
Relationships between Plantar Pressure Distribution and Rearfoot Alignment in the Taiwanese College Athletes with Plantar Fasciopathy during Static Standing and Walking


Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Instruments and Equipment
2.3. PPDs Assessment
- Roll both trouser legs up to above the knees to prevent the clothing from limiting movements of the extremities;
- Stand barefoot on the sensing cushion with the specific marks and measuring range of the JC Mat;
- Relax the body. Control and balance the center of gravity by standing with feet shoulder-width apart and with body weight evenly distributed on feet;
- Stampede for six to eight steps, then stand still with a natural posture and arms hanging straight down at the sides;
- Face the experiment instructor. Look the instructor straight in the eye. Keep the body stationary and balanced until no obvious changes are seen in the foot pressure value measured by the JC Mat.
2.4. PPDs Data Analysis
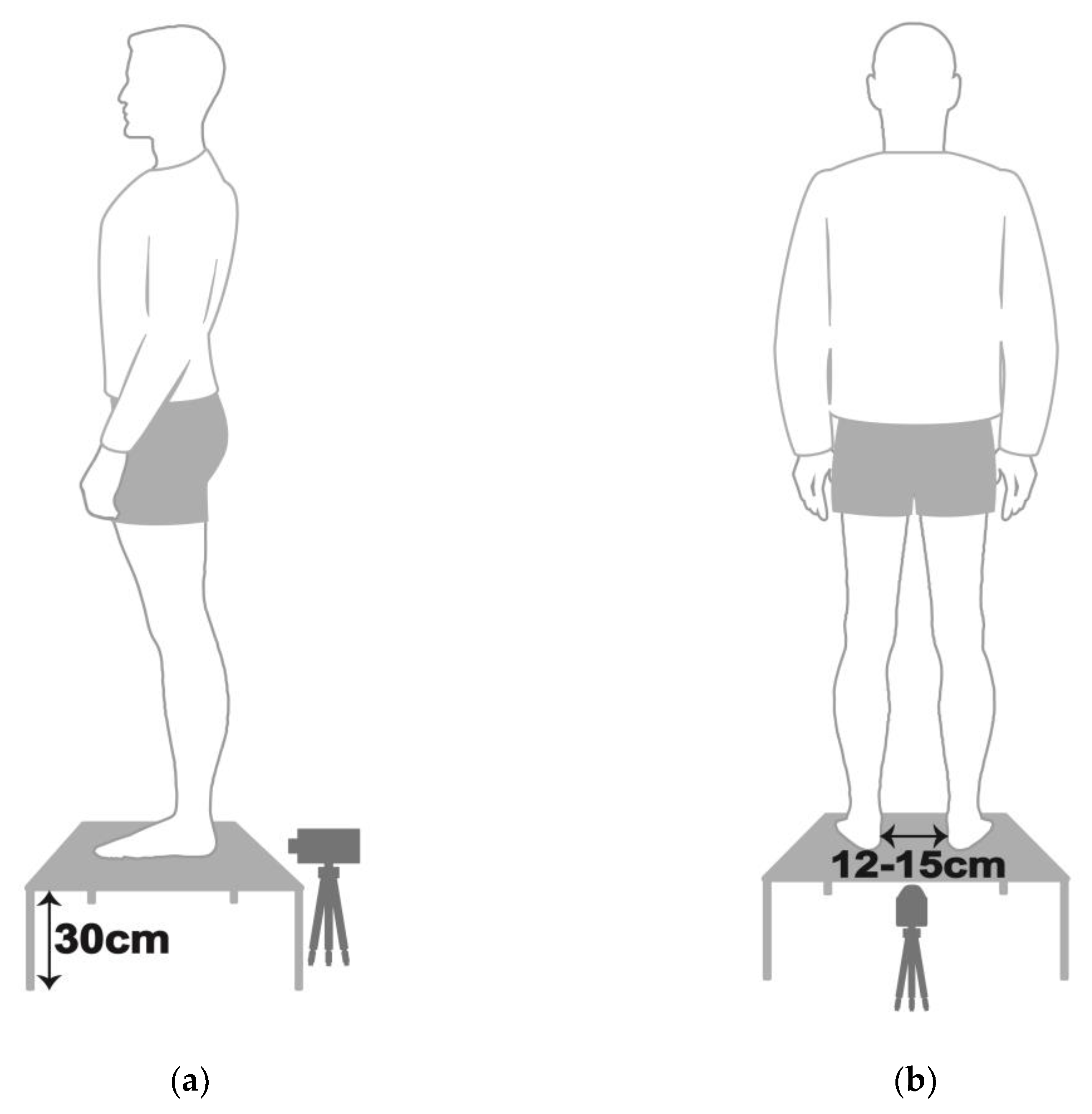
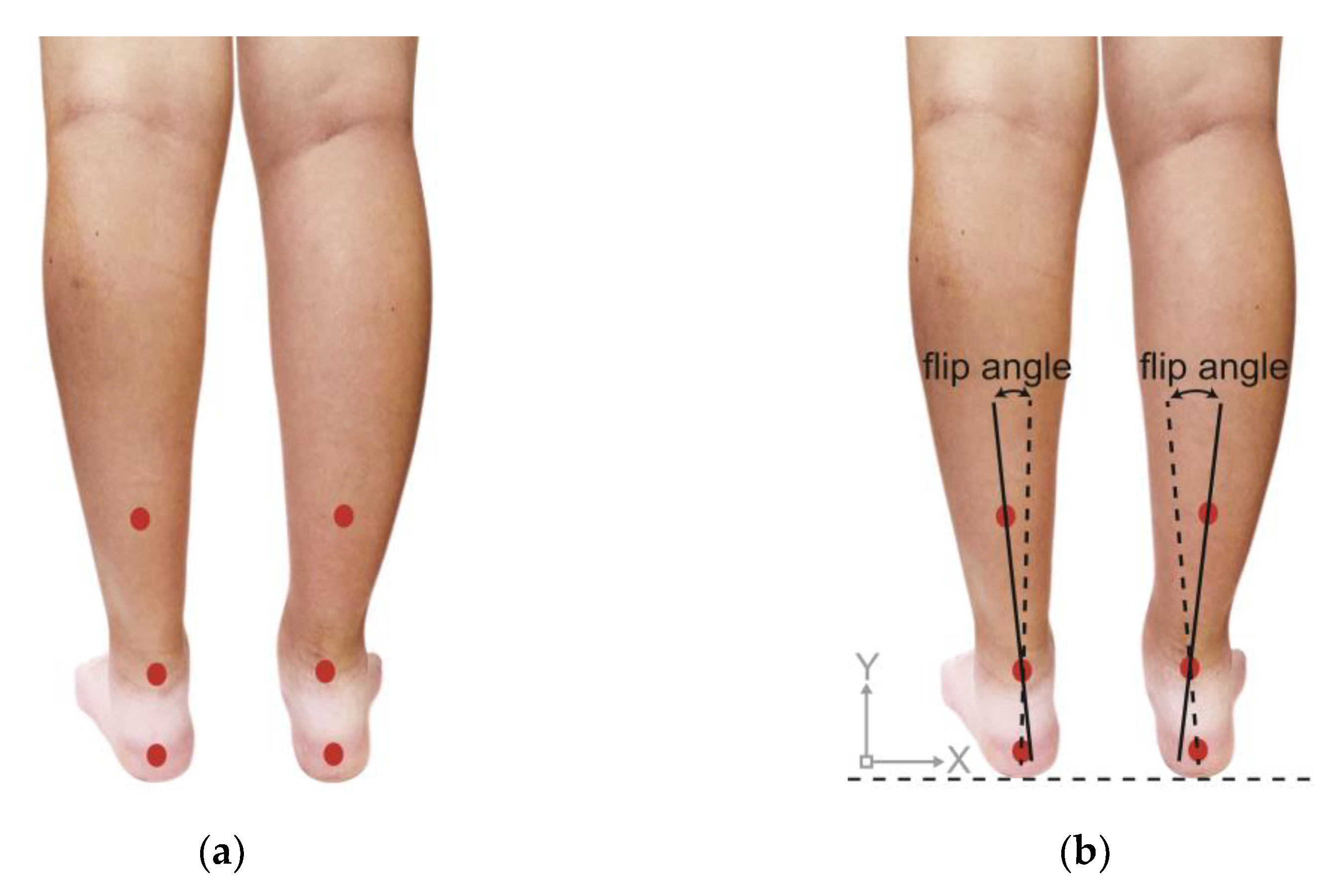
2.5. Rearfoot Postural Alignment Assessment
2.6. Self-Reported Health Status Examination
2.7. Pain Assessment
- Plantar pain reproduced by palpating the plantar medial calcaneal tubercle at the site of the plantar fascial insertion on the heel bone;
- Plantar pain reproduced with passive dorsiflexion of the foot and toes;
- Passive dorsiflexion of the first metatarsophalangeal joint (test to provoke symptoms at the plantar fascia by creating maximal stretch), positive test if the pain is reproduced.
- The physiotherapist examined the PF athletes’ self-reported health status and pain complaints, and guided them to stand with bare feet and roll their trouser legs up to above the knees.
- The physiotherapist examined the PF participants’ lower extremities by palpating and pressing their feet (including navicular bones, cuboid bones, phalanges, metatarsals, and calcaneus), ankles, patella, knees, hips, tibias, fibulas and femur according to the participants’ self-reported health status, and re-examined the corresponding position on the other side of the pain areas. The physiotherapist, then, assessed the skeletal arrangement of the participants’ lower limbs.
- In order to confirm the participants’ pain areas precisely, the physiotherapist examined the following specific parts of the participants’ common pain areas: (1) soft tissues, e.g., the plantar fascia, the Achilles tendon, the gastrocnemius, the tibialis anterior and posterior, the biceps, the quadriceps femoris, the medial and lateral ankle ligaments, the anterior cruciate ligaments, the medial and lateral collateral ligaments, the abductor hallucis and abductor digiti minimi of plantar plate and the lower back; (2) bone tissues of both feet, i.e., navicular bones, cuboid bones, phalanges, metatarsals, and calcaneus; (3) the ankles; (4) the patella; (5) the knees; (6) the hips and (7) tibias.
2.8. Statistical Analysis
3. Results
3.1. Arch Index
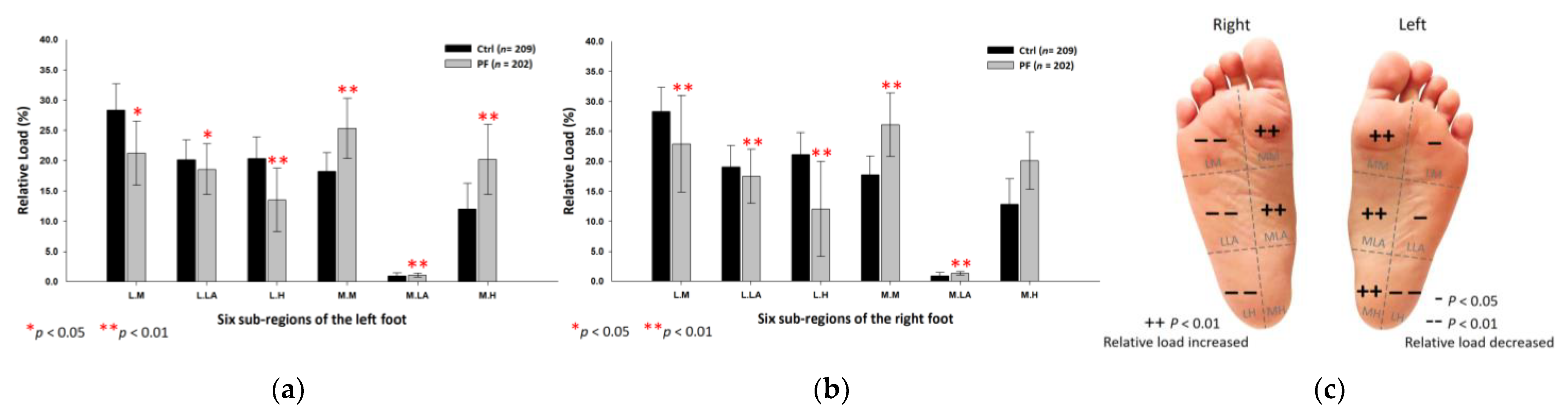
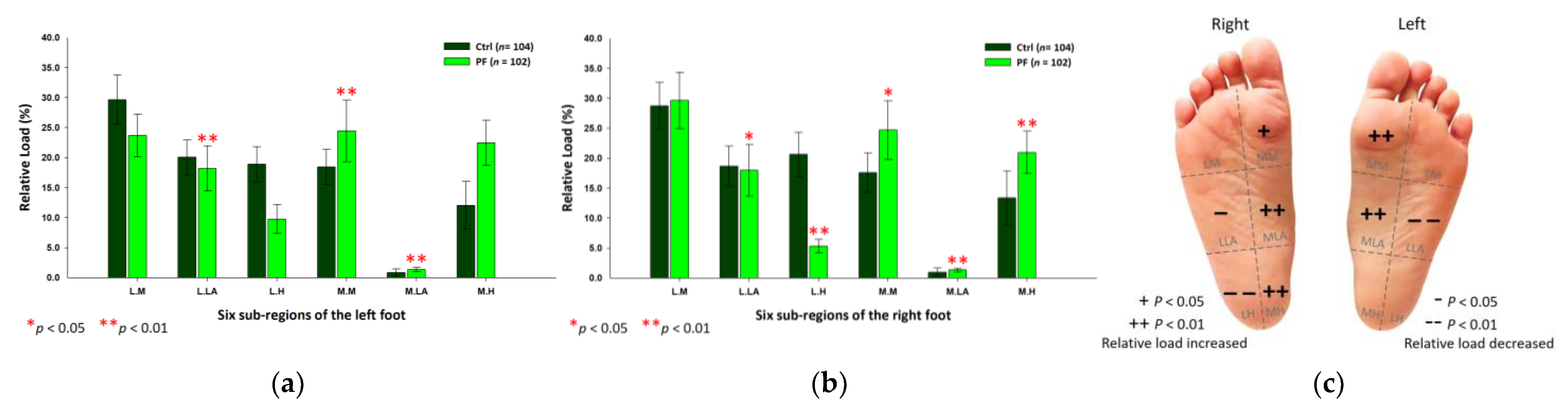
3.2. PPDs Assessment in Static Standing
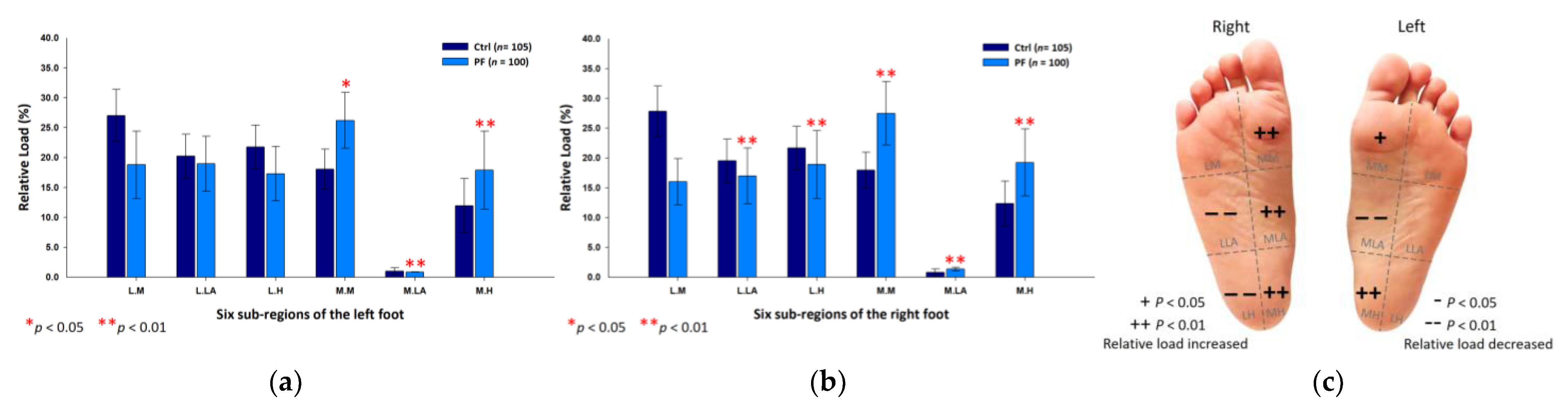
