
Risk Factors for Venous Thromboembolism in Severe COVID-19: A Study-Level Meta-Analysis of 21 Studies

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
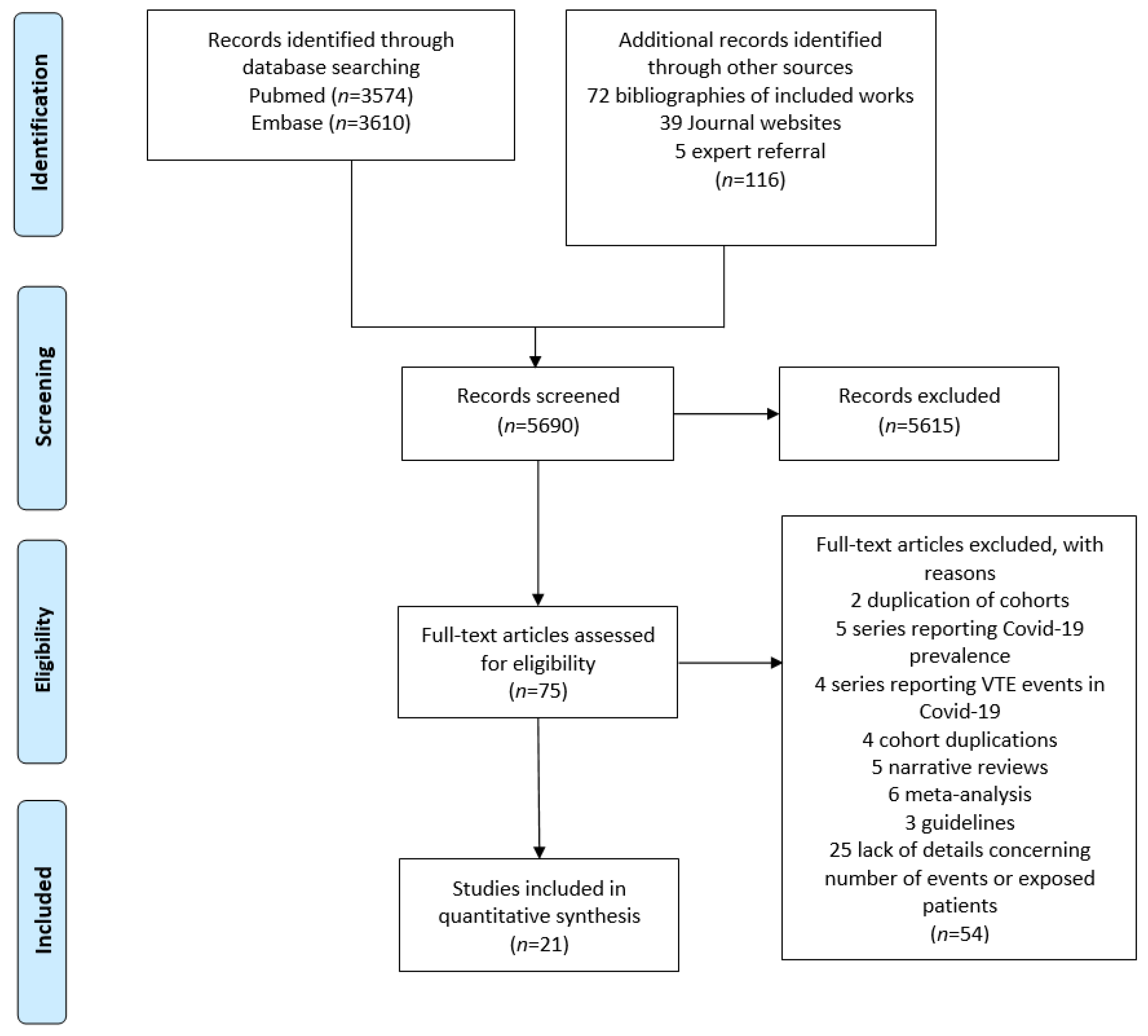
2.1. Search Strategy
2.2. Study Selection
- -
- Demographic characteristics: age, male sex;
- -
- Patient history factors: body-mass-index (BMI) and obesity (BMI ≥ 30 kg·m−2), alcohol and tobacco use, history of cancer, history of previous VTE, several medical conditions (including cardiac disease, cerebrovascular disease, chronic kidney disease, chronic liver disease, chronic lung disease, diabetes mellitus, immunodeficiency, human immunodeficiency virus (HIV) infection, hypertension and use of angiotensin convertor enzyme (ACE) inhibitors);
- -
- Therapeutic management and disease severity markers: Acute Physiology and Chronic Health Evaluation II (APACHE II), Simplified Acute Physiology Score II (SAPS-II), Sepsis-related Organ Failure Assessment score (SOFA), Therapeutic Intervention Scoring Systemc-10 (TISS-10), arterial oxygen partial pressure/fractional inspired oxygen (PaO2/FiO2), requirement and duration of use of neuromuscular blockers and inotropic drugs, length of hospital stay and disease duration, acute kidney injury and requirement for renal replacement therapy, myocarditis, requirement for extracorporeal membrane oxygenation (ECMO), use of anticoagulant treatment (including prophylactic, intermediate and therapeutic dosage);
- -
- Inflammation biomarkers: C-reactive protein (CRP), ferritin, fibrinogen, interleukin-6 (IL-6) and procalcitonin.
