
Heat Strain and Use of Heat Mitigation Strategies among COVID-19 Healthcare Workers Wearing Personal Protective Equipment—A Retrospective Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Study Protocol
2.3. Data Analysis
3. Results
3.1. Participant Characteristics
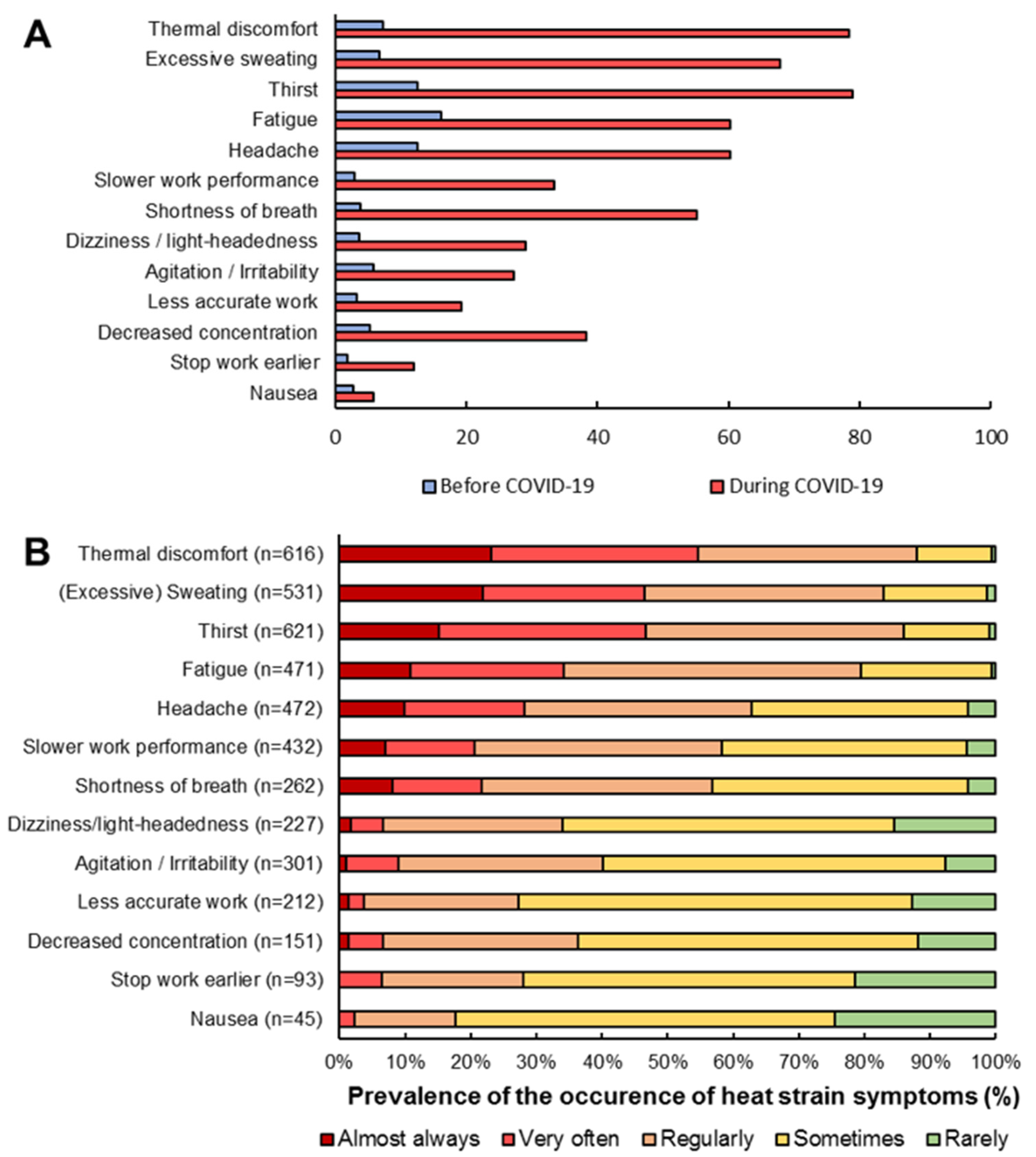
3.2. Prevalence of Heat Strain Symptoms
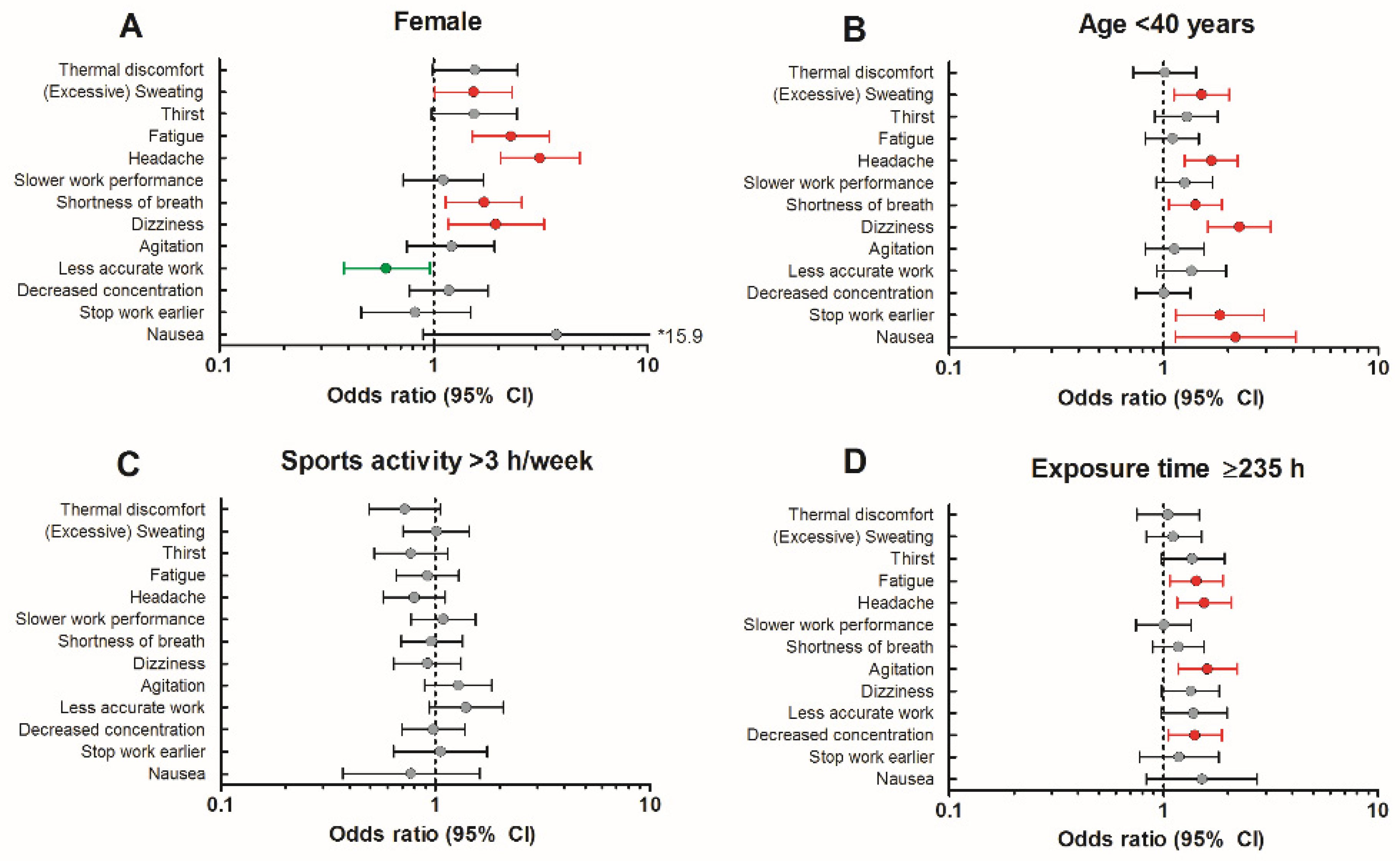
3.3. Factors Associated with Heat Strain Symptoms
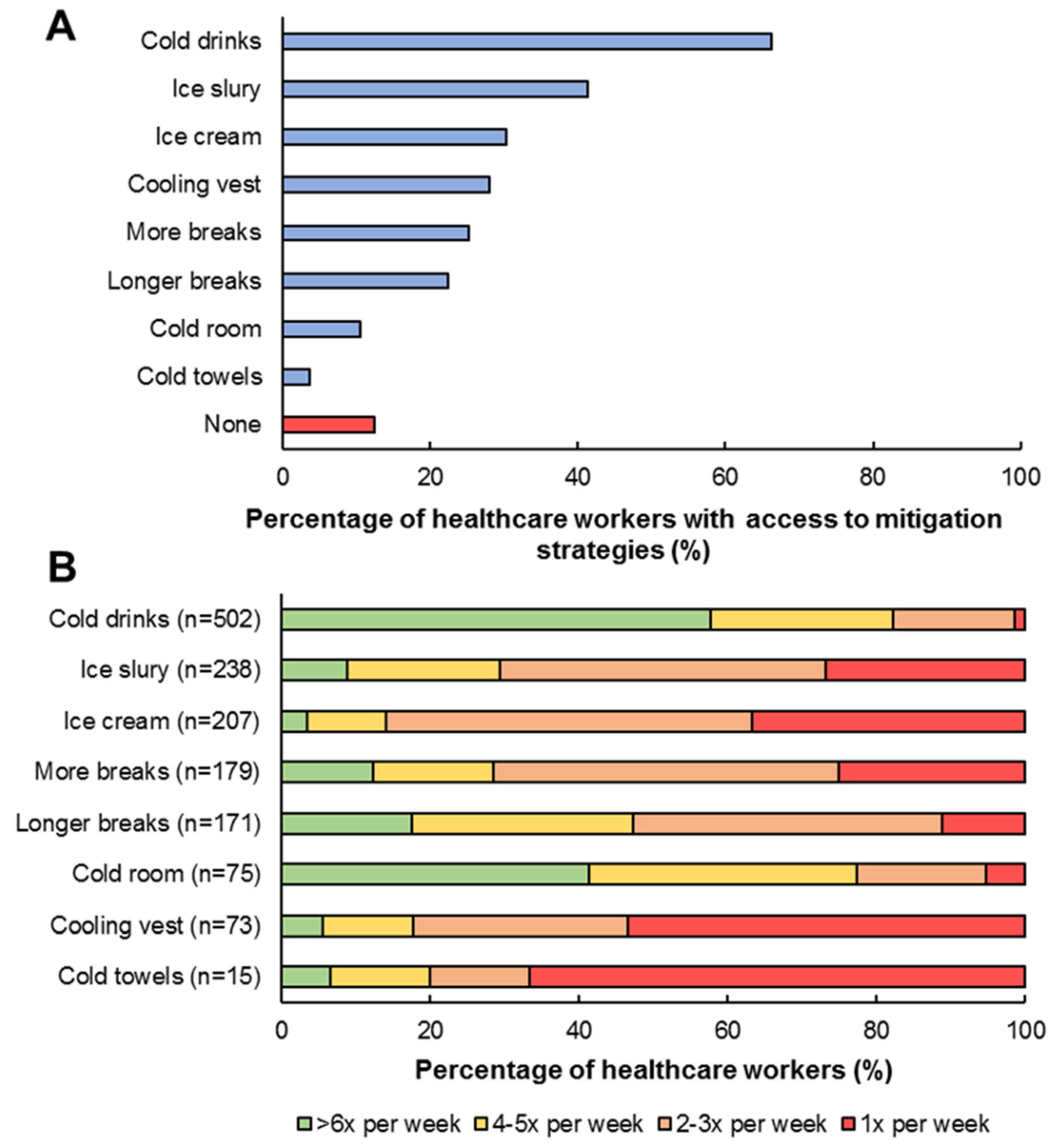
3.4. Heat Mitigation Strategies
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Liu, Q.; Luo, D.; Haase, J.E.; Guo, Q.; Wang, X.Q.; Liu, S.; Xia, L.; Liu, Z.; Yang, J.; Yang, B.X. The experiences of health-care providers during the COVID-19 crisis in China: A qualitative study. Lancet Glob. Health 2020, 8, e790–e798. [Google Scholar] [CrossRef]
- Greenberg, N.; Docherty, M.; Gnanapragasam, S.; Wessely, S. Managing mental health challenges faced by healthcare workers during COVID-19 pandemic. BMJ 2020, 368, m1211. [Google Scholar] [CrossRef] [Green Version]
- Verhoeven, V.; Tsakitzidis, G.; Philips, H.; Van Royen, P. Impact of the COVID-19 pandemic on the core functions of primary care: Will the cure be worse than the disease? A qualitative interview study in Flemish GPs. BMJ Open 2020, 10, e039674. [Google Scholar] [CrossRef] [PubMed]
- Ohta, R.; Ryu, Y.; Sano, C. Effects of Implementation of Infection Control Measures against COVID-19 on the Condition of Japanese Rural Nursing Homes. Int. J. Environ. Res. Public Health 2021, 18, 5805. [Google Scholar] [CrossRef] [PubMed]
