
Assessment of Retrospective COVID-19 Spatial Clusters with Respect to Demographic Factors: Case Study of Kansas City, Missouri, United States



Abstract
:1. Introduction
2. Materials and Methods
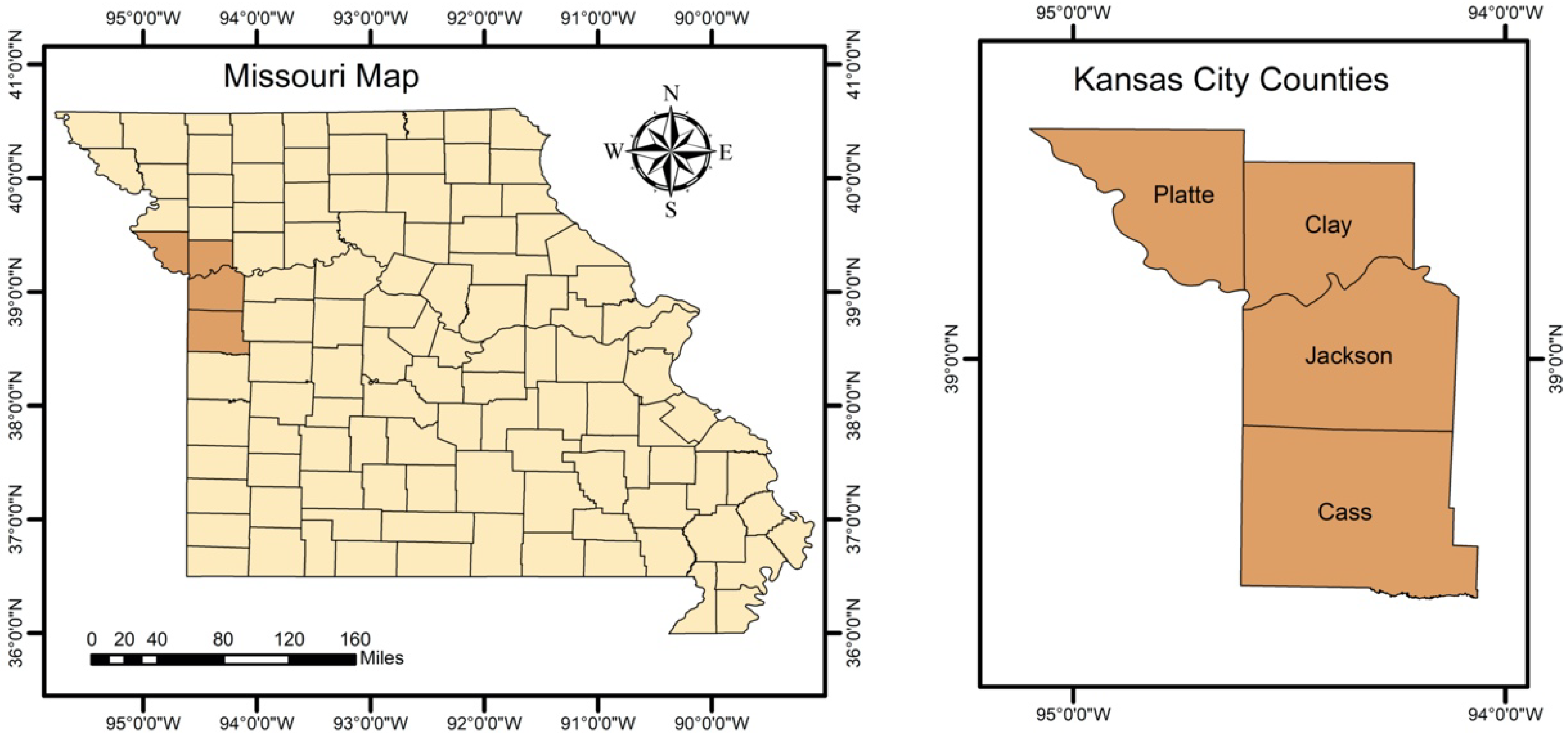
2.1. Study Area
2.2. Data Source
