
Using Lean Six Sigma to Redesign the Supply Chain to the Operating Room Department of a Private Hospital to Reduce Associated Costs and Release Nursing Time to Care


 ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
- Standardisation of stock handling over the sterile area redline,
- A reduction in the value of stock going out of date by a minimum of 50%,
- Providing POU stock to avoid out-of-stock situations,
- Creation of dedicated storage areas by surgical and anaesthesia specialty in the main OR stores,
- Remove non-value-added (NVA) activity for nursing staff and release time to care,
- Development of a proof of concept in a pilot OR suite to roll out to the other OR suites, and
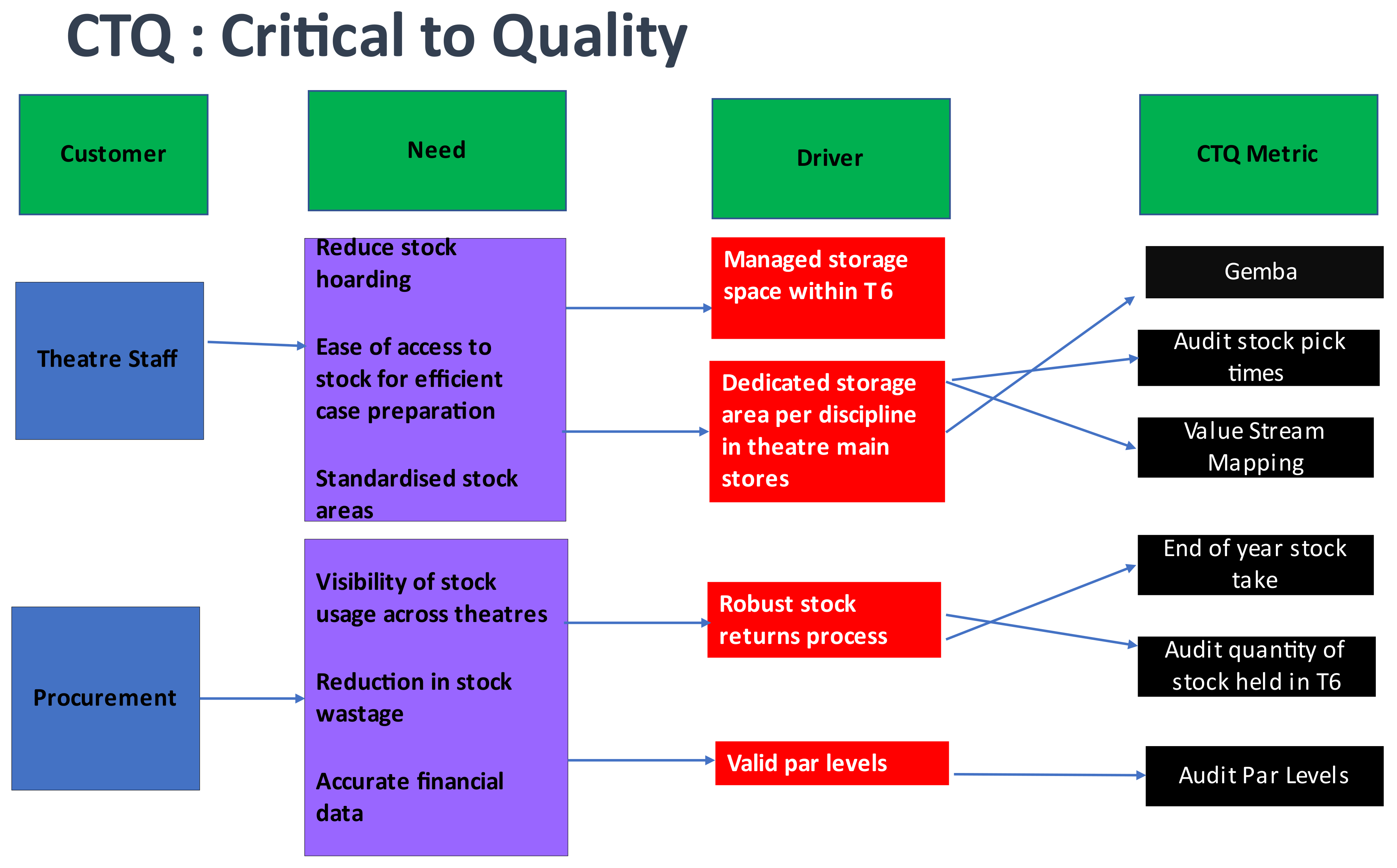
2.1. Define
- A duration of 30 min working alongside individual OR nurses [n = 12] and procurement staff [n = 2] opportunistically (interviewing OR nurses as they dealt with supply and stock for surgical cases).
