
Parental Book-Reading to Preterm Born Infants in NICU: The Effects on Language Development in the First Two Years

 ,
,  ,
, 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedure and Measures
2.3. Data Analysis
3. Results
3.1. Sample Characteristics
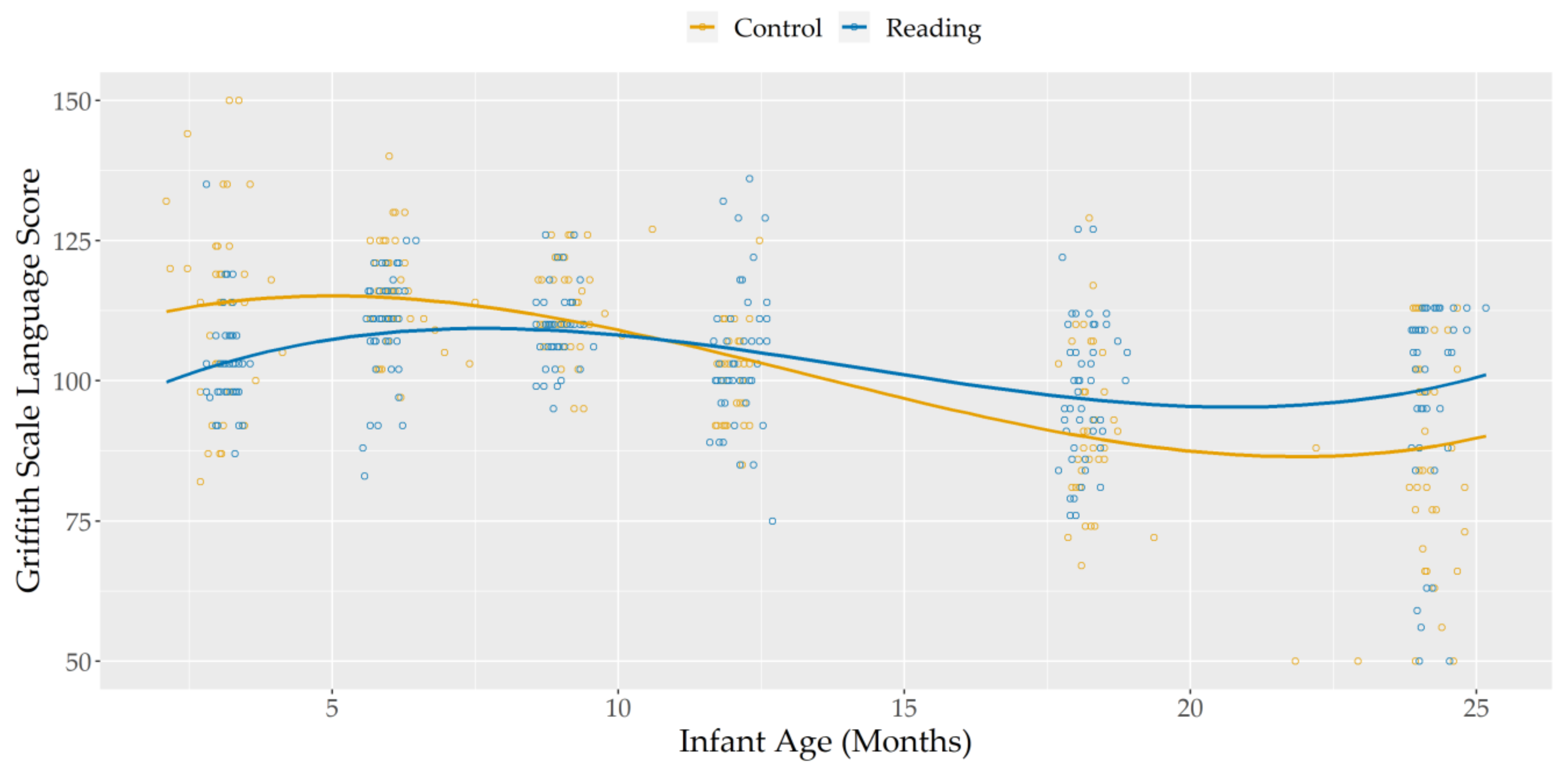
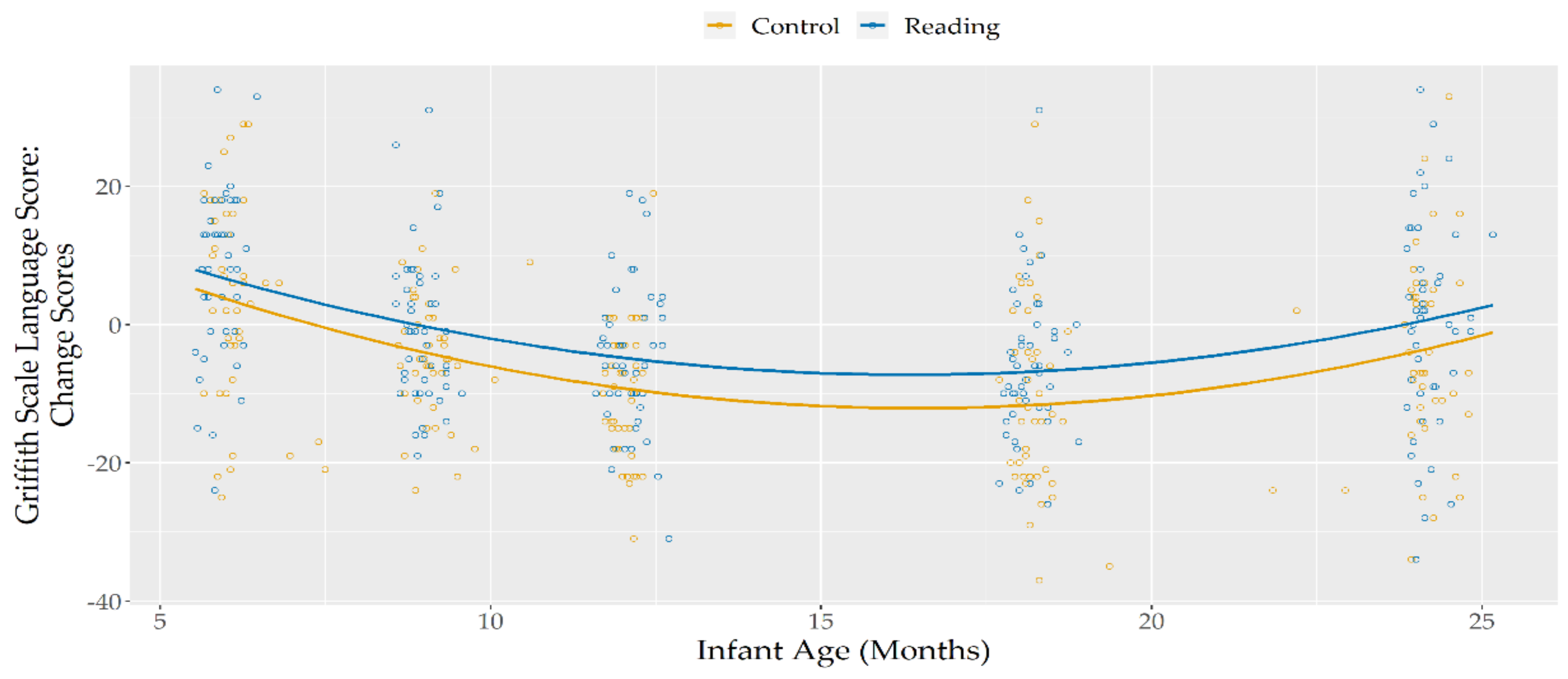
3.2. Language Development across Time
4. Discussion
Limitations and Strengths
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Born too Soon: The Global Action Report on Preterm Birth; World Health Organization: Geneva, Switzerland, 2012. [Google Scholar]
- Manuck, T.A.; Rice, M.M.; Bailit, J.L.; Grobman, W.A.; Reddy, U.M.; Wapner, R.J.; Thorp, J.M.; Caritis, S.N.; Prasad, M.; Tita, A.T.; et al. Eunice Kennedy Shriver National Institute of Child Health and Human Development Maternal-Fetal Medicine Units Network. Preterm neonatal morbidity and mortality by gestational age: A contemporary cohort. Am. J. Obstet. Gynecol. 2016, 215, 103.e1–103.e14. [Google Scholar] [CrossRef] [Green Version]
- Walani, S.R. Global burden of preterm birth. Int. J. Gynecol. Obstet. 2020, 150, 31–33. [Google Scholar] [CrossRef]
- Bhutta, A.; Cleves, M.A.; Casey, P.H.; Cradock, M.M.; Anand, K.J. Cognitive and behavioral outcomes of school-aged children who were born preterm. JAMA 2002, 288, 728–737. [Google Scholar] [CrossRef]
- Anderson, P.J. Neuropsychological outcomes of children born very preterm. Semin. Fetal. Neonatal. Med. 2014, 19, 90–96. [Google Scholar] [CrossRef]
- Jarjour, I.T. Neurodevelopmental outcome after extreme prematurity: A review of the literature. Pediatr. Neurol. 2015, 52, 143–152. [Google Scholar] [CrossRef]
- Scharf, R.J.; Stroustrup, A.; Conaway, M.R.; DeBoer, M.D. Growth and development in children born very low birthweight. Arch. Dis. Child. Fetal. Neonatal. Ed. 2016, 101, F433–F438. [Google Scholar] [CrossRef] [Green Version]
- Reidy, N.; Morgan, A.; Thompson, D.K.; Inder, T.E.; Doyle, L.W.; Anderson, P.J. Impaired language abilities and white matter abnormalities in children born very preterm and/or very low birth weight. J. Pediatr. 2013, 162, 719–724. [Google Scholar] [CrossRef] [Green Version]
- Guarini, A.; Marini, A.; Savini, S.; Alessandroni, R.; Faldella, G.; Sansavini, A. Linguistic features in children born very preterm at preschool age. Dev. Med. Child Neurol. 2016, 58, 949–956. [Google Scholar] [CrossRef] [Green Version]
- Vandormael, C.; Schoenhals, L.; Filippa, M.; Borradori Tolsa, C. Language in preterm born children: Atypical development and effects of early interventions on neuroplasticity. Neural. Plast. 2019, 2019, 6873270. [Google Scholar] [CrossRef] [Green Version]
- Eilers, R.E.; Oller, D.K.; Levine, S.; Basinger, D.; Lynch, M.P.; Urbano, R. The role of prematurity and socioeconomic status in the onset of canonical babbling in infants. Infant Behav. Dev. 1993, 16, 297–315. [Google Scholar] [CrossRef]
- Soraya, M.; Mahmoudi Bakhtiyari, B.; Badiee, Z.; Kazemi, Y.; Soleimani, B. A comparative study of size of expressive lexicon in prematurely born children with full-term 18–36 month’s children. Aud. Vestib. Res. 2017, 21, 76–82. [Google Scholar] [CrossRef]
- Crunelle, D.; Le Normand, M.T.; Delfosse, M.J. [Oral and written language production in prematures children: Results in 7 1/2-year-old]. Folia Phoniatr. Logop. 2003, 55, 115–127. [Google Scholar] [CrossRef] [PubMed]
