
Relationship between Physical Activity and Physical and Mental Health Status in Pregnant Women: A Prospective Cohort Study of the Japan Environment and Children’s Study

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
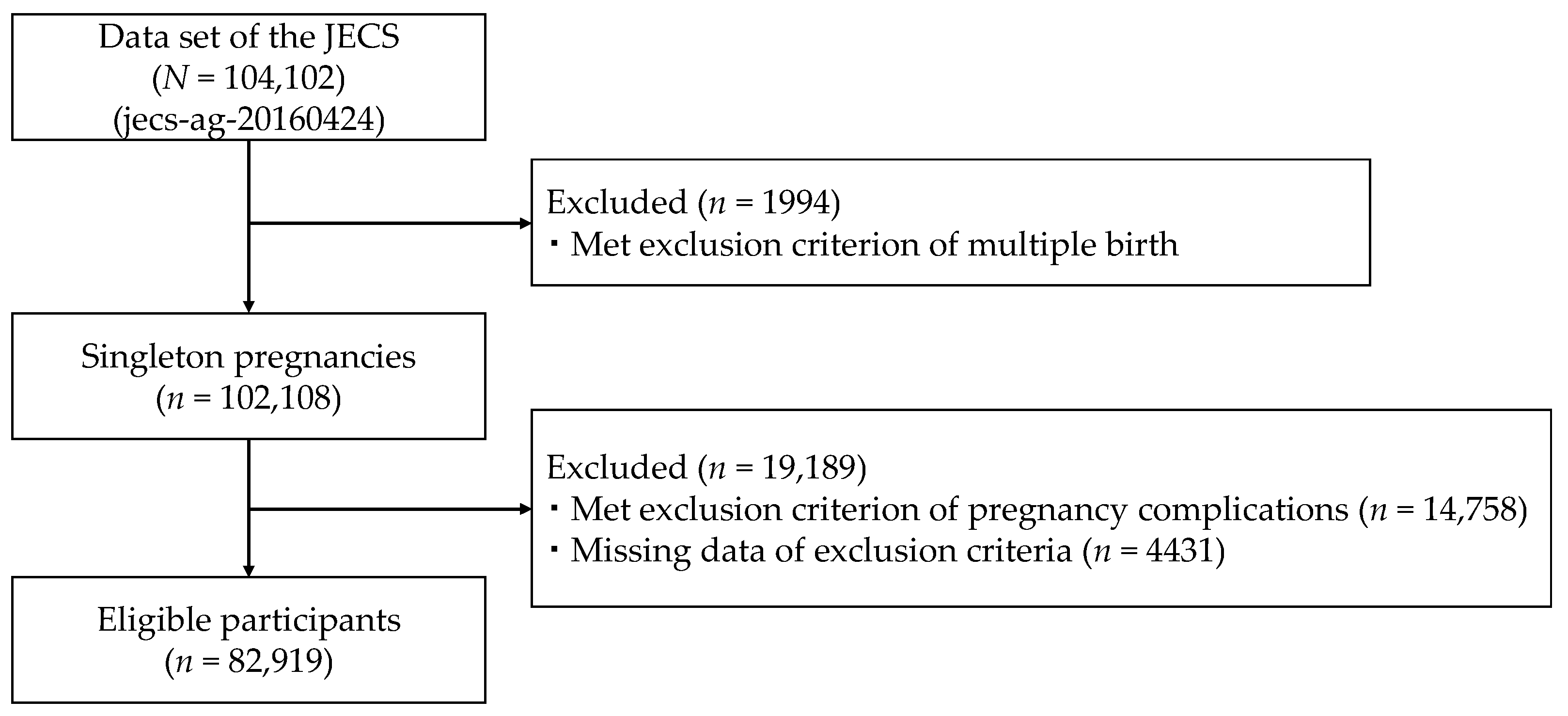
2.2. Participants
2.3. Variables
2.3.1. Exposures
2.3.2. Outcomes
2.3.3. Covariates
2.4. Bias
2.5. Statistical Methods
3. Results
3.1. Physical Activity Levels before Pregnancy and Physical and Mental Health Status in the First Trimester
3.2. Physical Activity Levels in the Second and Third Trimesters and Physical and Mental Health Status
3.3. Physical Activity Levels and Physical and Mental Health Status in the Second and Third Trimesters
4. Discussion
4.1. Appropriate Range of Pre-Pregnancy Physical Activity Levels for Women
4.2. Appropriate Range of Physical Activity Levels for Pregnant Women
4.3. Appropriate Range for Changes in Physical Activity Levels during Pregnancy
4.4. Study Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dye, T.D.; Knox, K.L.; Artal, R.; Aubry, R.H.; Wojtowycz, M.A. Physical Activity, Obesity, and Diabetes in Pregnancy. Am. J. Epidemiol. 1997, 146, 961–965. [Google Scholar] [CrossRef] [Green Version]
- American College of Obstetricians and Gynecologists. Physical Activity and Exercise During Pregnancy and the Postpartum Period: ACOG Committee Opinion, Number 804. Obstet. Gynecol. 2020, 135, e178–e188. [Google Scholar] [CrossRef] [Green Version]
- Strøm, M.; Mortensen, E.L.; Halldorson, T.I.; Østerdal, M.L.; Olsen, S.F. Leisure-Time Physical Activity in Pregnancy and Risk of Postpartum Depression: A prospective study in a large national birth cohort. J. Clin. Psychiatry 2009, 70, 1707–1714. [Google Scholar] [CrossRef]
- Takami, M.; Tsuchida, A.; Takamori, A.; Aoki, S.; Ito, M.; Kigawa, M.; Kawakami, C.; Hirahara, F.; Hamazaki, K.; Inadera, H.; et al. Effects of physical activity during pregnancy on preterm delivery and mode of delivery: The Japan Environment and Children’s Study, birth cohort study. PLoS ONE 2018, 13, e0206160. [Google Scholar] [CrossRef] [Green Version]
- Rêgo, A.S.; Alves, M.T.; Batista, R.; Ribeiro, C.C.C.; Bettiol, H.; Cardoso, V.C.; Barbieri, M.A.; Loureiro, F.H.F.; Silva, A. Physical activity in pregnancy and adverse birth outcomes. Cad. Saúde Pública 2016, 32, e00086915. [Google Scholar] [CrossRef] [Green Version]
- Nascimento, S.L.; Surita, F.; Cecatti, J.G. Physical exercise during pregnancy: A systematic review. Curr. Opin. Obstet. Gynecol. 2012, 24, 387–394. [Google Scholar] [CrossRef]
- Kramer, M.S.; McDonald, S.W. Aerobic exercise for women during pregnancy. Cochrane Database Syst. Rev. 2006, 2006, CD000180. [Google Scholar] [CrossRef]
- American College of Sports Medicine. ACSM’s Guidelines for Exercise Testing and Prescription, 10th ed.; Riebe, D., Ehrman, J., Liguori, G., Magal, M., Eds.; Wolters Kluwer Health: Philadelphia, PA, USA, 2018. [Google Scholar]
- Evenson, K.R.; Barakat, R.; Brown, W.J.; Dargent-Molina, P.; Haruna, M.; Mikkelsen, E.M.; Mottola, M.F.; Owe, K.M.; Rousham, E.K.; Yeo, S. Guidelines for Physical Activity During Pregnancy: Comparisons from Around the World. Am. J. Lifestyle Med. 2014, 8, 102–121. [Google Scholar] [CrossRef] [Green Version]