- Davey, S.L.; Lee, B.J.; Robbins, T.; Randeva, H.; Thake, C.D. Heat stress and PPE during COVID-19: Impact on healthcare workers’ performance, safety and well-being in NHS settings. J. Hosp. Infect. 2021, 108, 185–188. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Venugopal, V.; Latha, P.K.; Alhadad, S.B.; Leow, C.H.W.; Goh, N.Y.; Tan, E.; Kjellstrom, T.; Morabito, M.; Lee, J.K.W. Heat Stress and Thermal Perception amongst Healthcare Workers during the COVID-19 Pandemic in India and Singapore. Int. J. Environ. Res. Public Health 2020, 17, 8100. [Google Scholar] [CrossRef] [PubMed]
- Messeri, A.B.M.; Pietrafesa, E.; Pinto, I.; de’Donato, F.; Crisci, A.; Lee, J.K.W.; Marinaccio, A.; Levi, M.; Morabito, A. Web Survey to Evaluate the Thermal Stress Associated with Personal Protective Equipment among Healthcare Workers during the COVID-19 Pandemic in Italy. Int. J. Environ. Res. Public Health 2021, 18, 3861. [Google Scholar] [CrossRef] [PubMed]
- Bongers, C.C.; de Korte, J.Q.; Catoire, M.; Greefhorst, J.; Hopman, M.T.E.; Kingma, B.; Eijsvogels, T.M.H. Infographic. Cooling strategies to attenuate PPE-induced heat strain during the COVID-19 pandemic. Br. J. Sports Med. 2021, 55, 69–70. [Google Scholar] [CrossRef]
- Bongers, C.C.; Hopman, M.T.; Eijsvogels, T.M. Cooling interventions for athletes: An overview of effectiveness, physiological mechanisms, and practical considerations. Temperature 2017, 4, 60–78. [Google Scholar] [CrossRef] [Green Version]
- Gao, C.; Kuklane, K.; Wang, F.; Holmer, I. Personal cooling with phase change materials to improve thermal comfort from a heat wave perspective. Indoor Air 2012, 22, 523–530. [Google Scholar] [CrossRef]