- 2.
- 40 min meetings with OR managers [n = 8], co-ordinators [n = 4] and OR procurement staff [n = 2]. These interviews were semi-structured and facilitated an interview format that allowed pre-determined topics to be covered (waste, health, and safety, space, and layout) that had been found in the 30 min interviews; however, it also afforded the flexibility to discuss individual participant’s experiences in more detail [40].
- Nursing time to prepare stock for cases,
- End of year stocktake, and
- Value of location of stock within the pilot OR (OR 6).
2.2. Measure
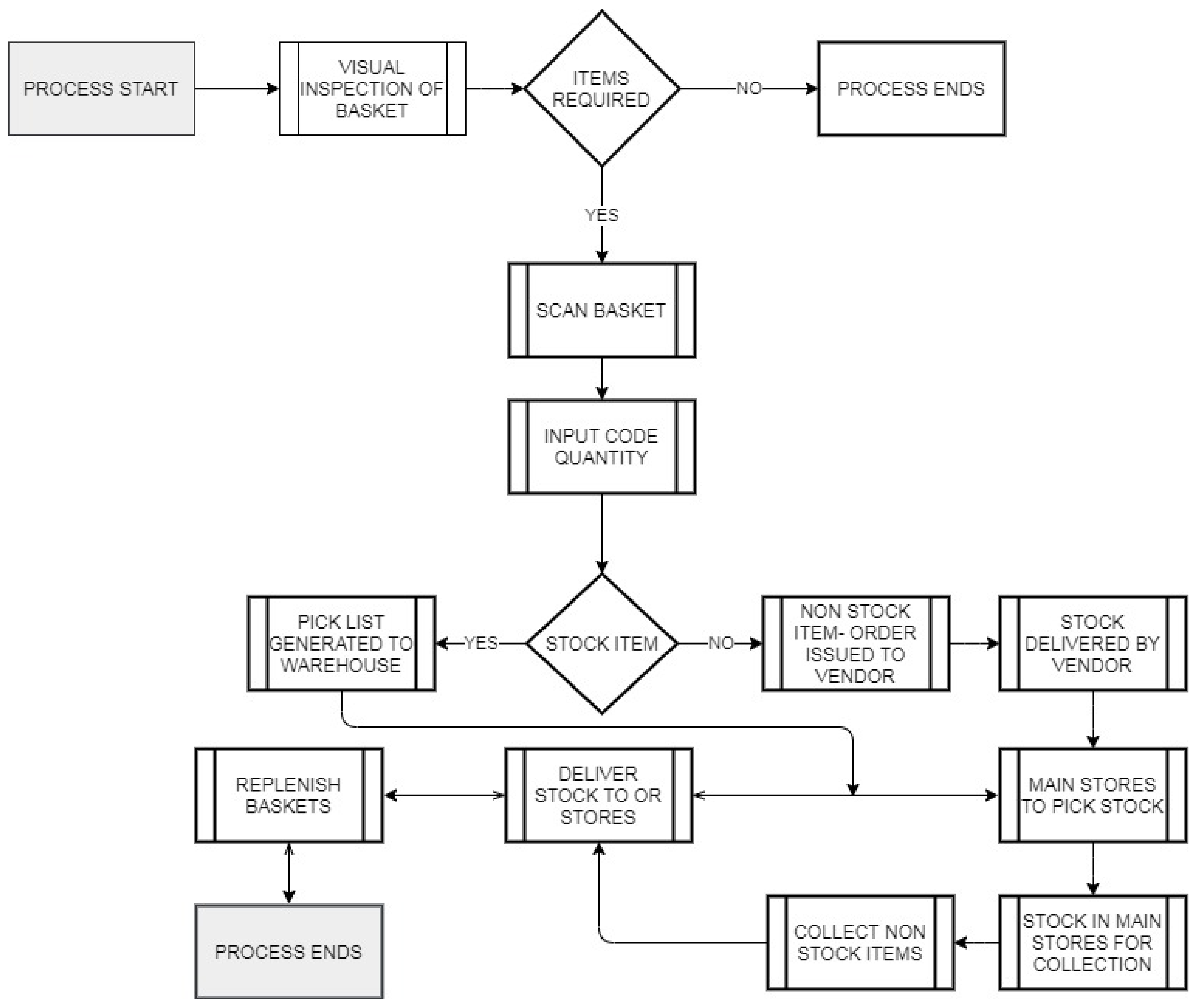
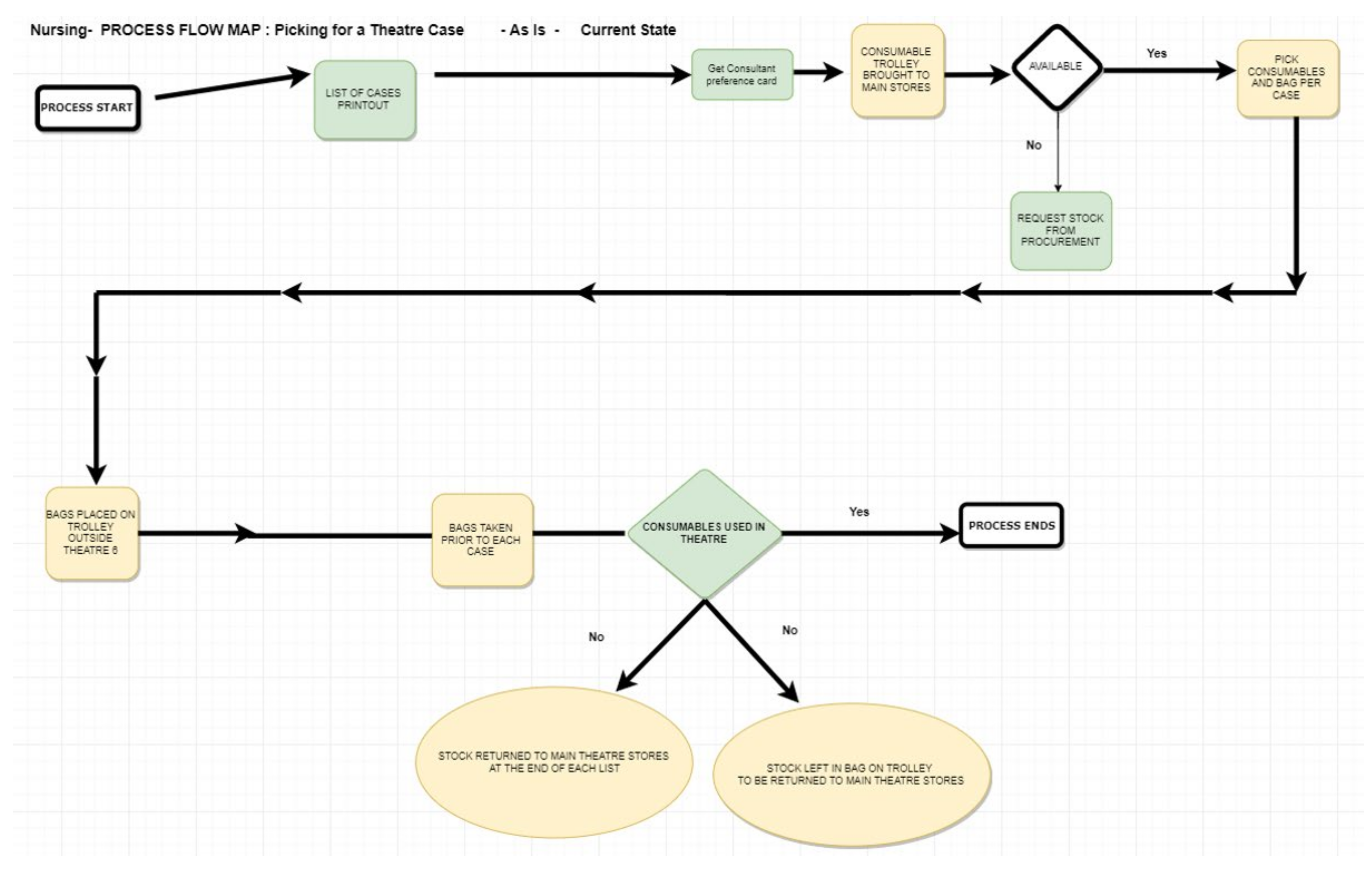
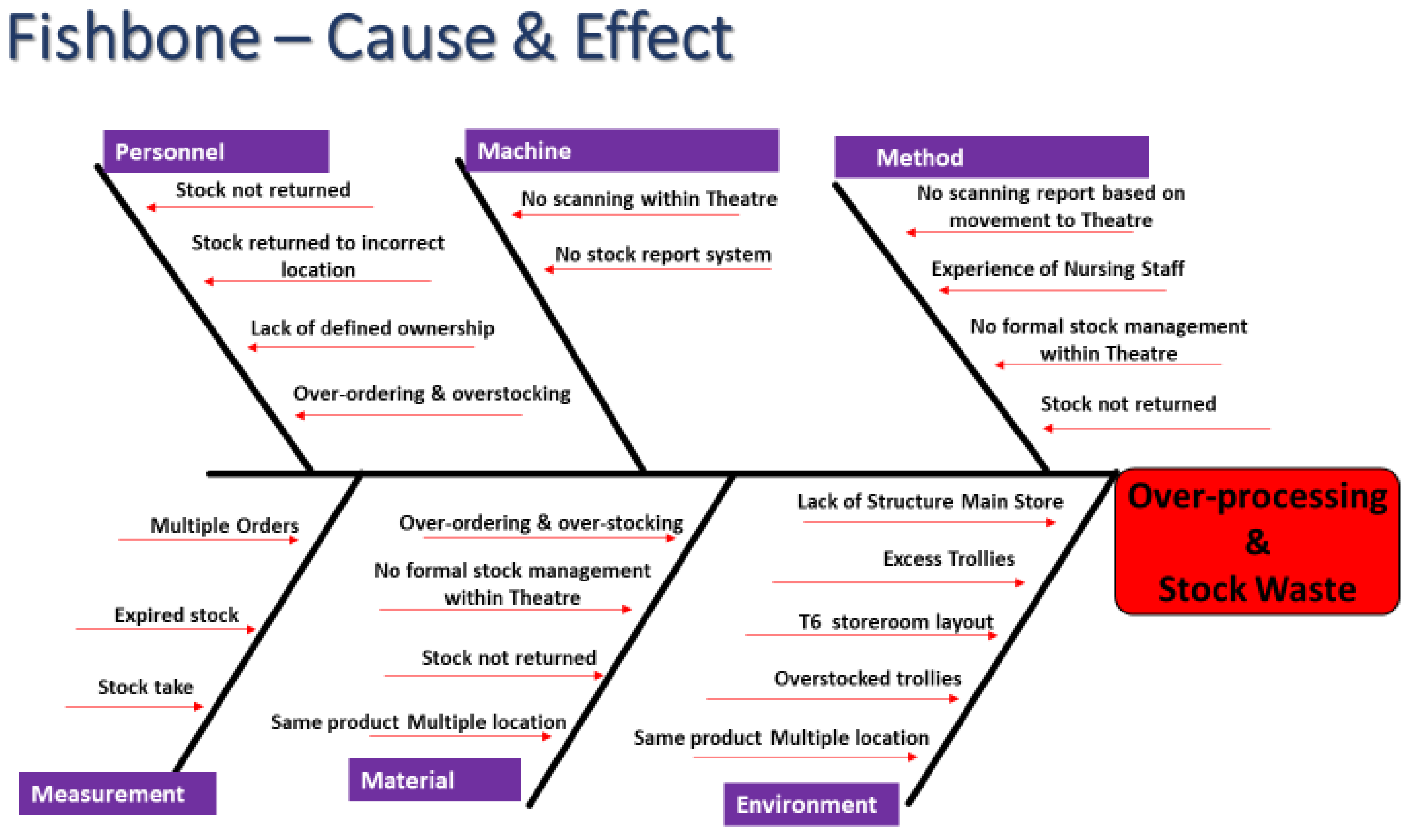
2.3. Analyse
2.4. Improve
3. Results
3.1. Reduction in Stock Holding Value
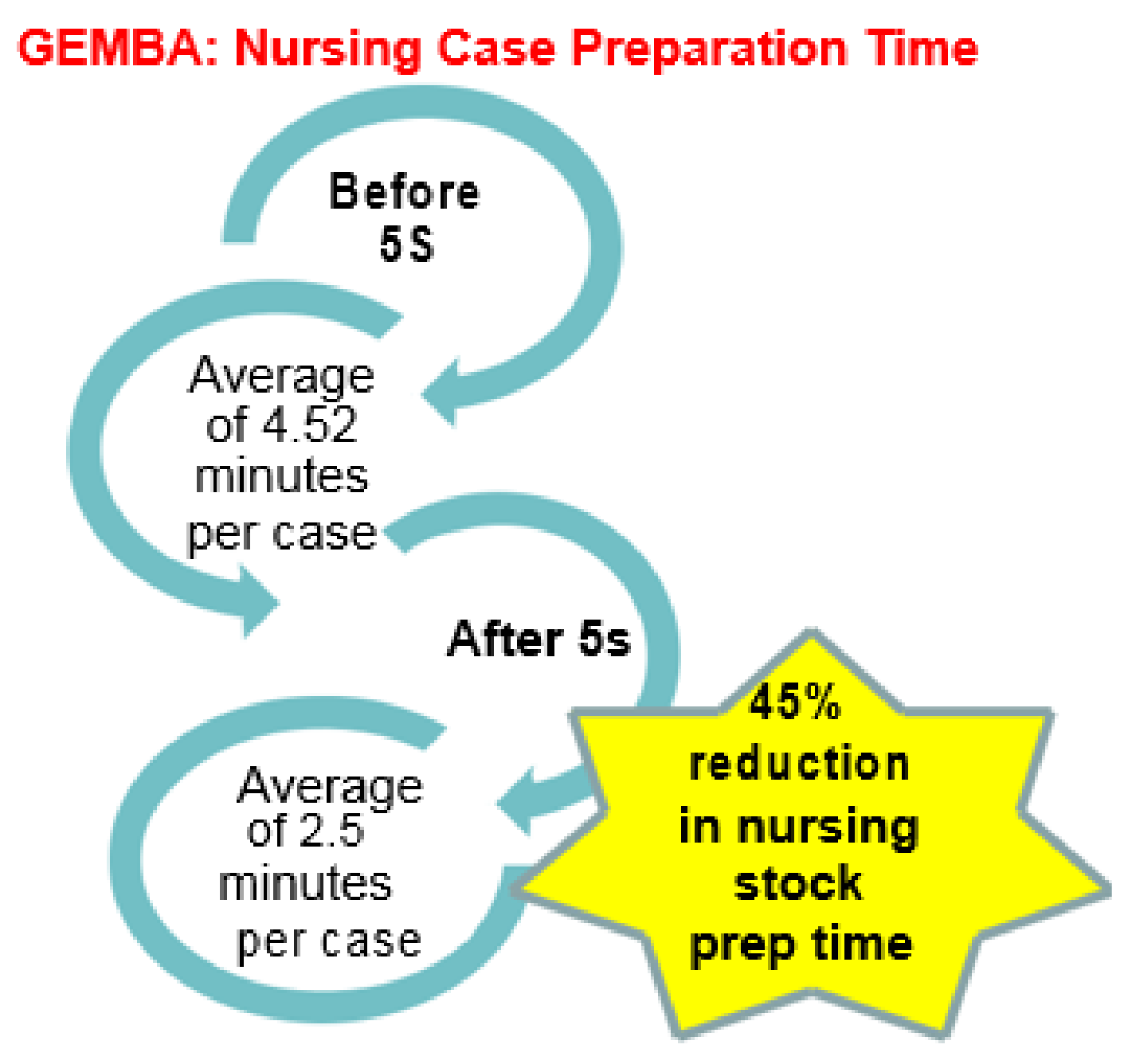
3.2. Reduction in OR Nursing Stock Prep Time
3.3. Reduction in Value of Stock Going out of Date
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Teeling, S.P.; Dewing, J.; Baldie, D. A Discussion of the Synergy and Divergence Between Lean Six Sigma and Person Centered Improvement Sciences. Int. J. Res. Nurs. 2020, 11, 10–23. [Google Scholar] [CrossRef] [Green Version]
- Teeling, S.P.; Dewing, J.; Baldie, D. A Realist Inquiry to Identify the Contribution of Lean Six Sigma to Person-Centred Care and Cultures. Int. J. Environ. Res. Public Health 2021, 18, 10427. [Google Scholar] [CrossRef]
- Womack, J.P.; Jones, D.T. Lean Thinking; Free Press: New York, NY, USA, 2003. [Google Scholar]
- Kollberg, B.; Dahlgaard, J.J.; Brehmer, P.O. Measuring lean initiatives in healthcare services: Issues and findings. Int. J. Product. Perform. Manag. 2007, 56, 7–24. [Google Scholar] [CrossRef]
- Aherne, J.; Whelton, J. Applying Lean in Healthcare: A Collection of International Case Studies; Productivity Press: New York, NY, USA, 2010. [Google Scholar]