- TTakito, M.Y.; Benicio, M.H.; Neri Lde, C. Physical activity by pregnant women and outcomes for newborns: A systematic review. Rev. Saude. Publica 2009, 43, 1059–1069. [Google Scholar] [CrossRef] [Green Version]
- Mottola, M.F.; Davenport, M.H.; Ruchat, S.-M.; Davies, G.A.; Poitras, V.J.; Gray, C.; Garcia, A.J.; Barrowman, N.; Adamo, K.B.; Duggan, M.; et al. 2019 Canadian guideline for physical activity throughout pregnancy. Br. J. Sports Med. 2018, 52, 1339–1346. [Google Scholar] [CrossRef] [Green Version]
- Kardel, K.R. Effects of intense training during and after pregnancy in top-level athletes. Scand. J. Med. Sci. Sports 2005, 15, 79–86. [Google Scholar] [CrossRef]
- Bø, K.; Artal, R.; Barakat, R.; Brown, W.; Davies, G.A.L.; Dooley, M.; Evenson, K.R.; Haakstad, L.A.H.; Henriksson-Larsen, K.; Kayser, B.; et al. Exercise and pregnancy in recreational and elite athletes: 2016 evidence summary from the IOC expert group meeting, Lausanne. Part 1—exercise in women planning pregnancy and those who are pregnant. Br. J. Sports Med. 2016, 50, 571–589. [Google Scholar] [CrossRef] [PubMed]
- Beetham, K.S.; Giles, C.; Noetel, M.; Clifton, V.; Jones, J.C.; Naughton, G. The effects of vigorous intensity exercise in the third trimester of pregnancy: A systematic review and meta-analysis. BMC Pregnancy Childbirth 2019, 19, 281. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, A.; van der Waerden, J.; Melchior, M.; Bolze, C.; El-Khoury, F.; Pryor, L. Physical activity during pregnancy and postpartum depression: Systematic review and meta-analysis. J. Affect. Disord. 2019, 246, 29–41. [Google Scholar] [CrossRef]
- Fan, S.; Guan, J.; Cao, L.; Wang, M.; Zhao, H.; Chen, L.; Yan, L. Psychological effects caused by COVID-19 pandemic on pregnant women: A systematic review with meta-analysis. Asian J. Psychiatry 2021, 56, 102533. [Google Scholar] [CrossRef]
- Ishitsuka, K.; Nakayama, S.F.; Kishi, R.; Mori, C.; Yamagata, Z.; Ohya, Y.; Kawamoto, T.; Kamijima, M. Japan Environment and Children’s Study: Backgrounds, activities, and future directions in global perspectives. Environ. Health Prev. Med. 2017, 22, 61. [Google Scholar] [CrossRef]
- Kawamoto, T.; Nitta, H.; Murata, K.; Toda, E.; Tsukamoto, N.; Hasegawa, M.; Yamagata, Z.; Kayama, F.; Kishi, R.; Ohya, Y.; et al. Rationale and study design of the Japan environment and children’s study (JECS). BMC Public Health 2014, 14, 25. [Google Scholar] [CrossRef] [Green Version]
- Michikawa, T.; Nitta, H.; Nakayama, S.F.; Yamazaki, S.; Isobe, T.; Tamura, K.; Suda, E.; Ono, M.; Yonemoto, J.; Iwai-Shimada, M.; et al. Baseline Profile of Participants in the Japan Environment and Children’s Study (JECS). J. Epidemiol. 2018, 28, 99–104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International Physical Activity Questionnaire: 12-Country Reliability and Validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murase, N.; Katsumura, T.; Ueda, C.; Inoue, S.; Shimomitsu, T. International standardization of physical activity level: Reliability and validity study of the Japanese version of the International Physical Activity Questionnaire (IPAQ). J. Health Welf. Stat. 2003, 49, 1–9. [Google Scholar]