- -
- Coagulation tests: activated partial thromboplastin time (APTT), D-dimers, Prothrombin Time (PT), score for disseminated intravascular coagulation (DIC) from the International Society on Thrombosis and Haemostasis (ISTH);
- -
- Haematological parameters: complete blood count (including: leukocytes, lymphocytes, neutrophils, haemoglobin, and platelets);
- -
- Biological markers of organ dysfunction: alanine aminotransferase (ALT), aspartate aminotransferase (AST), creatine kinase serum level, creatinine level, lactate dehydrogenase (LDH), N-terminal pro-brain natriuretic peptide (NT-proBNP), troponin T, and troponin I level.
2.3. Quality Assessment
2.4. Outcomes
2.5. Statistical Analysis
2.6. Role of the Funding Source
2.7. Data Availability
3. Results
3.1. Literature Search and Study Characteristics
3.2. Risk of Bias
3.3. Identification of Risk Factors for VTE
3.3.1. Demographic and Past History Factors
3.3.2. Therapeutic Management and Disease Severity
3.3.3. Inflammation Biomarkers
3.3.4. Coagulation Tests
3.3.5. Haematological Parameters
3.3.6. Biological Markers of Organ Dysfunction
3.4. Sensitivity Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rothan, H.A.; Byrareddy, S.N. The epidemiology and pathogenesis of coronavirus disease (COVID-19) outbreak. J. Autoimmun. 2020, 109, 102433. [Google Scholar] [CrossRef]
- Iba, T.; Levy, J.H.; Levi, M.; Thachil, J. Coagulopathy in COVID-19. J. Thromb. Haemost. 2020, 18, 2103–2109. [Google Scholar] [CrossRef] [PubMed]
- Goshua, G.; Pine, A.B.; Meizlish, M.L.; Chang, C.-H.; Zhang, H.; Bahel, P.; Baluha, A.; Bar, N.; Bona, R.D.; Burns, A.J.; et al. Endotheliopathy in COVID-19-associated coagulopathy: Evidence from a single-centre, cross-sectional study. Lancet Haematol. 2020, 7, e575–e582. [Google Scholar] [CrossRef]
- Tan, B.K.; Mainbourg, S.; Friggeri, A.; Bertoletti, L.; Douplat, M.; Dargaud, Y.; Grange, C.; Lobbes, H.; Provencher, S.; Lega, J.C. Arterial and venous thromboembolism in COVID-19: A study-level meta-analysis. Thorax 2021, 76, 970–979. [Google Scholar] [CrossRef]
- Mai, V.; Tan, B.K.; Mainbourg, S.; Potus, F.; Cucherat, M.; Lega, J.C.; Provencher, S. Venous thromboembolism in COVID-19 compared to non-COVID-19 cohorts: A systematic review with meta-analysis. Vascul. Pharmacol. 2021, 139, 106882. [Google Scholar] [CrossRef] [PubMed]
- REMAP-CAP Investigators; ACTIV-4a Investigators; ATTACC Investigators; Goligher, E.C.; Bradbury, C.A.; McVerry, B.J.; Lawler, P.R.; Berger, J.S.; Gong, M.N.; Carrier, M.; et al. Therapeutic Anticoagulation with Heparin in Critically Ill Patients with Covid-19. N. Engl. J. Med. 2021, 385, 777–789. [Google Scholar] [CrossRef]
- Perepu, U.; Chambers, I.; Wahab, A.; Ten Eyck, P.; Wu, C.; Dayal, S.; Sutamtewagul, G.; Bailey, S.R.; Rosenstein, L.J.; Lentz, S.R. Standard prophylactic versus intermediate dose enoxaparin in adults with severe COVID-19: A multi-center, open-label, randomized controlled trial. J. Thromb. Haemost. 2021, 19, 2225–2234. [Google Scholar] [CrossRef] [PubMed]