- Leite, H.d.R.; Vieira, G.E. Lean philosophy and its applications in the service industry: A review of the current knowledge. Production 2015, 25, 529–541. [Google Scholar] [CrossRef] [Green Version]
- Syrett, M.; Lammiman, J. From Leanness to Fitness; Cromwell Press: London, UK, 1997. [Google Scholar]
- Taiichi, O. Toyota Production System: Beyond Large-Scale Production; CRC Press: Boca Raton, FL, USA, 1988. [Google Scholar]
- Pande, P.S.; Neuman, R.P.; Cavanagh, R.R. The Six Sigma Way Team Fieldbook: An Implementation Guide for Process Improvement; McGraw-Hill: New York, NY, USA, 2002. [Google Scholar]
- Rath & Strong. Six Sigma Pocket Guide; McGraw-Hill: New York, NY, USA, 2002. [Google Scholar]
- George, M.L.; Rowlands, D.; Price, M.; Maxey, J. The Lean Six Sigma Pocket Toolbook; McGraw-Hill: New York, NY, USA, 2005. [Google Scholar]
- Bisgaard, S.; Freiesleben, J. Economics of Six Sigma Programs. Qual. Eng. 2000, 13, 325–331. [Google Scholar] [CrossRef]
- Antony, J. Six Sigma: A strategy for supporting innovation in pursuit of business excellence—Invited paper. Int. J. Technol. Manag. 2007, 37, 8–12. [Google Scholar] [CrossRef]
- Aapaoja, A.; Haapasalo, H.; Söderström, P. Early Stakeholder Involvement in the Project Definition Phase: Case Renovation. ISRN Ind. Eng. 2013, 2013, 953915. [Google Scholar] [CrossRef] [Green Version]
- Mitropoulos, P.; Howell, G.A. Renovation projects: Design process problems and improvement mechanisms. J. Manag. Eng. 2002, 18, 179–185. [Google Scholar] [CrossRef]
- Sunder, M.V. Synergies of Lean Six Sigma. IUP J. Oper. Manag. 2013, 12, 21–31. [Google Scholar]
- Bakar, F.A.A.; Subari, K.; Daril, M.A.M. Critical success factors of Lean Six Sigma deployment: A current review. Int. J. Lean Six Sigma 2015, 6, 339–348. [Google Scholar] [CrossRef]
- Taner, M.T.; Sezen, B.; Antony, J. An overview of six sigma applications in the healthcare industry. Int. J. Health Care Qual. Assur. 2007, 20, 329–340. [Google Scholar] [CrossRef]