2.3. Methods
2.3.1. Statistical Analysis
2.3.2. Cluster Analysis
3. Results
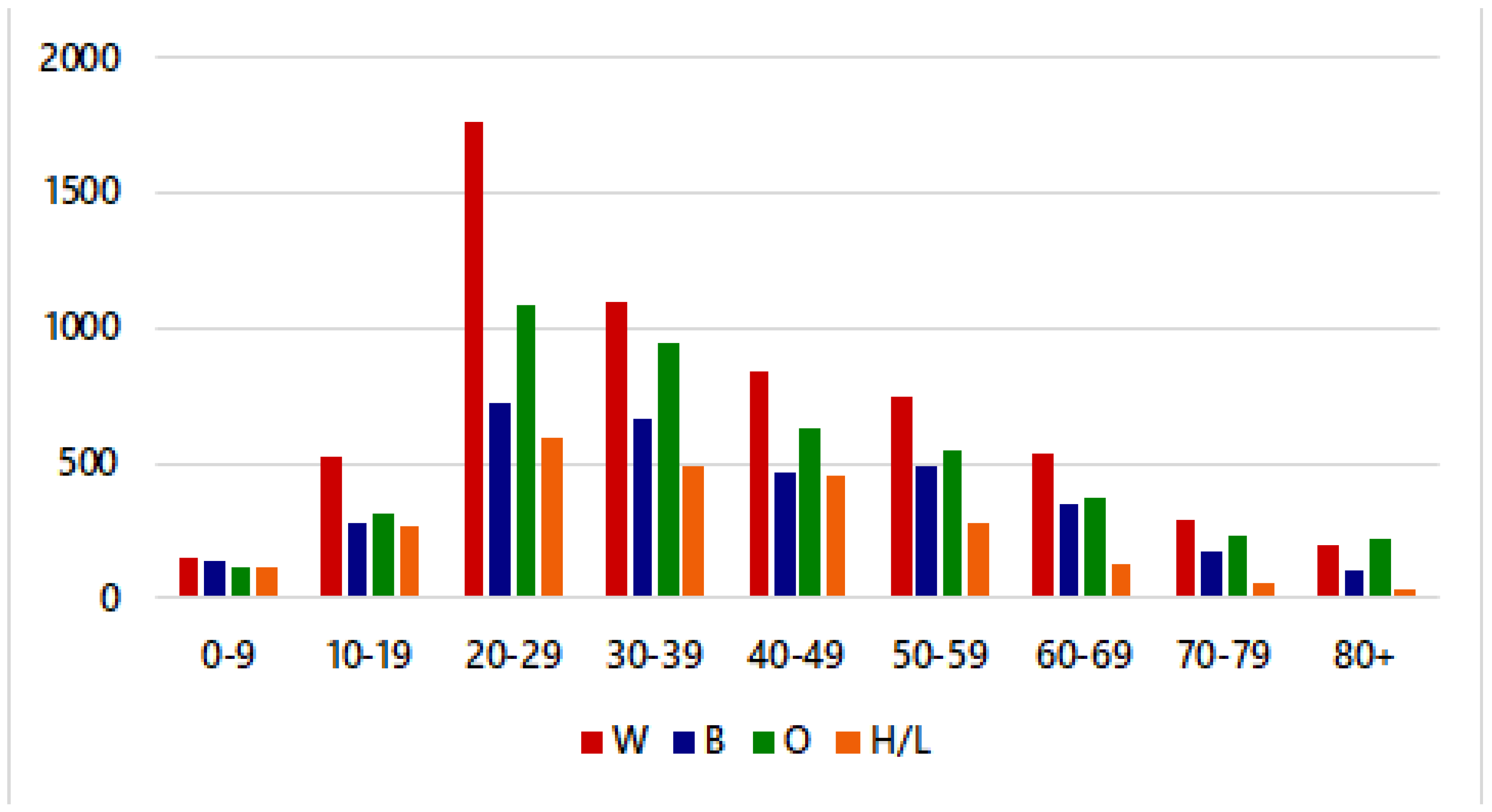
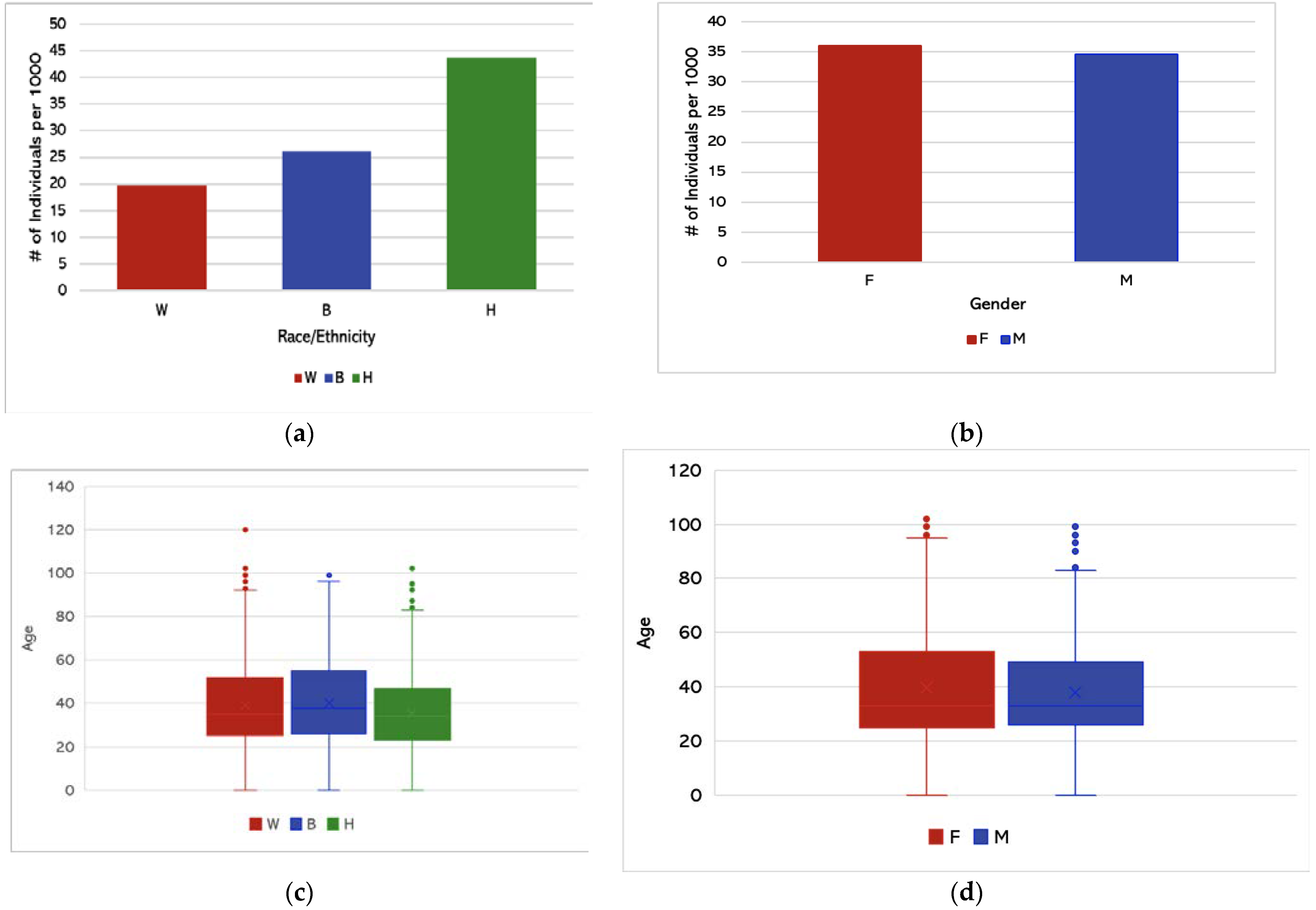
3.1. Descriptive Statistics
3.2. Hypothesis Testing
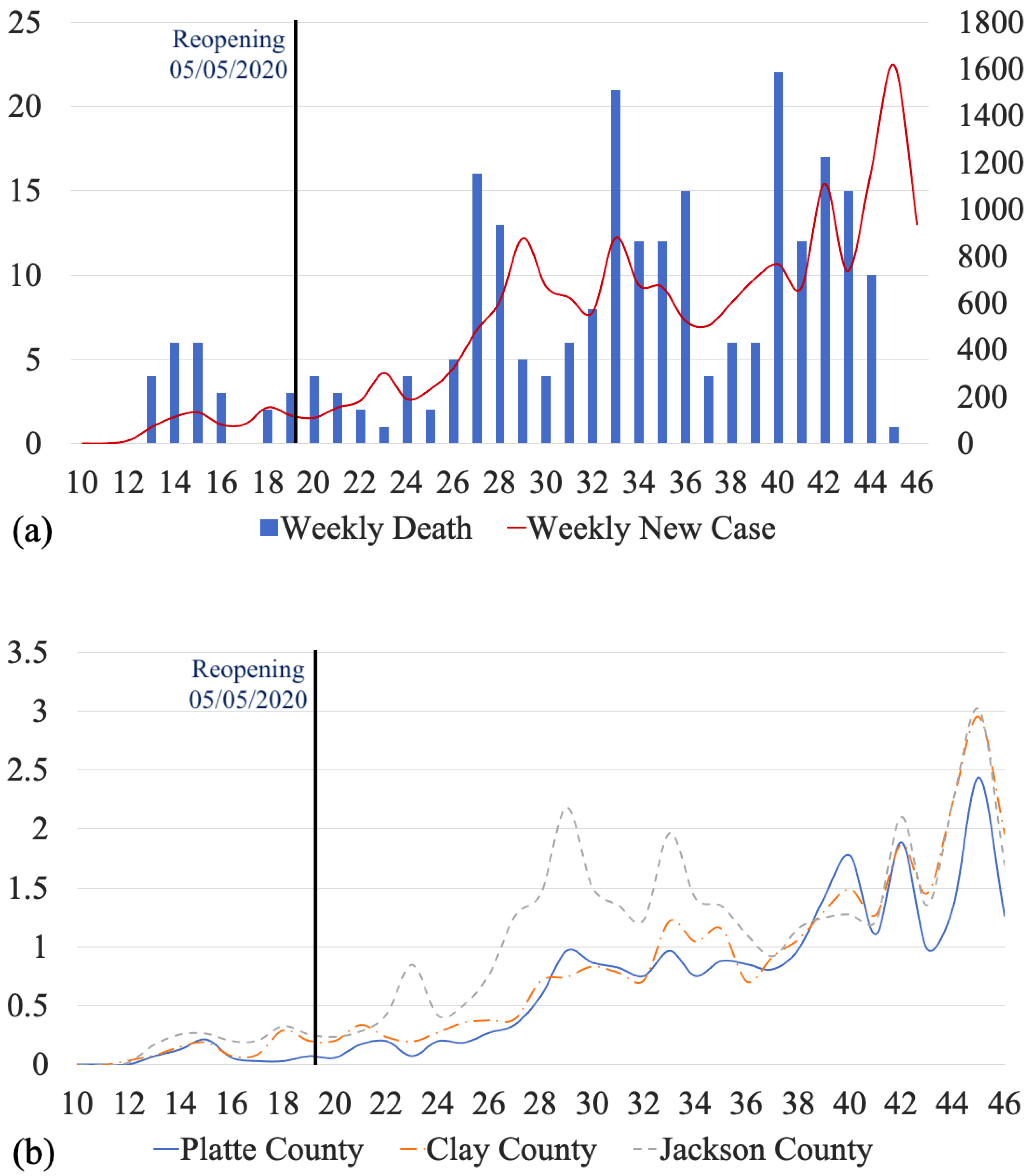