- Cuker, A.; Tseng, E.K.; Nieuwlaat, R.; Angchaisuksiri, P.; Blair, C.; Dane, K.; Davila, J.; DeSancho, M.T.; Diuguid, D.; Griffin, D.O.; et al. American Society of Hematology 2021 guidelines on the use of anticoagulation for thromboprophylaxis in patients with COVID-19. Blood Adv. 2021, 5, 872–888. [Google Scholar] [CrossRef]
- Mai, V.; Mainbourg, S.; Tan, B.K.; Lega, J.-C.; Provencher, S. Significant Major Bleeding in Hospitalized Patients with COVID-19 Receiving Thromboprophylaxis. Thromb. Haemost. 2021, 121, 1670–1673. [Google Scholar] [CrossRef] [PubMed]
- Riley, R.D.; Moons, K.G.M.; Snell, K.I.E.; Ensor, J.; Hooft, L.; Altman, D.G.; Hayden, J.; Collins, G.S.; Debray, T.P.A. A guide to systematic review and meta-analysis of prognostic factor studies. BMJ 2019, 364, k4597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Foroutan, F.; Guyatt, G.; Zuk, V.; Vandvik, P.O.; Alba, A.C.; Mustafa, R.; Vernooij, R.; Arevalo-Rodriguez, I.; Munn, Z.; Roshanov, P.; et al. GRADE Guidelines 28: Use of GRADE for the assessment of evidence about prognostic factors: Rating certainty in identification of groups of patients with different absolute risks. J. Clin. Epidemiol. 2020, 121, 62–70. [Google Scholar] [CrossRef] [PubMed]
- PPage, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Int. J. Surg. 2021, 88, 105906. [Google Scholar] [CrossRef] [PubMed]
- Chinn, S. A simple method for converting an odds ratio to effect size for use in meta-analysis. Stat. Med. 2000, 19, 3127–3131. [Google Scholar] [CrossRef]
- Hozo, S.P.; Djulbegovic, B.; Hozo, I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med. Res. Methodol. 2005, 5, 13. [Google Scholar] [CrossRef] [Green Version]
- Al-Samkari, H.; Gupta, S.; Leaf, R.K.; Wang, W.; Rosovsky, R.P.; Brenner, S.K.; Hayek, S.S.; Berlin, H.; Kapoor, R.; Shaefi, S.; et al. Thrombosis, Bleeding, and the Observational Effect of Early Therapeutic Anticoagulation on Survival in Critically Ill Patients With COVID-19. Ann. Intern. Med. 2021, 174, 622–632. [Google Scholar] [CrossRef] [PubMed]
- Bellmunt-Montoya, S.; Riera, C.; Gil, D.; Rodríguez, M.; García-Reyes, M.; Martínez-Carnovale, L.; Marrero, C.; Gil, M.; Ruiz-Rodríguez, J.C.; Ferrer, R.; et al. COVID-19 Infection in Critically Ill Patients Carries a High Risk of Venous Thrombo-embolism. Eur. J. Vasc. Endovasc. Surg. 2021, 61, 628–634. [Google Scholar] [CrossRef]
- Contou, D.; Pajot, O.; Cally, R.; Logre, E.; Fraissé, M.; Mentec, H.; Plantefève, G. Pulmonary embolism or thrombosis in ARDS COVID-19 patients: A French monocenter retrospective study. PLoS ONE 2020, 15, e0238413. [Google Scholar] [CrossRef]
- Cui, S.; Chen, S.; Li, X.; Liu, S.; Wang, F. Prevalence of venous thromboembolism in patients with severe novel coronavirus pneumonia. J. Thromb. Haemost. 2020, 18, 1421–1424. [Google Scholar] [CrossRef] [PubMed]
