
“Nobody Listened”. Mothers’ Experiences and Needs Regarding Professional Support Prior to Their Admission to an Infant Mental Health Day Clinic

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Participants and Recruitment
2.3. Ethics Statement
2.4. Data Collection
2.5. Data Analysis
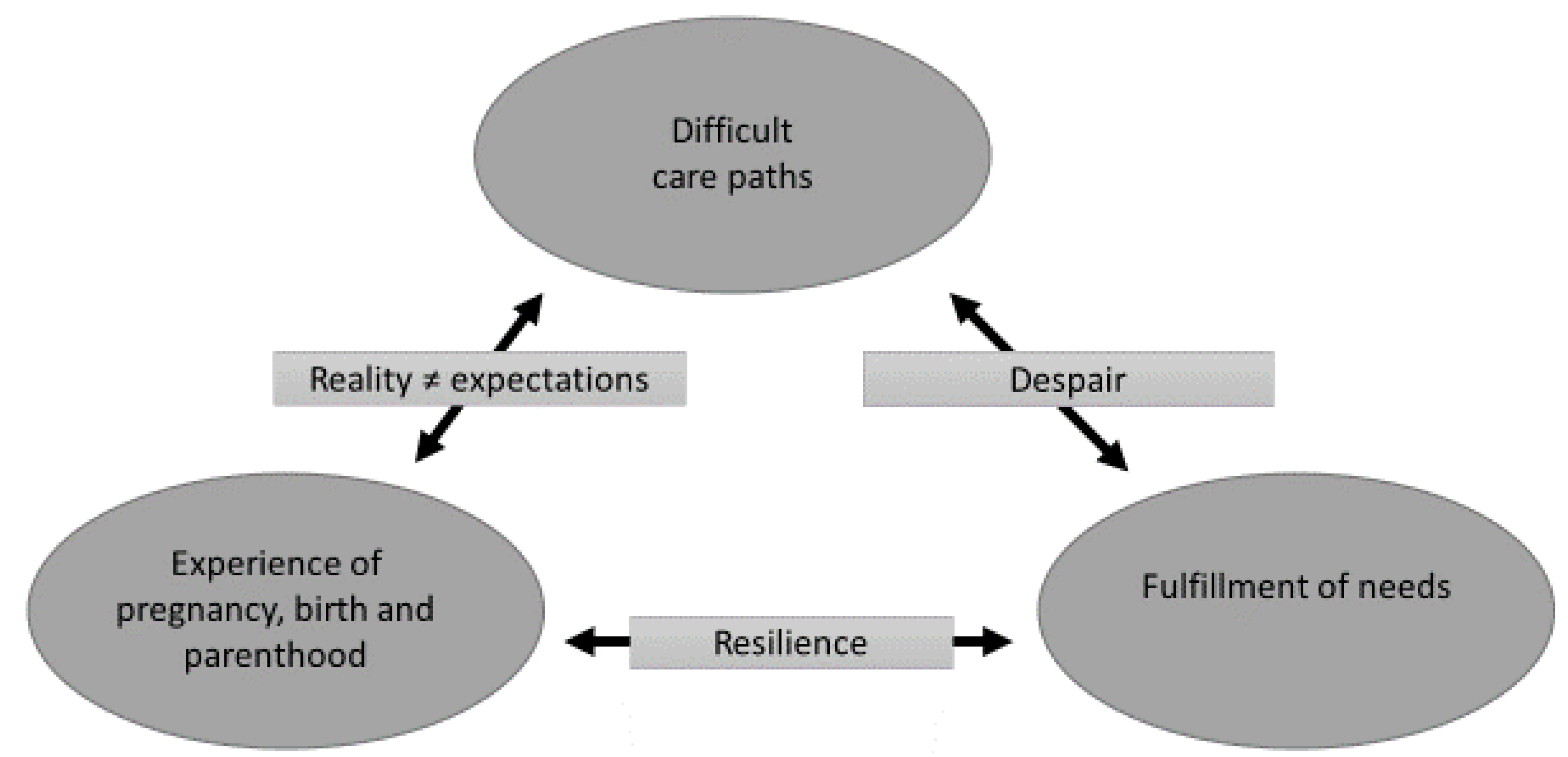
3. Results
3.1. Experiences of Pregnancy, Birth and Parenthood, and Difficult Care Paths
“I have always thought that I’m going to have a child and nature will prepare you for it’.”—M10
“If you read in magazines: people give birth and it’s a ‘pink cloud’ and everything goes well and ‘we are so happy with our baby’.”—M10
“I was convinced that someone who has had a difficult time as a child is well suited to do better for another child because you have more insight into the damage that this causes for a child. And I wish, yes, I wanted to show that I might be able to do it better.”—M7
“And yes, then it just went downhill but I didn’t show it.”—M6
“But I always pretended to be fine when they (cfr. midwife and maternity nurse) came to visit, so maybe this might be my own mistake because: you have your pride, it is your first child. You don’t want to admit that it’s actually not fine.”—M9
“…and I never lied about my story. Because there are a lot of people who pretend to the world that it’s all a bed of roses, but I never did that.”—M12
“I saw on TV a mother being interviewed in the news, and she was talking about [infant mental health facility] […] and then I looked it up on the internet, I contacted them and that’s how I got an intake”—M2
“It was very threatening in the beginning. It’s baby psychiatry, that’s a big word. In our environment, everyone said: ‘a baby to a psychiatrist? What will they do? Chat with it?’.”—M3
“And then I said, with tears in my eyes: ‘here it ends, this doesn’t work. I cannot afford that (cfr. psychotherapy)’.”—M1
3.2. Experiences of Pregnancy, Birth and Parenthood; and Fulfillment of Needs
“The lack of sleep, that was the biggest trigger for me. That completely undermined my resilience.”—M5
“I screamed for help but no one, no one heard me, no one really listened.”—M12
“I felt completely, well, very little supported by my partner. Uhm, we’ve almost stopped talking to each other.”—M13
“I really felt completely isolated from the world, I felt completely misunderstood.”—M6
“Yes, I have noticed that I had a lot of support just by chatting with other moms, who also experienced similar situations (…)”—M11
“When I was admitted (cfr. to a crisis psychiatric ward), I really had the feeling ‘I don’t want that child, I really don’t. I, I would prefer to give him up for adoption (…)’”—M10
