
Four-Year Trajectories of Health-Related Quality of Life in People Living with HIV: Impact of Unmet Basic Needs across Age Groups in Positive Spaces, Healthy Places

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Positive Spaces, Healthy Places (PSHP) Cohort
2.2. Sample and Data Analyses
2.3. Measures
2.4. Statistical Analysis
3. Results
3.1. Sample Characteristics
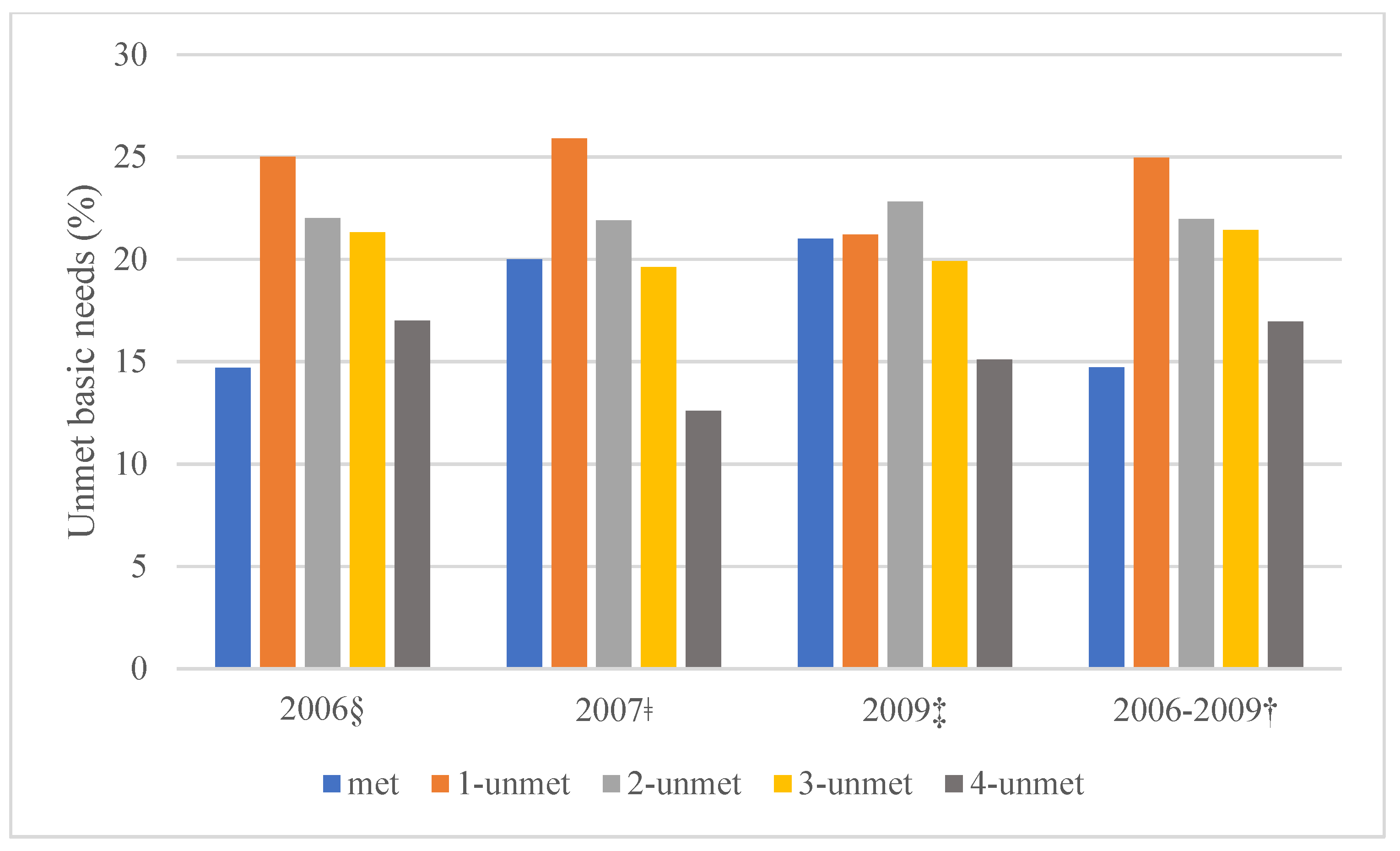
3.2. Unmet Basic Needs
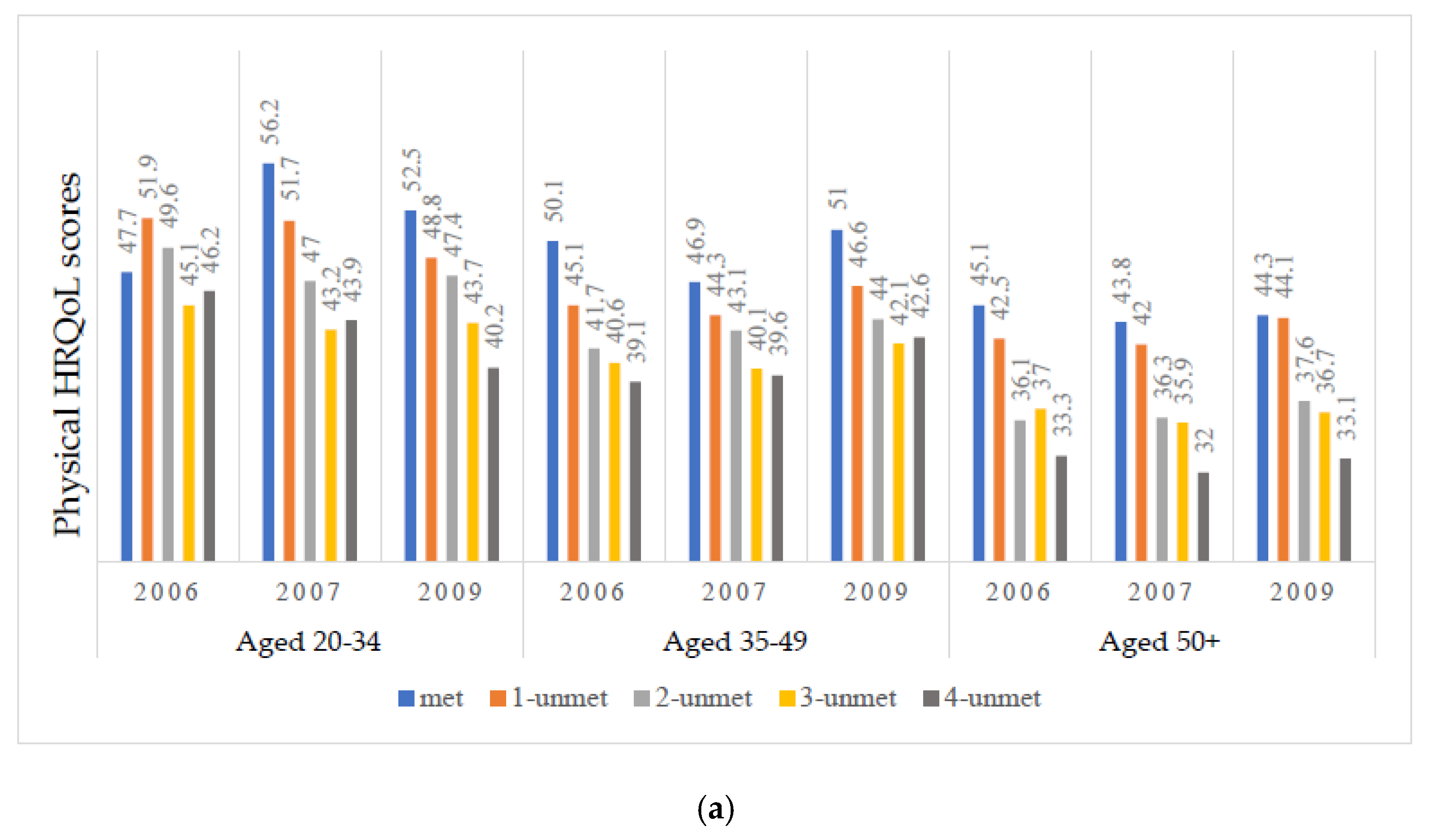
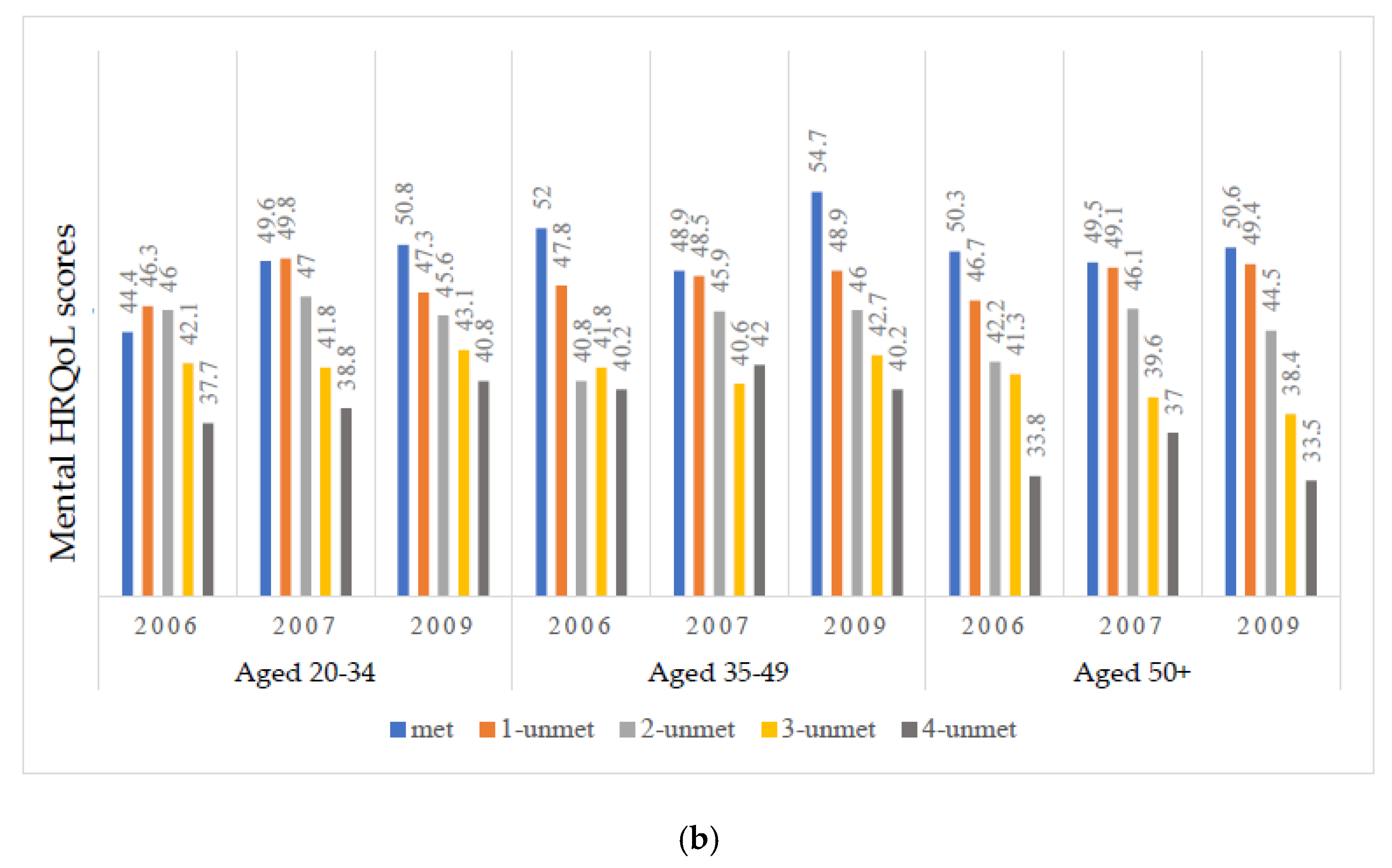
3.3. Physical and Mental Health-Related Quality of Life
3.4. Individual Growth Curve Models in Physical and Mental Health-Related Quality of Life