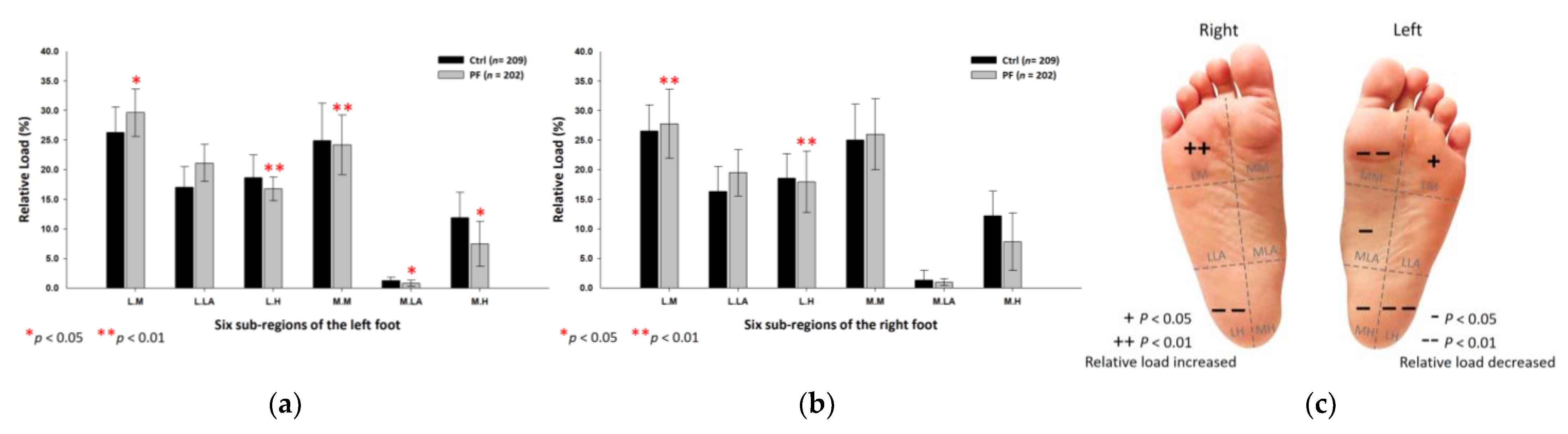
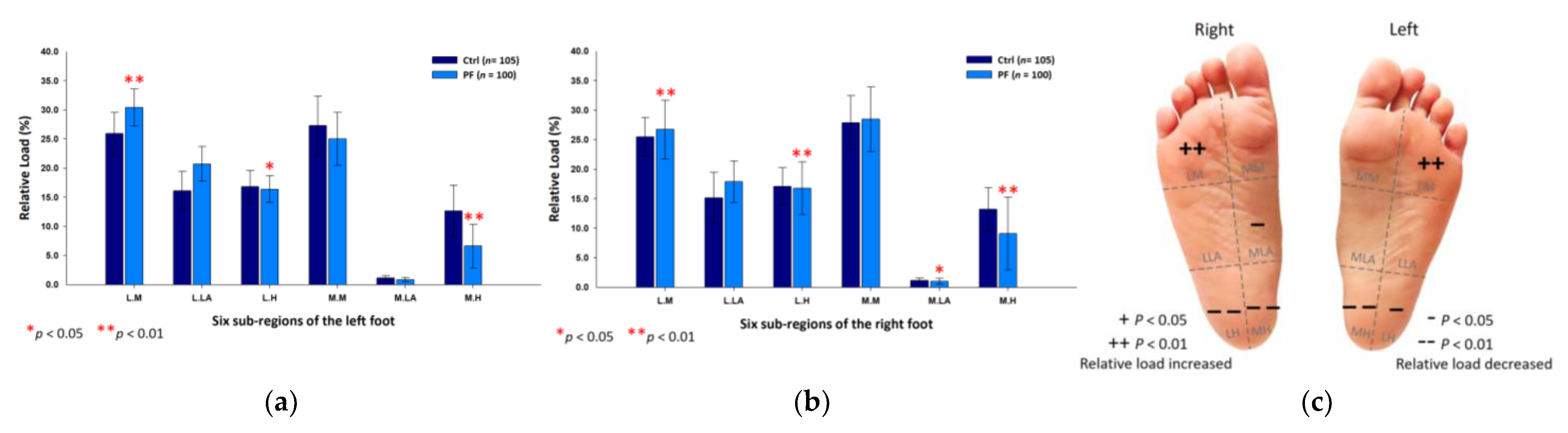
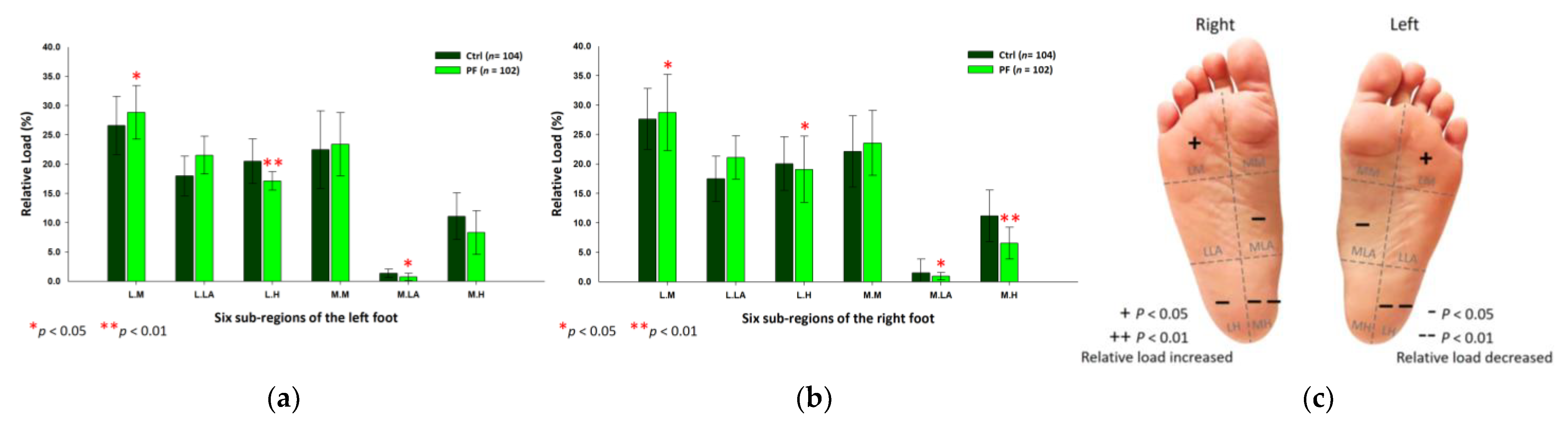
3.3. PPDs Assessment during the Midstance Phase of Walking
3.4. PPDs of the Static Standing Versus the Midstance Phase of Walking
3.5. Rearfoot Postural Alignment Assessment
3.6. Self-Reported Health Status and Pain Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Taunton, J.E.; Ryan, M.B.; Clement, D.B.; McKenzie, D.C.; Lloyd-Smith, D.R. Plantar fasciitis: A retrospective analysis of 267 cases. Phys. Ther. Sport 2002, 3, 57–65. [Google Scholar] [CrossRef]
- Lopes, A.D.; Junior, L.C.H.; Yeung, S.S.; Costa, L.O.P. What are the Main running-related musculoskeletal injuries? A systematic review. Sports Med. 2012, 42, 891–905. [Google Scholar] [CrossRef] [PubMed]
- Kibler, W.B.; Goldberg, C.; Chandler, T.J. Functional biomechanical deficits in running athletes with plantar fasciitis. Am. J. Sports Med. 1991, 19, 66–71. [Google Scholar] [CrossRef]
- Wearing, S.C.; Smeathers, J.E.; Urry, S.R.; Hennig, E.M.; Hills, A.P. The pathomechanics of plantar fasciitis. Sports Med. 2006, 36, 585–611. [Google Scholar] [CrossRef]
- Rome, K.; Howe, T.; Haslock, I. Risk factors associated with the development of plantar heel pain in athletes. Foot 2001, 11, 119–125. [Google Scholar] [CrossRef]
- Saragiotto, B.T.; Yamato, T.P.; Lopes, A.D. What do recreational runners think about risk factors for running injuries? A descriptive study of their beliefs and opinions. J. Orthop. Sports Phys. Ther. 2014, 44, 733–738. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pohl, M.B.; Hamill, J.; Davis, I.S. Biomechanical and anatomic factors associated with a history of plantar fasciitis in female runners. Clin. J. Sport Med. 2009, 19, 372–376. [Google Scholar] [CrossRef]
- Ribeiro, A.P.; Trombini-Souza, F.; Tessutti, V.; Lima, F.R.; Sacco, I.C.N.; João, S.M.A. Rearfoot alignment and medial longitudinal arch configurations of runners with symptoms and histories of plantar fasciitis. Clinics 2011, 66, 1027–1033. [Google Scholar] [CrossRef] [Green Version]
- Di Caprio, F.; Buda, R.; Mosca, M.; Calabró, A.; Giannini, S. Foot and lower limb diseases in runners: Assessment of risk factors. J. Sports Sci. Med. 2010, 9, 587–596. [Google Scholar] [PubMed]
- Ribeiro, A.P.; Trombini-Souza, F.; Tessutti, V.D.; Lima, F.R.; João, S.M.A.; Sacco, I.C.N. The effects of plantar fasciitis and pain on plantar pressure distribution of recreational runners. Clin. Biomech. 2011, 26, 194–199. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.Y.; Hertel, J.; Lee, S.C. Rearfoot eversion has indirect effects on plantar fascia tension by changing the amount of arch collapse. Foot 2010, 20, 64–70. [Google Scholar] [CrossRef] [PubMed]
- Williams, D.S., III; Davis, I.M.; Scholz, J.P.; Hamill, J.; Buchanan, T.S. High-arched runners exhibit increased leg stiffness compared to low-arched runners. Gait Posture 2004, 19, 263–269. [Google Scholar] [CrossRef]
- Sneyers, C.J.; Lysens, R.; Feys, H.; Andries, R. Influence of malalignment of feet on the plantar pressure pattern in running. Foot Ankle Int. 1995, 16, 624–632. [Google Scholar] [CrossRef]