- Guidelines for Data Processing and Analysis of the International Physical Activity Questionnaire (IPAQ)—Short and Long Forms. Web Site. 2005. Available online: https://www.academia.edu/5346814/Guidelines_for_Data_Processing_and_Analysis_of_the_International_Physical_Activity_Questionnaire_IPAQ_Short_and_Long_Forms_Contents (accessed on 22 October 2021).
- Shibata, A.; Oka, K.; Nakamura, Y.; Muraoka, I. Recommended level of physical activity and health-related quality of life among Japanese adults. Health Qual. Life Outcomes 2007, 5, 64. [Google Scholar] [CrossRef] [Green Version]
- Tokuda, Y.; Okubo, T.; Ohde, S.; Jacobs, J.; Takahashi, O.; Omata, F.; Yanai, H.; Hinohara, S.; Fukui, T. Assessing Items on the SF-8 Japanese Version for Health-Related Quality of Life: A Psychometric Analysis Based on the Nominal Categories Model of Item Response Theory. Value Health 2009, 12, 568–573. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fukuhara, S.; Suzukamo, Y. Manual of the SF-8 Japanese Version; Institute for Health Outcomes and Process Evaluation Research: Kyoto, Japan, 2004. [Google Scholar]
- Gómez, L.F.; Moreno, J.; Gómez, O.L.; Carvajal, R.; Parra, D.C. Physical activity and health-related quality of life among adult women in Cali, Colombia: A cross-sectional study. Qual. Life Res. 2013, 22, 2351–2358. [Google Scholar] [CrossRef] [PubMed]
- Lang, L.; Zhang, L.; Zhang, P.; Li, Q.; Bian, J.; Guo, Y. Evaluating the reliability and validity of SF-8 with a large representative sample of urban Chinese. Health Qual. Life Outcomes 2018, 16, 55. [Google Scholar] [CrossRef] [Green Version]
- Roberts, B.; Browne, J.; Ocaka, K.F.; Oyok, T.; Sondorp, E. The reliability and validity of the SF-8 with a conflict-affected population in northern Uganda. Health Qual. Life Outcomes 2008, 6, 108. [Google Scholar] [CrossRef] [Green Version]
- Onagbiye, S.O.; Moss, S.J.; Cameron, M. Validity and reliability of the Setswana translation of the Short Form-8 health-related quality of life health survey in adults. Health SA Gesondheid 2018, 23, 1092. [Google Scholar] [CrossRef]
- Wirtz, M.A.; Schulz, A.; Brähler, E. Confirmatory and bi-factor analysis of the Short Form Health Survey 8 (SF-8) scale structure in a German general population sample. Health Qual. Life Outcomes 2021, 19, 73. [Google Scholar] [CrossRef]
- Tendais, I.; Figueiredo, B.; Mota, J.; Conde, A. Physical activity, health-related quality of life and depression during pregnancy. Cad. Saúde Pública 2011, 27, 219–228. [Google Scholar] [CrossRef]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.-P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef]
- Ishikawa-Takata, K.; Tabata, I. Exercise and physical activity reference for health promotion 2006 (EPAR2006). J. Epidemiol. 2007, 17, 177. [Google Scholar] [CrossRef]