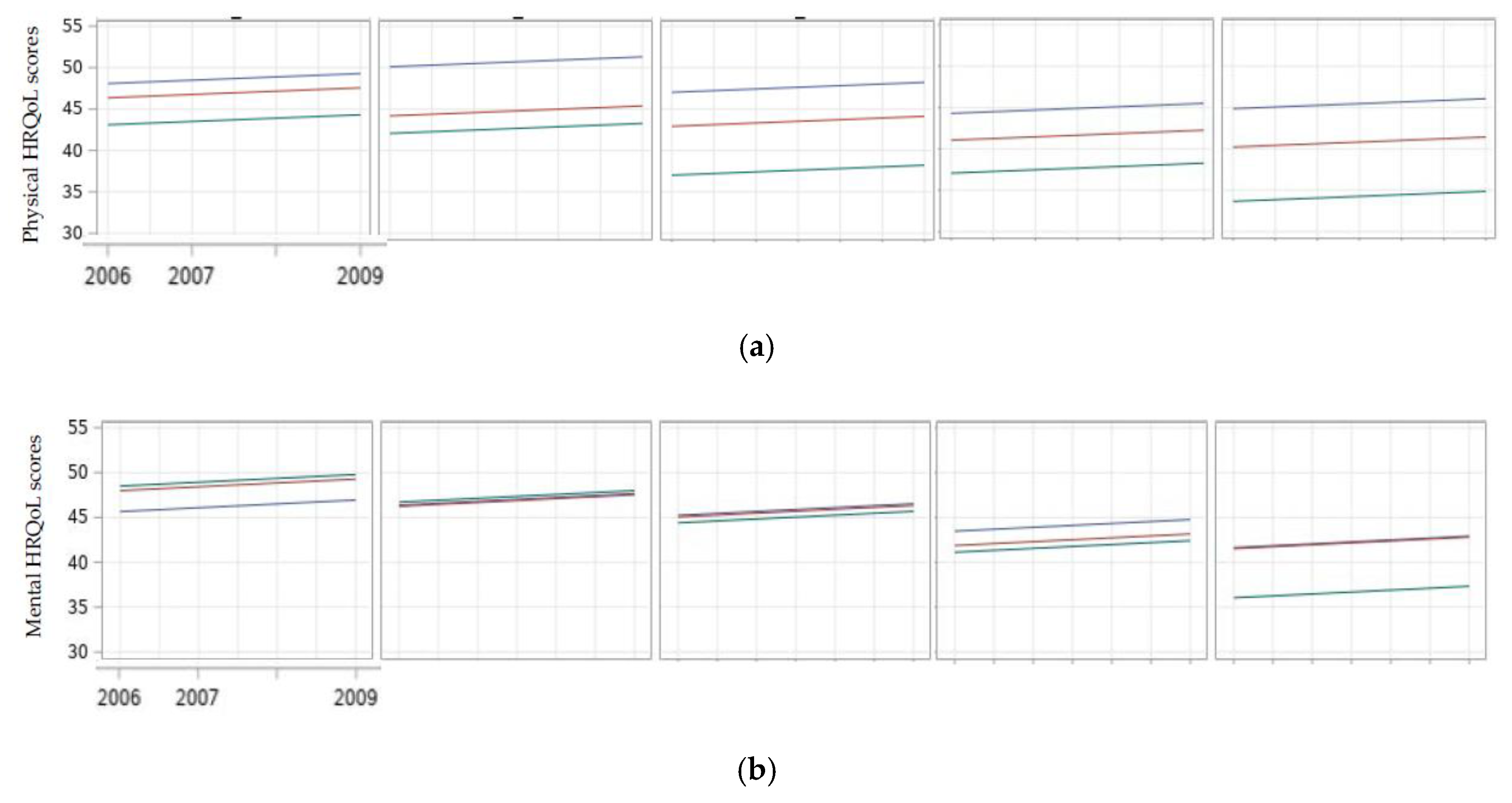
3.5. The Trajectories of Physical and Mental Health-Related Quality of Life
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- UNAIDS. Global HIV & AIDS statistics—Fact Sheet. 2021. Available online: https://www.unaids.org/en/resources/fact-sheet (accessed on 3 March 2021).