- Queen, R.M.; Mall, N.A.; Nunley, J.A.; Chuckpaiwong, B. Differences in plantar loading between flat and normal feet during different athletic tasks. Gait Posture 2009, 29, 582–586. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.Y.; Hertel, J. Effect of static foot alignment on plantar-pressure measures during running. J. Sport Rehabil. 2012, 21, 137–143. [Google Scholar] [CrossRef]
- Rodrigues, P.; Chang, R.; TenBroek, T.; van Emmerik, R.; Hamill, J. Evaluating the coupling between foot pronation and tibial internal rotation continuously using vector coding. J. Appl. Biomech. 2015, 31, 88–94. [Google Scholar] [CrossRef]
- Kwong, P.K.; Kay, D.; Voner, R.T.; White, M.W. Plantar fasciitis. Mechanics and pathomechanics of treatment. Clin. Sports Med. 1988, 7, 119–126. [Google Scholar] [CrossRef]
- Menz, H.B.; Dufour, A.B.; Riskowski, J.L.; Hillstrom, H.J.; Hannan, M.T. Association of planus foot posture and pronated foot function are associated with foot pain: The Framingham foot study. Arthritis Care Res. 2013, 65, 1991–1999. [Google Scholar] [CrossRef] [Green Version]
- Schepsis, A.A.; Leach, R.E.; Gorzyca, J. Plantar fasciitis. Etiology, treatment, surgical results, and review of the literature. Clin. Orthop. Relat. Res. 1991, 266, 185–196. [Google Scholar]
- League, A.C. Current concepts review: Plantar fasciitis. Foot Ankle Int. 2008, 29, 358–366. [Google Scholar] [CrossRef] [PubMed]
- Bedi, H.S.; Love, B.R. Differences in impulse distribution in patients with plantar fasciitis. Foot Ankle Int. 1998, 19, 153–156. [Google Scholar] [CrossRef]
- Wearing, S.C.; Smeathers, J.E.; Urry, S.R. The effect of plantar fasciitis on vertical foot-ground reaction force. Clin. Orthop. Relat. Res. 2003, 409, 175–185. [Google Scholar] [CrossRef] [PubMed]
- Wearing, S.C.; Smeathers, J.E.; Sullivan, P.M.; Yates, B.; Urry, S.R.; Dubois, P. Plantar fasciitis: Are pain and fascial thickness associated with arch shape and loading? Phys. Ther. 2007, 87, 1002–1008. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, A.P.; Sacco, I.C.; Dinato, R.C.; João, S.M.A. Relationships between static foot alignment and dynamic plantar loads in runners with acute and chronic stages of plantar fasciitis: A cross-sectional study. Braz. J. Phys. Ther. 2016, 20, 87–95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wearing, S.C.; Hills, A.P.; Byrne, N.M.; Hennig, E.M.; McDonald, M. The arch index: A measure of flat or fat feet? Foot Ankle Int. 2004, 25, 575–581. [Google Scholar] [CrossRef] [PubMed]
- Faria, A.; Gabriel, R.; Abrantes, J.; Brás, R.; Moreira, H. The relationship of body mass index, age and triceps-surae musculotendinous stiffness with the foot arch structure of postmenopausal women. Clin. Biomech. 2010, 25, 588–593. [Google Scholar] [CrossRef]
- Jankowicz-Szymanska, A.; Mikolajczyk, E. Genu Valgum and Flat Feet in Children with Healthy and Excessive Body Weight. Pediatric Phys. Ther. 2016, 28, 200–206. [Google Scholar] [CrossRef] [PubMed]
- Yan, S.; Li, R.; Shi, B.; Wang, R.; Yang, L. Mixed factors affecting plantar pressures and center of pressure in obese children: Obesity and flatfoot. Gait Posture 2020, 80, 7–13. [Google Scholar] [CrossRef]