- Sansavini, A.; Guarini, A.; Alessandroni, R.; Faldella, G.; Giovanelli, G.; Salvioli, G. Are early grammatical and phonological working memory abilities affected by preterm birth? J. Commun. Disord. 2007, 40, 239–256. [Google Scholar] [CrossRef]
- Kunnari, S.; Yliherva, A.; Paavola, L.; Peltoniemi, O.M. Expressive language skills in Finnish two-year-old extremely- and very-low-birth-weight preterm children. Folia Phoniatr. Logo.p 2012, 64, 5–11. [Google Scholar] [CrossRef]
- Stolt, S.; Savini, S.; Guarini, A.; Caselli, M.C.; Matomäki, J.; Lapinleimu, H.; Haataja, L.; Lehtonen, L.; Alessandroni, R.; Faldella, G.; et al. Does the native language influence lexical composition in very preterm children at the age of two years? A cross-linguistic comparison study of Italian and Finnish children. First Lang. 2017, 37, 368–390. [Google Scholar] [CrossRef]
- Guarini, A.; Sansavini, A.; Fabbri, C.; Savini, S.; Alessandroni, R.; Faldella, G.; Karmiloff-Smith, A. Long-term effects of preterm birth on language and literacy at eight years. J. Child Lang. 2010, 37, 865–885. [Google Scholar] [CrossRef]
- Casiro, O.G.; Moddemann, D.M.; Stanwick, R.S.; Panikkar-Thiessen, V.K.; Cowan, H.; Cheang, M.S. Language development of very low birth weight infants and fullterm controls at 12 months of age. Early Hum. Dev. 1990, 24, 65–77. [Google Scholar] [CrossRef]
- Jansson-Verkasalo, E.; Ruusuvirta, T.; Huotilainen, M.; Alku, P.; Kushnerenko, E.; Suominen, K.; Rytky, S.; Luotonen, M.; Kaukola, T.; Tolonen, U.; et al. Atypical perceptual narrowing in prematurely born infants is associated with compromised language acquisition at 2 years of age. BMC Neurosci. 2010, 11, 88. [Google Scholar] [CrossRef] [Green Version]
- Ortiz-Mantilla, S.; Choudhury, N.; Leevers, H.; Benasich, A.A. Understanding language and cognitive deficits in very low birth weight children. Dev. Psychobiol. 2008, 50, 107–126. [Google Scholar] [CrossRef]
- Webb, A.R.; Heller, H.T.; Benson, C.B.; Lahav, A. Mother’s voice and heartbeat sounds elicit auditory plasticity in the human brain before full gestation. Proc. Natl. Acad. Sci. USA 2015, 112, 3152–3157. [Google Scholar] [CrossRef] [Green Version]
- Swain, I.U.; Zelazo, P.R.; Clifton, R.K. Newborn infants’ memory for speech sounds retained over 24 hours. Dev. Psychol. 1993, 29, 312–323. [Google Scholar] [CrossRef]
- Valiante, A.G.; Barr, R.G.; Zelazo, P.R.; Papageorgiou, A.N.; Young, S.N. A typical feeding enhances memory for spoken words in healthy 2 to 3 days old newborns. Pediatrics 2006, 117, e476–e486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Filippa, M.; Poisbeau, P.; Mairesse, J.; Monaci, M.G.; Baud, O.; Hüppi, P.; Grandjean, D.; Kuhn, P. Pain, Parental involvement, and oxytocin in the Neonatal Intensive Care Unit. Front. Psychol. 2019, 10, 715. [Google Scholar] [CrossRef]
- Filippa, M.; Panza, C.; Ferrari, F.; Frassoldati, R.; Kuhn, P.; Balduzzi, S.; D’Amico, R. Systematic review of maternal voice interventions demonstrates increased stability in preterm infants. Acta Paediatr. 2017, 106, 1220–1229. [Google Scholar] [CrossRef] [PubMed]
- Best, K.; Bogossian, F.; New, K. Language exposure of preterm infants in the neonatal unit: A systematic review. Neonatology 2018, 114, 261–276. [Google Scholar] [CrossRef]