- Graban, M. Lean Hospitals—Improving Quality, Patient Safety, and Employee Engagement, 2nd ed.; CRC Press: Boca Raton, FL, USA, 2012. [Google Scholar]
- Womack, J. Gemba Walks, 2nd ed.; Lean Enterprise Institute, Inc.: Cambridge, MA, USA, 2013. [Google Scholar]
- Langabeer, J.R.; DelliFraine, J.L.; Heineke, J.; Abbass, I. Implementation of Lean and Six Sigma quality initiatives in hospitals: A goal theoretic perspective. Oper. Manag. Res. 2009, 2, 13–27. [Google Scholar] [CrossRef]
- Fillingham, D. Can lean save lives? Leadersh. Health Serv. 2007, 20, 231–241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cookson, D.; Read, C.; Mukherjee, P.; Cooke, M. Improving the quality of Emergency Department care by removing waste using Lean Value Stream mapping. Int. J. Clin. Leadersh. 2011, 17, 25–30. [Google Scholar]
- Mazzocato, P.; Thor, J.; Backman, U.; Brommels, M.; Carlsson, J.; Fredrik, J.; Hagmar, M.; Savage, C. Complexity complicates lean: Lessons from seven emergency services. J. Health Organ. Manag. 2014, 28, 266–288. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teichgräber, U.K.; de Bucourt, M. Applying value stream mapping techniques to eliminate non-value-added waste for the procurement of endovascular stents. Eur. J. Radiol. 2012, 81, e47–e52. [Google Scholar] [CrossRef]
- O’Hora, L.; Stanley, J.; Fox, L.; Murphy, K. An investigation of the effectiveness of lean six sigma strategies in reducing computed tomography order to report time. Radiogr. Irel. 2015, 18, 13–17. [Google Scholar]
- Hynes, J.P.; Murray, A.S.; Murray, O.M.; Eustace, S.K.; Gilchrist, S.; Dolan, A.; Lawler, L.P. Use of Lean Six Sigma methodology shows reduction of inpatient waiting time for peripherally inserted central catheter placement. Clin. Radiol. 2019, 74, 733.e5–733.e9. [Google Scholar] [CrossRef] [PubMed]
- Niemeijer, G.C.; Trip, A.; de Jong, L.J.; Wendt, K.W.; Does, R.J.M.M. Impact of 5 Years of Lean Six Sigma in a University Medical Center. Qual. Manag. Health Care 2012, 21, 262–268. [Google Scholar] [CrossRef] [PubMed]