- Park, S.Y.; Park, D.J. Comparison of Foot Structure, Function, Plantar Pressure and Balance Ability According to the Body Mass Index of Young Adults. Osong. Public Health Res. Perspect. 2019, 10, 102–107. [Google Scholar] [CrossRef]
- Lim, J.U.; Lee, J.H.; Kim, J.S.; Hwang, Y.I.; Kim, T.H.; Lim, S.Y.; Yoo, K.H.; Jung, K.S.; Kim, Y.K.; Rhee, C.K. Comparison of World Health Organization and Asia-Pacific body mass index classifications in COPD patients. Int. J. Chronic Obstr. Pulm. Dis. 2017, 21, 2465–2475. [Google Scholar] [CrossRef] [Green Version]
- Chow, T.H.; Chen, Y.S.; Wang, J.C. Characteristics of Plantar Pressures and Related Pain Profiles in Elite Sprinters and Recreational Runners. J. Am. Podiatr. Med. Assoc. 2018, 108, 33–44. [Google Scholar] [CrossRef] [PubMed]
- Chow, T.H.; Chen, Y.S.; Tsai, W.C.; Lin, M.H. Plantar Pressure Profiles and Possible Foot Syndromes of Taiwanese College Elite Basketball Players. J. Am. Podiatr. Med. Assoc. 2021, 111, 5. [Google Scholar] [CrossRef] [PubMed]
- Cavanagh, P.R.; Rodgers, M.M. The arch index: A useful measure from footprints. J. Biomech. 1987, 20, 547–551. [Google Scholar] [CrossRef]
- Cornwall, M.W.; McPoil, T.G. Influence of rearfoot postural alignment on rearfoot motion during walking. Foot 2004, 14, 133–138. [Google Scholar] [CrossRef]
- Jensen, M.P.; Karoly, P.; Braver, S. The measurement of clinical pain intensity: A comparison of six methods. Pain 1986, 27, 117–126. [Google Scholar] [CrossRef]
- Mickle, K.J.; Steele, J.R.; Munro, B.J. The feet of overweight and obese young children: Are they flat or fat? Obesity 2006, 14, 1949–1953. [Google Scholar] [CrossRef]
- Chang, R.; Rodrigues, P.A.; Van Emmerik, R.E.A.; Hamill, J. Multi-segment foot kinematics and ground reaction forces during gait of individuals with plantar fasciitis. J. Biomech. 2014, 47, 2571–2577. [Google Scholar] [CrossRef]
- Lee, J.H.; Jung, H.W.; Jang, W.Y. A prospective study of the muscle strength and reaction time of the quadriceps, hamstring, and gastrocnemius muscles in patients with plantar fasciitis. BioMed Cent. Musculoskelet. Disord. 2020, 21, 722. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, J.; Burns, J.; Adams, R.; Pappas, E.; Crosbie, J. Plantar heel pain and foot loading during normal walking. Gait Posture 2015, 41, 688–693. [Google Scholar] [CrossRef]
- Pavan, P.G.; Stecco, C.; Darwish, S.; Natali, A.N.; De Caro, R. Investigation of the mechanical properties of the plantar aponeurosis. Surg. Radiol. Anat. 2011, 33, 905–911. [Google Scholar] [CrossRef] [PubMed]
- Engkananuwat, P.; Kanlayanaphotporn, R.; Purepong, N. Effectiveness of the Simultaneous Stretching of the Achilles Tendon and Plantar Fascia in Individuals with Plantar Fasciitis. Foot Ankle Int. 2018, 39, 75–82. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.; Zwirner, J.; Templer, F.; Kieser, D.; Klima, S.; Hammer, N. On the morphological relations of the Achilles tendon and plantar fascia via the calcaneus: A cadaveric study. Sci. Rep. 2021, 11, 5986. [Google Scholar] [CrossRef] [PubMed]
