
Prevalence and Demographic, Socioeconomic, and Behavioral Risk Factors of Self-Reported Symptoms of Sexually Transmitted Infections (STIs) among Ever-Married Women: Evidence from Nationally Representative Surveys in Bangladesh

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources and Sample
2.2. Outcome Variables
2.3. Explanatory Variables
2.4. Statistical Analysis
3. Results
3.1. Sample Characteristics
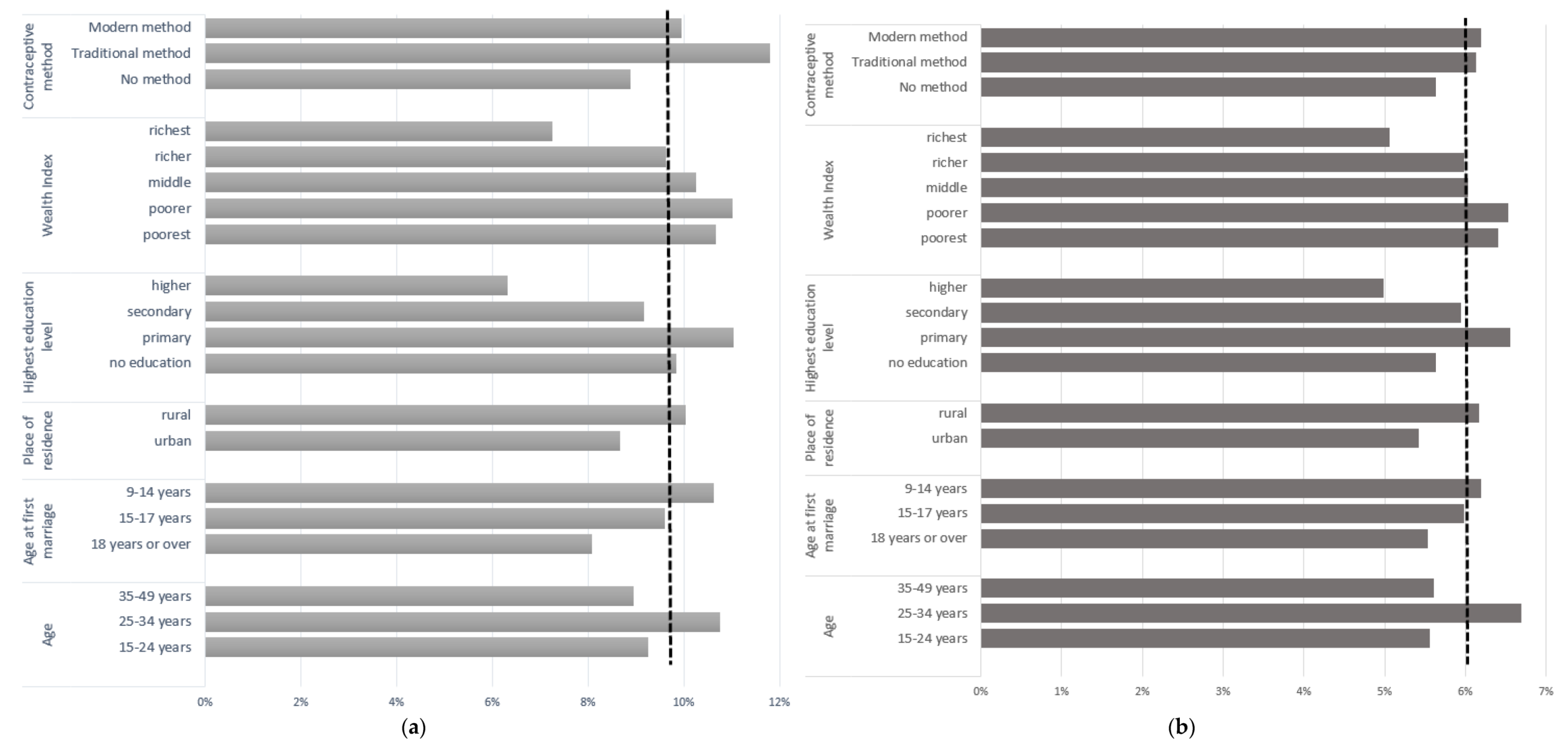
3.2. Prevalence of STI Symptoms by Key Risk Factors
3.3. Associations of STI Symptoms with Demographic, Socioeconomic, and Behavioral Risk Factors
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mwatelah, R.; McKinnon, L.R.; Baxter, C.; Abdool Karim, Q.; Abdool Karim, S.S. Mechanisms of sexually transmitted infection-induced inflammation in women: Implications for HIV risk. J. Int. AIDS Soc. 2019, 22, e25346. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organisation. Sexually Transmitted Infections (STIs). 2019. Available online: https://www.who.int/news-room/fact-sheets/detail/sexually-transmitted-infections-(stis) (accessed on 22 February 2021).