- Autenrieth, C.S.; Beck, E.J.; Stelzle, D.; Mallouris, C.; Mahy, M.; Ghys, P. Global and regional trends of people living with HIV aged 50 and over: Estimates and projections for 2000–2020. PLoS ONE 2018, 13, e0207005. [Google Scholar]
- Haddad, N.; Robert, A.; Weeks, A.; Popovic, N.; Siu, W.; Archibald, C. HIV in Canada-Surveillance Report, 2018. Can. Commun. Dis. Rep. 2019, 45, 304–312. [Google Scholar] [CrossRef] [PubMed]
- Sok, P. Older Persons with HIV in Canada. J. Infect. Dis. Epidemiol. 2019, 5, 84. [Google Scholar]
- Deeks, S.G.; Tracy, R.; Douek, D.C. Systemic Effects of Inflammation on Health during Chronic HIV Infection. Immunity 2013, 39, 633–645. [Google Scholar] [CrossRef] [Green Version]
- Paiardini, M.; Müller-Trutwin, M. HIV-associated chronic immune activation. Immunol. Rev. 2013, 254, 78–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deeks, S.G. HIV infection, inflammation, immunosenescence, and aging. Annu. Rev. Med. 2011, 62, 141–155. [Google Scholar] [CrossRef] [Green Version]
- Sokoya, T.; Steel, H.C.; Nieuwoudt, M.; Rossouw, T.M. HIV as a Cause of Immune Activation and Immunosenescence. Mediat. Inflamm. 2017, 2017, 6825493. [Google Scholar] [CrossRef] [PubMed]
- Aberg, J.A. Aging, inflammation, and HIV infection. Top. Antivir. Med. 2012, 20, 101–105. [Google Scholar]
- Mata-Marín, J.A.; Martínez-Osio, M.H.; Arroyo-Anduiza, C.I.; Berrospe-Silva, M.D.L.; Chaparro-Sánchez, A.; Cruz-Grajales, I.; Cruz-Herrera, J.E.; Noguez, U.; Gaytán-Martínez, J.E.; Jerónimo-Morales, M. Comorbidities and polypharmacy among HIV-positive patients aged 50 years and over: A case–control study. BMC Res. Notes 2019, 12, 556. [Google Scholar] [CrossRef]
- Pourcher, V.; Gourmelen, J.; Bureau, I.; Bouee, S. Comorbidities in people living with HIV: An epidemiologic and economic analysis using a claims database in France. PLoS ONE 2020, 15, e0243529. [Google Scholar] [CrossRef]
- Erlandson, K.M.; Allshouse, A.A.; Jankowski, C.M.; Mawhinney, S.; Kohrt, W.M.; Campbell, T.B. Relationship of physical function and quality of life among persons aging with HIV infection. AIDS 2014, 28, 1939–1943. [Google Scholar] [CrossRef] [Green Version]
- Campsmith, M.L.; Nakashima, A.K.; Davidson, A.J. Self-reported health-related quality of life in persons with HIV infection: Results from a multi-site interview project. Health Qual. Life Outcomes 2003, 1, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- George, S.; Bergin, C.; Clarke, S.; Courtney, G.; Codd, M.B. Health-related quality of life and associated factors in people with HIV: An Irish cohort study. Health Qual. Life Outcomes 2016, 14, 115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lyons, A.; Pitts, M.; Grierson, J. Exploring the Psychological Impact of HIV: Health Comparisons of Older Australian HIV-Positive and HIV-Negative Gay Men. AIDS Behav. 2012, 16, 2340–2349. [Google Scholar] [CrossRef]
- Balderson, B.H.; Grothaus, L.; Harrison, R.G.; McCoy, K.; Mahoney, C.; Catz, S. Chronic illness burden and quality of life in an aging HIV population. AIDS Care 2012, 25, 451–458. [Google Scholar] [CrossRef] [PubMed]
- Thurn, M.; Gustafson, D.R. Faces of Frailty in Aging with HIV Infection. Curr. HIV/AIDS Rep. 2017, 14, 31–37. [Google Scholar] [CrossRef] [Green Version]
- Piggott, D.A.; Erlandson, K.M.; Yarasheski, K.E. Frailty in HIV: Epidemiology, Biology, Measurement, Interventions, and Research Needs. Curr. HIV/AIDS Rep. 2016, 13, 340–348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cahill, S.; Valadéz, R. Growing Older with HIV/AIDS: New Public Health Challenges. Am. J. Public Health 2013, 103, e7–e15. [Google Scholar] [CrossRef]
- Hessol, N.A.; Zepf, R.; Zobell, E.; Weiser, S.D.; John, M.D. Food Insecurity and Aging Outcomes in Older Adults Living with HIV. AIDS Behav. 2017, 21, 3506–3514. [Google Scholar] [CrossRef]
- Furlotte, C.; Schwartz, K.; Koornstra, J.J.; Naster, R. ‘Got a room for me?’ Housing Experiences of Older Adults Living with HIV/AIDS in Ottawa. Can. J. Aging/Rev. Can. Vieil. 2012, 31, 37–48. [Google Scholar] [CrossRef]
- Greene, M.; Hessol, N.A.; Perissinotto, C.; Zepf, R.; Parrott, A.H.; Foreman, C.; Whirry, R.; Gandhi, M.; John, M. Loneliness in Older Adults Living with HIV. AIDS Behav. 2017, 22, 1475–1484. [Google Scholar] [CrossRef] [PubMed]
- Grov, C.; Golub, S.A.; Parsons, J.; Brennan, M.; Karpiak, S.E. Loneliness and HIV-related stigma explain depression among older HIV-positive adults. AIDS Care 2010, 22, 630–639. [Google Scholar] [CrossRef] [PubMed]
- Slater, L.Z. Social support, social stigma, health, coping, and quality of life in older gay men with HIV. Diss. Abstr. Int. Sect. B Sci. Eng. 2012, 72, 6675. [Google Scholar]