- Tettey, A.H.; Gholston, S.E.; Welch, P.; Dyas, S. Application of Lean Six Sigma to Improve Inventory Management in an Emergency Department. J. Manag. Eng. Integr. 2016, 9, 126–131. [Google Scholar]
- Moons, K.; Waeyenbergh, G.; Pintelon, L. Measuring the logistics performance of internal hospital supply chains—A literature study. Omega 2018, 82, 205–217. [Google Scholar] [CrossRef]
- Guerrero, W.J.; Yeung, T.G.; Guéret, C. Joint-optimization of inventory policies on a multi-product multi-echelon pharmaceutical system with batching and ordering constraints. Eur. J. Oper. Res. 2013, 231, 98–108. [Google Scholar] [CrossRef]
- Taghizadegan, S. Mastering Lean Six Sigma: Advanced Black Belt Concepts; Momentum Press: New York, NY, USA, 2013. [Google Scholar]
- Williams, S.J. Improving Healthcare Operations: The Application of Lean, Agile, and Legality in Care Pathway Design; Palgrave Macmillan: Cham, Switzerland, 2017; pp. 1–136. [Google Scholar]
- Riebling, N.B.; Norouzzadeh, S.; Reeder, G. Quantifying patient satisfaction with process metrics using a weighted bundle approach. BMJ Open Qual. 2019, 8, e000458. [Google Scholar]
- Found, P.; Harrison, R. Understanding the lean voice of the customer. Int. J. Lean Six Sigma 2012, 3, 251–267. [Google Scholar] [CrossRef]
- Dalton, J. Gemba Walks. In Great Big Agile; Apress: Berkeley, CA, USA, 2019. [Google Scholar]
- Pranckevicius, D.; Diaz, D.M.; Gitlow, H. A Lean Six Sigma Case Study: An Application of the “5S” Techniques. J. Adv. Manag. Res. 2008, 5, 63–79. [Google Scholar] [CrossRef]
- Grude, K.; Haug, T.; Andersen, E.S. Goal Directed Management—Effective Strategies and Techniques; Kogan Page: New York, NY, USA, 1984. [Google Scholar]
- Kemper, E.A.; Stringfield, S.; Teddlie, C. Mixed methods sampling strategies in social science research. In Handbook of Mixed Methods in the Social and Behavioral Sciences; Tashakkori, A., Teddlie, C., Eds.; Sage: Thousand Oaks, CA, USA, 2003; pp. 273–296. [Google Scholar]
