental Research and Public Health. 2021; 18(20):10650. https://doi.org/10.3390/ijerph182010650
Chicago/Turabian StyleGonzález-Mesa, Ernesto, Jesús Jiménez-López, Marta Blasco-Alonso, and Daniel Lubián-López. 2021. "Obstetricians’ Attitude towards Childbirth" International Journal of Environmental Research and Public Health 18, no. 20: 10650. https://doi.org/10.3390/ijerph182010650
APA StyleGonzález-Mesa, E., Jiménez-López, J., Blasco-Alonso, M., & Lubián-López, D. (2021). Obstetricians’ Attitude towards Childbirth. International Journal of Environmental Research and Public Health, 18(20), 10650. https://doi.org/10.3390/ijerph182010650