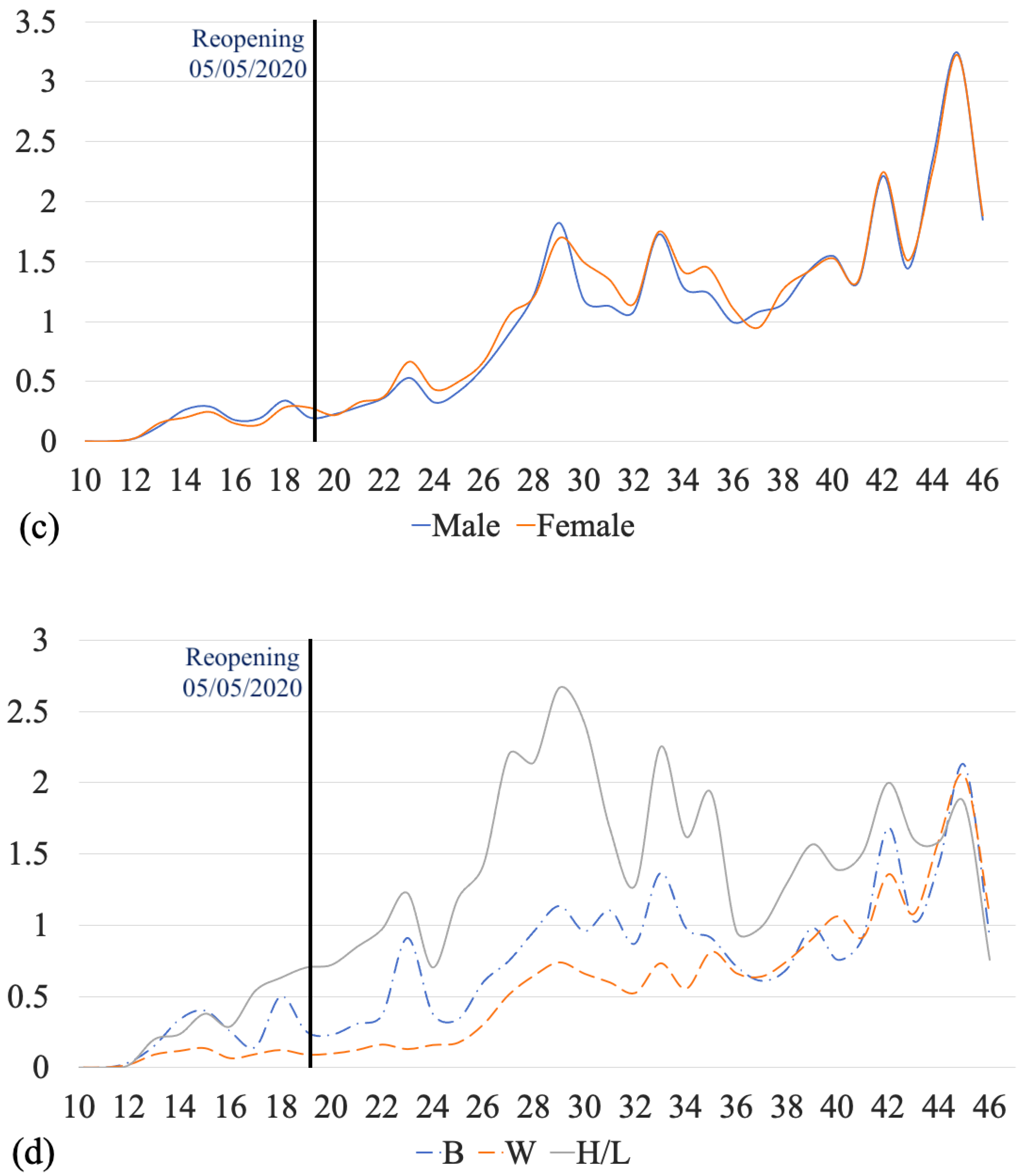
3.3. Times-Series Analysis
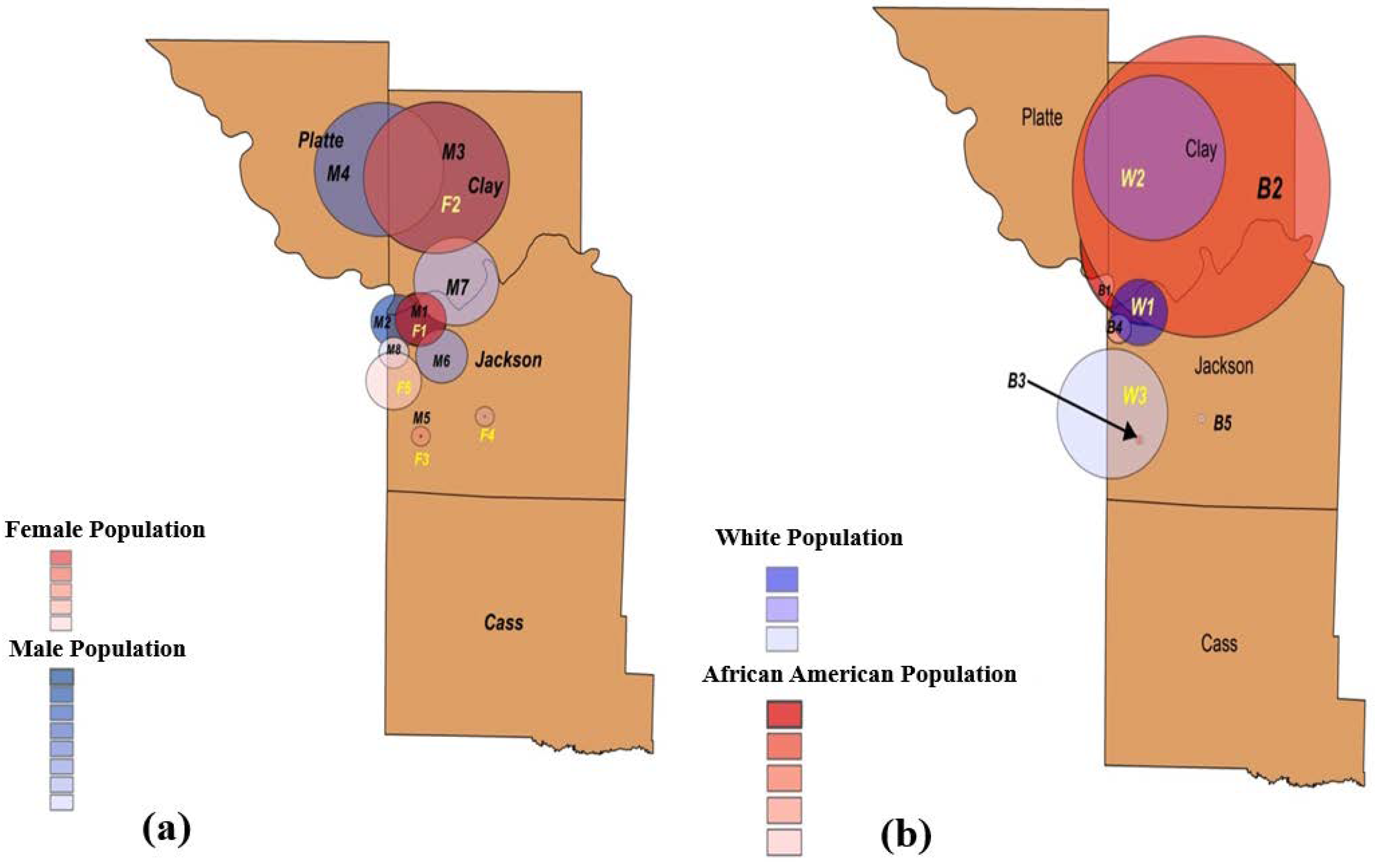
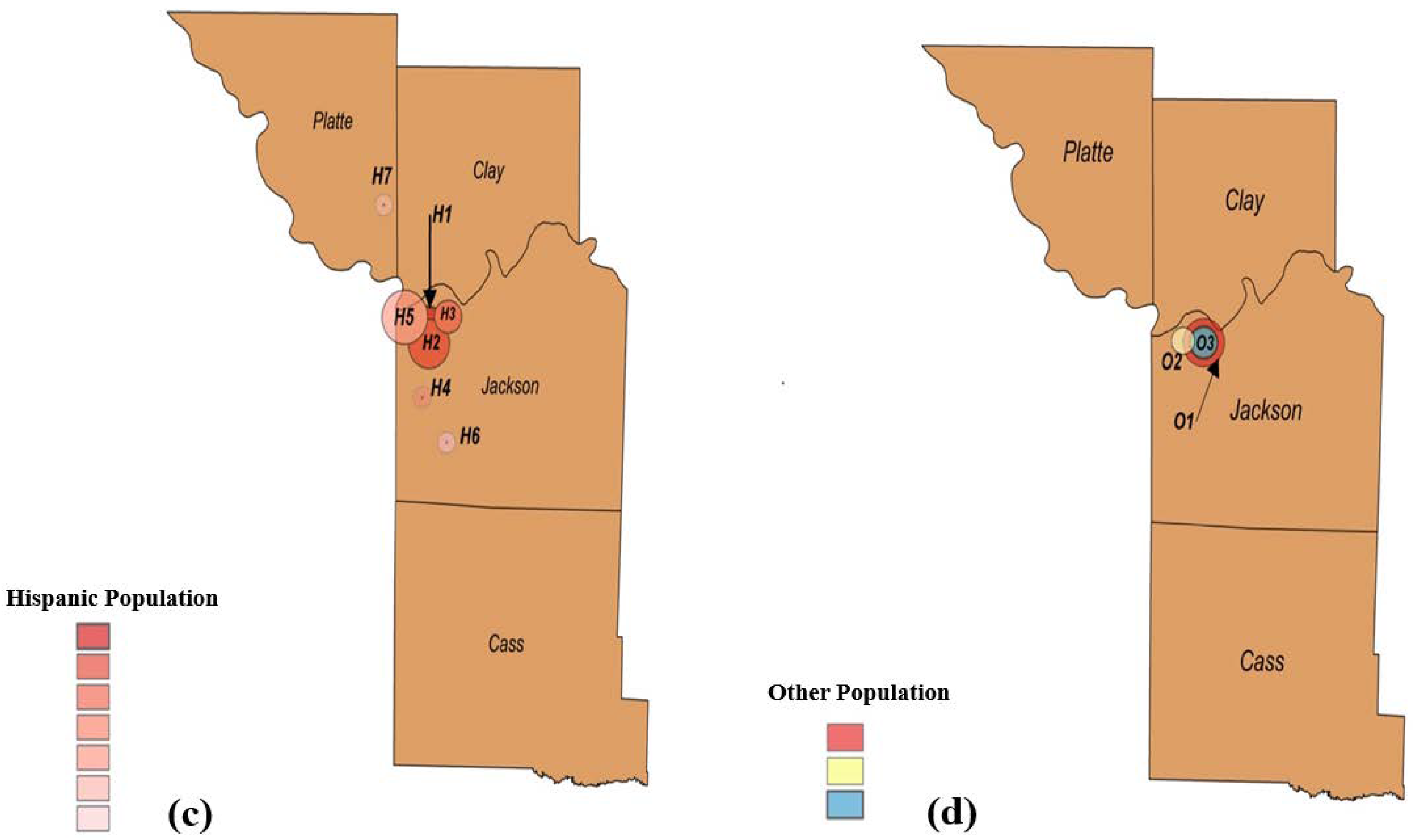
3.4. Cluster Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Centers of Disease Control and Prevention. Symptoms of COVID-19. 2021. Available online: https://www.cdc.gov/coronavirus/2019-ncov/symptoms-testing/symptoms.html (accessed on 14 July 2021).
- Shi, Y.; Wang, G.; Cai, X.-P.; Deng, J.-W.; Zheng, L.; Zhu, H.-H.; Zheng, M.; Yang, B.; Chen, Z. An overview of COVID-19. J. Zhejiang Univ. Sci. B 2020, 21, 343–360. [Google Scholar] [CrossRef]
- Centers of Disease Control and Prevention. How COVID-19 Spreads. 2021. Available online: https://www.cdc.gov/coronavirus/2019-ncov/prevent-getting-sick/how-covid-spreads.html (accessed on 14 July 2021).