- Petrovic, D.; Perovic, M.; Lazovic, B.; Pantic, I. Association between walking, dysphoric mood and anxiety in late pregnancy: A cross-sectional study. Psychiatry Res. 2016, 246, 360–363. [Google Scholar] [CrossRef]
- Landolfi, E. Exercise Addiction. Sports Med. 2013, 43, 111–119. [Google Scholar] [CrossRef] [PubMed]
- Levit, M.; Weinstein, A.; Weinstein, Y.; Tzur-Bitan, D.; Weinstein, A. A study on the relationship between exercise addiction, abnormal eating attitudes, anxiety and depression among athletes in Israel. J. Behav. Addict. 2018, 7, 800–805. [Google Scholar] [CrossRef]
- Berghella, V.; Saccone, G. Exercise in pregnancy! Am. J. Obstet. Gynecol. 2017, 216, 335–337. [Google Scholar] [CrossRef] [PubMed]
- Daley, A.; Jolly, K.; MacArthur, C. The effectiveness of exercise in the management of post-natal depression: Systematic review and meta-analysis. Fam. Pract. 2009, 26, 154–162. [Google Scholar] [CrossRef] [Green Version]
- Pivarnik, J.M.; Szymanski, L.M.; Conway, M.R. The Elite Athlete and Strenuous Exercise in Pregnancy. Clin. Obstet. Gynecol. 2016, 59, 613–619. [Google Scholar] [CrossRef] [PubMed]
- Tenforde, A.S.; Toth, K.E.S.; Langen, E.; Fredericson, M.; Sainani, K.L. Running Habits of Competitive Runners During Pregnancy and Breastfeeding. Sports Health A Multidiscip. Approach 2015, 7, 172–176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakahara, K.; The Japan Environment and Children’s Study Group; Michikawa, T.; Morokuma, S.; Ogawa, M.; Kato, K.; Sanefuji, M.; Shibata, E.; Tsuji, M.; Shimono, M.; et al. Influence of physical activity before and during pregnancy on infant’s sleep and neurodevelopment at 1-year-old. Sci. Rep. 2021, 11, 8099. [Google Scholar] [CrossRef]


{kind=link}
| Variables and Categories | n = 82,919 | |
|---|---|---|
| n | (%) | |
| Age at pregnancy | ||
| <20 | 941 | (1.1) |
| 20–29 | 33,120 | (39.9) |
| 30–39 | 44,607 | (53.8) |
| ≥40 | 2708 | (3.3) |
| Missing | 1543 | (1.9) |
| Annual household income (million Japanese yen) | ||
| <2 | 4249 | (5.1) |
| 2–4 | 26,100 | (31.5) |
| 4–6 | 24,652 | (29.7) |
| 6–8 | 11,742 | (14.2) |
| 8–10 | 4869 | (5.9) |
| ≥10 | 3184 | (3.8) |
| Missing | 8123 | (9.8) |
| Mother’s final academic background | ||
| Junior high school | 3781 | (4.6) |
| High school | 25,637 | (30.9) |
| Higher professional school | 1322 | (1.6) |
| Technical college | 18,243 | (22.0) |
| Two-year college | 13,916 | (16.8) |
| Four-year college | 16,102 | (19.4) |
| Graduate school | 1145 | (1.4) |
| Missing | 2773 | (3.3) |
| Marital status | ||
| Married | 77,551 | (93.5) |
| Single | 2863 | (3.5) |
| Divorced or Widowed | 637 | (0.8) |
| Missing | 1868 | (2.3) |
| Causing stressful events of the past year | ||
| No | 45,771 | (55.2) |
| Yes | 34,271 | (41.3) |
| Missing | 2877 | (3.5) |
| Experience of domestic violence during pregnancy | ||
| No | 68,934 | (83.1) |
| Yes | 11,153 | (13.5) |
| Missing | 2832 | (3.4) |
| Undergoing fertility treatment | ||
| No | 74,479 | (89.8) |
| Yes | 6531 | (7.9) |
| Missing | 1909 | (2.3) |
| Number of pregnancies before current pregnancy | ||
| 0 | 24,334 | (29.3) |
| 1 | 28,093 | (33.9) |