- Faruk, S.R.; Chowdhury, M.K.; Kamal, S.B.; Shamim, S.M.A.; Mohit, I. STD/AIDS Asia and world perspective. Clin. Med. Investig. 2018, 3, 1–2. [Google Scholar]
- Hwang, L.Y.; Ma, Y.; Moscicki, A.-B. Biological and Behavioral Risks for Incident Chlamydia trachomatis Infection in a Prospective Cohort. Obstet. Gynecol. 2014, 124, 954–960. [Google Scholar] [CrossRef] [Green Version]
- Silveira, M.F.; Bruni, M.P.; Stauffert, D.; Golparian, D.; Unemo, M. Prevalence and risk factors associated with Chlamydia trachomatis, Neisseria gonorrhoeae, and Mycoplasma genitalium among women in Pelotas, Southern Brazil. Int. J. STD AIDS 2020, 31, 432–439. [Google Scholar] [CrossRef] [PubMed]
- Ostrach, B.; Singer, M. At special risk: Biopolitical vulnerability and HIV/STI syndemics among women. Health Sociol. Rev. 2012, 21, 258–271. [Google Scholar] [CrossRef]
- Shannon, C.L.; Klausner, J.D. The growing epidemic of sexually transmitted infections in adolescents: A neglected population. Curr. Opin. Pediatr. 2018, 30, 137. [Google Scholar] [CrossRef]
- Abdulai, M.A.; Baiden, F.; Afari-Asiedu, S.; Gyabaa-Febir, L.; Adjei, K.K.; Mahama, E.; Tawiah-Agyemang, C.; Newton, S.K.; Asante, K.P.; Owusu-Agyei, S. The Risk of Sexually Transmitted Infection and Its Influence on Condom Use among Pregnant Women in the Kintampo North Municipality of Ghana. J. Sex. Transm. Dis. 2017, 2017, 8642685. [Google Scholar] [CrossRef] [Green Version]
- Jesmin, S.S.; Cready, C.M. Can a woman refuse sex if her husband has a sexually transmitted infection? Attitudes toward safer-sex negotiation among married women in Bangladesh. Cult. Health Sex. 2014, 16, 666–682. [Google Scholar] [CrossRef]
- Korenromp, E.L.; Wi, T.; Resch, S.; Stover, J.; Broutet, N. Costing of National STI Program Implementation for the Global STI Control Strategy for the Health Sector, 2016–2021. PLoS ONE 2017, 12, e0170773. [Google Scholar] [CrossRef] [Green Version]
- Morrow, R.A.; Gibney, L.; Macaluso, M.; Kirk, K.; Hassan, M.S.; Schwebke, J.; Vermund, S.H.; Choudhury, P. Faculty Opinions recommendation of Prevalence of infectious diseases in Bangladeshi women living adjacent to a truck stand: HIV/STD/hepatitis/genital tract infections. Sex. Transm. Infect. 2001, 77, 344–350. [Google Scholar] [CrossRef] [Green Version]
- Shirin, T.; Rahman, S.; Rabbi, F.J.; Kabir, H.; Mamun, K. Prevalence of Sexually Transmitted Diseases and Transmission of HIV in Dhaka, Bangladesh. Bangladesh J. Med. Microbiol. 2009, 3, 27–33. [Google Scholar] [CrossRef] [Green Version]
- Bogaerts, J.; Ahmed, J.; Akhter, N.; Begum, N.; Rahman, M.; Nahar, S.; Van Ranst, M.; Verhaegen, J. Sexually transmitted infections among married women in Dhaka, Bangladesh: Unexpected high prevalence of herpes simplex type 2 infection. Sex. Transm. Infect. 2001, 77, 114–119. [Google Scholar] [CrossRef] [Green Version]
- Alam, N.; Rahman, M.; Gausia, K.; Yunus, M.D.; Islam, N.; Chaudhury, P.; Monira, S.; Funkhouser, E.; Vermund, S.H.; Killewo, J. Sexually Transmitted Infections and Risk Factors Among Truck Stand Workers in Dhaka, Bangladesh. Sex. Transm. Dis. 2007, 34, 99–103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Babi, A.; Issa, T.; Issanov, A.; Akilzhanova, A.; Nurgaliyeva, K.; Abugalieva, Z.; Ukybassova, T.; Daribay, Z.; Khan, S.A.; Chan, C.K.; et al. Prevalence of high-risk human papillomavirus infection among Kazakhstani women attending gynecological outpatient clinics. Int. J. Infect. Dis. 2021, 109, 8–16. [Google Scholar] [CrossRef] [PubMed]
- Mathebula, R.; Kuonza, L.R.; Musekiwa, A.; Kularatne, R.; Maseko, V.; Kufa, T. Factors associated with repeat genital symptoms among sexually transmitted infection service attendees in South Africa, 2015–2016. S. Afr. Med. J. 2020, 110, 661–666. [Google Scholar]
- Nankinga, O.; Misinde, C.; Kwagala, B. Gender relations, sexual behaviour, and risk of contracting sexually transmitted infections among women in union in Uganda. BMC Public Health 2016, 16, 440. [Google Scholar] [CrossRef] [Green Version]
- Shabnam, S. Sexually Transmitted Infections and Spousal Violence: The Experience of Married Women in India. Indian J. Gend. Stud. 2017, 24, 24–46. [Google Scholar] [CrossRef]