- Patel, A.; Jernigan, D.B.; Abdirizak, F. Initial public health response and interim clinical guidance for the 2019 novel coronavirus outbreak—United States, 31 December 2019–4 February 2020. Arab. Archaeol. Epigr. 2019, 20, 889–895. [Google Scholar] [CrossRef]
- Culp, W.C. Coronavirus Disease 2019. A&a Pract. 2020, 14, e01218. [Google Scholar]
- Miller, I.F.; Becker, A.D.; Grenfell, B.T.; Metcalf, C.J.E. Disease and healthcare burden of COVID-19 in the United States. Nat. Med. 2020, 26, 1212–1217. [Google Scholar] [CrossRef]
- Patton, M. The Impact Of Covid-19 On U.S. Economy and Financial Markets. 2020. Available online: https://www.forbes.com/sites/mikepatton/2020/10/12/the-impact-of-covid-19-on-us-economy-and-financial-markets/?sh=7f88fad62d20 (accessed on 8 June 2021).
- Sharif, A.; Aloui, C.; Yarovaya, L. COVID-19 pandemic, oil prices, stock market, geopolitical risk and policy uncertainty nexus in the US economy: Fresh evidence from the wavelet-based approach. Int. Rev. Financ. Anal. 2020, 70, 101496. [Google Scholar] [CrossRef]
- Erwin, P.C.; Mucheck, K.W.; Brownson, R.C. Different Responses to COVID-19 in Four US States: Washington, New York, Missouri, and Alabama. Am. J. Public Health 2021, 111, 647–651. [Google Scholar] [CrossRef] [PubMed]
- Vasquez Reyes, M. The Disproportional Impact of COVID-19 on African Americans. Health Hum. Rights 2020, 22, 299–307. [Google Scholar]
- Tai, D.B.G.; Shah, A.; Doubeni, C.A.; Sia, I.G.; Wieland, M.L. The Disproportionate Impact of COVID-19 on Racial and Ethnic Minorities in the United States. Clin. Infect. Dis. 2021, 72, 703–706. [Google Scholar] [CrossRef] [PubMed]
- U.S. Census Bureau. U.S. Census Bureau, Kansas City. 2020. Available online: https://www.census.gov/quickfacts/kansascitycitymissouri (accessed on 31 October 2021).
- Centers of Disease Control and Prevention. Basics of COVID-19. 2021. Available online: https://www.cdc.gov/coronavirus/2019-ncov/your-health/about-covid-19/basics-covid-19.html?CDC_AA_refVal=https%3A%2F%2Fwww.cdc.gov%2Fcoronavirus%2F2019-ncov%2Fcdcresponse%2Fabout-COVID-19.html (accessed on 14 July 2021).
- Centers of Disease Control and Prevention. Introduction to COVID-19 Racial and Ethnic Health Disparities. 2021. Available online: https://www.cdc.gov/coronavirus/2019-ncov/community/health-equity/racial-ethnic-disparities/index.html (accessed on 20 July 2021).
- Centers of Disease Control and Prevention. Disparities in COVID-19-Associated Hospitalizations. 2021. Available online: https://www.cdc.gov/coronavirus/2019-ncov/community/health-equity/racial-ethnic-disparities/disparities-hospitalization.html (accessed on 20 July 2021).
- Kansas City Health Department. KCMO Coronavirus Activity Timeline. 2020. Available online: https://www.kshb.com/news/coronavirus/kansas-city-missouri-makes-list-of-cities-named-possible-covid-19-hot-spots (accessed on 8 July 2021).
- James, E. Kansas City, Missouri, Makes List of Cities Named Possible COVID-19 Hot Spots. 2020. Available online: https://www.kshb.com/news/coronavirus/kansas-city- (accessed on 8 June 2021).
- Kansas City Health Department. Kansas City COVID-19 Information Center. 2021. Available online: https://kcmo.maps.arcgis.com/apps/dashboards/a9cb1fa166aa44de99dab0b946b08799 (accessed on 8 July 2021).
- Burton, M.; Satterwhite, L.; Shi, X.; Allen, A.; Castro, M. Hospital Collaboration in Response to the COVID-19 Pandemic in Kansas City Metropolitan Region. Kans. J. Med. 2021, 14, 108–110. [Google Scholar] [CrossRef]
- Dalla, S.; Bacon, B.; Ayres, J.M.; Holmstead, S.; Elliot, A.J.A. 3D-printed N95 equivalent for personal protective equipment shortages: The Kansas City Mask. J. 3D Print. Med. 2020, 4, 211–217. [Google Scholar] [CrossRef]
- Dalla, S.; Shinde, R.; Ayres, J.; Waller, S.; Nachtigal, J. 3D-printed snorkel mask adapter for failed N95 fit tests and personal protective equipment shortages. J. 3D Print. Med. 2020, 4, 203–209. [Google Scholar] [CrossRef]
- Billings, S.; Englin, E.; Hall, J.; Smith, A. Adaptation of delivery of SCCP clinical pharmacist roundtable event using a virtual platform due to COVID. J. Am. Coll. Clin. Pharm. 2020, 3, 1658–1659. [Google Scholar]
- Dokken, D.; Ahmann, E. Mental Health Needs during COVID-19: Responses in Pediatric Health Care. Pediatric Nurs. 2020, 46, 304–307. [Google Scholar]