| 2 | 17,093 | (20.6) |
| ≥3 | 12,703 | (15.3) |
| Missing | 696 | (0.8) |
| Experience of miscarriage or stillbirth before current pregnancy | ||
| No | 55,884 | (67.4) |
| Yes | 25,671 | (31.0) |
| Missing | 1364 | (1.6) |
| BMI 1 in the first trimester | ||
| <18.5 | 13,439 | (16.2) |
| 18.5–24.9 | 60,349 | (72.8) |
| 25.0–29.9 | 6359 | (7.7) |
| 30.0–34.9 | 1399 | (1.7) |
| ≥35 | 342 | (0.4) |
| Missing | 1031 | (1.2) |
| BMI in the second to third trimesters | ||
| <18.5 | 2087 | (2.5) |
| 18.5–24.9 | 61,390 | (74.0) |
| 25.0–29.9 | 13,824 | (16.7) |
| 30.0–34.9 | 2256 | (2.7) |
| ≥35 | 433 | (0.5) |
| Missing | 2929 | (3.5) |
| Employment status in the first trimester | ||
| No | 29,362 | (35.4) |
| Yes | 48,785 | (58.8) |
| Missing | 4772 | (5.8) |
| Employment status in the second to third trimesters | ||
| No | 36,788 | (44.4) |
| Yes | 42,189 | (50.9) |
| Missing | 3942 | (4.8) |
| PA Levels before Pregnancy | Categories (min/wk) | Poorer Physical Health in the First Trimester | Poorer Mental Health in the First Trimester | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| OR 1 (95% CI) 2 | AOR 3 (95% CI) | AOR (MI) 4 (95% CI) | OR 1 (95% CI) 2 | AOR 3 (95% CI) | AOR (MI) 4 (95% CI) | ||||||||
| Time spent walking (3.3 METs) | <10 | – | – | – | – | – | – | ||||||
| 10–180 | 1.125 | (1.080–1.172) | 1.079 | (1.031–1.129) | 1.087 | (1.043–1.133) | 0.991 | (0.953–1.030) | 1.033 | (0.989–1.079) | 1.010 | (0.970–1.051) | |
| 180–360 | 1.078 | (1.025–1.134) | 1.026 | (0.970–1.085) | 1.044 | (0.992–1.099) | 0.988 | (0.942–1.037) | 1.020 | (0.967–1.076) | 1.006 | (0.957–1.057) | |
| 360–540 | 0.990 | (0.929–1.054) | 0.956 | (0.892–1.026) | 0.969 | (0.909–1.033) | 0.929 | (0.875–0.988) | 0.976 | (0.912–1.045) | 0.934 | (0.877–0.994) | |
| 540–720 | 1.082 | (0.986–1.186) | 1.064 | (0.962–1.177) | 1.069 | (0.974–1.173) | 0.961 | (0.880–1.050) | 0.960 | (0.872–1.058) | 0.953 | (0.872–1.043) | |
| 720–900 | 0.997 | (0.917–1.083) | 1.029 | (0.938–1.128) | 0.989 | (0.910–1.076) | 0.966 | (0.891–1.048) | 0.989 | (0.904–1.081) | 0.950 | (0.875–1.032) | |
| 900–1080 | 1.030 | (0.960–1.106) | 1.021 | (0.946–1.103) | 1.038 | (0.967–1.115) | 1.079 | (1.007–1.157) | 1.048 | (0.971–1.131) | 1.035 | (0.964–1.111) | |
| 1080–1260 | 1.037 | (0.971–1.107) | 1.042 | (0.970–1.119) | 1.042 | (0.976–1.113) | 1.063 | (0.997–1.133) | 1.040 | (0.970–1.116) | 1.014 | (0.951–1.083) | |
| Time spent on moderate PA 5 (4.0 METs) | <10 | – | – | – | – | – | – | ||||||
| 10–180 | 1.106 | (1.059–1.156) | 1.083 | (1.032–1.136) | 1.100 | (1.053–1.150) | 1.028 | (0.987–1.071) | 1.029 | (0.984–1.077) | 1.041 | (0.998–1.086) | |
| 180–360 | 1.059 | (0.997–1.125) | 1.078 | (1.010–1.152) | 1.081 | (1.018–1.149) | 1.055 | (0.996–1.117) | 1.032 | (0.968–1.099) | 1.055 | (0.995–1.118) | |
| 360–540 | 1.017 | (0.938–1.104) | 1.049 | (0.958–1.147) | 1.051 | (0.968–1.141) | 1.088 | (1.005–1.178) | 1.065 | (0.975–1.164) | 1.071 | (0.988–1.161) | |
| 540–720 | 1.091 | (0.983–1.210) | 1.147 | (1.023–1.285) | 1.121 | (1.010–1.244) | 1.105 | (0.999–1.222) | 1.089 | (0.975–1.216) | 1.080 | (0.975–1.196) | |