- Pawson, R.; Tilley, N. Realistic Evaluation; Sage Publications: London, UK, 1997. [Google Scholar]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Bryman, A. Social Research Methods; Oxford University Press: Oxford, UK, 2008. [Google Scholar]
- Colligan, L.; Anderson, J.E.; Potts, H.W.; Berman, J. Does the Process map influence the outcome of quality improvement work? A comparison of a sequential flow diagram and a hierarchal task analysis diagram. BMC Health Serv. Res. 2010, 1, 7. [Google Scholar] [CrossRef] [Green Version]
- Swanson, C. Reorganizing a resuscitation room using Six Sigma (6S) principles. J. Emerg. Nurs. 2014, 40, 371–376. [Google Scholar] [CrossRef]
- Deming, W. The New Economics for Industry, Government, Education, 3rd ed.; MIT Press: Cambridge, MA, USA, 2018. [Google Scholar]
- Manley, K.; Titchen, A.; Hardy, S. Work-based learning in the context of contemporary health care education and practice: A concept analysis. Pract. Dev. Health Care 2009, 8, 87–127. [Google Scholar] [CrossRef]
- Henrique, D.B.; Godinho Filho, M. A Systematic Literature Review of Empirical Research in Lean and Six Sigma in Healthcare. Total Qual. Manag. Bus. Excell. 2020, 31, 429–449. [Google Scholar] [CrossRef]
- McNamara, M.; Teeling, S.P. Developing a University-Accredited Lean Six Sigma Curriculum to Overcome System Blindness. Int. J. Qual. Health Care 2019, 31 (Suppl. 1), 3–5. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Improvement Tool | Description | Reference Number |
|---|---|---|
| Project Charter | A project charter defines the problem statement and attains baseline data for the project. Used to identify goals of the project and what is in scope | [32] |
| SMART Goals Specific, Measurable, Achievable, Relevant, and Timebound | SMART is used to manage the project goals, to determine if they are Specific, Measurable, Achievable, Relevant and Timebound | [32] |