“That [crf. baby dancing] was one of the few moments that we really enjoyed each other. (…) Because it was so intense to feel that connection with him. I really needed that to feel like ‘oh, it’s there. It is just very difficult between us for a while, but it is there’.”—M6
“We just got a lot of information at the infant mental health facility, that was something to hold on to and an explanation for certain situations”—M1
“Yes, the negative spiral of ‘I’m a bad mother … and there is no reason for me to carry on like this’. That really was my attitude.”—M10
“I have always had the feeling that the infant mental health facility provided a safety net after our discharge.”—M6
3.3. Difficult Care Paths and Fulfillment of Needs
“But [sighs] most doctors always stay above you (…).”—M5
“I felt like the worst mother ever because what kind of mother can’t comfort her own child?”—M9
“Uhm, but I lost myself in my job…”—M6
“I only encountered a lack of understanding in the medical world and that frustrates me the most …”—M11
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nyström, K.; Öhrling, K. Parenthood experiences during the child’s first year: Literature review. J. Adv. Nurs. 2004, 46, 319–330. [Google Scholar] [CrossRef]
- Barimani, M.; Vikstrom, A.; Rosander, M.; Forslund Frykedal, K.; Berlin, A. Facilitating and inhibiting factors in transition to parenthood—Ways in which health professionals can support parents. Scand. J. Caring. Sci. 2017, 31, 537–546. [Google Scholar] [CrossRef] [PubMed]
- Widarsson, M.; Kerstis, B.; Sundquist, K.; Engstrom, G.; Sarkadi, A. Support needs of expectant mothers and fathers: A qualitative study. J. Perinat. Educ. 2012, 21, 36–44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seefat-van Teeffelen, A.; Nieuwenhuijze, M.; Korstjens, I. Women want proactive psychosocial support from midwives during transition to motherhood: A qualitative study. Midwifery 2011, 27, e122–e127. [Google Scholar] [CrossRef] [PubMed]
- Viveiros, C.J.; Darling, E.K. Perceptions of barriers to accessing perinatal mental health care in midwifery: A scoping review. Midwifery 2019, 70, 106–118. [Google Scholar] [CrossRef] [PubMed]
- Nagle, U.; Farrelly, M. Women’s views and experiences of having their mental health needs considered in the perinatal period. Midwifery 2018, 66, 79–87. [Google Scholar] [CrossRef] [PubMed]
- Blount, A.J.; Adams, C.R.; Anderson-Berry, A.L.; Hanson, C.; Schneider, K.; Pendyala, G. Biopsychosocial Factors during the Perinatal Period: Risks, Preventative Factors, and Implications for Healthcare Professionals. Int. J. Environ. Res. Public Health 2021, 18, 8206. [Google Scholar] [CrossRef]