- Vyas, S. Marital violence and sexually transmitted infections among women in post-revolution Egypt. Sex. Reprod. Health 2017, 13, 68–74. [Google Scholar] [CrossRef]
- Yosef, T. Sexually transmitted infection associated syndromes among pregnant women attending antenatal care clinics in southwest Ethiopia. Heliyon 2021, 7, e07576. [Google Scholar] [CrossRef] [PubMed]
- Anguzu, G.; Flynn, A.; Musaazi, J.; Kasirye, R.; Atuhaire, L.K.; Kiragga, A.N.; Kabagenyi, A.; Mujugira, A. Relationship between socioeconomic status and risk of sexually transmitted infections in Uganda: Multilevel analysis of a nationally representative survey. Int. J. STD AIDS 2018, 30, 284–291. [Google Scholar] [CrossRef]
- Rahman, M.; Nakamura, K.; Seino, K.; Kizuki, M. Intimate Partner Violence and Symptoms of Sexually Transmitted Infections: Are the Women from Low Socio-economic Strata in Bangladesh at Increased Risk. Int. J. Behav. Med. 2014, 21, 348–357. [Google Scholar] [CrossRef]
- Isara, A.; Baldeh, A.-K. Prevalence of sexually transmitted infections among pregnant women attending antenatal clinics in West Coast Region of The Gambia. Afr. Health Sci. 2021, 21, 585–592. [Google Scholar] [CrossRef]
- Gani, M.S.; Chowdhury, A.M.R.; Nyström, L. Urban–rural and socioeconomic variations in lifetime prevalence of symptoms of sexually transmitted infections among Bangladeshi adolescents. Asia Pac. Fam. Med. 2014, 13, 7. [Google Scholar] [CrossRef] [Green Version]
- Huda, M.N.; Sikder, A.; Rahman, M.; Mohiuddin, M.; Islam, M.S. Access to Mass Media and Awareness of Sexually Transmitted Diseases (STDs) Among the Truck Drivers in Dhaka City: Do Mass Media Make Them Aware? S. Asian J. Soc. Sci. 2016, 1, 1–15. [Google Scholar]
- National Institute of Population Research Training—NIPORT. Bangladesh, Mitra Associates, and ICF International, Bangladesh Demographic and Health Survey 2014; Technical Report; National Institute of Population Research and Training: Dhaka, Bangladesh, 2016.
- Decker, M.; Miller, E.; Kapur, N.; Gupta, J.; Raj, A.; Silverman, J. Intimate partner violence and sexually transmitted disease symptoms in a national sample of married Bangladeshi women. Int. J. Gynecol. Obstet. 2008, 100, 18–23. [Google Scholar] [CrossRef] [PubMed]
- Shakya, S.; Thingulstad, S.; Syversen, U.; Nordbø, S.A.; Madhup, S.; Vaidya, K.; Karmacharya, B.M.; Åsvold, B.O.; Afset, J.E. Prevalence of Sexually Transmitted Infections among Married Women in Rural Nepal. Infect. Dis. Obstet. Gynecol. 2018, 2018, 4980396. [Google Scholar] [CrossRef]
- Tariqujjaman; Hasan; Moitry, A.; Huda, S.; Irfan, S.; Rahman, M.; Kafi, M.A.H.; Azad; Sarma, H.; Hossain, M. Prevalence and correlates of HIV/AIDS knowledge among ever married women of reproductive age in Bangladesh: An update from the Bangladesh Demographic and Health Survey 2014. Am. J. Prev. Med. Public Health 2020, 6, 26. [Google Scholar] [CrossRef]
- Fatusi, A.; Wang, W. Multiple sexual partnership mediates the association between early sexual debut and sexually transmitted infection among adolescent and young adult males in Nigeria. Eur. J. Contracept. Reprod. Health Care 2009, 14, 134–143. [Google Scholar] [CrossRef] [PubMed]
- Yaya, S.; Bishwajit, G.; Danhoundo, G.; Shah, V.; Ekholuenetale, M. Trends and determinants of HIV/AIDS knowledge among women in Bangladesh. BMC Public Health 2016, 16, 812. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khan, M.N.; Islam, M.M. Women’s attitude towards wife-beating and its relationship with reproductive healthcare seeking behavior: A countrywide population survey in Bangladesh. PLoS ONE 2018, 13, e0198833. [Google Scholar] [CrossRef] [PubMed]
- Maldonado, G.; Greenland, S. Simulation Study of Confounder-Selection Strategies. Am. J. Epidemiol. 1993, 138, 923–936. [Google Scholar] [CrossRef] [Green Version]
- ICF International. Demographic and Health Surveys Sampling and Household Listing Manual. DHS Toolkit. 2012. Available online: https://dhsprogram.com/publications/publication-dhsm4-dhs-questionnaires-and-manuals.cfm (accessed on 3 November 2020).