- Ginther, D.K.; Zambrana, C. Association of Mask Mandates and COVID-19 Case Rates, Hospitalizations, and Deaths in Kansas. JAMA Netw. Open 2021, 4, e2114514. [Google Scholar] [CrossRef]
- Framme, C.; Gottschling, J.; Buley, P.; Rohwer-Mensching, K.; Junker, B.; Dittberner, M.; Volkmann, I. Einfluss des COVID-19-Shutdowns auf die Arbeitsleistung einer Universitäts-Augenpoliklinik. Der Ophthalmol. 2021, 118, 1–11. [Google Scholar] [CrossRef]
- Practice Notes from the AAAI. J. Allergy Clin. Immunol. Pract. 2021, 9, A43–A45. [CrossRef]
- Mody, A.; Pfeifauf, K.; Bradley, C.; Fox, B.; Hlatshwayo, M.G.; Ross, W.; Sanders-Thompson, V.; Maddox, K.J.; Reidhead, M.; Schootman, M.; et al. Understanding Drivers of Coronavirus Disease 2019 (COVID-19) Racial Disparities: A Population-Level Analysis of COVID-19 Testing Among Black and White Populations. Clin. Infect. Dis. 2020, 27. [Google Scholar] [CrossRef]
- Ramprasad, A.; Qureshi, F.; Jones, B.J.L. Contributions to Health Disparities Observed in the COVID19 Pandemic. J. Natl. Med. Assoc. 2020, 112, S13–S14. [Google Scholar] [CrossRef]
- Kulldorff, M.; Nagarwalla, N. Spatial disease clusters: Detection and inference. Stat. Med. 1995, 14, 799–810. [Google Scholar] [CrossRef] [PubMed]
- Feng, T. Spatial and Temporal Patterns of Primary Syphilis and Secondary Syphilis in Shenzhen, China; Hu, Y., Ed.; IntechOpen: Rijeka, Croatia, 2011; p. 5. [Google Scholar]
- Shunxiang, C.; Cai, S.; Zhang, H.; Lin, W.; Fan, Y.; Qiu, J.; Sun, L.; Chang, B.; Zhang, Z.; Nie, S. Spatial, temporal, and spatiotemporal analysis of malaria in Hubei Province, China from 2004–2011. Malar. J. 2015, 14, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.; Qiu, Y.; Yang, R.; Li, L.; Hou, J.; Lu, K.; Xu, L. The characteristics of spatial-temporal distribution and cluster of tuberculosis in Yunnan Province, China, 2005–2018. BMC Public Health 2019, 19, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Talbot, T.; Kumar, S.; Kulldorff, M. The Bernoulli Spatial Scan Statistic for Birth Defect Data. 2015. Available online: https://www.satscan.org/tutorials/nysbirthdefect/SaTScanTutorialNYSBirthDefect.pdf (accessed on 3 March 2021).
- Coleman, M.; Coleman, M.; Mabuza, A.M.; Kok, G.; Coetzee, M.; Durrheim, D.N. Using the SaTScan method to detect local malaria clusters for guiding malaria control programmes. Malar. J. 2009, 8, 68. [Google Scholar] [CrossRef] [Green Version]
- Sandall, S. EpiTrax User Guide. 2019. Available online: https://clphs.health.mo.gov/lphs/diseaseprevention/epitrax/pdf/user-guide.pdf (accessed on 3 March 2021).
- US Zip code Organization. United States Zip Code 2020. Available online: https://www.unitedstateszipcodes.org/ (accessed on 3 March 2021).
- Kulldorff, M.; Feuer, E.J.; Miller, B.A.; Freedma, L.S. Breast Cancer Clusters in the Northeast United States: A Geographic Analysis. Am. J. Epidemiol. 1997, 146, 161–170. [Google Scholar] [CrossRef]
- Kulldorff, M. Prospective time periodic geographical disease surveillance using a scan statistic. J. R. Stat. Soc. Ser. A Soc. 2001, 164, 61–72. [Google Scholar] [CrossRef]
- Xu, B.; Madden, M.; Stallknecht, D.E.; Hodler, T.W.; Parker, K.C. Spatial and spatial-temporal clustering analysis of hemorrhagic disease in white-tailed deer in the southeastern USA: 1980–2003. Prev. Vet. Med. 2012, 106, 339–347. [Google Scholar] [CrossRef] [PubMed]
- Araújo, M.P.D.; Nunes, V.M.D.A.; Costa, L.D.A.; de Souza, T.A.; Torres, G.D.V.; Nobre, T.T.X. Health conditions of potential risk for severe Covid-19 in institutionalized elderly people. PLoS ONE 2021, 16, e0245432. [Google Scholar] [CrossRef]
- Mueller, A.L.; McNamara, M.S.; Sinclair, D.A. Why does COVID-19 disproportionately affect older people? Aging 2020, 12, 9959–9981. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Minimum | Maximum | Mean | Median | STD | Range | |
|---|---|---|---|---|---|---|
| Cases | 13 | 1618 | 504.29 | 524 | 375.74 | 1605 |
| Deaths | 0 | 22 | 7.14 | 5 | 6.06 | 22 |
| Group | Count | Sum | Average | Variance | ||
|---|---|---|---|---|---|---|
| White | 6142 | 240,691 | 39.1877 | 365.1475 | ||
| African American | 3384 | 136,436 | 40.3179 | 384.2199 | ||
| Hispanic | 2429 | 86,656 | 35.6756 | 293.8412 | ||
| Source of Variation | SS | Df | MS | F | p-Value | F Crit |
| Between Groups | 32,432.19 | 2 | 16,216.1 | 45.5431 | 0 | 2.9965 |