- Stecco, C.; Corradin, M.; Macchi, V.; Morra, A.; Porzionato, A.; Biz, C.; De Caro, R. Plantar fascia anatomy and its relationship with Achilles tendon and paratenon. J. Anat. 2013, 223, 665–676. [Google Scholar] [CrossRef] [PubMed]
- Snow, S.W.; Bohne, W.H.; DiCarlo, E.; Chang, V.K. Anatomy of the Achilles tendon and plantar fascia in relation to the calcaneus in various age groups. Foot Ankle Int. 1995, 16, 418–421. [Google Scholar] [CrossRef] [PubMed]
- Carlson, R.E.; Fleming, L.L.; Hutton, W.C. The biomechanical relationship between the tendoachilles, plantar fascia and metatarsophalangeal joint dorsiflexion angle. Foot Ankle Int. 2000, 21, 18–25. [Google Scholar] [CrossRef] [PubMed]
- Cheng, H.Y.; Lin, C.L.; Wang, H.W.; Chou, S.W. Finite element analysis of plantar fascia under stretch-the relative contribution of windlass mechanism and Achilles tendon force. J. Biomech. 2008, 41, 1937–1944. [Google Scholar] [CrossRef] [PubMed]
- Cheung, J.T.; Zhang, M.; An, K.N. Effect of Achilles tendon loading on plantar fascia tension in the standing foot. Clin. Biomech. 2006, 21, 194–203. [Google Scholar] [CrossRef]
- Giacomozzi, C.; D’Ambrogi, E.; Uccioli, L.; Macellari, V. Does the thickening of Achilles tendon and plantar fascia contribute to the alteration of diabetic foot loading? Clin. Biomech. 2005, 20, 532–539. [Google Scholar] [CrossRef]
- Tahririan, M.A.; Motififard, M.; Tahmasebi, M.N.; Siavashi, B. Plantar fasciitis. J. Res. Med. Sci. 2021, 17, 799–804. [Google Scholar]
- Zhou, J.P.; Yu, J.F.; Feng, Y.N.; Liu, C.L.; Su, P.; Shen, S.H.; Zhang, Z.J. Modulation in the elastic properties of gastrocnemius muscle heads in individuals with plantar fasciitis and its relationship with pain. Sci. Rep. 2020, 10, 2770. [Google Scholar] [CrossRef]
- Gutteck, N.; Schilde, S.; Delank, K.S. Pain on the Plantar Surface of the Foot. Dtsch. Ärzteblatt Int. 2019, 116, 83–88. [Google Scholar] [CrossRef]
- Jha, R.K.; Uprety, S.; Shah, L.L. Functional outcome in patients with chronic plantar fasciitis treated with plantar fascia stretching vs. tendoachilles stretching exercises. J. Inst. Med. Nepal 2013, 35, 32–38. [Google Scholar] [CrossRef]
- Grieve, R.; Palmer, S. Physiotherapy for plantar fasciitis: A UK-wide survey of current practice. Physiotherapy 2017, 103, 193–200. [Google Scholar] [CrossRef] [PubMed]
- Malfait, B.; Dingenen, B.; Smeets, A.; Staes, F.; Pataky, T.; Robinson, M.A.; Vanrenterghem, J.; Verschueren, S. Knee and hip joint kinematics predict quadriceps and hamstrings neuromuscular activation patterns in drop jump landings. PLoS ONE 2016, 11, e0153737. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomas, A.C.; McLean, S.G.; Palmieri-Smith, R.M. Quadriceps and hamstrings fatigue alters hip and knee mechanics. J. Appl. Biomech. 2010, 26, 159–170. [Google Scholar] [CrossRef] [PubMed]
- Ward, S.H.; Blackburn, J.T.; Padua, D.A.; Stanley, L.E.; Harkey, M.S.; Luc-Harkey, B.A.; Pietrosimone, B. Quadriceps neuromuscular function and jump-landing sagittal-plane knee biomechanics after anterior cruciate ligament reconstruction. J. Athl. Train. 2018, 53, 135–143. [Google Scholar] [CrossRef] [Green Version]
