
Use of E-Health in Dutch General Practice during the COVID-19 Pandemic


Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample and Data Collection
2.2. Web Survey
2.3. General Practice Type Definition
2.4. Data Analysis
3. Results
3.1. Sample Characteristics
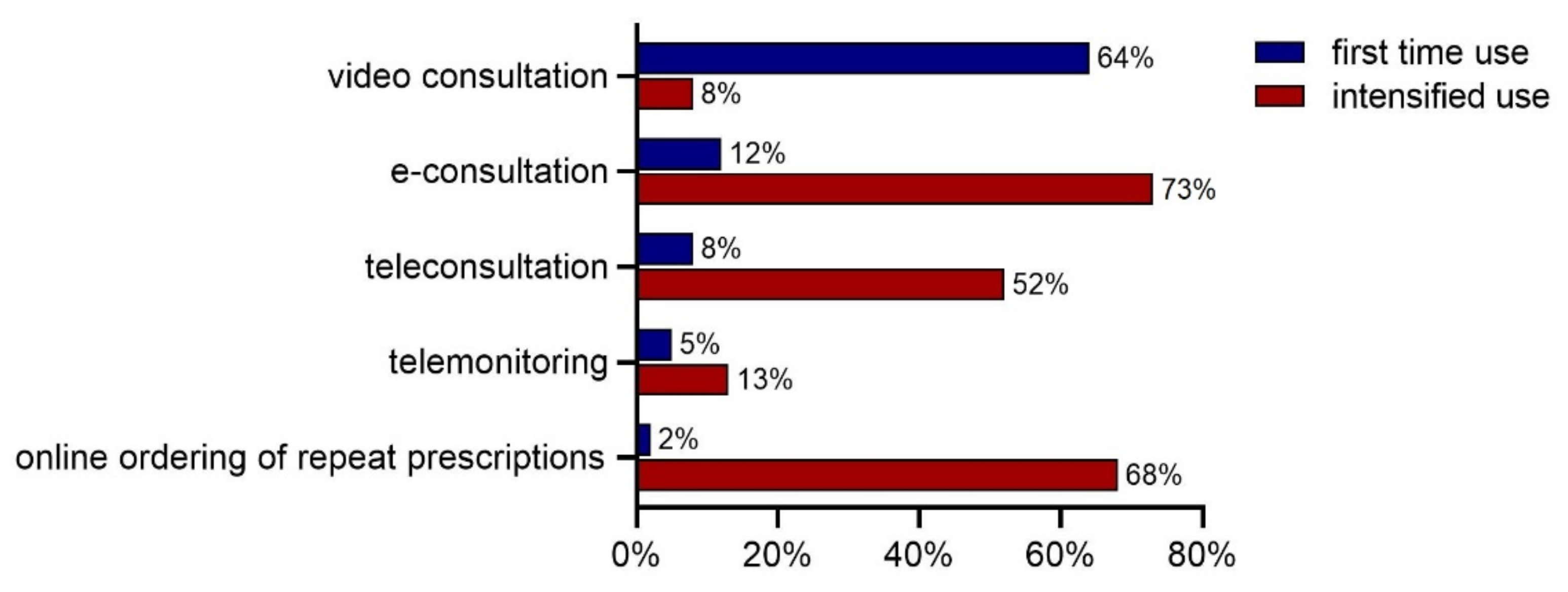
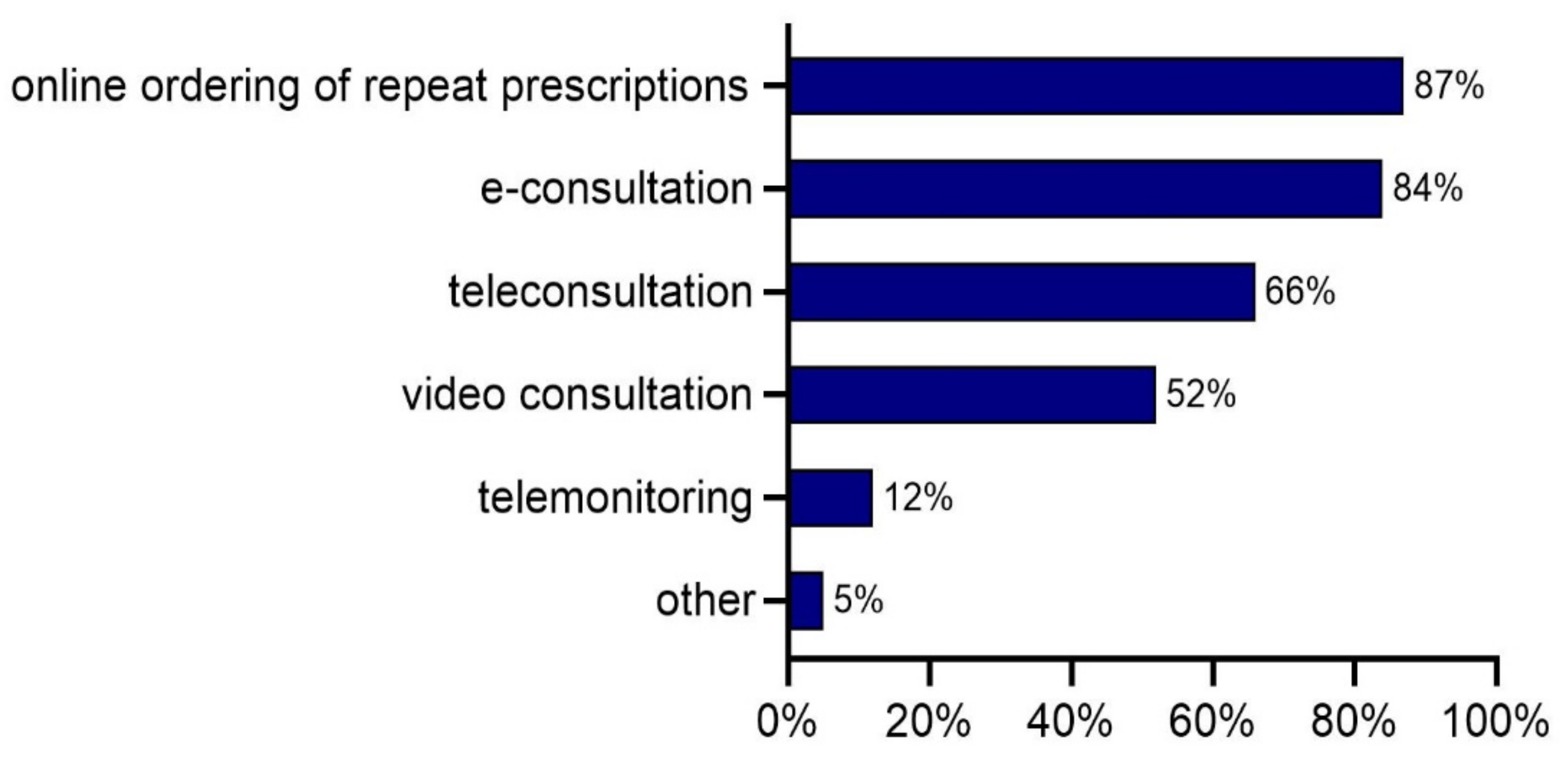
3.2. Use of E-Health
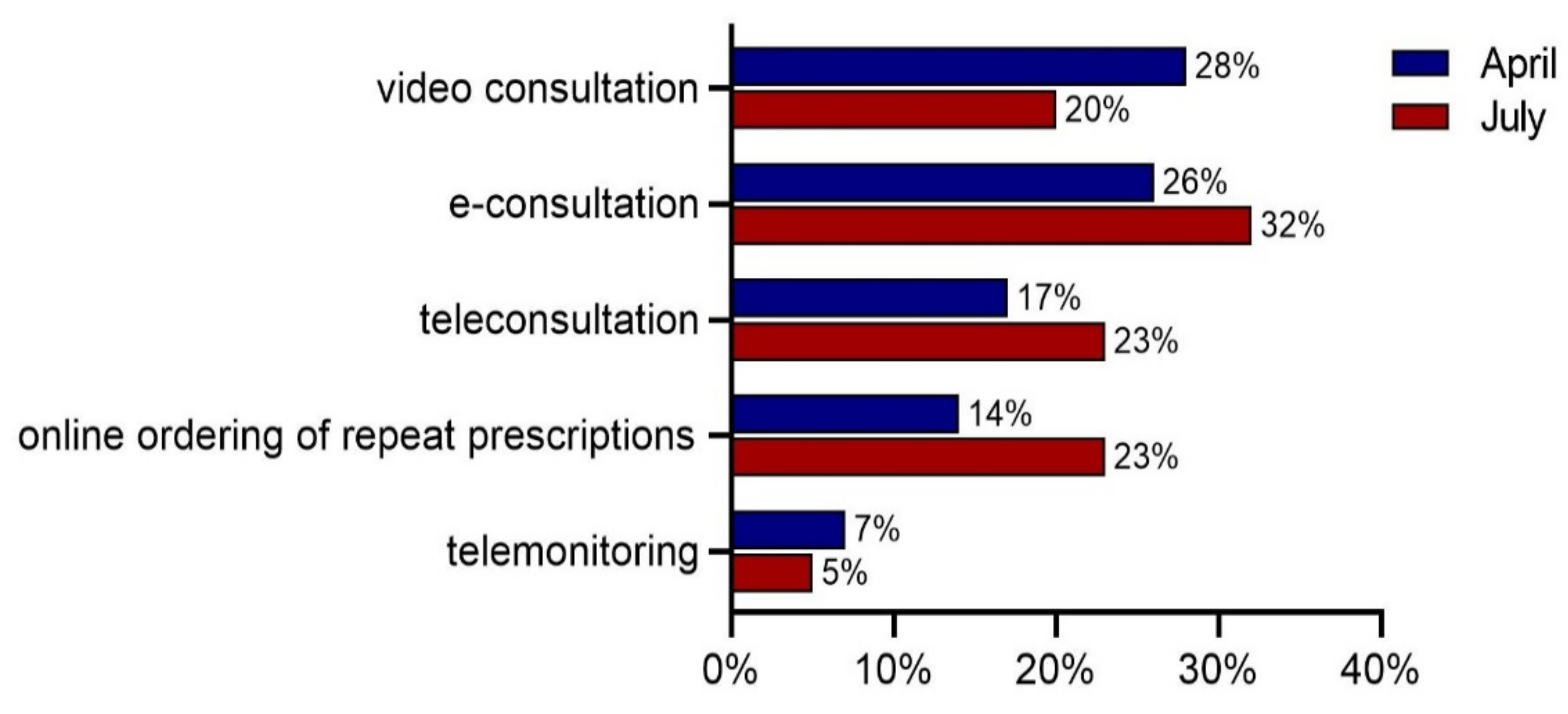
3.3. Intention to Maintain Use of E-Health
3.4. Practice Type Differences
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Huston, P.; Campbell, J.; Russell, G.; Goodyear-Smith, F.; Phillips, R.L.; van Weel, C.; Hogg, W. COVID-19 and primary care in six countries. BJGP Open 2020, 4. [Google Scholar] [CrossRef] [PubMed]
- Bokolo, A.J. Application of telemedicine and eHealth technology for clinical services in response to COVID-19 pandemic. Health Technol. 2021, 11, 359–366. [Google Scholar] [CrossRef] [PubMed]