| SIPOC Suppliers, Inputs, Process, Outputs, and Customers | A high-level SIPOC (Supplier, Input, Process, Output, and Customer) highlights the process steps and defines the customers and stakeholders | [33] |
| RACI Responsible, Accountable, Consulted Informed | Identifies which stakeholders are responsible, accountable, which need to be kept informed or consulted | [32] |
| CTQ Critical To Quality | The CTQ is designed to capture the key measurable characteristics of a process or service whose performance standards must be met to satisfy the service user | [34] |
| VOC Voice of the Customer | Engaging with the customer to gather their feedback about their experiences with and expectations for your products or services | [1,2,35] |
| Gemba | Observation of the actual process taking place | [36] |
| Fishbone | Identifies root causes, representing the effect and the factors or causes influencing it | [32] |
| 5S | A system to reduce waste and optimise productivity through maintaining an orderly workplace and using visual cues. A cyclical methodology of ‘Sort, Set in Order, Shine, Standardise and Sustain the Cycle’ | [37] |
| Standardisation for Stock Handling—Solutions | |
|---|---|
| A 5S process carried out in OR stock room—visual management | Relocation of the OR red-line demarcating sterile areas to facilitate stock management |
| A 5S process carried out in OR 6—visual management | Introduction of returns baskets to facilitate stock management post-surgical case list |
| Implementation of centralised suture storage | Inclusion of the OR procurement team as part of the overall OR team within the department |
| A condensed list of suture codes | |
| Description | Value |
|---|---|
| Stock value pre-intervention October 2018 | €221,052 |
| Stock value post-intervention December 2018 | €181,913 |
| Percentage reduction %—post-intervention | 17.7% |
| Boxes | Codes | Percentage Reduction % | |
|---|---|---|---|
| Stock Count Pre-Intervention September 2018 | 1112 Boxes | 247 Codes | |