- Bongers, C.C.; Thijssen, D.H.; Veltmeijer, M.T.; Hopman, M.T.; Eijsvogels, T.M. Precooling and percooling (cooling during exercise) both improve performance in the heat: A meta-analytical review. Br. J. Sports Med. 2015, 49, 377–384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ciuha, U.; Gronkvist, M.; Mekjavic, I.B.; Eiken, O. Strategies for increasing evaporative cooling during simulated desert patrol mission. Ergonomics 2016, 59, 298–309. [Google Scholar] [CrossRef] [PubMed]
- Hemmatjo, R.; Motamedzade, M.; Aliabadi, M.; Kalatpour, O.; Farhadian, M. The effect of practical cooling strategies on physiological response and cognitive function during simulated firefighting tasks. Health Promot. Perspect. 2017, 7, 66–73. [Google Scholar] [CrossRef] [PubMed]
- de Korte, J.Q.; Bongers, C.C.W.G.; Catoire, M.; Kingma, B.R.M.; Eijsvogels, T.M.H. Cooling vests alleviate perceptual heat strain perceived by COVID-19 nurses. Temperature 2021, 1–11. [Google Scholar] [CrossRef]
- Periard, J.D.; Eijsvogels, T.M.H.; Daanen, H.A.M. Exercise under heat stress: Thermoregulation, hydration, performance implications, and mitigation strategies. Physiol. Rev. 2021, 101, 1873–1979. [Google Scholar] [CrossRef]
- Millyard, A.; Layden, J.D.; Pyne, D.B.; Edwards, A.M.; Bloxham, S.R. Impairments to Thermoregulation in the Elderly During Heat Exposure Events. Gerontol. Geriatr. Med. 2020, 6, 2333721420932432. [Google Scholar] [CrossRef]