- Desborough, M.J.R.; Doyle, A.J.; Griffiths, A.; Retter, A.; Breen, K.A.; Hunt, B.J. Image-proven thromboembolism in patients with severe COVID-19 in a tertiary critical care unit in the United Kingdom. Thromb. Res. 2020, 193, 1–4. [Google Scholar] [CrossRef]
- Dujardin, R.W.; Hilderink, B.N.; Haksteen, W.E.; Middeldorp, S.; Vlaar, A.P.; Thachil, J.; Müller, M.C.; Juffermans, N.P. Biomarkers for the prediction of venous thromboembolism in critically ill COVID-19 patients. Thromb. Res. 2020, 196, 308–312. [Google Scholar] [CrossRef]
- Fraissé, M.; Logre, E.; Pajot, O.; Mentec, H.; Plantefève, G.; Contou, D. Thrombotic and hemorrhagic events in critically ill COVID-19 patients: A French monocenter retrospective study. Crit. Care 2020, 24, 275. [Google Scholar] [CrossRef] [PubMed]
- Gibson, C.J.; Alqunaibit, D.; Smith, K.E.; Bronstein, M.; Eachempati, S.R.; Kelly, A.G.; Lee, C.; Minneman, J.A.; Narayan, M.; Shou, J.; et al. Probative Value of the D-Dimer Assay for Diagnosis of Deep Venous Thrombosis in the Coronavirus Disease 2019 Syndrome. Crit. Care Med. 2020, 48, e1322–e1326. [Google Scholar] [CrossRef]
- Grandmaison, G.; Andrey, A.; Périard, D.; Engelberger, R.P.; Carrel, G.; Doll, S.; Dexpert, J.B.; Krieger, C.; Ksouri, H.; Hayoz, D.; et al. Systematic Screening for Venous Thromboembolic Events in COVID-19 Pneumonia. TH Open 2020, 4, e113–e115. [Google Scholar] [CrossRef] [PubMed]
- Helms, J.; Severac, F.; Merdji, H.; Schenck, M.; Clere-Jehl, R.; Baldacini, M.; Ohana, M.; Grunebaum, L.; Castelain, V.; Anglés-Cano, E.; et al. Higher anticoagulation targets and risk of thrombotic events in severe COVID-19 patients: Bi-center cohort study. Ann. Intensive Care 2021, 11, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Hippensteel, J.A.; Burnham, E.L.; Jolley, S.E. Prevalence of Venous Thromboembolism in Critically Ill Patients with COVID-19. Br. J. Haematol. 2020, 190, e134–e137. [Google Scholar] [CrossRef] [PubMed]
- Maatman, T.K.; Jalali, F.; Feizpour, C.; Douglas, A. Routine Venous Thromboembolism Prophylaxis May Be Inadequate in the Hypercoagulable State of Severe Coronavirus Disease 2019. Crit. Care Med. 2020, 48, e783–e790. [Google Scholar] [CrossRef] [PubMed]
- Mirsadraee, S.; Gorog, D.A.; Mahon, C.F.; Rawal, B.; Semple, T.R.; Nicol, E.D.; Arachchillage, D.R.; Devaraj, A.; Price, S.; Desai, S.R.; et al. Prevalence of Thrombotic Complications in ICU-Treated Patients With Coronavirus Disease 2019 Detected With Systematic CT Scanning. Crit. Care Med. 2021, 49, 804–815. [Google Scholar] [CrossRef] [PubMed]
- Mueller-Peltzer, K.; Krauss, T.; Benndorf, M.; Lang, C.N.; Bamberg, F.; Bode, C.; Duerschmied, D.; Staudacher, D.L.; Zotzmann, V. Pulmonary artery thrombi are co-located with opacifications in SARS-CoV2 induced ARDS. Respir. Med. 2020, 172, 106135. [Google Scholar] [CrossRef]
- Nahum, J.; Morichau-Beauchant, T.; Daviaud, F.; Echegut, P.; Fichet, J.; Maillet, J.M.; Thierry, S. Venous Thrombosis Among Critically Ill Patients With Coronavirus Disease 2019 (COVID-19). JAMA Netw. Open 2020, 3, e2010478. [Google Scholar] [CrossRef]