| 720–900 | 1.021 | (0.922–1.131) | 1.054 | (0.943–1.179) | 1.076 | (0.970–1.193) | 1.175 | (1.061–1.301) | 1.126 | (1.007–1.260) | 1.126 | (1.015–1.249) | |
| 900–1080 | 1.014 | (0.934–1.101) | 1.007 | (0.922–1.100) | 1.038 | (0.955–1.127) | 1.183 | (1.089–1.285) | 1.105 | (1.010–1.208) | 1.120 | (1.030–1.218) | |
| 1080–1260 | 0.960 | (0.869–1.060) | 1.008 | (0.904–1.124) | 1.005 | (0.910–1.111) | 1.035 | (0.938–1.141) | 0.938 | (0.842–1.046) | 0.971 | (0.878–1.073) | |
| Time spent on vigorous PA 6 (8.0 METs) | <10 | – | – | – | – | – | – | ||||||
| 10–180 | 1.018 | (0.958–1.081) | 0.990 | (0.927–1.057) | 0.988 | (0.930–1.050) | 1.117 | (1.054–1.184) | 1.106 | (1.038–1.178) | 1.087 | (1.025–1.153) | |
| 180–360 | 0.908 | (0.830–0.993) | 0.880 | (0.798–0.970) | 0.897 | (0.819–0.981) | 1.127 | (1.031–1.232) | 1.082 | (0.980–1.193) | 1.072 | (0.979–1.174) | |
| 360–540 | 0.992 | (0.864–1.139) | 0.974 | (0.838–1.133) | 0.996 | (0.867–1.144) | 1.284 | (1.117–1.475) | 1.256 | (1.077–1.466) | 1.218 | (1.057–1.402) | |
| 540–720 | 0.902 | (0.753–1.079) | 0.901 | (0.739–1.099) | 0.914 | (0.763–1.095) | 1.351 | (1.119–1.630) | 1.244 | (1.011–1.531) | 1.247 | (1.031–1.509) | |
| 720–900 | 1.074 | (0.882–1.308) | 1.192 | (0.955–1.486) | 1.161 | (0.952–1.415) | 1.511 | (1.231–1.853) | 1.410 | (1.121–1.774) | 1.376 | (1.118–1.693) | |
| 900–1080 | 0.915 | (0.803–1.043) | 0.948 | (0.821–1.094) | 0.961 | (0.842–1.096) | 1.509 | (1.310–1.739) | 1.364 | (1.167–1.594) | 1.373 | (1.189–1.585) | |
| 1080–1260 | 0.626 | (0.508–0.771) | 0.626 | (0.496–0.789) | 0.672 | (0.545–0.829) | 1.467 | (1.160–1.857) | 1.214 | (0.934–1.580) | 1.239 | (0.976–1.574) | |
| PA Levels during Pregnancy | Categories (min/wk) | Poorer Physical Health in the Second to Third Trimesters | Poorer Mental Health in the Second to Third Trimesters | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| OR 1 (95% CI) 2 | AOR 3 (95% CI) | AOR (MI) 4 (95% CI) | OR 1 (95% CI) 2 | AOR 3 (95% CI) | AOR (MI) 4 (95% CI) | ||||||||
| Time spent walking (3.3 METs) | <10 | – | – | – | – | – | – | ||||||
| 10–180 | 0.968 | (0.929–1.008) | 0.986 | (0.943–1.031) | 0.987 | (0.947–1.029) | 0.919 | (0.887–0.952) | 0.933 | (0.897–0.970) | 0.932 | (0.899–0.967) | |
| 180–360 | 0.888 | (0.845–0.933) | 0.911 | (0.863–0.962) | 0.912 | (0.868–0.959) | 0.859 | (0.822–0.897) | 0.885 | (0.843–0.929) | 0.866 | (0.828–0.906) | |
| 360–540 | 0.886 | (0.831–0.944) | 0.920 | (0.857–0.987) | 0.914 | (0.857–0.975) | 0.880 | (0.831–0.931) | 0.881 | (0.827–0.938) | 0.878 | (0.829–0.931) | |
| 540–720 | 0.840 | (0.765–0.922) | 0.863 | (0.780–0.956) | 0.858 | (0.782–0.942) | 0.905 | (0.833–0.983) | 0.884 | (0.806–0.969) | 0.888 | (0.816–0.967) | |
| 720–900 | 0.854 | (0.778–0.937) | 0.861 | (0.778–0.954) | 0.866 | (0.789–0.952) | 0.899 | (0.827–0.976) | 0.850 | (0.775–0.932) | 0.855 | (0.786–0.932) | |
| 900–1080 | 0.931 | (0.852–1.017) | 0.943 | (0.855–1.039) | 0.917 | (0.839–1.003) | 0.976 | (0.903–1.055) | 0.982 | (0.901–1.070) | 0.964 | (0.890–1.045) | |