- COVID-19 Health System Response Monitor. Policy Responses for Netherlands. Available online: https://www.covid19healthsystem.org/countries/netherlands/livinghit.aspx?Section=3.1%20Planning%20services&Type=Section (accessed on 20 January 2021).
- (NHG). GPs and the Dutch Helathcare System. Available online: https://www.nhg.org/english/gp-dutch-healthcare-system (accessed on 20 October 2021).
- Statistics Netherlands (CBS). More People Feeling Healthy in Q2 2020. Available online: https://www.cbs.nl/en-gb/news/2020/35/more-people-feeling-healthy-in-q2-2020 (accessed on 18 August 2021).
- Schers, H.; van Weel, C.; van Boven, K.; Akkermans, R.; Bischoff, E.; olde Hartman, T. The COVID-19 Pandemic in Nijmegen, the Netherlands: Changes in Presented Health Problems and Demand for Primary Care. Ann. Fam. Med. 2021, 19, 44–47. [Google Scholar] [CrossRef] [PubMed]
- Wouters, M.; Huygens, M.; Voogdt, H.; Meurs, M.; de Groot, J.; de Bruin, K.; Brabers, A.; Hofstede, C.; Friele, R.; van Gennip, L. Samen Aan Zet! eHealth-Monitor 2019; Nictiz, Nivel: Den Haag/Utrecht, the Netherlands, 2019. [Google Scholar]
- Valverde-Albacete, J.; Folkvord, F.; Lupiáñez-Villanueva, F.; Hocking, L.; Devaux, A.; Altenhofer, M.; Harshfield, A.; Fauli, C. Benchmarking Deployment of eHealth among General Practitioners (2018); European Commission: Luxembourg, 2019. [Google Scholar]
- Batenburg, R. Healthcare Professionals Registries. Available online: https://www.nivel.nl/en/beroepenregistraties-de-gezondheidszorg/healthcare-professionals-registries (accessed on 28 July 2021).