- Millar, B.; Starks, T.J.; Gurung, S.; Parsons, J.T. The Impact of Comorbidities, Depression, and Substance Use Problems on Quality of Life Among Older Adults Living With HIV. AIDS Behav. 2016, 21, 1684–1690. [Google Scholar] [CrossRef] [PubMed]
- Venturini, A.; Cenderello, G.; Di Biagio, A.; Giannini, B.; Ameri, M.; Giacomini, M.; Montefiori, M.; Setti, M.; Mazzarello, G.; Merlano, C.; et al. Quality of life in an Italian cohort of people living with HIV in the era of combined antiretroviral therapy (Evidence from I.A.N.U.A. study-investigation on antiretroviral therapy). AIDS Care 2017, 29, 1373–1377. [Google Scholar] [CrossRef]
- Rodriguez-Penney, A.T.; Iudicello, J.E.; Riggs, P.K.; Doyle, K.; Ellis, R.J.; Letendre, S.L.; Grant, I.; Woods, S.P. Co-Morbidities in Persons Infected with HIV: Increased Burden with Older Age and Negative Effects on Health-Related Quality of Life. AIDS Patient Care STDs 2013, 27, 5–16. [Google Scholar] [CrossRef] [Green Version]
- Slater, L.Z.; Moneyham, L.; Vance, D.E.; Raper, J.L.; Mugavero, M.J.; Childs, G. Support, Stigma, Health, Coping, and Quality of Life in Older Gay Men With HIV. J. Assoc. Nurses AIDS Care 2013, 24, 38–49. [Google Scholar] [CrossRef]
- Guaraldi, G.; Prakash, M.; Moecklinghoff, C.; Stellbrink, H.-J. Morbidity in older HIV-infected patients: Impact of long-term antiretroviral use. Aids Rev. 2014, 16, 75–89. [Google Scholar]
- Zeballos, D.; Lins, L.; Brites, C. Frailty and Its Association with Health-Related Quality of Life in Older HIV Patients, in Salvador, Brazil. AIDS Res. Hum. Retrovir. 2019, 35, 1074–1081. [Google Scholar] [CrossRef]
- Thompson, A.S.; Blankenship, K.M.; Selwyn, P.A.; Khoshnood, K.; Lopez, M.; Balacos, K.; Altice, F.L. Evaluation of an innovative program to address the health and social service needs of drug-using women with or at risk for HIV infection. J. Community Health 1998, 23, 419–440. [Google Scholar] [CrossRef]
- Riley, E.D.; Moore, K.; Sorensen, J.L.; Tulsky, J.P.; Bangsberg, D.R.; Neilands, T.B. Basic Subsistence Needs and Overall Health Among Human Immunodeficiency Virus-infected Homeless and Unstably Housed Women. Am. J. Epidemiol. 2011, 174, 515–522. [Google Scholar] [CrossRef]
- Kalichman, S.C.; Cherry, C.; White, D.; Kalichman, M.O.; Amaral, C.; Swetzes, C. Falling through the cracks: Unmet health service needs among people living with HIV in Atlanta, Georgia. J. Assoc. Nurses AIDS Care 2012, 23, 244–254. [Google Scholar] [CrossRef] [Green Version]
- Durbin, A.; Sirotich, F.; Antoniou, T.; Roesslein, K.; Durbin, J.; Lunsky, Y. Unmet needs among men with human immunodeficiency virus in community mental health care: A cross-sectional study. AIDS Care 2016, 28, 878–883. [Google Scholar] [CrossRef]
- Nápoles, T.M.; Batchelder, A.W.; Lin, A.; Moran, L.; Johnson, M.O.; Shumway, M.; Luetkemeyer, A.F.; Peters, M.G.; Eagen, K.V.; Riley, E.D. HCV treatment barriers among HIV/HCV co-infected patients in the US: A qualitative study to understand low uptake among marginalized populations in the DAA era. J. Public Health 2019, 41, e283–e289. [Google Scholar] [CrossRef]
- Sok, P.; Gardner, S.; Bekele, T.; Globerman, J.; Seeman, M.V.; Greene, S.; Sobota, M.; Koornstra, J.J.; Monette, L.; Hambly, K.; et al. Unmet basic needs negatively affect health-related quality of life in people aging with HIV: Results from the Positive Spaces, Healthy Places study. BMC Public Health 2018, 18, 644. [Google Scholar] [CrossRef]
- Gruszczyńska, E.; Rzeszutek, M. Trajectories of Health-Related Quality of Life and Perceived Social Support among People Living with HIV Undergoing Antiretroviral Treatment: Does Gender Matter? Front. Psychol. 2019, 10, 1664. [Google Scholar] [CrossRef] [Green Version]
- Teeraananchai, S.; Kerr, S.J.; Amin, J.; Ruxrungtham, K.; Law, M.G. Life expectancy of HIV-positive people after starting combination antiretroviral therapy: A meta-analysis. HIV Med. 2017, 18, 256–266. [Google Scholar] [CrossRef]
- Kong, A.M.; Pozen, A.; Anastos, K.; Kelvin, E.A.; Nash, D. Non-HIV Comorbid Conditions and Polypharmacy among People Living with HIV Age 65 or Older Compared with HIV-Negative Individuals Age 65 or Older in the United States: A Retrospective Claims-Based Analysis. AIDS Patient Care STDs 2019, 33, 93–103. [Google Scholar] [CrossRef] [PubMed]
- Phyo, A.Z.Z.; Freak-Poli, R.; Craig, H.; Gasevic, D.; Stocks, N.P.; Gonzalez-Chica, D.A.; Ryan, J. Quality of life and mortality in the general population: A systematic review and meta-analysis. BMC Public Health 2020, 20, 1596. [Google Scholar] [CrossRef] [PubMed]