- Filippa, M.; Lordier, L.; De Almeida, J.S.; Monaci, M.G.; Adam-Darque, A.; Grandjean, D.; Kuhn, P.; Hüppi, P.S. Early vocal contact and music in the NICU: New insights into preventive interventions. Pediatr. Res. 2020, 87, 249–264. [Google Scholar] [CrossRef]
- Zimmerman, I.L.; Castilleja, N.F. The role of a language scale for infant and preschool assessment. Ment. Retard. Dev. Disabil. Res. Rev. 2005, 11, 238–246. [Google Scholar] [CrossRef]
- Raikes, H.; Pan, B.A.; Luze, G.; Tamis-LeMonda, C.S.; Brooks-Gunn, J.; Constantine, J.; Tarullo, L.B.; Raikes, H.A.; Rodriguez, E.T. Mother-child bookreading in low-income families: Correlates and outcomes during the first three years of life. Child Dev. 2006, 77, 924–953. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Westrup, B. Newborn Individualized Developmental Care and Assessment Program (NIDCAP)-family-centered developmentally supportive care. Early Hum. Dev. 2007, 83, 443–449. [Google Scholar] [CrossRef]
- Als, H.; McAnulty, G.B. The newborn individualized developmental care and assessment program (NIDCAP) with Kangaroo Mother Care (KMC): Comprehensive care for preterm infants. Curr. Womens Health Rev. 2011, 7, 288–301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnston, C.C.; Filion, F.; Nuyt, A.M. Recorded maternal voice for preterm neonates undergoing heel lance. Adv. Neonatal. Care 2007, 7, 258–266. [Google Scholar] [CrossRef]
- Bozzette, M. Healthy preterm infant responses to taped maternal voice. J. Perinat. Neonatal. Nurs. 2008, 22, 307–316. [Google Scholar] [CrossRef]
- Cevasco, A.M. The effects of mothers’ singing on full-term and preterm infants and maternal emotional responses. J. Music Ther. 2008, 45, 273–306. [Google Scholar] [CrossRef] [Green Version]
- Krueger, C.; Parker, L.; Chiu, S.H.; Theriaque, D. Maternal voice and short-term outcomes in preterm infants. Dev. Psychobiol. 2010, 52, 205–212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caskey, M.; Stephens, B.; Tucker, R.; Vohr, B. Importance of parent talk on the development of preterm infant vocalizations. Pediatrics 2011, 128, 910–916. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caskey, M.; Stephens, B.; Tucker, R.; Vohr, B. Adult talk in the NICU with preterm infants and developmental outcomes. Pediatrics 2014, 133, 578–584. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doheny, L.; Hurwitz, S.; Insoft, R.; Ringer, S.; Lahav, A. Exposure to biological maternal sounds improves cardiorespiratory regulation in extremely preterm infants. J. Matern. Fetal. Neonatal. Med. 2012, 25, 1591–1594. [Google Scholar] [CrossRef] [PubMed]
- Zimmerman, E.; Keunen, K.; Norton, M. Weight gain velocity in very low-birth-weight infants: Effects of exposure to biological maternal sounds. Am. J. Perinat. 2013, 30, 863–870. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rand, K.; Lahav, A. Maternal sounds elicit lower heart rate in preterm newborns in the first month of life. Early Hum. Dev. 2014, 90, 679–683. [Google Scholar] [CrossRef] [Green Version]
- Picciolini, O.; Porro, M.; Meazza, A.; Gianni, M.L.; Rivoli, C.; Lucco, G.; Barretta, F.; Bonzini, M.; Mosca, F. Early exposure to maternal voice: Effects on preterm infants development. Early Hum. Dev. 2014, 90, 287–292. [Google Scholar] [CrossRef] [PubMed]