- Labovitz, J.M.; Yu, J.; Kim, C. The role of hamstring tightness in plantar fasciitis. Foot Ankle Spec. 2011, 4, 141–144. [Google Scholar] [CrossRef]
- Harty, J.; Soffe, K.; O’Toole, G.; Stephens, M.M. The role of hamstring tightness in plantar fasciitis. Foot Ankle Int. 2005, 26, 1089–1092. [Google Scholar] [CrossRef] [PubMed]
- Shashua, A.; Flechter, S.; Avidan, L.; Ofir, D.; Melayev, A.; Kalichman, L. The effect of additional ankle and midfoot mobilizations on plantar fasciitis: A randomized controlled trial. J. Orthop. Sports Phys. Ther. 2015, 45, 265–272. [Google Scholar] [CrossRef]
- Thomas, J.L.; Christensen, J.C.; Kravitz, S.R.; Mendicino, R.W.; Schuberth, J.M.; Vanore, J.V.; Weil, L.S., Sr.; Zlotoff, H.J.; Bouché, R.; Baker, J. The diagnosis and treatment of heel pain: A clinical practice guideline–revision 2010. J. Foot Ankle Surg. 2010, 49, S1–S19. [Google Scholar] [CrossRef] [PubMed]
- Irving, D.B.; Cook, J.L.; Young, M.A.; Menz, H.B. Obesity and pronated foot type may increase the risk of chronic plantar heel pain: A matched case-control study. BioMed Cent. Musculoskelet. Disord. 2007, 17, 8–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bolgla, L.A.; Malone, T.R. Plantar fasciitis and the windlass mechanism: A biomechanical link to clinical practice. J. Athl. Train. 2004, 39, 77–82. [Google Scholar]
- Shultz, S.J.; Nguyen, A.D.; Leonard, M.D.; Schmitz, R.J. Thigh strength and activation as predictors of knee biomechanics during a drop jump task. Med. Sci. Sports Exerc. 2009, 41, 857–866. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lloyd, D.G.; Buchanan, T.S. Strategies of muscular support of varus and valgus isometric loads at the human knee. J. Biomech. 2001, 34, 1257–1267. [Google Scholar] [CrossRef]
- Norton, A.A.; Callaghan, J.J.; Amendola, A.; Phisitkul, P.; Wongsak, S.; Liu, S.S.; Fruehling-Wall, C. Correlation of knee and hindfoot deformities in advanced knee OA: Compensatory hindfoot alignment and where it occurs. Clin. Orthop. Relat. Res. 2015, 473, 166–174. [Google Scholar] [CrossRef] [Green Version]
- Ohi, H.; Iijima, H.; Aoyama, T.; Kaneda, E.; Ohi, K.; Abe, K. Association of frontal plane knee alignment with foot posture in patients with medial knee osteoarthritis. BioMed Cent. Musculoskelet. Disord. 2017, 18, 246. [Google Scholar] [CrossRef] [PubMed]
- Wyndow, N.; De Jong, A.; Rial, K.; Tucker, K.; Collins, N.; Vicenzino, B.; Russell, T.; Crossley, K. The relationship of foot and ankle mobility to the frontal plane projection angle in asymptomatic adults. J. Foot Ankle Res. 2016, 9, 3. [Google Scholar] [CrossRef] [Green Version]
- Becerro-de-Bengoa-Vallejo, R.; Losa-Iglesias, M.E.; Rodriguez-Sanz, D. Static and dynamic plantar pressures in children with and without sever disease: A case-control study. Phys. Ther. 2014, 94, 818–826. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farhan, H.; Moreno-Duarte, I.; Latronico, N.; Zafonte, R.; Eikermann, M. Acquired muscle weakness in the surgical intensive care unit: Nosology, epidemiology, diagnosis, and prevention. Anesthesiology 2016, 124, 207–234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Backstrom, K.; Moore, A. Plantar fasciitis. Phys. Ther. Case Rep. 2000, 3, 154–162. [Google Scholar]