- Rourke, S.B.; Positive Spaces Healthy Places The Positive Spaces Healthy Places Team; Bekele, T.; Tucker, R.; Greene, S.; Sobota, M.; Koornstra, J.; Monette, L.; Bacon, J.; Bhuiyan, S.; et al. Housing Characteristics and their Influence on Health-Related Quality of Life in Persons Living with HIV in Ontario, Canada: Results from the Positive Spaces, Healthy Places Study. AIDS Behav. 2012, 16, 2361–2373. [Google Scholar] [PubMed] [Green Version]
- Wu, A.W.; Revicki, D.A.; Jacobson, D.; Malitz, F.E. Evidence for reliability, validity and usefulness of the Medical Outcomes Study HIV Health Survey (MOS-HIV). Qual. Life Res. 1997, 6, 481–493. [Google Scholar] [CrossRef] [PubMed]
- Revicki, D.A.; Sorensen, S.; Wu, A.W. Reliability and Validity of Physical and Mental Health Summary Scores from the Medical Outcomes Study HIV Health Survey. Med. Care 1998, 36, 126–137. [Google Scholar] [CrossRef] [PubMed]
- Cooper, V.; EmERGE Consortium; Clatworthy, J.; Harding, R.; Whetham, J. Measuring quality of life among people living with HIV: A systematic review of reviews. Health Qual. Life Outcomes 2017, 15, 220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sherbourne, C.D.; Stewart, A.L. The MOS social support survey. Soc. Sci. Med. 1991, 32, 705–714. [Google Scholar] [CrossRef]
- Vilagut, G.; Forero, C.G.; Barbglia, G.; Alonso, J. Screening for Depression in the General Population with the Center for Epidemiologic Studies Depression (CES-D): A Systematic Review with Meta-Analysis. PLoS ONE 2016, 11, e0155431. [Google Scholar]
- Yudko, E.; Lozhkina, O.; Fouts, A. A comprehensive review of the psychometric properties of the Drug Abuse Screening Test. J. Subst. Abus. Treat. 2007, 32, 189–198. [Google Scholar] [CrossRef]
- Babor, F.T.; Higgins-Biddle, C.J.; Saunders, B.J.; Monteiro, G.M. AUDIT. The Alcohol Use Disorders Identification Test. Guidelines for Use in Primary Care, 2nd ed.; WHO: Geneva, Switzerland, 2001. [Google Scholar]
- Curran, P.J.; Obeidat, K.; Losardo, D. Twelve Frequently Asked Questions About Growth Curve Modeling. J. Cogn. Dev. 2010, 11, 121–136. [Google Scholar] [CrossRef] [Green Version]
- Gibbons, R.D.; Hedeker, D.; DuToit, S. Advances in Analysis of Longitudinal Data. Annu. Rev. Clin. Psychol. 2010, 6, 79–107. [Google Scholar] [CrossRef] [Green Version]
- Singer, J.D. Using SAS PROC MIXED to Fit Multilevel Models, Hierarchical Models, and individual Growth Models. J. Educ. Behav. Stat. 1998, 23, 323–355. [Google Scholar] [CrossRef] [Green Version]
- Liu, S.; Rovine, M.J.; Molenaar, P.C.M. Selecting a linear mixed model for longitudinal data: Repeated measures analysis of variance, covariance pattern model, and growth curve approaches. Psychol. Methods 2012, 17, 15–30. [Google Scholar] [CrossRef]
- Fazeli, P.L.; Montoya, J.L.; McDavid, C.N.; Moore, D.J. Older HIV+ and HIV- Adults Provide Similar Definitions of Successful Aging: A Mixed-Methods Examination. Gerontologist 2020, 60, 385–395. [Google Scholar] [CrossRef] [PubMed]
- Fang, X.; Vincent, W.; Calabrese, S.K.; Heckman, T.G.; Sikkema, K.J.; Humphries, D.; Hansen, N.B. Resilience, stress, and life quality in older adults living with HIV/AIDS. Aging Ment. Health 2015, 19, 1015–1021. [Google Scholar] [CrossRef]
- Stanic, A.; Rybin, D.; Cannata, F.; Hohl, C.; Brody, J.; Gaeta, J.; Bharel, M. The impact of the housing status on clinical outcomes and health care utilization among individuals living with HIV. AIDS Care 2019, 33, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Hopman, W.M.; Towheed, T.; Anastassiades, T.; Tenenhouse, A.; Poliquin, S.; Berger, C.; Joseph, L.; Brown, J.P.; Murray, T.M.; Adachi, J.D.; et al. Canadian normative data for the SF-36 health survey. CMAJ 2000, 163, 265–271. [Google Scholar]
- Dutra, B.S.; Lédo, A.P.; Lins-Kusterer, L.; Luz, E.; Prieto, I.R.; Brites, C. Changes health-related quality of life in HIV-infected patients following initiation of antiretroviral therapy: A longitudinal study. Braz. J. Infect. Dis. 2019, 23, 211–217. [Google Scholar] [CrossRef]
- Liu, C.; Weber, K.; Robison, E.; Hu, Z.; Jacobson, L.P.; Gange, S.J. Assessing the effect of HAART on change in quality of life among HIV-infected women. AIDS Res. Ther. 2006, 3, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, H.; Cohen, P. Using individual growth model to analyze the change in quality of life from adolescence to adulthood. Health Qual. Life Outcomes 2006, 4, 10. [Google Scholar] [CrossRef] [Green Version]
- Weinfurt, K.P.; Castel, L.D.; Li, Y.; Timbie, J.W.; Glendenning, G.A.; Schulman, K.A. Health-related quality of life among patients with breast cancer receiving zoledronic acid or pamidronate disodium for metastatic bone lesions. Med. Care 2004, 42, 164–175. [Google Scholar] [CrossRef] [PubMed]