- Shah, A.; Donovan, K.; McHugh, A.; Pandey, M.; Aaron, L.; Bradbury, C.A.; Stanworth, S.J.; Alikhan, R.; Kier, S.V.; Maher, K.; et al. Thrombotic and haemorrhagic complications in critically ill patients with COVID-19: A multicentre observational study. Crit. Care 2020, 24, 561. [Google Scholar] [CrossRef]
- Soumagne, T.; Lascarrou, J.B.; Hraiech, S.; Horlait, G.; Higny, J.; d’Hondt, A.; Grimaldi, D.; Gaudry, S.; Courcelle, R.; Carbutti, G.; et al. Factors Associated With Pulmonary Embolism Among Coronavirus Disease 2019 Acute Respiratory Distress Syndrome: A Multicenter Study among 375 Patients. Crit Care Explor 2020, 2, e0166. [Google Scholar] [CrossRef]
- Torres-Machorro, A.; Anguiano-Álvarez, V.M.; Grimaldo-Gómez, F.A.; Rodríguez-Zanella, H.; de la Rosa, E.C.; Mora-Canela, S.; Lerma, C.; García-Cruz, E.; Ramos-Enriquez, Á.; Ramirez-Marroquin, S.; et al. Asymptomatic deep vein thrombosis in critically ill COVID-19 patients despite therapeutic levels of anti-Xa activity. Thromb. Res. 2020, 196, 268–271. [Google Scholar] [CrossRef]
- Trigonis, R.A.; Holt, D.B.; Yuan, R.; Siddiqui, A.A.; Craft, M.K.; Khan, B.A.; Kapoor, R.; Rahman, O. Incidence of Venous Thromboembolism in Critically Ill Coronavirus Disease 2019 Patients Receiving Prophylactic Anticoagulation. Crit. Care Med. 2020, 48, e805–e808. [Google Scholar] [CrossRef] [PubMed]
- Voicu, S.; Bonnin, P.; Stépanian, A.; Chousterman, B.G.; Le Gall, A.; Malissin, I.; Deye, N.; Siguret, V.; Mebazaa, A.; Mégarbane, B. High Prevalence of Deep Vein Thrombosis in Mechanically Ventilated COVID-19 Patients. J. Am. Coll. Cardiol. 2020, 76, 480–482. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Feng, X.; Zhang, D.; Jiang, C.; Mei, H.; Wang, J.; Zhang, C.; Li, H.; Xia, X.; Kong, S.; et al. Deep Vein Thrombosis in Hospitalized Patients With COVID-19 in Wuhan, China. Circulation 2020, 142, 114–128. [Google Scholar] [CrossRef]
- Lim, W.; Meade, M.; Lauzier, F.; Zarychanski, R.; Mehta, S.; Lamontagne, F.; Dodek, P.; McIntyre, L.; Hall, R.; Heels-Ansdell, D.; et al. Failure of anticoagulant thromboprophylaxis: Risk factors in medical-surgical critically ill patientS. Crit. Care Med. 2015, 43, 401–410. [Google Scholar] [CrossRef]
- Khan, F.; Tritschler, T.; Kahn, S.R.; Rodger, M.A. Venous thromboembolism. Lancet 2021, 398, 64–77. [Google Scholar] [CrossRef]
- Lamontagne, F.; McIntyre, L.; Dodek, P.; Heels-Ansdell, D.; Meade, M.; Pemberton, J.; Skrobik, Y.; Seppelt, I.; Vlahakis, N.E.; Muscedere, J.; et al. Nonleg Venous Thrombosis in Critically Ill Adults: A Nested Prospective Cohort Study. JAMA Intern. Med. 2014, 174, 689–696. [Google Scholar] [CrossRef]
- Eck, R.J.; Hulshof, L.; Wiersema, R.; Thio, C.H.; Hiemstra, B.; van den Oever, N.C.; Gans, R.O.; van der Horst, I.C.; Meijer, K.; Keus, F. Incidence, prognostic factors, and outcomes of venous thromboembolism in critically ill patients: Data from two prospective cohort studies. Crit Care 2021, 25, 27. [Google Scholar] [CrossRef]