- Lancet, T. Women’s voices: Speaking up about perinatal mental health. Lancet 2017, 389, 882. [Google Scholar] [CrossRef] [Green Version]
- Russell, K.; Ashley, A.; Chan, G.; Gibson, S.; Jones, R. Maternal Mental Health—Women’s Voices; Royal College of Obstetricians and Gynaecologists: London, UK, 2017; p. 42. [Google Scholar]
- Tripathy, P. A public health approach to perinatal mental health: Improving health and wellbeing of mothers and babies. J. Gynecol. Obstet. Hum. Reprod. 2020, 49, 101747. [Google Scholar] [CrossRef]
- Zeanah, P.D.; Nagle, G.A.; Stafford, B.S.; Rice, T.; Farrer, J. Addressing Social-Emotional Development and Infant Mental Health in Early Childhood Systems; Executive Summary; Halfon, N., Rice, T., Inkelas, M., Eds.; Building State Early Childhood Comprehensive Systems Series; No 12. National Center for Infant and Early Childhood Health Policy: Los Angeles, CA, USA, 2004; p. 56. [Google Scholar]
- Lyons-Ruth, K.; Todd Manly, J.; Von Klitzing, K.; Tamminen, T.; Emde, R.; Fitzgerald, H.; Paul, C.; Keren, M.; Berg, A.; Foley, M.; et al. The Worldwide Burden of Infant Mental and Emotional Disorder: Report of the Task Force of the World Association for Infant Mental Health. Infant Ment. Health J. 2017, 38, 695–705. [Google Scholar] [CrossRef] [Green Version]
- Morawska, A.; Dittman, C.K.; Rusby, J.C. Promoting Self-Regulation in Young Children: The Role of Parenting Interventions. Clin. Child Fam. Psychol. Rev. 2019, 22, 43–51. [Google Scholar] [CrossRef] [PubMed]
- Cook, F.; Giallo, R.; Hiscock, H.; Mensah, F.; Sanchez, K.; Reilly, S. Infant Regulation and Child Mental Health Concerns: A Longitudinal Study. Pediatrics 2019, 143, e20180977. [Google Scholar] [CrossRef] [Green Version]
- Nolvi, S.; Karlsson, L.; Bridgett, D.J.; Pajulo, M.; Tolvanen, M.; Karlsson, H. Maternal postnatal psychiatric symptoms and infant temperament affect early mother-infant bonding. Infant Behav. Dev. 2016, 43, 13–23. [Google Scholar] [CrossRef]
- Barker, D.J. The origins of the developmental origins theory. J. Intern. Med. 2007, 261, 412–417. [Google Scholar] [CrossRef]
- Van den Bergh, B.R. Developmental programming of early brain and behaviour development and mental health: A conceptual framework. Dev. Med. Child Neurol. 2011, 53 (Suppl. 4), 19–23. [Google Scholar] [CrossRef] [Green Version]
- Zero to Three Infant Mental Health Task Force Steering, C. Definition of Infant Mental Health. Available online: https://www.zerotothree.org/early-development/infant-and-early-childhood-mental-health (accessed on 12 October 2021).