- van Buuren, S.; Boshuizen, H.C.; Knook, D.L. Multiple imputation of missing blood pressure covariates in survival analysis. Stat. Med. 1999, 18, 681–694. [Google Scholar] [CrossRef]
- Spratt, M.; Carpenter, J.; Sterne, J.; Carlin, J.; Heron, J.; Henderson, J.; Tilling, K. Strategies for Multiple Imputation in Longitudinal Studies. Am. J. Epidemiol. 2010, 172, 478–487. [Google Scholar] [CrossRef]
- Huda, M.N. A Mixed-Methods Study of Sex Work and the HIV Prevention Environment for Female Sex Workers in Bangladesh; The University of New South Wales: Sydney, Australia, 2019. [Google Scholar]
- Santhya, K.; Jejeebhoy, S.J. Early marriage and HIV/AIDS: Risk factors among young women in India. Econ. Political Wkly. 2007, 42, 1291–1297. [Google Scholar]
- Uddin, J.; Pulok, M.; Johnson, R.; Rana, J.; Baker, E. Association between child marriage and institutional delivery care services use in Bangladesh: Intersections between education and place of residence. Public Health 2019, 171, 6–14. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, M.C.; Wodon, Q. Impact of Child Marriage on Literacy and Education Attainment in Africa; UNICEF and UNESCO Statistics: Washington, DC, USA, 2014. [Google Scholar]
- Makino, M.; Shonchoy, A.S.; Wahhaj, Z. Early Effects of the COVID-19 Lockdown on Children in Rural Bangladesh. 2021. Available online: https://knowledgecommons.popcouncil.org/cgi/viewcontent.cgi?article=2254&context=departments_sbsr-pgy (accessed on 18 August 2021).
- Deese, J.; Pradhan, S.; Goetz, H.; Morrison, C. Contraceptive use and the risk of sexually transmitted infection: Systematic review and current perspectives. Open Access J. Contracept. 2018, 9, 91–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ross, J. Is oral contraceptive associated with genital warts? Sex. Transm. Infect. 1996, 72, 330–333. [Google Scholar] [CrossRef] [Green Version]
- Amanullah, A.S.M.; Huda, M.N. Commercial sex and vulnerability to HIV infection: A study among the children of sex workers (SWs) in Tangail brothel. In Sex Workers and Their Children in Bangladesh: Addressing Risks and Vulnerabilities; Sabet, D.M., Rahman, T.A.S., Eds.; University of Liberal Arts Bangladesh and ActionAid Bangladesh: Dhaka, Bangladesh, 2012; pp. 59–81. [Google Scholar]
- Chacko, M.R.; von Sternberg, K.; Velasquez, M.M.; Wiemann, C.M.; Smith, P.B.; DiClemente, R. Young women’s perspective of the pros and cons to seeking screening for chlamydia and gonorrhea: An exploratory study. J. Pediatric Adolesc. Gynecol. 2008, 21, 187–193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rogers, A.J.; Achiro, L.; Bukusi, E.A.; Hatcher, A.M.; Kwena, Z.; Musoke, P.L.; Turan, J.M.; Weke, E.; Darbes, L. Couple interdependence impacts HIV-related health behaviours among pregnant couples in southwestern Kenya: A qualitative analysis. J. Int. AIDS Soc. 2016, 19, 21224. [Google Scholar] [CrossRef] [PubMed]
- Mullany, B.C.; Ram, F.; Singh, A.; Magadi, M.; Diamond, I.; Madise, N.; Smith, P.; Gawde, N.C.; Sivakami, M.; Babu, B.V.; et al. Spousal agreement on maternal health practices in Kathmandu, Nepal. J. Biosoc. Sci. 2010, 42, 689–693. [Google Scholar] [CrossRef]