- Sadeghipour, P.; Talasaz, A.H.; Rashidi, F.; Sharif-Kashani, B.; Beigmohammadi, M.T.; Farrokhpour, M.; Sezavar, S.H.; Payandemehr, P.; Dabbagh, A.; Moghadam, K.G.; et al. Effect of Intermediate-Dose vs Standard-Dose Prophylactic Anticoagulation on Thrombotic Events, Extracorporeal Membrane Oxygenation Treatment, or Mortality Among Patients With COVID-19 Admitted to the Intensive Care Unit: The INSPIRATION Randomized Clinical Trial. JAMA 2021, 325, 1620–1630. [Google Scholar]
- ATTACC Investigators; ACTIV-4a Investigators; REMAP-CAP Investigators; Lawler, P.R.; Goligher, E.C.; Berger, J.S.; Neal, M.D.; McVerry, B.J.; Nicolau, J.C.; Gong, M.N.; et al. Therapeutic Anticoagulation with Heparin in Noncritically Ill Patients with Covid-19. N. Engl. J. Med. 2021, 385, 790–802. [Google Scholar] [CrossRef] [PubMed]
- Sholzberg, M.; Tang, G.H.; Rahhal, H.; AlHamzah, M.; Kreuziger, L.B.; Áinle, F.N.; Alomran, F.; Alayed, K.; Alsheef, M.; AlSumait, F.; et al. Effectiveness of therapeutic heparin versus prophylactic heparin on death, mechanical ventilation, or intensive care unit admission in moderately ill patients with covid-19 admitted to hospital: RAPID randomised clinical trial. BMJ 2021, 375, n2400. [Google Scholar] [CrossRef] [PubMed]
- Yu, B.; Gutierrez, V.P.; Carlos, A.; Hoge, G.; Pillai, A.; Kelly, J.D.; Menon, V. Empiric use of anticoagulation in hospitalized patients with COVID-19: A propensity score-matched study of risks and benefits. Biomark. Res. 2021, 9, 29. [Google Scholar] [CrossRef]
- Darzi, A.J.; Karam, S.G.; Charide, R.; Etxeandia-Ikobaltzeta, I.; Cushman, M.; Gould, M.K.; Mbuagbaw, L.; Spencer, F.A.; Spyropoulos, A.C.; Streiff, M.B.; et al. Prognostic factors for VTE and bleeding in hospitalized medical patients: A systematic review and meta-analysis. Blood 2020, 135, 1788–1810. [Google Scholar] [CrossRef] [PubMed]
- McGonagle, D.; O’Donnell, J.S.; Sharif, K.; Emery, P.; Bridgewood, C. Immune mechanisms of pulmonary intravascular coagulopathy in COVID-19 pneumonia. Lancet Rheumatol. 2020, 2, e437–e445. [Google Scholar] [CrossRef]
- Bonaventura, A.; Vecchié, A.; Dagna, L.; Martinod, K.; Dixon, D.L.; Van Tassell, B.W.; Dentali, F.; Montecucco, F.; Massberg, S.; Levi, M.; et al. Endothelial dysfunction and immunothrombosis as key pathogenic mechanisms in COVID-19. Nat. Rev. Immunol. 2021, 21, 319–329. [Google Scholar] [CrossRef] [PubMed]
- Al-Samkari, H.; Karp Leaf, R.S.; Dzik, W.H.; Carlson, J.C.; Fogerty, A.E.; Waheed, A.; Goodarzi, K.; Bendapudi, P.K.; Bornikova, L.; Gupta, S.; et al. COVID-19 and coagulation: Bleeding and thrombotic manifestations of SARS-CoV-2 infection. Blood 2020, 136, 489–500. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Study | Country | Nb | FU | Design | Diagnostic of COVID-19 | Male% | Mean Age (y) | Diagnosis of VTE | Type of VTE Event | VTE Rate | Data Collection |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Al-Samkari [15] | USA | 3239 | 27 | P, C, M | RT-PCR | 64.5% | 61 | NA | DVT, PE | 6% | ICU admission |