- Shellhaas, R.A.; Burns, J.W.; Barks, J.D.E.; Fauziya Hassan, F.; Chervin, R.D. Maternal voice and infant sleep in the Neonatal Intensive Care Unit. Pediatrics 2019, 144, e30190288. [Google Scholar] [CrossRef]
- Standley, J.M.; Moore, R.S. Therapeutic effects of music and mother’s voice on premature infants. Pediatr. Nurs. 1995, 21, 509–512. [Google Scholar]
- Lejeune, F.; Brand, L.A.; Palama, A.; Parra, J.; Marcus, L.; Barisnikov, K.; Debillon, T.; Gentaz, E.; Berne-Audéoud, F. Preterm infant showed better object handling skills in a neonatal intensive care unit during silence than with a recorded female voice. Acta Paediatr. 2019, 108, 460–467. [Google Scholar] [CrossRef] [PubMed]
- Filippa, M.; Devouche, E.; Arioni, C.; Imberty, M.; Gratier, M. Live maternal speech and singing have beneficial effects on hospitalized preterm infants. Acta Paediatr. 2013, 102, 1017–1020. [Google Scholar] [CrossRef]
- Loewy, J.; Stewart, K.; Dassler, A.M.; Telsey, A.; Homel, P. The effects of music therapy on vital signs, feeding, and sleep in premature infants. Pediatrics 2013, 131, 902–918. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arnon, S.; Diamant, C.; Bauer, S.; Reveg, R.; Sirota, G.; Litmanovitz, I. Maternal singing during kangaroo care led to autonomic stability in preterm infants and reduced maternal anxiety. Acta Pediatr. 2014, 103, 1039–1044. [Google Scholar] [CrossRef] [PubMed]
- Kehl, S.M.; La Marca-Ghaemmaghami, P.; Haller, M.; Pichler-Stachl, E.; Bucher, H.U.; Bassler, D.; Haslbeck, F.B. Creative music therapy with premature infants and their parents: A mixed-method pilot study on parents’ anxiety, stress and depressive symptoms and parent–infant attachment. Int. J. Environ. Res. Public Health 2021, 18, 265. [Google Scholar] [CrossRef] [PubMed]
- Provenzi, L.; Broso, S.; Montirosso, R. Do mothers sound good? A systematic review of the effects of maternal voice exposure on preterm infants’ development. Neurosci. Biobehav. Rev. 2018, 88, 42–50. [Google Scholar] [CrossRef] [PubMed]
- Tronick, E.Z.; Als, H.; Adamson, L.; Wise, S.; Brazelton, T.B. The infant’s response to entrapment between contradictory messages in face-to-face interaction. J. Am. Acad. Child Adolesc. Psychiatry. 1978, 17, 1–13. [Google Scholar] [CrossRef]
- Feldman, R. Parent-infant synchrony and the construction of shared timing; physiological precursors, developmental outcomes, and risk conditions. J. Child Psychol. Psychiatry 2007, 48, 329–354. [Google Scholar] [CrossRef]
- Kärtner, J.; Keller, H.; Yovsi, R.D. Mother-infant interaction during the first 3 months: The emergence of culture-specific contingency patterns. Child Dev. 2010, 81, 540–554. [Google Scholar] [CrossRef]
- Beebe, B.; Messinger, D.; Bahrick, L.E.; Margolis, A.; Buck, K.A.; Chen, H. A systems view of mother-infant face-to-face communication. Dev. Psychol. 2016, 52, 556–571. [Google Scholar] [CrossRef]
- Biasini, A.; Fantini, F.; Neri, E.; Stella, M.; Arcangeli, T. Communication in the Neonatal Intensive Care Unit: A continuous challenge. J. Matern. Fetal. Neonatal. Med. 2012, 25, 2126–2129. [Google Scholar] [CrossRef] [PubMed]