- Schofield, T.; Connell, R.W.; Walker, L.; Wood, J.F.; Butland, D.L. Understanding men’s health and illness: A gender-relations approach to policy, research, and practice. J. Am. Coll. Health 2000, 48, 247–256. [Google Scholar] [CrossRef] [PubMed]
- Salam, M.A.; Alim, M.A.; Noguchi, T. Spousal abuse against women and its consequences on reproductive health: A study in the urban slums in Bangladesh. Matern. Child Health J. 2006, 10, 83–94. [Google Scholar] [CrossRef] [PubMed]
- Hess, K.L.; Javanbakht, M.; Brown, J.M.; Weiss, R.E.; Hsu, P.; Gorbach, P.M. Intimate Partner Violence and Sexually Transmitted Infections Among Young Adult Women. Sex. Transm. Dis. 2012, 39, 366–371. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Variables | Measuement Scales | Descriptions | |
|---|---|---|---|
| Demographic factors | Age | Categorical | Three age groups are recoded as 15–24, 25–34, 35–49 years, with 15–24 years as a reference group. |
| Age at first marriage | Categorical | Age at first marriage is grouped as 9–14, 15–17, 18 years or older, with 18 years or older as reference group. | |
| Type of residence | Binary | Type of residence is recoded into a dummy variable (rural = 0 and urban = 1), with rural as a reference group. | |
| Socioeconomic factors | Education | Categorical | Education has four groups: no education (reference), primary, secondary, higher. |
| Partner’s education | Categorical | Partner’s education is recoded as no education (reference), primary, secondary, higher. | |
| Wealth quintile | Categorical | Wealth quintile is categorized into five groups: poorest (reference), poorer, middle, richer, richest. | |
| Paidwork status | Binary | Paidwork is recoded into a dummy variable: no = 0 (reference), yes = 1. | |
| Behavioral factors | Contraceptive method | Categorical | Contraceptive method has three categories such as no method (reference), traditional method, modern method. |
| Knowledge about STI | Binary | Knowledge about STI is coded as a binary variable, with no = 0 (reference), yes = 1. | |
| Wife beating justified | Binary | Wife beating justified has two groups: with no = 0 (reference), yes = 1. | |
| Women’s healthcare decision-making | Categorical | Women’s healthcare decision-making is categorized into 4 groups: wife (reference), wife and husband, respondent and someone else, and husband. | |
| Exposure to mass media | Categorical | Exposure to mass media is coded as not at all (reference), irregular, regular. | |
| Survey year | Categorical | Survey year has three groups: 2007 (reference), 2011, 2014. |
| Had Abnormal Genital Discharge in the Past 12 Months Prior to the Survey (n = 41,777) | Had Genital Sores/Ulcers in Past 12 Months Prior to the Survey (n = 41,777) | |||||
|---|---|---|---|---|---|---|
| No (n = 37,598) | Yes (n = 4179) | p-Value | No (n = 39,155) | Yes (n = 2622) | p-Value | |
| Demographic factors | ||||||
| Age | <0.001 | <0.001 | ||||
| 15–24 years | 11,981 (32.8%) | 1306 (31.2%) | 12,525 (32.8%) | 762 (31.2%) | ||
| 25–34 years | 13,070 (34.6%) | 1606 (38.9%) | 13,642 (34.6%) | 1034 (38.9%) | ||
| 35–49 years | 12,547 (32.6%) | 1267 (29.9%) | 12,988 (32.6%) | 826 (29.9%) | ||
| Age at first marriage | ||||||
| 18 years and older | 8726 (21.5%) | 803 (17.6%) | 8986 (21.5%) | 543 (17.6%) | ||
| 15–17 years | 14,804 (39.1%) | 1652 (38.8%) | 15,422 (39.1%) | 1034 (38.8%) | ||