- Kamonseki, D.H.; Gonçalves, G.A.; Yi, L.C.; Júnior, I.L. Effect of stretching with and without muscle strengthening exercises for the foot and hip in patients with plantar fasciitis: A randomized controlled single-blind clinical trial. Man. Ther. 2016, 23, 76–82. [Google Scholar] [CrossRef] [PubMed]
- Fredericson, M.; Cookingham, C.L.; Chaudhari, A.M.; Dowdell, B.C.; Oestreicher, N.; Sahrmann, S.A. Hip abductor weakness in distance runners with iliotibial band syndrome. Clin. J. Sport Med. 2000, 10, 169–175. [Google Scholar] [CrossRef] [PubMed]
- Sahrmann, S. Diagnosis and Treatment of Movement Impairment Syndromes-E-Book; Elsevier Inc.: St. Louis, MO, USA, 2013. [Google Scholar]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Control Group 1 | PF Group 2 | |||||
|---|---|---|---|---|---|---|
| Total | Male | Female | Total | Male | Female | |
| Number | 209 | 105 | 104 | 202 | 100 | 102 |
| Age (years) | 20.1 ± 0.9 | 19.9 ± 0.9 | 20.2 ± 0.8 | 21.2 ± 0.8 | 22.1 ± 0.9 | 20.2 ± 0.7 |
| Height (cm) | 165.7 ± 5.9 | 168.4 ± 5.2 | 162.9 ± 5.2 | 168.6 ± 7.5 | 170.5 ± 5.8 | 166.6 ± 4.9 |
| Mass (kg) | 61.2 ± 4.7 | 63.7 ± 4.5 | 58.6 ± 3.5 | 64.5 ± 4.8 | 65.4 ± 4.1 | 63.5 ± 3.1 |
| BMI | 22.3 ± 1.2 | 22.4 ± 1.0 | 22.1 ± 1.3 | 22.7 ± 1.5 | 22.5 ± 1.6 | 22.8 ± 1.7 |
| Gender | Left Foot | Right Foot | ||||
|---|---|---|---|---|---|---|
| Control Group | PF Group | p Value 1 | Control Group | PF Group | p Value 1 | |
| Total | 0.22 ± 0.08 | 0.24 ± 0.06 | 0.593 | 0.23 ± 0.08 | 0.25 ± 0.06 | 0.565 |
| Male | 0.23 ± 0.08 | 0.26 ± 0.07 | 0.042 | 0.24 ± 0.08 | 0.27 ± 0.07 | 0.037 |
| Female | 0.21 ± 0.08 | 0.22 ± 0.09 | 0.587 | 0.22 ± 0.08 | 0.23 ± 0.08 | 0.687 |
| Gender and Region | Static Standing | Midstance Phase of Walking | ||
|---|---|---|---|---|
| Left Foot | Right Foot | Left Foot | Right Foot | |
| Total (n = 202) | ||||
| Lateral Metatarsal bone (LM) | 21.27 ± 5.29 | 22.90 ± 8.06 | 29.62 ± 4.01 2 | 27.76 ± 5.84 2 |
| Lateral Longitudinal Arch (LLA) | 18.58 ± 4.19 | 17.50 ± 4.51 | 21.13 ± 3.12 2 | 19.50 ± 3.93 2 |
| Lateral Heel (LH) | 13.51 ± 5.25 | 12.06 ± 7.92 | 16.77 ± 2.01 2 | 17.95 ± 5.21 2 |
| Medial Metatarsal bone (MM) | 25.33 ± 4.97 | 26.08 ± 5.30 | 24.19 ± 5.04 1 | 25.99 ± 6.01 |
| Medial Longitudinal Arch (MLA) | 1.12 ± 0.36 | 1.36 ± 0.30 | 0.81 ± 0.51 2 | 0.98 ± 0.57 2 |
| Medial Heel (MH) | 20.20 ± 5.78 | 20.11 ± 4.76 | 7.48 ± 3.82 2 | 7.82 ± 4.88 2 |
| Male (n = 100) | ||||
| Lateral Metatarsal bone (LM) | 18.79 ± 5.61 | 16.03 ± 3.87 | 30.42 ± 3.18 2 | 26.74 ± 4.96 2 |
| Lateral Longitudinal Arch (LLA) | 18.95 ± 4.58 | 16.98 ± 4.67 | 20.71 ± 2.97 2 | 17.88 ± 3.51 |
| Lateral Heel (LH) | 17.32 ± 4.56 | 18.91 ± 5.67 | 16.39 ± 2.31 | 16.79 ± 4.48 2 |
| Medial Metatarsal bone (MM) | 26.21 ± 4.67 | 27.49 ± 5.32 | 25.00 ± 4.55 | 28.47 ± 5.47 |
| Medial Longitudinal Arch (MLA) | 0.87 ± 0.02 | 1.37 ± 0.31 | 0.85 ± 0.38 | 1.02 ± 0.49 2 |
| Medial Heel (MH) | 17.88 ± 6.52 | 19.24 ± 5.63 | 6.63 ± 3.75 2 | 9.09 ± 6.14 2 |
| Female (n = 102) | ||||
| Lateral Metatarsal bone (LM) | 23.71 ± 3.57 | 29.64 ± 4.68 | 28.85 ± 4.57 2 | 28.75 ± 6.47 |