- Neri, E.; Agostini, F.; Perricone, G.; Morales, M.R.; Biasini, A.; Monti, F.; Polizzi, C. Mother- and father-infant interactions at 3 months of corrected age: The effect of severity of preterm birth. Infant Behav. Dev. 2017, 49, 97–103. [Google Scholar] [CrossRef] [PubMed]
- Biasini, A.; Monti, F.; Fiuzzi, F.; Stella, M.; China, M.; Neri, E. Tale reading to premature babies in Neonatal Intensive Care Unit is a further step up in caring for them: Two years later results. In Health Communication: Advocacy Strategies, Effectiveness and Emerging Challenges; Caron, R., Ed.; Nova Science Publisher: New York, NY, USA, 2015; pp. 1–14. [Google Scholar]
- Vally, Z.; Murray, L.; Tomlinson, M.; Cooper, P.J. The impact of dialogic book-sharing training on infant language and attention: A randomized controlled trial in a deprived South African community. J. Child Psychol. Psychiatry 2015, 56, 865–873. [Google Scholar] [CrossRef]
- Dowdall, N.; Melendez-Torres, G.J.; Murray, L.; Gardner, F.; Hartford, L.; Cooper, P.J. Shared Picture Book Reading Interventions for Child Language Development: A Systematic Review and Meta-Analysis. Child Dev. 2020, 91, e383–e399. [Google Scholar] [CrossRef] [PubMed]
- Harries, V.; Brown, A. The association between baby care books that promote strict care routines and infant feeding, night-time care, and maternal-infant interactions. Mater. Child Nutr. 2019, 15, e12858. [Google Scholar] [CrossRef] [Green Version]
- Canfield, C.F.; Miller, E.B.; Shaw, D.S.; Morris, P.; Alonso, A.; Mendelsohn, A.L. Beyond language: Impacts of shared reading on parenting stress and early parent-child relational health. Dev. Psychol. 2020, 56, 1305–1315. [Google Scholar] [CrossRef]
- Horowitz-Kraus, T.; Hutton, J.S. From emergent literacy to reading: How learning to read changes a child’s brain. Acta Paediatr. 2015, 104, 648–656. [Google Scholar] [CrossRef]
- Horowitz-Kraus, T.; Hutton, J.S. Brain connectivity in children is increased by the time they spend reading books and decreased by the length of exposure to screen-based media. Acta Paediatr. 2018, 107, 685–693. [Google Scholar] [CrossRef]
- Albarran, A.S.; Reich, S.M. Using baby books to increase new mothers’ self-efficacy and improve toddler language development. Inf. Child. Dev. 2014, 23, 374–387. [Google Scholar] [CrossRef]
- Duursma, E. The effects of fathers’ and mothers’ reading to their children on language outcomes of children participating in early Head Start in the United States. Father. A J. Theory Res. Pract. About Men Father. 2014, 12, 283–302. [Google Scholar]
- Niklas, F.; Cohrssen, C.; Tayler, C. The sooner, the better: Early reading to children. SAGE Open. 2016, 6. [Google Scholar] [CrossRef]
- Brown, M.I.; Westerveld, M.F.; Trembath, D.; Gillon, G.T. Promoting language and social communication development in babies through an early storybook reading intervention. Int. J. Speech Lang. Pathol. 2018, 20, 337–349. [Google Scholar] [CrossRef]
- O’Farrelly, C.; Doyle, O.; Victory, G.; Palamaro-Munsell, E. Shared reading in infancy and later development: Evidence from an early intervention. J. Appl. Dev. Psychol. 2018, 54, 69–83. [Google Scholar] [CrossRef]
- Muhinyi, A.; Rowe, M.L. Shared reading with preverbal infants and later language development. J. Appl. Dev. Psychol. 2019, 64, 101053. [Google Scholar] [CrossRef]