| 9–14 years | 14,068 (39.4%) | 1724 (43.6%) | 14,747 (39.4%) | 1045 (43.6%) | ||
| Type of residence | <0.001 | <0.001 | ||||
| urban | 13,581 (26.4%) | 1341 (23.4%) | 14,072 (26.4%) | 850 (23.4%) | ||
| rural | 24,017 (73.6%) | 2838 (76.6%) | 25,083 (73.6%) | 1772 (76.6%) | ||
| Socioeconomic factors | ||||||
| Education | <0.001 | <0.001 | ||||
| No education | 9091 (26.3%) | 1038 (26.8%) | 9516 (26.3%) | 613 (26.8%) | ||
| Primary | 10,997 (29.3%) | 1388 (33.9%) | 11,514 (29.3%) | 871 (33.9%) | ||
| Secondary | 13,860 (36.3%) | 1522 (34.2%) | 14,433 (36.3%) | 949 (34.2%) | ||
| Higher | 3650 (8.2%) | 231 (5.1%) | 3692 (8.2%) | 189 (5.1%) | ||
| Partner’s education | <0.001 | <0.001 | ||||
| No education | 10,438 (29.7%) | 1243 (31.8%) | 10,939 (29.7%) | 742 (31.8%) | ||
| Primary | 10,113 (27.0%) | 1302 (30.8%) | 10,633 (27.0%) | 782 (30.8%) | ||
| Secondary | 11,032 (28.9%) | 1191 (27.5%) | 11,457 (28.9%) | 766 (27.5%) | ||
| Higher | 6015 (14.3%) | 443 (9.9%) | 6126 (14.3%) | 332 (9.9%) | ||
| Wealth quintile | <0.001 | <0.001 | ||||
| Poorest | 6106 (17.4%) | 788 (19.4%) | 6423 (17.4%) | 471 (19.4%) | ||
| Poorer | 6856 (19.0%) | 883 (21.9%) | 7193 (19.0%) | 546 (21.9%) | ||
| Middle | 7353 (20.1%) | 866 (21.4%) | 7689 (20.1%) | 530 (21.4%) | ||
| Richer | 7915 (21.1%) | 911 (21.0%) | 8272 (21.1%) | 554 (21.0%) | ||
| Richest | 9368 (22.4%) | 731 (16.3%) | 9578 (22.4%) | 521 (16.3%) | ||
| Paid work status | <0.001 | <0.001 | ||||
| No | 30,244 (79.0%) | 3280 (76.5%) | 31,490 (79.0%) | 2034 (76.5%) | ||
| Yes | 7354 (21.0%) | 899 (23.5%) | 7665 (21.0%) | 588 (23.5%) | ||
| Behavioral factors | ||||||
| Contraceptive method | <0.001 | <0.001 | ||||
| No method | 15,020 (40.3%) | 1539 (36.7%) | 15,603 (40.3%) | 956 (36.7%) | ||
| Traditional method | 3203 (8.5%) | 419 (10.6%) | 3387 (8.5%) | 235 (10.6%) | ||
| Modern method | 19,375 (51.2%) | 2221 (52.7%) | 20,165 (51.2%) | 1431 (52.7%) | ||
| Knowledge about STI | <0.001 | <0.001 | ||||
| No | 10,254 (28.6%) | 1160 (29.2%) | 10,759 (28.6%) | 655 (29.2%) | ||
| Yes | 27,344 (71.4%) | 3019 (70.8%) | 28,396 (71.4%) | 1967 (70.8%) | ||
| Wife beating justified if she refuses to have sex | <0.001 | 0 (0.0%) | <0.001 | |||
| No | 34,526 (92.0%) | 3805 (91.4%) | 35,967 (92.0%) | 2364 (91.4%) | ||
| Yes | 3072 (8.0%) | 374 (8.6%) | 3188 (8.0%) | 258 (8.6%) | ||
| Decisions regarding own health care | <0.001 | <0.001 | ||||
| Wife | 5273 (13.4%) | 676 (15.6%) | 5523 (13.4%) | 426 (15.6%) | ||
| Wife and husband | 18,142 (48.2%) | 1797 (44.2%) | 18,748 (48.2%) | 1191 (44.2%) | ||
| Respondent and someone else | 2844 (8.1%) | 286 (7.0%) | 2973 (8.1%) | 157 (7.0%) | ||
| Husband | 11,339 (30.3%) | 1420 (33.2%) | 11,911 (30.3%) | 848 (33.2%) | ||
| Exposure to mass media | <0.001 | <0.001 | ||||
| Not at all | 12,879 (35.1%) | 1485 (36.0%) | 13,452 (35.1%) | 912 (36.0%) | ||
| Irregular | 3892 (10.4%) | 536 (12.7%) | 4127 (10.4%) | 301 (12.7%) | ||
| Regular | 20,827 (54.4%) | 2158 (51.3%) | 21,576 (54.4%) | 1409 (51.3%) | ||
| Model 1 | 95% CI | Model 2 | 95% CI | Model 3 | 95% CI | |
|---|---|---|---|---|---|---|
| Demographic factors | ||||||
| Age (Ref: 15–24 years) | ||||||
| 25–34 years | 1.17 ** | (1.06–1.30) | 1.17 ** | (1.05–1.29) | 1.14 ** | (1.03–1.27) |
| 35–49 years | 0.94 | (0.85–1.03) | 0.94 | (0.84–1.04) | 0.91 | (0.82–1.02) |