| 1080–1260 | 0.881 | (0.811–0.957) | 0.868 | (0.793–0.950) | 0.876 | (0.806–0.952) | 0.958 | (0.890–1.032) | 0.923 | (0.851–1.002) | 0.948 | (0.879–1.022) | |
| Time spent on moderate PA 5 (4.0 METs) | <10 | - | - | - | - | - | - | ||||||
| 10–180 | 1.003 | (0.951–1.058) | 0.990 | (0.934–1.049) | 0.987 | (0.935–1.042) | 1.017 | (0.970–1.065) | 0.983 | (0.933–1.035) | 0.983 | (0.937–1.031) | |
| 180–360 | 0.966 | (0.892–1.046) | 0.952 | (0.873–1.037) | 0.961 | (0.887–1.041) | 1.151 | (1.072–1.236) | 1.086 | (1.004–1.174) | 1.094 | (1.018–1.177) | |
| 360–540 | 1.046 | (0.937–1.167) | 1.074 | (0.952–1.211) | 1.051 | (0.941–1.173) | 1.098 | (0.997–1.208) | 0.997 | (0.897–1.109) | 1.008 | (0.914–1.112) | |
| 540–720 | 1.142 | (0.995–1.312) | 1.106 | (0.953–1.283) | 1.136 | (0.988–1.305) | 1.182 | (1.050–1.332) | 1.163 | (1.020–1.326) | 1.123 | (0.994–1.268) | |
| 720–900 | 1.147 | (1.001–1.315) | 1.129 | (0.974–1.308) | 1.137 | (0.991–1.305) | 1.088 | (0.968–1.223) | 1.015 | (0.892–1.154) | 0.990 | (0.877–1.116) | |
| 900–1080 | 1.092 | (0.975–1.224) | 1.061 | (0.938–1.200) | 1.053 | (0.940–1.181) | 1.138 | (1.031–1.256) | 1.059 | (0.950–1.180) | 1.069 | (0.966–1.183) | |
| 1080–1260 | 1.008 | (0.884–1.149) | 1.025 | (0.888–1.183) | 1.010 | (0.885–1.153) | 1.372 | (1.218–1.544) | 1.242 | (1.090–1.416) | 1.226 | (1.085–1.384) | |
| Time spent on vigorous PA 6 (8.0 METs) | <10 | - | - | - | - | - | - | ||||||
| 10–180 | 0.919 | (0.809–1.044) | 0.914 | (0.795–1.051) | 0.923 | (0.812–1.050) | 1.409 | (1.254–1.583) | 1.250 | (1.099–1.423) | 1.224 | (1.086–1.379) | |
| 180–360 | 1.073 | (0.842–1.368) | 1.208 | (0.920–1.585) | 1.110 | (0.870–1.417) | 1.469 | (1.184–1.822) | 1.270 | (0.999–1.616) | 1.271 | (1.019–1.585) | |
| 360–540 | 1.135 | (0.802–1.606) | 1.150 | (0.785–1.684) | 1.138 | (0.805–1.610) | 1.648 | (1.210–2.244) | 1.341 | (0.951–1.892) | 1.350 | (0.982–1.856) | |
| 540–720 | 0.905 | (0.636–1.288) | 0.939 | (0.641–1.375) | 0.921 | (0.647–1.311) | 1.734 | (1.242–2.421) | 1.497 | (1.040–2.153) | 1.490 | (1.065–2.085) | |
| 720–900 | 1.173 | (0.798–1.725) | 1.101 | (0.726–1.670) | 1.211 | (0.823–1.783) | 1.881 | (1.329–2.664) | 1.585 | (1.077–2.332) | 1.749 | (1.226–2.497) | |
| 900–1080 | 0.959 | (0.707–1.302) | 0.934 | (0.669–1.302) | 0.979 | (0.720–1.331) | 1.737 | (1.305–2.312) | 1.501 | (1.093–2.061) | 1.488 | (1.110–1.994) | |
| 1080–1260 | 0.699 | (0.422–1.160) | 0.732 | (0.407–1.315) | 0.700 | (0.421–1.166) | 2.179 | (1.268–3.747) | 1.550 | (0.844–2.847) | 1.873 | (1.076–3.261) | |
| Change in PA Levels 1 | Difference in PA Levels 2 (MET-min/wk) | Poorer Physical Health in the Second to Third Trimesters | Poorer Mental Health in the Second to Third Trimesters | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| OR 3 (95% CI) 4 | AOR 5 (95% CI) | AOR (MI) 6 (95% CI) | OR 3 (95% CI) 4 | AOR 5 (95% CI) | AOR (MI) 6 (95% CI) | ||||||||
| No Change | ±0.5 SD (−1945.5–486.8) | – | – | – | – | – | – | ||||||
| Increased | 0.5–1.0 SD (486.8–1703.0) | 0.891 | (0.845–0.940) | 0.910 | (0.859–0.963) | 0.906 | (0.859–0.955) | 0.971 | (0.926–1.017) | 0.953 | (0.905–1.004) | 0.944 | (0.899–0.990) |