- Braid, S.; Bernstein, J. Improved cognitive developmental in preterm infants with shared book reading. Neonatal Netw. 2015, 34, 811–818. [Google Scholar] [CrossRef]
- Zuccarini, M.; Suttora, C.; Bello, A.; Aceti, A.; Corvaglia, L.; Caselli, M.C.; Guarini, A.; Sansavini, A. A parent-implemented language intervention for late talkers: An exploratory study on low-risk preterm and full-term children. Int. J. Environ. Res. Public Health 2020, 17, 9123. [Google Scholar] [CrossRef]
- Lariviere, J.; Rennick, J.E. Parent picture-book reading to infants in neonatal intensive care unit as an intervention supporting parent-infant interaction and later book reading. J. Dev. Behav. Pediatr. 2011, 32, 146–152. [Google Scholar] [CrossRef]
- Levesque, B.M.; Tran, A.; Levesque, E.; Shrestha, H.; Silva, R.; Adams, M.; Valles, M.; Burke, J.; Corning-Clarke, A.; Ferguson, C. Implementation of a pilot program of Reach Out and Read® in the neonatal intensive care unit: A quality improvement initiative. J. Perinatol. Off. J. Calif. Perinat. Assoc. 2018, 38, 759–766. [Google Scholar] [CrossRef] [PubMed]
- Shanty, L.; Dowling, R.; Sonnenschein, S.; Hussey-Gardner, B. Evaluation of an early language and literacy program for parents of infants in the NICU. Neonatal Netw. 2019, 38, 206–216. [Google Scholar] [CrossRef]
- Jain, V.G.; Kessler, C.; Lacina, L.; Szumlas, G.A.; Crosh, C.; Hutton, J.S.; Needlman, R.; Dewitt, T.G. Encouraging parental reading for high-risk Neonatal Intensive Care Unit infants. J. Pediatr. 2021, 232, 95–102. [Google Scholar] [CrossRef] [PubMed]
- Neri, E.; Agostini, F.; Baldoni, F.; Facondini, E.; Biasini, A.; Monti, F. Preterm infant development, maternal distress and sensitivity: The influence of severity of birth weight. Early Hum. Dev. 2017, 106–107C, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Neri, E.; Genova, F.; Monti, F.; Trombini, E.; Biasini, A.; Stella, M.; Agostini, F. Developmental dimensions in preterm infants during the first year of life: The influence of severity of prematurity and maternal generalized anxiety. Front. Psychol. 2020, 11, 455. [Google Scholar] [CrossRef] [Green Version]
- Symington, A.; Pinelli, J. Developmental care for promoting development and preventing morbidity in preterm infants. Cochrane Database Syst. Rev. 2006, 2, CD001814. [Google Scholar] [CrossRef] [PubMed]
- Darcy, A.E.; Hancock, L.E.; Ware, E.J. A descriptive study of noise in the neonatal intensive care unit. Ambient levels and perceptions of contributing factors. Adv. Neonatal. Care 2008, 8, 165–175. [Google Scholar] [CrossRef]
- Griffiths, R. The Griffiths Mental Development Scales; Association for Research in Infant and Child Development Test Agency: Henley, UK, 1996. [Google Scholar]
- Mariani, E.; Biasini, A.; Marvulli, L.; Martini, S.; Aceti, A.; Faldella, G.; Corvaglia, L.; Sansavini, A.; Savini, S.; Agostini, F.; et al. Strategies of increased protein intake in ELBW infants fed by human milk lead to long term benefits. Front. Public Health 2018, 6, 272. [Google Scholar] [CrossRef] [PubMed]
- Gibertoni, D.; Sansavini, A.; Savini, S.; Locatelli, C.; Ancora, G.; Perrone, E.; Ialonardi, M.; Rucci, P.; Fantini, M.P.; Faldella, G.; et al. Neurodevelopmental trajectories of preterm infants of italian native-born and migrant mothers and role of neonatal feeding. Int. J. Environ. Res. Public Health 2020, 17, 4588. [Google Scholar] [CrossRef]