| Age at first marriage (Ref: 18 years or older) | ||||||
| 9–14 years | 1.41 *** | (1.27–1.56) | 1.22 *** | (1.09–1.37) | 1.21 *** | (1.08–1.36) |
| 15–17 years | 1.23 *** | (1.09–1.38) | 1.11 | (0.99–1.25) | 1.11 | (0.98–1.24) |
| Type of residence (Ref: Rural) | ||||||
| Urban | 1.16 ** | (1.04–1.28) | 1.01 | (0.90–1.13) | 1.02 | (0.91–1.15) |
| Socioeconomic factors | ||||||
| Education (Ref: No education) a | ||||||
| Primary | 1.12 | (0.99–1.26) | 1.08 | (0.95–1.23) | ||
| Secondary | 1 | (0.88–1.14) | 0.95 | (0.83–1.09) | ||
| Higher | 0.84 | (0.67–1.05) | 0.79* | (0.63–1.00) | ||
| Partner’s education (Ref: No education) a | ||||||
| Primary | 1.07 | (0.97–1.19) | 1.06 | (0.96–1.18) | ||
| Secondary | 0.97 | (0.86–1.10) | 0.96 | (0.85–1.08) | ||
| Higher | 0.86 | (0.72–1.03) | 0.84 | (0.71–1.01) | ||
| Wealth quintile (Ref: Poorest) | ||||||
| Poorer | 1.06 | (0.94–1.20) | 1.04 | (0.92–1.18) | ||
| Middle | 1.01 | (0.88–1.15) | 0.95 | (0.83–1.10) | ||
| Richer | 0.97 | (0.85–1.12) | 0.9 | (0.78–1.04) | ||
| Richest | 0.79 ** | (0.67–0.94) | 0.74 *** | (0.62–0.88) | ||
| Paid work status (Ref: No) c | ||||||
| Yes | 1.15 ** | (1.04–1.28) | 1.13 * | (1.02–1.26) | ||
| Behavioral factors | ||||||
| Contraceptive method (Ref: No method) | ||||||
| Traditional method | 1.42 *** | (1.23–1.64) | ||||
| Modern method | 1.09 * | (1.00–1.19) | ||||
| Knowledge about STI (Ref: No) a | ||||||
| Yes | 1.1 | (0.98–1.22) | ||||
| Wife beating justified (Ref: No) b | ||||||
| Yes | 1.03 | (0.90–1.18) | ||||
| Women’s healthcare decision-making (Ref: Wife) a | ||||||
| Wife and husband | 0.76 *** | (0.68–0.85) | ||||
| Respondent and someone else | 0.85 | (0.71–1.02) | ||||
| Husband | 0.91 | (0.80–1.04) | ||||
| Exposure to mass media (Ref: Not at all) | ||||||
| Irregular | 1.22 ** | (1.07–1.38) | ||||
| Regular | 1.11 * | (1.00–1.23) | ||||
| Survey year (Ref: 2007) | ||||||
| Survey Year = 2011 | 1.47 *** | (1.29–1.66) | 1.49 *** | (1.31–1.69) | 1.49 *** | (1.31–1.69) |
| Survey Year = 2014 | 1.57 *** | (1.37–1.79) | 1.54 *** | (1.35–1.76) | 1.56 *** | (1.37–1.78) |
| Constant | 0.05 *** | (0.05–0.06) | 0.07 *** | (0.05–0.08) | 0.07 *** | (0.05–0.09) |
| Observations | 41,777 | 41,777 | 41,777 |
| Model 1 | 95% CI | Model 2 | 95% CI | Model 3 | 95% CI | |
|---|---|---|---|---|---|---|
| Demographic factors | ||||||
| Age (Ref: 15–24 years) | ||||||
| 25–34 years | 1.22 *** | (1.09–1.37) | 1.24 *** | (1.10–1.40) | 1.21 ** | (1.06–1.37) |
| 35–49 years | 1.00 | (0.89–1.13) | 1.06 | (0.93–1.22) | 1.05 | (0.91–1.21) |
| Age at first marriage (Ref: 18 years or older) | ||||||
| 9–14 years | 1.13 | (0.99–1.28) | 1.07 | (0.94–1.23) | 1.06 | (0.93–1.22) |
| 15–17 years | 1.09 | (0.96–1.24) | 1.05 | (0.92–1.19) | 1.04 | (0.92–1.19) |
| Type of residence (Ref: Rural) | ||||||
| Urban | 1.14 * | (1.01–1.28) | 1.05 | (0.92–1.20) | 1.08 | (0.95–1.23) |
| Socioeconomic factors | ||||||
| Education (Ref: no education) a | ||||||
| Primary | 1.19 * | (1.03–1.37) | 1.14 | (0.99–1.31) | ||
| Secondary | 1.17 | (0.99–1.39) | 1.09 | (0.92–1.28) | ||
| Higher | 1.09 | (0.83–1.42) | 1.01 | (0.77–1.32) | ||
| Partner’s education (Ref: No education) a | ||||||
| Primary | 1.07 | (0.94–1.22) | 1.06 | (0.93–1.21) | ||