| Lateral Longitudinal Arch (LLA) | 18.21 ± 3.74 | 18.00 ± 4.32 | 21.54 ± 3.22 2 | 21.09 ± 3.67 2 |
| Lateral Heel (LH) | 9.78 ± 2.44 | 5.35 ± 1.12 | 17.13 ± 1.59 2 | 19.08 ± 5.63 2 |
| Medial Metatarsal bone (MM) | 24.46 ± 5.13 | 24.69 ± 4.91 | 23.40 ± 5.38 | 23.57 ± 5.53 |
| Medial Longitudinal Arch (MLA) | 1.37 ± 0.37 | 1.35 ± 0.29 | 0.77 ± 0.61 2 | 0.94 ± 0.65 2 |
| Medial Heel (MH) | 22.47 ± 3.78 | 20.97 ± 3.54 | 8.31 ± 3.73 2 | 6.57 ± 2.70 2 |
| Gender | Left Foot | Right Foot | ||||
|---|---|---|---|---|---|---|
| Control Group | PF Group | p Value 1 | Control Group | PF Group | p Value 1 | |
| Total | 4.01 ± 2.52 | 5.87 ± 3.03 | 0.037 | 5.04 ± 3.83 | 11.85 ± 5.71 | 0.000 |
| Male | 3.64 ± 2.51 | 5.51 ± 3.76 | 0.000 | 4.72 ± 3.38 | 11.66 ± 6.87 | 0.000 |
| Female | 4.40 ± 2.47 | 6.23 ± 2.03 | 0.216 | 5.39 ± 4.25 | 12.02 ± 4.31 | 0.225 |
| Bone Pain | Soft-Tissue Pain | ||
|---|---|---|---|
| Pain Area | College Athletes with PF (No. [%]) | Pain Area | College Athletes with PF (No. [%]) |
| Foot (Calcaneus) | 167 (82.7) | Plantar fascia (medial band) | 156 (77.2) |
| Foot (Plantar metatarsal bone 1st & 2nd) | 115 (56.9) | Plantar fascia (medial band) | 121 (59.9) |
| Foot (Metatarsophalangeal joint 1st & 2nd) | 92 (45.5) | Plantar fascia (medial band) | 103 (51.0) |
| Lateral ankle joint | 73 (36.1) | Achilles tendon | 88 (43.6) |
| Medial knee joint | 61 (30.2) | Gastrocnemius | 81 (40.1) |
| Femur | 56 (27.7) | Hamstring muscles | 76 (37.6) |
| Patella | 55 (27.2) | Quadriceps femoris | 69 (34.2) |
| Lateral knee joint | 47 (23.3) | Plantar plate (Abductor hallucis) | 41 (20.3) |
| Tibia | 38 (18.8) | Plantar plate (Abductor digiti minimi) | 35 (17.3) |
| Hip joint | 27 (13.4) | Lower back | 30 (14.9) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chow, T.-H.; Chen, Y.-S.; Hsu, C.-C. Relationships between Plantar Pressure Distribution and Rearfoot Alignment in the Taiwanese College Athletes with Plantar Fasciopathy during Static Standing and Walking. Int. J. Environ. Res. Public Health 2021, 18, 12942. https://doi.org/10.3390/ijerph182412942
Chow T-H, Chen Y-S, Hsu C-C. Relationships between Plantar Pressure Distribution and Rearfoot Alignment in the Taiwanese College Athletes with Plantar Fasciopathy during Static Standing and Walking. International Journal of Environmental Research and Public Health. 2021; 18(24):12942. https://doi.org/10.3390/ijerph182412942
Chicago/Turabian StyleChow, Tong-Hsien, Yih-Shyuan Chen, and Chin-Chia Hsu. 2021. "Relationships between Plantar Pressure Distribution and Rearfoot Alignment in the Taiwanese College Athletes with Plantar Fasciopathy during Static Standing and Walking" International Journal of Environmental Research and Public Health 18, no. 24: 12942. https://doi.org/10.3390/ijerph182412942
APA StyleChow, T. -H., Chen, Y. -S., & Hsu, C. -C. (2021). Relationships between Plantar Pressure Distribution and Rearfoot Alignment in the Taiwanese College Athletes with Plantar Fasciopathy during Static Standing and Walking. International Journal of Environmental Research and Public Health, 18(24), 12942. https://doi.org/10.3390/ijerph182412942