- Gibertoni, D.; Corvaglia, L.; Vandini, S.; Rucci, P.; Savini, S.; Alessandroni, R.; Sansavini, A.; Fantini, M.P.; Faldella, G. Positive effect of human milk feeding during NICU hospitalization on 24 month neurodevelopment of very low birth weight infants: An Italian cohort study. PLoS ONE 2015, 10, e0116552. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sansavini, A.; Savini, S.; Guarini, A.; Broccoli, S.; Alessandroni, R.; Faldella, G. The effect of gestational age on developmental outcomes: A longitudinal study in the first 2 years of life. Child Care Health Dev. 2011, 37, 26–36. [Google Scholar] [CrossRef]
- Gleason, J.B.; Ely, R. Gender differences in language development. In Biology, Society, and Behavior: The Development of Sex Differences in Cognition; McGillicuddy-De Lisi, A., De Lisi, R., Eds.; Ablex Publishing Corporation: New York, NY, USA, 2002; pp. 127–154. [Google Scholar]
- Benjamini, Y.; Hochberg, Y. Controlling the false discovery rate: A practical and powerful approach to multiple testing. J. R. Stat. Soc. Ser. B 1995, 57, 289–300. [Google Scholar] [CrossRef]
- R Core Team. Writing R Extensions; R Foundation for Statistical Computing: Vienna, Austria, 2021. [Google Scholar]
- Maccoby, E.E.; Jacklin, C.N. The Psychology of Sex Differences; Stanford University Press: Stanford, CA, USA, 1974. [Google Scholar]
- Fenson, L.; Dale, P.S.; Reznick, J.S.; Bates, E.; Thal, D.J.; Pethick, S.J. Variability in early communicative development. Monogr. Soc. Res. Child Dev. 1994, 59, 1–173. [Google Scholar] [CrossRef] [PubMed]
- Sansavini, A.; Guarini, A.; Savini, S.; Broccoli, S.; Justice, L.; Alessandroni, R.; Faldella, G. Longitudinal trajectories of gestural and linguistic abilities in very preterm infants in the second year of life. Neuropsychologia 2011, 49, 3677–3688. [Google Scholar] [CrossRef] [PubMed]
- Eriksson, M.; Marschik, P.B.; Tulviste, T.; Almgren, M.; Pérez Pereira, M.; Wehberg, S.; Marjanovič-Umek, L.; Gayraud, F.; Kovacevic, M.; Gallego, C. Differences between girls and boys in emerging language skills: Evidence from 10 language communities. B. J. Dev. Psychol. 2012, 30, 326–343. [Google Scholar] [CrossRef] [PubMed]
- Etchell, A.; Adhikari, A.; Weinberg, L.S.; Choo, A.L.; Garnett, E.O.; Chow, H.M.; Chang, S.E. A systematic literature review of sex differences in childhood language and brain development. Neuropsychologia 2018, 114, 19–31. [Google Scholar] [CrossRef]
- Hyde, J.S. The gender similarities hypothesis. Am. Psychol. 2005, 60, 581–592. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hyde, J.S.; Linn, M.C. Gender differences in verbal ability: A meta-analysis. Psychol. Bull. 1988, 104, 53–69. [Google Scholar] [CrossRef]
- Wallentin, M. Putative sex differences in verbal abilities and language cortex: A critical review. Brain Lang. 2009, 108, 175–183. [Google Scholar] [CrossRef]
- Isaacs, D. Out of the mouths of babes. J. Paediatr. Child Health 2010, 46, 703. [Google Scholar] [CrossRef]
- Mol, S.E.; Bus, A.G. To read or not to read: A meta-analysis of print exposure from infancy to early adulthood. Psychol. Bull. 2011, 137, 267–296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spinelli, M.; Frigerio, A.; Montali, L.; Fasolo, M.; Spada, M.S.; Mangili, G. I still have difficulties feeling like a mother: The transition to motherhood of preterm infants mothers. Psychol. Health 2016, 31, 184–204. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Reading Group (N = 55) | Control Group (N = 45) | p | |