| Secondary | 1.02 | (0.88–1.19) | 1.01 | (0.86–1.17) | ||
| Higher | 0.95 | (0.77–1.19) | 0.94 | (0.76–1.17) | ||
| Wealth quintile (Ref: Poorest) | ||||||
| Poorer | 1.01 | (0.87–1.18) | 0.99 | (0.85–1.15) | ||
| Middle | 0.93 | (0.79–1.09) | 0.88 | (0.75–1.04) | ||
| Richer | 0.93 | (0.78–1.10) | 0.86 | (0.72–1.04) | ||
| Richest | 0.81 * | (0.67–0.99) | 0.75 ** | (0.61–0.93) | ||
| Paid work status (Ref: No) c | ||||||
| Yes | 1.23 ** | (1.09–1.38) | 1.20 ** | (1.07–1.36) | ||
| Behavioral factors | ||||||
| Contraceptive method (Ref: No method) | ||||||
| Traditional method | 1.09 | (0.92–1.31) | ||||
| Modern method | 1.07 | (0.96–1.18) | ||||
| Knowledge about STI (Ref: No) a | ||||||
| Yes | 1.26 *** | (1.11–1.42) | ||||
| Wife beating justified (Ref: No) b | ||||||
| Yes | 1.27 ** | (1.08–1.49) | ||||
| Women’s healthcare decision-making (Ref: wife) a | ||||||
| Wife and husband | 0.81 ** | (0.70–0.93) | ||||
| Respondent and someone else | 0.78 * | (0.62–0.98) | ||||
| Husband | 0.88 | (0.76–1.02) | ||||
| Exposure to mass media (Ref: Not at all) | ||||||
| Irregular | 1.02 | (0.86–1.20) | ||||
| Regular | 1.05 | (0.92–1.20) | ||||
| Survey year (Ref: 2007) | ||||||
| Survey Year = 2011 | 1.35 *** | (1.16–1.56) | 1.37 *** | (1.18–1.59) | 1.38 *** | (1.19–1.59) |
| Survey Year = 2014 | 1.05 | (0.90–1.23) | 1.02 | (0.88–1.19) | 1.03 | (0.88–1.20) |
| Constant | 0.04 *** | (0.04–0.05) | 0.04 *** | (0.03–0.05) | 0.04 *** | (0.03–0.06) |
| Observations | 41,777 | 41,777 | 41,777 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huda, M.N.; Ahmed, M.U.; Uddin, M.B.; Hasan, M.K.; Uddin, J.; Dune, T.M. Prevalence and Demographic, Socioeconomic, and Behavioral Risk Factors of Self-Reported Symptoms of Sexually Transmitted Infections (STIs) among Ever-Married Women: Evidence from Nationally Representative Surveys in Bangladesh. Int. J. Environ. Res. Public Health 2022, 19, 1906. https://doi.org/10.3390/ijerph19031906
Huda MN, Ahmed MU, Uddin MB, Hasan MK, Uddin J, Dune TM. Prevalence and Demographic, Socioeconomic, and Behavioral Risk Factors of Self-Reported Symptoms of Sexually Transmitted Infections (STIs) among Ever-Married Women: Evidence from Nationally Representative Surveys in Bangladesh. International Journal of Environmental Research and Public Health. 2022; 19(3):1906. https://doi.org/10.3390/ijerph19031906
Chicago/Turabian StyleHuda, Md. Nazmul, Moin Uddin Ahmed, Md. Bakhtiar Uddin, Md Kamrul Hasan, Jalal Uddin, and Tinashe Moira Dune. 2022. "Prevalence and Demographic, Socioeconomic, and Behavioral Risk Factors of Self-Reported Symptoms of Sexually Transmitted Infections (STIs) among Ever-Married Women: Evidence from Nationally Representative Surveys in Bangladesh" International Journal of Environmental Research and Public Health 19, no. 3: 1906. https://doi.org/10.3390/ijerph19031906
APA StyleHuda, M. N., Ahmed, M. U., Uddin, M. B., Hasan, M. K., Uddin, J., & Dune, T. M. (2022). Prevalence and Demographic, Socioeconomic, and Behavioral Risk Factors of Self-Reported Symptoms of Sexually Transmitted Infections (STIs) among Ever-Married Women: Evidence from Nationally Representative Surveys in Bangladesh. International Journal of Environmental Research and Public Health, 19(3), 1906. https://doi.org/10.3390/ijerph19031906