- Ajzen, I. The theory of planned behavior. Organ. Behav. Hum. Decis. Process. 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Rogers, E.M. Diffusion of Innovations, 5th ed.; Free Press: New York, NY, USA, 2003. [Google Scholar]
- Davis, F.D. A Technology Acceptance Model for Empirically Testing New End-User Information Systems: Theory and Results; Massachusetts Institute of Technology: Cambridge, MA, USA, 1986. [Google Scholar]
- Tornatzky, L.G.; Fleischer, M.; Chakrabarti, A.K. The Processes of Technological Innovation; Lexington Books: Lexington, MA, USA, 1990. [Google Scholar]
- Wynn, R. E-Health in Norway Before and During the Initial Phase of the COVID-19 Pandemic. Stud. Health Technol. Inform. 2020, 272, 9–12. [Google Scholar] [CrossRef] [PubMed]
- Snoswell, C.L.; Caffery, L.J.; Haydon, H.M.; Thomas, E.E.; Smith, A.C. Telehealth uptake in general practice as a result of the coronavirus (COVID-19) pandemic. Aust. Health Rev. 2020, 44, 737–740. [Google Scholar] [CrossRef] [PubMed]
- Johnsen, T.M.; Norberg, B.L.; Kristiansen, E.; Zanaboni, P.; Austad, B.; Krogh, F.H.; Getz, L. Suitability of Video Consultations During the COVID-19 Pandemic Lockdown: Cross-sectional Survey Among Norwegian General Practitioners. J. Med. Internet Res. 2021, 23, e26433. [Google Scholar] [CrossRef] [PubMed]
- McKinsey&Company. Telehealth: A Quarter-Trillion-Dollar Post-COVID-19 Reality. Available online: https://www.mckinsey.com/industries/healthcare-systems-and-services/our-insights/telehealth-a-quarter-trillion-dollar-post-covid-19-reality# (accessed on 13 April 2021).
- Friends of Europe. A Highly Desirable Revolution in Digital Health. Available online: https://www.friendsofeurope.org/insights/a-highly-desirable-revolution-in-digital-health/ (accessed on 13 April 2021).
- Garg, S.; Gangadharan, N.; Bhatnagar, N.; Singh, M.; Raina, S.; Galwankar, S. Telemedicine: Embracing virtual care during COVID-19 pandemic. J. Fam. Med. Prim. Care 2020, 9, 4516–4520. [Google Scholar] [CrossRef]
- Bhaskar, S.; Bradley, S.; Chattu, V.K.; Adisesh, A.; Nurtazina, A.; Kyrykbayeva, S.; Sakhamuri, S.; Yaya, S.; Sunil, T.; Thomas, P.; et al. Telemedicine Across the Globe-Position Paper From the COVID-19 Pandemic Health System Resilience PROGRAM (REPROGRAM) International Consortium (Part 1). Front. Public Health 2020, 8. [Google Scholar] [CrossRef] [PubMed]
- Socha-Dietrich, K. Empowering the Health Workforce to Make the Most of the Digital Revolution; OECD Publishing: Paris, France, 2021. [Google Scholar] [CrossRef]
- Bush, M.; Lederer, A.L.; Li, X.; Palmisano, J.; Rao, S. The alignment of information systems with organizational objectives and strategies in health care. Int. J. Med. Inform. 2009, 78, 446–456. [Google Scholar] [CrossRef] [PubMed]
- Kidholm, K.; Ekeland, A.G.; Jensen, L.K.; Rasmussen, J.; Pedersen, C.D.; Bowes, A.; Flottorp, S.A.; Bech, M. A model for assessment of telemedicine applications: Mast. Int. J. Technol. Assess. Health Care 2012, 28, 44–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Partners of the TeleSCoPE Project. Draft European Code of Practice for Telehealth Services; TeleSCoPE: Coventry, UK, 2014; p. 60. [Google Scholar]
- Jensen, L.K.; Knarvik, U.; Pedersen, C.D.; Tangene, W.; Whitehouse, D. Personalised Blueprint for Telemedicine Deployment: Validated and Tested Version; Momentum: Brussels, Belgium, 2015. [Google Scholar]
- Vis, C.; Bührmann, L.; Riper, H.; Ossebaard, H.C. Health technology assessment frameworks for eHealth: A systematic review. Int. J. Technol. Assess. Health Care 2020, 36, 204–216. [Google Scholar] [CrossRef] [PubMed]