- Biel, M.G.; Tang, M.H.; Zuckerman, B. Pediatric Mental Health Care Must Be Family Mental Health Care. JAMA Pediatr. 2020, 174, 519–520. [Google Scholar] [CrossRef]
- Scope, A.; Booth, A.; Morrell, C.J.; Sutcliffe, P.; Cantrell, A. Perceptions and experiences of interventions to prevent postnatal depression. A systematic review and qualitative evidence synthesis. J. Affect. Disord. 2017, 210, 100–110. [Google Scholar] [CrossRef]
- Myors, K.A.; Schmied, V.; Johnson, M.; Cleary, M. ‘My special time’: Australian women’s experiences of accessing a specialist perinatal and infant mental health service. Health Soc. Care Community 2014, 22, 268–277. [Google Scholar] [CrossRef]
- Coates, D.; Davis, E.; Campbell, L. The experiences of women who have accessed a perinatal and infant mental health service: A qualitative investigation. Adv. Ment. Health 2017, 15, 88–100. [Google Scholar] [CrossRef]
- National Collaborating Centre for Mental Health (UK). Service User Experience in Adult Mental Health: Improving the Experience of Care for People Using Adult NHS Mental Health Services; British Psychological Society: Leicester, UK, 2012; p. 32. [Google Scholar] [PubMed]
- Dierckx de Casterle, B.; Gastmans, C.; Bryon, E.; Denier, Y. QUAGOL: A guide for qualitative data analysis. Int. J. Nurs Stud. 2012, 49, 360–371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, B.S.K.; Danckaerts, M.; Van den Bergh, B.R.H. Helping Families of Infants with Persistent Crying and Sleep Problems in a Day-Clinic. Front. Psychiatry 2021, 12, 591389. [Google Scholar] [CrossRef]
- Dierckx de Casterle, B.; De Vliegher, K.; Gastmans, C.; Mertens, E. Complex Qualitative Data Analysis: Lessons Learned From the Experiences with the Qualitative Analysis Guide of Leuven. Qual. Health Res. 2021, 31, 1083–1093. [Google Scholar] [CrossRef]
- Ritchie, J.; Lewis, J.; Elam, G.; Tennant, R.; Rahim, N. Designing and selecting samples. In Qualitative Research Practice; Ritchie, J., Lewis, J., McNaughton-Nicholls, C., Ormston, R., Eds.; Sage: London, UK, 2014. [Google Scholar]
- Young, C.; Ayers, S. Risk and Resilience in Pregnancy and Birth. In Multisystemic Resilience: Adaptation and Transformation in Contexts of Change; Ungar, M., Ed.; Oxford University Press: New York, NY, USA, 2021; pp. 57–78. [Google Scholar]
- Van Haeken, S.; Braeken, M.; Nuyts, T.; Franck, E.; Timmermans, O.; Bogaerts, A. Perinatal Resilience for the First 1000 Days of Life. Concept Analysis and Delphi Survey. Front. Psychol. 2020, 11, 563432. [Google Scholar] [CrossRef] [PubMed]
- Jones, C.C.G.; Jomeen, J.; Hayter, M. The impact of peer support in the context of perinatal mental illness: A meta-ethnography. Midwifery 2014, 30, 491–498. [Google Scholar] [CrossRef] [PubMed]
- Russell, C.C. The State of Knowledge about Prevention/Early Intervention; Invest in Kids: Toronto, ON, Canada, 2002; p. 382. [Google Scholar]
- Mihelic, M.; Filus, A.; Morawaska, A. Correlates of Prenatal Parenting Expectations in new Mothers: Is Better Self-Efficacy a Potential Target for Preventing Postnatal Adjustment Difficulties? Prev. Sci. 2016, 17, 949–959. [Google Scholar] [CrossRef] [PubMed]
- Bayrampour, H.; Hapsari, A.P.; Pavlovic, J. Barriers to addressing perinatal mental health issues in midwifery settings. Midwifery 2018, 59, 47–58. [Google Scholar] [CrossRef] [PubMed]
- Ford, E.; Lee, S.; Shakespeare, J.; Ayers, S. Diagnosis and management of perinatal depression and anxiety in general practice: A meta-synthesis of qualitative studies. Br. J. Gen. Pract. 2017, 67, e538–e546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldin Evans, M.; Phillippi, S.; Gee, R.E. Examining the Screening Practices of Physicians for Postpartum Depression: Implications for Improving Health Outcomes. Women’s Health Issues 2015, 25, 703–710. [Google Scholar] [CrossRef] [PubMed]
- Zuckerman, B.; Wong, S.L. Family history: An opportunity to disrupt transmission of behavioral health problems. Pediatrics 2019, 143, e20183383. [Google Scholar] [CrossRef]
- Fowles, E.R.; Cheng, H.R.; Mills, S. Postpartum health promotion interventions: A systematic review. Nurs. Res. 2012, 61, 269–282. [Google Scholar] [CrossRef] [PubMed]
- Noonan, M.; Jomeen, J.; Galvin, R.; Doody, O. Survey of midwives’ perinatal mental health knowledge, confidence, attitudes and learning needs. Women Birth 2018, 31, e358–e366. [Google Scholar] [CrossRef]