|---|---|---|---|
| Infants | |||
| Gender, % Male | 56.4 | 62.2 | 0.698 |
| Birth Weight, % ELBW | 34.6 | 46.7 | 0.305 |
| Gestational Age, % ELGA | 47.3 | 60.0 | 0.286 |
| Mothers | |||
| Age (Yrs), M ± SD | 35.20 ± 4.82 | 34.14 ± 5.10 | 0.301 |
| Nationality, % Italian | 85.5 | 91.1 | 0.578 |
| Education | 0.412 | ||
| Middle School, % | 16.4 | 20.0 | |
| High School, % | 47.3 | 60.0 | |
| University, % | 27.3 | 17.8 | |
| Marital Status, % Married | 49.1 | 64.4 | 0.128 |
| Infant Age | Reading Group (N = 55) | Control Group (N = 45) | ||
|---|---|---|---|---|
| M ± SD | Change Scores | M ± SD | Change Scores | |
| 3 months | 102.50 ± 1.74 | / | 112.80 ± 1.93 | / |
| 6 months | 109.48 ± 1.27 | 7.3 | 116.45 ± 1.41 | 3.66 |
| 9 months | 108.41 ± 1.02 | −0.64 | 111.75 ± 1.13 | −4.70 |
| 12 months | 103.20 ± 1.49 | −5.19 | 101.75 ± 1.65 | −10.00 |
| 18 months | 97.09 ± 1.79 | −6.27 | 91.75 ± 1.98 | −10.0 |
| 24 months | 97.11 ± 2.60 | 0.54 | 87.45 ± 2.88 | −4.30 |
| Effects | Degrees of Freedom | F Value | p |
|---|---|---|---|
| Group | 1, 88.04 | 0.51 | 0.637 |
| Infant Age (IA) | 1, 285.77 | 135.06 | ≤0.001 |
| IA (Quadratic) | 1, 140.20 | 25.90 | ≤0.001 |
| IA (Cubic) | 1, 281.98 | 69.00 | ≤0.001 |
| Group * IA | 1, 285.77 | 9.42 | 0.004 |
| Group * IA (Quadratic) | 1, 140.21 | 1.44 | 0.348 |
| Group * IA (Cubic) | 1, 281.97 | 0.07 | 0.798 |
| Effects | Degrees of Freedom | F Value | p |
|---|---|---|---|
| Group | 1, 88.32 | 5.40 | 0.038 |
| Infant Age (IA) | 1, 89.69 | 46.01 | ≤0.001 |
| IA (Quadratic) | 1, 89.63 | 51.18 | ≤0.001 |
| Group * IA | 1, 89.69 | 0.24 | 0.746 |
| Group * IA (Quadratic) | 1, 89.63 | 0.11 | 0.798 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Neri, E.; De Pascalis, L.; Agostini, F.; Genova, F.; Biasini, A.; Stella, M.; Trombini, E. Parental Book-Reading to Preterm Born Infants in NICU: The Effects on Language Development in the First Two Years. Int. J. Environ. Res. Public Health 2021, 18, 11361. https://doi.org/10.3390/ijerph182111361
Neri E, De Pascalis L, Agostini F, Genova F, Biasini A, Stella M, Trombini E. Parental Book-Reading to Preterm Born Infants in NICU: The Effects on Language Development in the First Two Years. International Journal of Environmental Research and Public Health. 2021; 18(21):11361. https://doi.org/10.3390/ijerph182111361
Chicago/Turabian StyleNeri, Erica, Leonardo De Pascalis, Francesca Agostini, Federica Genova, Augusto Biasini, Marcello Stella, and Elena Trombini. 2021. "Parental Book-Reading to Preterm Born Infants in NICU: The Effects on Language Development in the First Two Years" International Journal of Environmental Research and Public Health 18, no. 21: 11361. https://doi.org/10.3390/ijerph182111361
APA StyleNeri, E., De Pascalis, L., Agostini, F., Genova, F., Biasini, A., Stella, M., & Trombini, E. (2021). Parental Book-Reading to Preterm Born Infants in NICU: The Effects on Language Development in the First Two Years. International Journal of Environmental Research and Public Health, 18(21), 11361. https://doi.org/10.3390/ijerph182111361