| Bellmunt-Montoya [16] | Spain | 227 | 7 | P, NC, M | RT-PCR | 77% | 62 | AS | DVT, PE | 26.5% | ICU admission |
| Contou [17] | France | 26 | NA | R, NC, m | RT-PCR | 79% | 61 | ST | PE | 62% | Day of CTPA |
| Cui [18] | China | 81 | 14 | R, NA, m | RT-PCR and CT-scan | 46% | 60 | AS | DVT, PE | 25% | NA |
| Desborough [19] | UK | 66 | 28 | R, C, m | Antigen test | 73% | 59 | ST | DVT, PE | 15% | ICU admission |
| Dujardin [20] | Netherlands | 127 | NA | R, C, m | RT-PCR | 77% | 62 | AS | DVT, PE | 41% | ICU admission |
| Fraissé [21] | France | 92 | NA | R, C, m | NA | 79% | 61 | ST | DVT, PE | 40% | ICU admission |
| Gibson [22] | USA | 72 | NA | P, NA, m | RT-PCR | 79% | 64 | AS | DVT | 17% | Hospital admission |
| Grandmaison [23] | Switzerland | 29 | NA | P, NC, m | RT-PCR | 62% | 66 | AS (DVT) and ST (PE) | DVT, PE | 59% | NA |
| Helms [24] | France | 179 | 80 | P, C, M | RT-PCR | 73% | 62 | ST | DVT, PE | 32% | NA |
| Hippensteel [25] | USA | 91 | 26 | R, NC, m | NA | 58% | 56 | ST | DVT, PE | 26% | Hospital admission |
| Maatman [26] | USA | 109 | NA | R, C, M | RT-PCR | 62% | 61 | ST | DVT, PE | 16% | NA |
| Mirsadraee [27] | UK | 72 | 32 | R, C, m | RT-PCR | 74% | 52 | ST | DVT, PE | 58% | NA |
| Mueller-Peltzer [28] | Germany | 16 | 23 | R, NC, m | RT-PCR | 73% | 60 | AS | PE | 45% | Mixed |
| Nahum [29] | France | 34 | NA | P, C, m | RT-PCR and CT-scan | 78% | 62 | AS | DVT | 79% | NA |
| Shah [30] | UK | 187 | 20 | R, C, M | RT-PCR and CT-scan | 68% | 57 | ST | DVT, PE | 35% | < 48 h ICU admission |
| Soumagne [31] | France, Belgium | 375 | 28 | NA, C, M | RT-PCR | 77% | 62 | ST | PE | 36% | NA |
| Torres-Machorro [32] | Mexico | 30 | <9 | P, C, m | NA | 77% | 62 | AS | DVT | 30% | NA |
| Trigonis [33] | USA | 45 | NA | R, NC, m | NA | NA | 61 | ST | DVT | 42% | VTE screening |
| Voicu [34] | France | 56 | 10 | P, C, m | NA | 75% | NA | AS | DVT | 46% | NA |
| Zhang [35] | China | 143 | 19 | R, C, m | RT-PCR | 51% | 63 | AS | DVT, PE | 46%% | NA |
| Study | Study Participation | Study Attrition | Prognostic Factor Measurement | Outcome Measurement | Study Confounding | Statistical Analysis and Reporting |
|---|---|---|---|---|---|---|
| Al-Samkari [15] | ||||||
| Bellmunt-Montoya [16] | ||||||
| Contou [17] | ||||||
| Cui [18] | ||||||
| Desborough [19] | ||||||
| Dujardin [20] | ||||||
| Fraissé [21] | ||||||
| Gibson [22] | ||||||
| Grandmaison [23] | ||||||
| Helms [24] | ||||||
| Hippensteel [25] | ||||||
| Maatman [26] | ||||||
| Mirsadraee [27] | ||||||
| Mueller-Peltzer [28] | ||||||
| Nahum [29] | ||||||
| Shah [30] | ||||||
| Soumagne [31] | ||||||
| Torres-Machorro [32] | ||||||
| Trigonis [33] | ||||||
| Voicu [34] | ||||||
| Zhang [35] |
| Variable | Certainty Assessment Domains | Overall Certainty | SMD 95%CI | OR 95%CI | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| N | Study Design | Risk of Bias | Indirectness | Inconsistency | Imprecision | Publication Bias | ||||