- Yu, H.; Gao, C.; Zhang, Y.; He, R.; Zhou, L.; Liang, R. Trajectories of health-related quality of life during the natural history of dementia: A six-wave longitudinal study. Int. J. Geriatr. Psychiatry 2016, 32, 940–948. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Total n = 538 | Unmet Basic Needs n = 537 | |||||
|---|---|---|---|---|---|---|---|
| 0-Unmet (Met) n = 79 (14.71) | 1-Unmet n = 134 (24.95) | 2-Unmet n = 118 (21.97) | 3-Unmet n = 115 (21.42) | 4-Unmet n = 91 (16.95) | p Value ǂ | ||
| n (%)/ Median (IQR) | n (%)/ Median (IQR) | n (%)/ Median (IQR) | n (%)/ Median (IQR) | n (%)/ Median (IQR) | n (%)/ Median (IQR) | ||
| Physical HRQoL summary ‡ | 42.36 (34.30, 51.66) | 50.0 (39.58, 56.70) | 47.26 (36.0, 54.88) | 40.98 (33.28, 49.86) | 40.26 (33.91, 46.89) | 38.98 (29.69, 47.34) | <0.0001 |
| Mental HRQoL summary ‡ | 43.39 (35.89, 53.42) | 52.07 (42.22, 59.24) | 50.25 (39.40, 55.90) | 42.65 (34.68, 53.13) | 41.73 (35.04, 49.64) | 37.90 (30.94, 44.27) | <0.0001 |
| Demographics | |||||||
| Non-greater Toronto residents | 213 (39.59) | 19 (24.05) | 49 (36.57) | 49 (41.53) | 56 (48.70) | 40 (43.96) | 0.002 |
| Age (n = 507) | |||||||
| Young, 20–34 † | 75 (14.79) | 9 (12.16) | 16 (12.40) | 14 (12.73) | 15 (13.64) | 20 (24.10) | 0.136 |
| Middle-aged, 35–49 | 304 (59.96) | 40 (54.05) | 77 (59.69) | 67 (60.91) | 71 (64.55) | 49 (59.04) | |
| Old, 50+ | 128 (25.25) | 25 (33.78) | 36 (27.91) | 29 (26.36) | 24 (21.82) | 14 (16.87) | |
| Female | 134 (24.91) | 16 (20.25) | 23 (17.16) | 24 (20.34) | 33 (28.70) | 38 (41.76) | <0.0001 |
| Caucasian | 394 (73.23) | 57 (72.15) | 103 (76.87) | 89 (75.42) | 79 (68.70) | 66 (72.53) | 0.473 |
| Heterosexual (n = 530) | 195 (36.79) | 25 (32.05) | 30 (22.73) | 36 (30.51) | 53 (46.90) | 50 (56.82) | <0.0001 |
| SES/living and support conditions | |||||||
| No high school degree (n = 536) | 116 (21.64) | 10 (12.66) | 25 (18.80) | 30 (25.42) | 25 (21.74) | 26 (28.89) | 0.013 |
| Low income < 1150 CAD/m (n = 515) | 261 (50.68) | 37 (50.00) | 56 (43.75) | 59 (53.64) | 63 (55.75) | 46 (51.11) | 0.274 |
| Unemployed (n = 537) | 424 (78.96) | 55 (69.62) | 95 (70.90) | 102 (87.18) | 93 (80.87) | 78 (85.71) | 0.001 |
| Living alone (n = 486) | 259 (53.29) | 41 (60.29) | 66 (54.55) | 63 (60.00) | 51 (48.11) | 38 (44.19) | 0.026 |
| Low social support < 43 (n = 525) | 255 (48.57) | 36 (45.57) | 55 (41.67) | 59 (51.75) | 59 (53.64) | 46 (51.69) | 0.987 |
| HIV status | |||||||
| A history of AIDS diagnosis (n = 527) | 271 (51.41) | 35 (46.05) | 74 (56.06) | 61 (53.04) | 56 (49.12) | 45 (50.56) | 0.888 |
| CD4 T-cells < 200/mL (n = 454) | 256 (56.39) | 39 (54.93) | 72 (64.29) | 54 (51.92) | 52 (53.06) | 39 (57.35) | 0.526 |
| Health behavior risks | |||||||
| Depressive symptoms (n = 481) | 195 (40.54) | 9 (13.24) | 34 (28.57) | 49 (45.79) | 54 (52.94) | 49 (57.65) | <0.0001 |
| Drug abuse (n = 532) | 102 (19.17) | 7 (8.97) | 25 (18.66) | 26 (22.81) | 23 (20.00) | 21 (23.33) | 0.036 |
| Alcohol use disorder (n = 536) | 90 (16.79) | 9 (11.54) | 19 (14.29) | 26 (22.03) | 23 (20.00) | 12 (13.19) | 0.444 |
| A history of homelessness | 213 (39.59) | 27 (34.18) | 47 (35.07) | 50 (42.37) | 52 (45.22) | 36 (39.56) | 0.158 |
| A history of incarceration (n = 533) | 158 (29.64) | 18 (23.08) | 30 (22.56) | 45 (38.14) | 39 (34.51) | 26 (28.89) | 0.085 |
| Model 1 | Model 2 | Model 3 | Model 4 | Model 5 | Model 6 | |
|---|---|---|---|---|---|---|
| Fixed effects | ||||||
| Intercept | 43.30 (0.40) a | 42.69 (0.45) a | 46.19 (0.67) a | 50.98 (1.14) a | 54.63 (1.26) a | 52.50 (1.78) a |
| Time | 0.51 (0.15) b | 0.43 (0.15) b | 0.38 (0.15) c | 0.39 (0.16) c | 0.40 (0.16) c | |
| Unmet basic needs (met = ref.) | ||||||
| 1-unmet | −1.42 (0.67) c | −1.47 (0.68) c | −1.29 (0.70) d | 2.02 (1.87) | ||
| 2-unmet | −4.09 (0.71) a | −4.11 (0.72) a | −3.75 (0.75) a | −1.06 (1.96) | ||
| 3-unmet | −5.63 (0.75) a | −5.71 (0.76) a | −5.30 (0.78) a | −3.78 (1.91) c | ||
| 4-unmet | −6.69 (0.84) a | −6.78 (0.85) a | −6.40 (0.87) a | −3.21 (2.15) | ||
| Age groups (20–34 = ref.) | ||||||
| Middle-aged, 35–49 | −4.17 (1.10) a | −4.10 (1.07) b | −1.72 (1.88) | |||
| Old, 50+ | −8.85 (1.23) a | −8.21 (1.22) a | −4.98 (2.07) c | |||
| Non-greater Toronto resident | −3.43 (0.76) a | −3.34 (0.76) a | ||||
| Caucasian | −2.37 (0.84) b | −2.61 (0.84) b | ||||
| Low social support < 43 | −1.60 (0.60) b | −1.68 (0.55) b | ||||
| Drug abuse ≥ 6 DAST scores | −1.67 (0.73) c | −1.58 (0.73) c | ||||
| Interactions | ||||||
| 1-unmet × middle-aged | −4.21 (2.08) c | |||||
| 1-unmet × old | −3.06 (2.29) | |||||
| 2-unmet × middle-aged | −2.38 (2.18) | |||||
| 2-unmet × old | −5.03 (2.48) c | |||||
| 3-unmet × middle-aged | −1.52 (2.15) | |||||
| 3-unmet × old | −2.24 (2.49) | |||||