- Flouris, A.D.; Dinas, P.C.; Ioannou, L.G.; Nybo, L.; Havenith, G.; Kenny, G.P.; Kjellstrom, T. Workers’ health and productivity under occupational heat strain: A systematic review and meta-analysis. Lancet Planet Health 2018, 2, e521–e531. [Google Scholar] [CrossRef] [Green Version]
- Taylor, N.A. Challenges to temperature regulation when working in hot environments. Ind. Health 2006, 44, 331–344. [Google Scholar] [CrossRef] [Green Version]
- McLellan, T.M. Sex-related differences in thermoregulatory responses while wearing protective clothing. Eur. J. Appl. Physiol. Occup. Physiol. 1998, 78, 28–37. [Google Scholar] [CrossRef]
- Dufour, A.; Candas, V. Ageing and thermal responses during passive heat exposure: Sweating and sensory aspects. Eur. J. Appl. Physiol. 2007, 100, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Kenney, W.L.; Munce, T.A. Invited review: Aging and human temperature regulation. J. Appl. Physiol. (1985) 2003, 95, 2598–2603. [Google Scholar] [CrossRef] [PubMed]
- Kjellstrom, T.; Holmer, I.; Lemke, B. Workplace heat stress, health and productivity—An increasing challenge for low and middle-income countries during climate change. Glob. Health Action 2009, 2, 2047. [Google Scholar] [CrossRef] [PubMed]
- Grahn, D.; Makam, M.; Craig Heller, H. A method to reduce heat strain while clad in encapsulating outerwear. J. Occup. Environ. Hyg. 2018, 15, 573–579. [Google Scholar] [CrossRef] [PubMed]
- Sun, N.; Wei, L.; Shi, S.; Jiao, D.; Song, R.; Ma, L.; Wang, H.; Wang, C.; Wang, Z.; You, Y.; et al. A qualitative study on the psychological experience of caregivers of COVID-19 patients. Am. J. Infect. Control. 2020, 48, 592–598. [Google Scholar] [CrossRef] [PubMed]