| Stock Count Post-Intervention March 2019 | 741 Boxes | 194 codes | 33% |
| Stock Count 6 Months Post-Intervention September 2019 | 518 Boxes | 187 codes | 53% |
| Description | Value |
|---|---|
| Stock value pre-intervention December 2017 | €27,000 |
| Stock value post-intervention December 2018 | €2231 |
| Percentage reduction %—post-intervention | 91.7% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
O’Mahony, L.; McCarthy, K.; O’Donoghue, J.; Teeling, S.P.; Ward, M.; McNamara, M. Using Lean Six Sigma to Redesign the Supply Chain to the Operating Room Department of a Private Hospital to Reduce Associated Costs and Release Nursing Time to Care. Int. J. Environ. Res. Public Health 2021, 18, 11011. https://doi.org/10.3390/ijerph182111011
O’Mahony L, McCarthy K, O’Donoghue J, Teeling SP, Ward M, McNamara M. Using Lean Six Sigma to Redesign the Supply Chain to the Operating Room Department of a Private Hospital to Reduce Associated Costs and Release Nursing Time to Care. International Journal of Environmental Research and Public Health. 2021; 18(21):11011. https://doi.org/10.3390/ijerph182111011
Chicago/Turabian StyleO’Mahony, Lisa, Kerrie McCarthy, Josephine O’Donoghue, Seán Paul Teeling, Marie Ward, and Martin McNamara. 2021. "Using Lean Six Sigma to Redesign the Supply Chain to the Operating Room Department of a Private Hospital to Reduce Associated Costs and Release Nursing Time to Care" International Journal of Environmental Research and Public Health 18, no. 21: 11011. https://doi.org/10.3390/ijerph182111011
APA StyleO’Mahony, L., McCarthy, K., O’Donoghue, J., Teeling, S. P., Ward, M., & McNamara, M. (2021). Using Lean Six Sigma to Redesign the Supply Chain to the Operating Room Department of a Private Hospital to Reduce Associated Costs and Release Nursing Time to Care. International Journal of Environmental Research and Public Health, 18(21), 11011. https://doi.org/10.3390/ijerph182111011