| 4-unmet × middle-aged | −2.91 (2.42) | |||||
| 4-unmet × old | −6.21 (2.83) c | |||||
| Random variance | ||||||
| Intercepts (1,1) | 70.27 a | 79.52 a | 71.19 a | 64.42 a | 57.53 a | 57.10 a |
| Intercepts-slopes (2,1) | - | −4.32 c | −3.97 c | −3.78 c | −3.46 c | −3.32 d |
| Linear slopes (2,2) | - | 1.88 c | 1.56 c | 1.51 c | 1.59 c | 1.67 c |
| Residuals | 44.60 a | 39.93 a | 39.18 a | 39.01 a | 38.67 a | 37.30 a |
| Observations used | 1482 | 1482 | 1481 | 1395 | 1319 | 1319 |
| Fit statistics and model tests | ||||||
| -2LL | 10,730.4 | 10,713.8 | 10,614.4 | 9943.4 | 9357.6 | 9321.9 |
| AIC | 10,736.4 | 10,721.8 | 10,622.4 | 9951.4 | 9365.6 | 9329.9 |
| BIC | 10,749.3 | 10,739.0 | 10,639.5 | 9968.3 | 9382.5 | 9346.8 |
| Chi-square | 508.42 a | 521.67 a | 470.48 a | 400.39 a | 328.23 a | 329.43 a |
| Model 1 | Model 2 | Model 3 | Model 4 | Model 5 | Model 6 | |
|---|---|---|---|---|---|---|
| Fixed effects | ||||||
| Intercept | 45.14 (0.42) a | 44.20 (0.48) a | 48.61 (0.74) a | 48.56 (1.25) a | 55.03 (1.36) a | 52.48 (2.08) a |
| Time | 0.78 (0.18) a | 0.68 (0.18) a | 0.65 (0.18) b | 0.41 (0.20) c | 0.43 (0.20) c | |
| Unmet basic needs (met = ref.) | ||||||
| 1-unmet | −1.68 (0.78) c | −1.65 (0.81) c | −1.49 (0.80) d | 0.72 (2.23) | ||
| 2-unmet | −4.41 (0.83) a | −4.34 (0.85) a | −2.98 (0.86) a | −0.41 (2.41) | ||
| 3-unmet | −7.20 (0.86) a | −7.08 (0.89) a | −5.89 (0.89) a | −2.18 (2.32) | ||
| 4-unmet | −9.60 (0.96) a | −9.44 (0.99) a | −7.39 (1.00) a | −4.01 (2.51) | ||
| Age groups (20–34 = ref.) | ||||||
| Middle-aged, 35–49 | −0.40 (1.17) | −0.23 (1.12) | 2.33 (2.84) | |||
| Old, 50+ | −0.92 (1.32) | −1.00 (1.25) | 2.84 (2.39) | |||
| Female | −1.97 (0.90) c | −1.81 (0.90) c | ||||
| Low income < 1150 CAD/m | −1.31 (0.60) c | −1.25 (0.61) c | ||||
| Unemployed | −2.88 (0.73) a | −3.10 (0.74) a | ||||
| Low social support < 43 | −5.23 (0.61) a | −5.24 (0.61) a | ||||
| Drug abuse ≥ 6 DAST scores | −5.43 (0.80) a | −5.32 (0.80) a | ||||
| Interactions (20–34 [ref.]) | ||||||
| 1-unmet × middle-aged | −2.47 (2.46) | |||||
| 1-unmet × old | −2.52 (2.70) | |||||
| 2-unmet × middle-aged | −2.53 (2.63) | |||||
| 2-unmet × old | −3.70 (2.95) | |||||
| 3-unmet × middle-aged | −3.93 (2.57) | |||||
| 3-unmet × old | −5.19 (2.95) d | |||||
| 4-unmet × middle-aged | −2.45 (2.79) | |||||
| 4-unmet × old | −8.44 (3.25) b | |||||
| Random variance | ||||||
| Intercepts (1,1) | 71.70 a | 79.72 a | 68.31 a | 67.38 a | 55.10 a | 55.20 a |
| Intercepts-slopes (2,1) | - | −3.83 | −4.67 c | −3.83 c | −5.64 c | −5.67 c |
| Linear slopes (2,2) | - | 2.73 c | 2.32 c | 2.03 c | 3.70 b | 3.65 b |
| Residuals | 65.09 a | 57.70 a | 56.55 a | 57.40 a | 49.40 a | 49.31 a |
| Observations used | 1482 | 1482 | 1481 | 1395 | 1274 | 1274 |
| Fit statistics and model tests | ||||||
| -2 LL | 11,140.5 | 11,117.4 | 10,982.7 | 10,348.7 | 9276.9 | 9240.9 |
| AIC | 11,146.5 | 11,125.4 | 10,990.7 | 10,356.7 | 9284.9 | 9248.9 |
| BIC | 11,159.3 | 11,142.6 | 11,007.8 | 10,373.6 | 9301.7 | 9265.8 |
| Chi-square | 354.41 a | 370.52 a | 296.42 a | 280.22 a | 189.23 a | 187.68 a |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sok, P.; Seeman, M.V.; Nisenbaum, R.; Watson, J.; Rourke, S.B.; on behalf of the PSHP Team. Four-Year Trajectories of Health-Related Quality of Life in People Living with HIV: Impact of Unmet Basic Needs across Age Groups in Positive Spaces, Healthy Places. Int. J. Environ. Res. Public Health 2021, 18, 12256. https://doi.org/10.3390/ijerph182212256
Sok P, Seeman MV, Nisenbaum R, Watson J, Rourke SB, on behalf of the PSHP Team. Four-Year Trajectories of Health-Related Quality of Life in People Living with HIV: Impact of Unmet Basic Needs across Age Groups in Positive Spaces, Healthy Places. International Journal of Environmental Research and Public Health. 2021; 18(22):12256. https://doi.org/10.3390/ijerph182212256
Chicago/Turabian StyleSok, Phan, Mary V. Seeman, Rosane Nisenbaum, James Watson, Sean B. Rourke, and on behalf of the PSHP Team. 2021. "Four-Year Trajectories of Health-Related Quality of Life in People Living with HIV: Impact of Unmet Basic Needs across Age Groups in Positive Spaces, Healthy Places" International Journal of Environmental Research and Public Health 18, no. 22: 12256. https://doi.org/10.3390/ijerph182212256
APA StyleSok, P., Seeman, M. V., Nisenbaum, R., Watson, J., Rourke, S. B., & on behalf of the PSHP Team. (2021). Four-Year Trajectories of Health-Related Quality of Life in People Living with HIV: Impact of Unmet Basic Needs across Age Groups in Positive Spaces, Healthy Places. International Journal of Environmental Research and Public Health, 18(22), 12256. https://doi.org/10.3390/ijerph182212256