| Within Groups | 4,255,633 | 11,952 | 356.0603 | |||
| Total | 4,288,065 | 11,954 | ||||
| W vs. B | B vs. H | H vs. W | |
|---|---|---|---|
| P (T ≤ t) two-tail | 0.00637 | 1.07657 × 10−20 | 3.62 × 10−15 |
| Bonferroni correction | 0.016667 | 0.016667 | 0.016667 |
| p < 0.01267 | True | True | True |
| Cluster | RR | Observed | Expected | Counties | # of Zip Codes | p-Value |
|---|---|---|---|---|---|---|
| Cluster F1 | 2.21 | 1907 | 973.51 | Jackson County | 9 | 1 × 10−17 |
| Cluster F2 | 1.41 | 1421 | 1052.37 | Platte County Clay County | 11 | 1 × 10−17 |
| Cluster F3 | 1.52 | 253 | 168.1 | Jackson County | 1 | 1.2 × 10−7 |
| Cluster F4 | 2.1 | 58 | 27.75 | Jackson County | 1 | 6.4 × 10−5 |
| Cluster F5 | 1.11 | 1913 | 1757.07 | Jackson County | 7 | 4 × 10−3 |
| Cluster M1 | 2.28 | 1848 | 926.56 | Jackson County | 9 | 1 × 10−17 |
| Cluster M2 | 2.18 | 1357 | 682.73 | Jackson County | 7 | 1 × 10−17 |
| Cluster M3 | 1.32 | 1195 | 937.12 | Platte County Clay County | 11 | 2.3 × 10−15 |
| Cluster M4 | 1.34 | 858 | 656.17 | Platte County | 8 | 1.1 × 10−12 |
| Cluster M5 | 1.56 | 220 | 142.81 | Jackson County | 1 | 2.8 × 10−7 |
| Cluster M6 | 1.27 | 472 | 376.74 | Jackson County | 3 | 1.7 × 10−4 |
| Cluster M7 | 1.18 | 942 | 810.54 | Clay CountyJackson County | 7 | 2.5 × 10−4 |
| Cluster M8 | 1.19 | 625 | 530.56 | Jackson County | 3 | 3.8 × 10−3 |
| Cluster | RR | Observed | Expected | Counties | # of Zip Codes | p-Value |
|---|---|---|---|---|---|---|
| Cluster W1 | 3.78 | 1247 | 388.13 | Jackson County | 11 | 1 × 10−17 |
| Cluster W2 | 1.74 | 1271 | 801.10 | Clay County Platte County | 11 | 1 × 10−17 |
| Cluster W3 | 1.38 | 1708 | 1342.82 | Jackson County | 13 | 1 × 10−17 |
| Cluster B1 | 1.89 | 798 | 474.39 | Clay County Platte County Jackson County | 18 | 1 × 10−17 |
| Cluster B2 | 1.97 | 681 | 383.40 | Clay County Platte County Jackson County | 23 | 1 × 10−17 |
| Cluster B3 | 1.62 | 113 | 70.84 | Jackson County | 1 | 2.6 × 10−4 |
| Cluster B4 | 1.64 | 85 | 52.45 | Jackson County | 3 | 2.4 × 10−3 |
| Cluster B5 | 2.88 | 18 | 6.27 | Jackson County | 1 | 0.012 |
| Cluster | RR | Observed | Expected | Counties | # of Zip Codes | p-Value |
|---|---|---|---|---|---|---|
| Cluster H1 | 2.16 | 985 | 583.41 | Jackson County | 5 | 1 × 10−17 |
| Cluster H2 | 2.17 | 516 | 268.92 | Jackson County | 5 | 1 × 10−17 |
| Cluster H3 | 1.76 | 505 | 315.69 | Jackson County | 3 | 1 × 10−17 |
| Cluster H4 | 4.77 | 61 | 13.06 | Jackson County | 1 | 1 × 10−17 |
| Cluster H5 | 1.69 | 467 | 300.60 | Jackson County | 6 | 1 × 10−17 |
| Cluster H6 | 1.90 | 95 | 50.85 | Jackson County | 1 | 2.4 × 10−6 |
| Cluster H7 | 2.39 | 47 | 19.86 | Platte County | 1 | 1.9 × 10−5 |
| Cluster O1 | 2.61 | 116 | 53.83 | Jackson County | 4 | 1.1 × 10−14 |
| Cluster O2 | 2.38 | 57 | 26.08 | Jackson County | 1 | 1.8 × 10−6 |
| Cluster O3 | 2.31 | 59 | 27.76 | Jackson County | 3 | 2.6 × 10−6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
AlQadi, H.; Bani-Yaghoub, M.; Balakumar, S.; Wu, S.; Francisco, A. Assessment of Retrospective COVID-19 Spatial Clusters with Respect to Demographic Factors: Case Study of Kansas City, Missouri, United States. Int. J. Environ. Res. Public Health 2021, 18, 11496. https://doi.org/10.3390/ijerph182111496
AlQadi H, Bani-Yaghoub M, Balakumar S, Wu S, Francisco A. Assessment of Retrospective COVID-19 Spatial Clusters with Respect to Demographic Factors: Case Study of Kansas City, Missouri, United States. International Journal of Environmental Research and Public Health. 2021; 18(21):11496. https://doi.org/10.3390/ijerph182111496
Chicago/Turabian StyleAlQadi, Hadeel, Majid Bani-Yaghoub, Sindhu Balakumar, Siqi Wu, and Alex Francisco. 2021. "Assessment of Retrospective COVID-19 Spatial Clusters with Respect to Demographic Factors: Case Study of Kansas City, Missouri, United States" International Journal of Environmental Research and Public Health 18, no. 21: 11496. https://doi.org/10.3390/ijerph182111496
APA StyleAlQadi, H., Bani-Yaghoub, M., Balakumar, S., Wu, S., & Francisco, A. (2021). Assessment of Retrospective COVID-19 Spatial Clusters with Respect to Demographic Factors: Case Study of Kansas City, Missouri, United States. International Journal of Environmental Research and Public Health, 18(21), 11496. https://doi.org/10.3390/ijerph182111496