| 1.0–1.5 SD (1703.0–2919.2) | 0.891 | (0.815–0.973) | 0.882 | (0.801–0.972) | 0.887 | (0.811–0.969) | 1.186 | (1.095–1.284) | 1.047 | (0.958–1.143) | 1.100 | (1.013–1.194) | |
| 1.5–2.0 SD (2919.2–4135.4) | 0.996 | (0.889–1.117) | 1.029 | (0.908–1.167) | 0.978 | (0.871–1.097) | 1.157 | (1.047–1.278) | 1.076 | (0.964–1.202) | 1.073 | (0.969–1.189) | |
| ≥2.0 SD (≥4135.4) | 0.901 | (0.796–1.019) | 0.909 | (0.794–1.041) | 0.903 | (0.797–1.022) | 1.503 | (1.342–1.684) | 1.225 | (1.081–1.388) | 1.313 | (1.169–1.473) | |
| Decreased | −0.5–−1.0 SD (−1945.5–−3161.7) | 1.080 | (1.014–1.149) | 1.119 | (1.046–1.198) | 1.106 | (1.039–1.178) | 1.124 | (1.065–1.186) | 1.076 | (1.014–1.141) | 1.070 | (1.013–1.131) |
| −1.0–−1.5 SD (−3161.7–−4377.9) | 1.065 | (0.987–1.150) | 1.092 | (1.005–1.188) | 1.102 | (1.021–1.190) | 1.192 | (1.116–1.273) | 1.125 | (1.046–1.211) | 1.115 | (1.042–1.193) | |
| −1.5–−2.0 SD (−4377.9–−5594.1) | 1.116 | (0.997–1.248) | 1.246 | (1.099–1.412) | 1.162 | (1.039–1.301) | 1.260 | (1.145–1.386) | 1.128 | (1.013–1.255) | 1.150 | (1.042–1.269) | |
| ≤−2.0 SD (≤−5594.1) | 1.010 | (0.933–1.094) | 1.142 | (1.044–1.249) | 1.100 | (1.015–1.193) | 1.553 | (1.447–1.668) | 1.303 | (1.202–1.412) | 1.333 | (1.239–1.435) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yamada, Y.; Ebara, T.; Matsuki, T.; Kano, H.; Tamada, H.; Kato, S.; Sato, H.; Sugiura-Ogasawara, M.; Saitoh, S.; Kamijima, M.; et al. Relationship between Physical Activity and Physical and Mental Health Status in Pregnant Women: A Prospective Cohort Study of the Japan Environment and Children’s Study. Int. J. Environ. Res. Public Health 2021, 18, 11373. https://doi.org/10.3390/ijerph182111373
Yamada Y, Ebara T, Matsuki T, Kano H, Tamada H, Kato S, Sato H, Sugiura-Ogasawara M, Saitoh S, Kamijima M, et al. Relationship between Physical Activity and Physical and Mental Health Status in Pregnant Women: A Prospective Cohort Study of the Japan Environment and Children’s Study. International Journal of Environmental Research and Public Health. 2021; 18(21):11373. https://doi.org/10.3390/ijerph182111373
Chicago/Turabian StyleYamada, Yasuyuki, Takeshi Ebara, Taro Matsuki, Hirohisa Kano, Hazuki Tamada, Sayaka Kato, Hirotaka Sato, Mayumi Sugiura-Ogasawara, Shinji Saitoh, Michihiro Kamijima, and et al. 2021. "Relationship between Physical Activity and Physical and Mental Health Status in Pregnant Women: A Prospective Cohort Study of the Japan Environment and Children’s Study" International Journal of Environmental Research and Public Health 18, no. 21: 11373. https://doi.org/10.3390/ijerph182111373
APA StyleYamada, Y., Ebara, T., Matsuki, T., Kano, H., Tamada, H., Kato, S., Sato, H., Sugiura-Ogasawara, M., Saitoh, S., Kamijima, M., & on behalf of the Japan Environment and Children’s Study (JECS) Group. (2021). Relationship between Physical Activity and Physical and Mental Health Status in Pregnant Women: A Prospective Cohort Study of the Japan Environment and Children’s Study. International Journal of Environmental Research and Public Health, 18(21), 11373. https://doi.org/10.3390/ijerph182111373