- Ruskin, K.J.; Ruskin, A.C.; Musselman, B.T.; Harvey, J.R.; Nesthus, T.E.; O’Connor, M. COVID-19, Personal Protective Equipment, and Human Performance. Anesthesiology 2021, 134, 518–525. [Google Scholar] [CrossRef]
- Foster, J.; Hodder, S.G.; Goodwin, J.; Havenith, G. Occupational Heat Stress and Practical Cooling Solutions for Healthcare and Industry Workers During the COVID-19 Pandemic. Ann. Work Expo. Health 2020, 64, 915–922. [Google Scholar] [CrossRef]
- Lamarche, D.T.; Meade, R.D.; D’Souza, A.W.; Flouris, A.D.; Hardcastle, S.G.; Sigal, R.J.; Boulay, P.; Kenny, G.P. The recommended Threshold Limit Values for heat exposure fail to maintain body core temperature within safe limits in older working adults. J. Occup. Environ. Hyg. 2017, 14, 703–711. [Google Scholar] [CrossRef]
- Meade, R.D.; Poirier, M.P.; Flouris, A.D.; Hardcastle, S.G.; Kenny, G.P. Do the Threshold Limit Values for Work in Hot Conditions Adequately Protect Workers? Med. Sci. Sports Exerc. 2016, 48, 1187–1196. [Google Scholar] [CrossRef]
- Tabah, A.; Ramanan, M.; Laupland, K.B.; Buetti, N.; Cortegiani, A.; Mellinghoff, J.; Conway Morris, A.; Camporota, L.; Zappella, N.; Elhadi, M.; et al. Personal protective equipment and intensive care unit healthcare worker safety in the COVID-19 era (PPE-SAFE): An international survey. J. Crit. Care 2020, 59, 70–75. [Google Scholar] [CrossRef]
- Gezondheidszorg, C.I.B. Hoeveel Zorgverleners Staan er in Het BIG-Register? Available online: https://www.bigregister.nl/over-het-big-register/cijfers (accessed on 20 January 2022).