- Florea, M.; Lazea, C.; Gaga, R.; Sur, G.; Lotrean, L.; Puia, A.; Stanescu, A.; Lupsor-Platon, M.; Florea, H.; Sur, M. Lights and Shadows of the Perception of the Use of Telemedicine by Romanian Family Doctors During the COVID-19 Pandemic. Int. J. Gen. Med. 2021, 14, 1575–1587. [Google Scholar] [CrossRef] [PubMed]
- Gomez, T.; Anaya, Y.B.; Shih, K.J.; Tarn, D.M. A Qualitative Study of Primary Care Physicians’ Experiences With Telemedicine During COVID-19. J. Am. Board Fam. Med. 2021, 34, S61–S70. [Google Scholar] [CrossRef] [PubMed]
- Scott, A.; Bai, T.; Zhang, Y. Association between telehealth use and general practitioner characteristics during COVID-19: Findings from a nationally representative survey of Australian doctors. BMJ Open 2021, 11, e046857. [Google Scholar] [CrossRef] [PubMed]
- Miner, H.; Fatehi, A.; Ring, D.; Reichenberg, J.S. Clinician Telemedicine Perceptions During the COVID-19 Pandemic. Telemed. e-Health 2021, 27, 508–512. [Google Scholar] [CrossRef] [PubMed]
- Thomas, E.E.; Haydon, H.M.; Mehrotra, A.; Caffery, L.J.; Snoswell, C.L.; Banbury, A.; Smith, A.C. Building on the momentum: Sustaining telehealth beyond COVID-19. J. Telemed. Telecare 2020, 1–8. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| E-Health Application | Solo Practice (n = 211) | Duo Practice (n = 480) | Group Practice (n = 383) | p-Value |
|---|---|---|---|---|
| E-consultation | 15% ± 0.355 | 12% ± 0.326 | 9% ± 0.289 | 0.114 |
| Online ordering of repeat prescriptions | 2% ± 0.137 | 1% ± 0.120 | 1% ± 0.114 | 0.849 |
| Video consultation | 60% ± 0.492 | 64% ± 0.482 | 67% ± 0.470 | 0.190 |
| Teleconsultation | 12% ± 0.324 | 6% ± 0.235 | 9% ± 0.292 | 0.019 * |
| Telemonitoring | 7% ± 0.258 | 4% ± 0.185 | 5% ± 0.228 | 0.113 |
| Other | 3% ± 0.167 | 2% ± 0.143 | 4% ± 0.200 | 0.179 |
| E-Health Application | Solo Practice (n = 149) | Duo Practice (n = 304) | Group Practice (n = 282) | p-Value |
|---|---|---|---|---|
| E-consultation | 83% ± 0.381 | 83% ± 0.380 | 83% ± 0.373 | 0.964 |
| Online ordering of repeat prescriptions | 81% ± 0.392 | 87% ± 0.331 | 88% ± 0.330 | 0.134 |
| Video consultation | 44% ± 0.498 | 51% ± 0.501 | 56% ± 0.498 | 0.058 |
| Teleconsultation | 51% ± 0.502 | 67% ± 0.417 | 70% ± 0.460 | 0.000 * |
| Telemonitoring | 8% ± 0.273 | 12% ± 0.324 | 13% ± 0.338 | 0.289 |
| Other | 7% ± 0.262 | 5% ± 0.217 | 10% ± 0.295 | 0.095 |
| None | 5% ± 0.212 | 1% ± 0.099 | 1% ± 0.118 | 0.019 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Keuper, J.; Batenburg, R.; Verheij, R.; van Tuyl, L. Use of E-Health in Dutch General Practice during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 12479. https://doi.org/10.3390/ijerph182312479
Keuper J, Batenburg R, Verheij R, van Tuyl L. Use of E-Health in Dutch General Practice during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2021; 18(23):12479. https://doi.org/10.3390/ijerph182312479
Chicago/Turabian StyleKeuper, Jelle, Ronald Batenburg, Robert Verheij, and Lilian van Tuyl. 2021. "Use of E-Health in Dutch General Practice during the COVID-19 Pandemic" International Journal of Environmental Research and Public Health 18, no. 23: 12479. https://doi.org/10.3390/ijerph182312479
APA StyleKeuper, J., Batenburg, R., Verheij, R., & van Tuyl, L. (2021). Use of E-Health in Dutch General Practice during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health, 18(23), 12479. https://doi.org/10.3390/ijerph182312479