- Hasson-Ohayon, I.; Malka, T.; Goldzweig, G.; Roe, D. The interaction between sense of mastery, social support, and parental distress among mothers with and without serious mental illness. Compr. Psychiatry 2018, 87, 59–63. [Google Scholar] [CrossRef]
- Biaggi, A.; Conroy, S.; Pawlby, S.; Pariante, C.M. Identifying the women at risk of antenatal anxiety and depression: A systematic review. J. Affect Disord. 2016, 191, 62–77. [Google Scholar] [CrossRef] [Green Version]
- Tsai, Y.J.; Hsu, Y.Y.; Hou, T.W.; Chang, C.H. Effects of a Web-Based Antenatal Care System on Maternal Stress and Self-Efficacy During Pregnancy: A Study in Taiwan. J. Midwifery Womens Health 2018, 63, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Ginja, S.; Coad, J.; Bailey, E.; Kendall, S.; Goodenough, T.; Nightingale, S.; Smiddy, J.; Day, C.; Deave, T.; Lingam, R. Associations between social support, mental wellbeing, self-efficacy and technology use in first-time antenatal women: Data from the BaBBLeS cohort study. BMC Pregnancy Childbirth 2018, 18, 441. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Questions About Experiences and Needs Regarding Professional Support |
|---|
| Can you tell me something about yourself and your family? |
| Can you tell me something about the time before you were admitted to the IMH day clinic? How did you experience this period? How did you experience admission at the IMH day clinic? What did the admission do to you? After you and your child were discharged from the IMH day clinic, how did you experience this period (focus is up to 2 years after pregnancy)? What does perinatal resilience mean to you? |
| Characteristics | Mothers (N = 13) | Fathers 1 (N = 11) |
|---|---|---|
| Ethnicity (n) | ||
| Caucasian | 13 | 11 |
| Mean age, in years (SD) * | 33.6 (4.3) | 34.3 (2.8) |
| Education level (n) | ||
| Until 18 years | 2 | 6 |
| Bachelor/Master degree | 11 | 5 |
| Employment * (n) | ||
| Employed | 8 | 11 |
| On sick/maternity leave | 5 | 0 |
| Student | 1 | 0 |
| Parity at admission (n) | ||
| Primiparous | 8 | |
| Multiparous | 5 | |
| Number of children (median, range) | 2 (1–3) | |
| Type of regulatory problem of infant (n) | ||
| Persistent sleep and crying problem | 5 | |
| Persistent crying problem | 4 | |
| Persistent sleep problem | 1 | |
| Persistent eating problem | 1 | |
| Persistent crying and eating problem | 1 | |
| Persistent sleep and crying and eating problem | 1 | |
| Admission of the infant to IMH day clinic | ||
| Mean age in months (SD) | 10.9 (5.2) | |
| Readmission (n) | 2 | |
| Mean total duration of admission, in months (SD) | 5.9 (2.0) | |
| Admission to crisis psychiatric ward during infant’s admission to IMH facility (n) | 4 | NA |
| Medication use * (n) | ||
| Antidepressants | 4 | NA |
| Other ** | 3 | NA |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nuyts, T.; Van Haeken, S.; Crombag, N.; Singh, B.; Ayers, S.; Garthus-Niegel, S.; Braeken, M.A.K.A.; Bogaerts, A. “Nobody Listened”. Mothers’ Experiences and Needs Regarding Professional Support Prior to Their Admission to an Infant Mental Health Day Clinic. Int. J. Environ. Res. Public Health 2021, 18, 10917. https://doi.org/10.3390/ijerph182010917
Nuyts T, Van Haeken S, Crombag N, Singh B, Ayers S, Garthus-Niegel S, Braeken MAKA, Bogaerts A. “Nobody Listened”. Mothers’ Experiences and Needs Regarding Professional Support Prior to Their Admission to an Infant Mental Health Day Clinic. International Journal of Environmental Research and Public Health. 2021; 18(20):10917. https://doi.org/10.3390/ijerph182010917
Chicago/Turabian StyleNuyts, Tinne, Sarah Van Haeken, Neeltje Crombag, Binu Singh, Susan Ayers, Susan Garthus-Niegel, Marijke Anne Katrien Alberta Braeken, and Annick Bogaerts. 2021. "“Nobody Listened”. Mothers’ Experiences and Needs Regarding Professional Support Prior to Their Admission to an Infant Mental Health Day Clinic" International Journal of Environmental Research and Public Health 18, no. 20: 10917. https://doi.org/10.3390/ijerph182010917
APA StyleNuyts, T., Van Haeken, S., Crombag, N., Singh, B., Ayers, S., Garthus-Niegel, S., Braeken, M. A. K. A., & Bogaerts, A. (2021). “Nobody Listened”. Mothers’ Experiences and Needs Regarding Professional Support Prior to Their Admission to an Infant Mental Health Day Clinic. International Journal of Environmental Research and Public Health, 18(20), 10917. https://doi.org/10.3390/ijerph182010917