{kind=link}
{kind=link}
{kind=link}
| Participant Characteristics | Total Group (n = 791) | Male (n = 108) | Female (n = 683) |
|---|---|---|---|
| Age (years) | 32 [27–45] | 33 [29–45] | 32 [26–45] |
| Height (cm) | 173 ± 8 | 183 ± 8 | 171 ± 7 |
| Weight (kg) | 71.0 [64.0–80.0] | 82.0 [75.0–90.8] | 70.0 [63.0–79.0] |
| BMI (kg/m2) | 23.8 [21.6–26.7] | 24.5 [22.2–26.3] | 23.7 [21.5–26.8] |
| Sports activity level (hours per week) | |||
| <1 h (n(%)) | 170 (21.5%) | 19 (17.6%) | 151 (22.1%) |
| 1–3 h (n(%)) | 437 (55.2%) | 48 (44.4%) | 389 (57.0%) |
| 4–6 h (n(%)) | 164 (20.7%) | 32 (29.6%) | 132 (19.3%) |
| ≥7 h (n(%)) | 20 (2.5%) | 9 (8.3%) | 11 (1.6%) |
| Type of work | |||
| Medium care/Intensive care (n(%)) | 328 (41.5%) | 62 (57.4%) | 266 (38.9%) |
| Nursing ward (n(%)) | 406 (51.3%) | 35 (32.4%) | 371 (54.3%) |
| First aid/Emergency care (n(%)) | 26 (3.3%) | 5 (4.6%) | 21 (3.1%) |
| Other medical departments (n(%)) | 31 (3.9%) | 6 (5.6%) | 25 (3.7%) |
| Number of weeks at COVID-19 ward | 10 [6–10] | 10 [6–10] | 10 [6–10] |
| Hours per week at COVID-19 ward | 28 [24–28] | 28 [24–28] | 28 [24–28] |
| Exposure time (hours) | 235 [141–280] | 209 [168–280] | 235 [141–280] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bongers, C.C.W.G.; de Korte, J.Q.; Zwartkruis, M.; Levels, K.; Kingma, B.R.M.; Eijsvogels, T.M.H. Heat Strain and Use of Heat Mitigation Strategies among COVID-19 Healthcare Workers Wearing Personal Protective Equipment—A Retrospective Study. Int. J. Environ. Res. Public Health 2022, 19, 1905. https://doi.org/10.3390/ijerph19031905
Bongers CCWG, de Korte JQ, Zwartkruis M, Levels K, Kingma BRM, Eijsvogels TMH. Heat Strain and Use of Heat Mitigation Strategies among COVID-19 Healthcare Workers Wearing Personal Protective Equipment—A Retrospective Study. International Journal of Environmental Research and Public Health. 2022; 19(3):1905. https://doi.org/10.3390/ijerph19031905
Chicago/Turabian StyleBongers, Coen C. W. G., Johannus Q. de Korte, Mike Zwartkruis, Koen Levels, Boris R. M. Kingma, and Thijs M. H. Eijsvogels. 2022. "Heat Strain and Use of Heat Mitigation Strategies among COVID-19 Healthcare Workers Wearing Personal Protective Equipment—A Retrospective Study" International Journal of Environmental Research and Public Health 19, no. 3: 1905. https://doi.org/10.3390/ijerph19031905
APA StyleBongers, C. C. W. G., de Korte, J. Q., Zwartkruis, M., Levels, K., Kingma, B. R. M., & Eijsvogels, T. M. H. (2022). Heat Strain and Use of Heat Mitigation Strategies among COVID-19 Healthcare Workers Wearing Personal Protective Equipment—A Retrospective Study. International Journal of Environmental Research and Public Health, 19(3), 1905. https://doi.org/10.3390/ijerph19031905