| Demographic factors | ||||||||||
| Age | 17 | Obs | S * | NS | S | S | Undetect | ꚛ○○○ | 0.11 (−0.09; 0.30) | 1.22 (0.85; 1.72) |
| BMI | 13 | Obs | S * | NS | NS | NS | Undetect | ꚛꚛꚛ○ | 0.02 (−0.08–0.12) | 1.04 (0.86–1.25) |
| Biological markers of organ dysfunction | ||||||||||
| ALAT | 4 | Obs | S * | NS | S | S | Undetect | ꚛ○○○ | 0.24 (−0.07; 0.56) | 1.55 (0.87; 2.75) |
| ASAT | 3 | Obs | S * | NS | S | S | Undetect | ꚛꚛ○○ | 0.25 (−0.09; 0.60) | 1.59 (0.85; 2.97) |
| Creatinine | 6 | Obs | S * | NS | S | NS | Undetect | ꚛꚛ○○ | −0.08 (−0.39; 0.24) | 0.87 (0.49; 1.54) |
| Creatine kinase | 1 | Obs | S * | NS | NS | S | Undetect | ꚛ○○○ | −0.25 (−0.73–0.23) | 0.64 (0.27–1.53) |
| LDH | 6 | Obs | S * | NS | S | S | Undetect | ꚛꚛ○○ | 0.44 (−0.03; 0.91) | 2.23 (0.95; 5.19) |
| LDH (peak) | 1 | Obs | S * | NS | NS | S | Undetect | ꚛꚛ○○ | 0.15 (−0.3–0.6) | 1.32 (0.58–2.95) |
| NT-proBNP | 2 | Obs | S * | NS | NS | S | Undetect | ꚛꚛ○○ | −0.06 (−0.66–0.54) | 0.90 (0.30–2.64) |
| Troponin I | 3 | Obs | S * | NS | S | S | Undetected | ꚛ○○○ | 0.94 (−0.10; 1.98) | 5.49 (0.83; 36.28) |
| Troponin T | 1 | Obs | S * | NS | NS | S | Detected | ꚛꚛ○○ | 1.19 (0.65; 1.73) | 8.64 (3.25; 22.97) |
| Scores | ||||||||||
| APACHEII | 1 | Obs | S * | NS | NS | S | Detected | ꚛ○○○ | 0.31 (0.02; 0.61) | 1.76 (1.04; 3.00) |
| DIC ISTH | 1 | Obs | S * | NS | NS | S | Detected | ꚛ○○○ | 0.44 (0.15; 0.73) | 2.23 (1.31; 3.79) |
| SAPSII | 3 | Obs | S * | NS | NS | S | Undetect | ꚛꚛ○○ | 0.13 (−0.22; 0.48) | 1.27 (0.68; 2.37) |
| SOFA | 3 | Obs | S * | NS | S | S | Undetect | ꚛ○○○ | 0.24 (−0.3–0.79) | 1.55 (0.58–4.17) |
| SOFA at VTE screening | 1 | Obs | S * | NS | NS | S | Detected | ꚛꚛ○○ | 0.72 (0.11–1.33) | 3.69 (1.22–11.2) |
| SOFA at intubation | 1 | Obs | S * | NS | NS | S | Undetect | ꚛꚛ○○ | 0.33 (−0.26–0.93) | 1.83 (0.62–5.4) |
| TISS 10 | 1 | Obs | S * | NS | NS | S | Undetect | ꚛꚛ○○ | −0.66 (−1.68; 0.36) | 0.30 (0.05–1.93) |
| Coagulation markers | ||||||||||
| aPTT ratio | 2 | Obs | S * | NS | S | S | Detected | ꚛ○○○ | 0.27 (−4.07; 4.60) | 1.63 (0.00; 2.76) |
| aPTT | 5 | Obs | S * | NS | NS | S | Undetect | ꚛꚛ○○ | 0.23 (−0.15–0.60) | 1.5 (0.76–2.99) |
| PT (absolute) | 6 | Obs | S * | NS | S | S | Undetect | ꚛ○○○ | 0.06 (−0.34; 0.45) | 1.11 (0.54; 2.27) |
| PT (%) | 2 | Obs | S * | NS | S | S | Undetect | ꚛ○○○ | −0.11 (−1.35; 1.13) | 0.82 (0.09; 7.69) |
| D-Dimer | 17 | Obs | S * | NS | S | NS | Undetect | ꚛꚛ○○ | 0.84 (0.51; 1.18) | 4.58 (2.52; 8.50) |
| D-Dimer (peak) | 3 | Obs | S * | NS | NS | NS | Undetec | ꚛꚛꚛ○ | 0.97 (0.64; 1.31) | 5.83 (3.18; 10.7) |
| D-Dimer at VTE screening | 2 | Obs | S * | NS | NS | S | Undetec | ꚛꚛ○○ | 0.90 (0.37; 1.44) | 5.14 (1.95; 13.6) |
| Inflammation makers | ||||||||||
| CRP | 12 | Obs | S * | NS | S | NS | Undetect | ꚛꚛ○○ | 0.32 (0.14–0.51) | 1.83 (1.32–2.53) |
| CRP (peak) | 1 | Obs | S * | NS | NS | S | Undetect | ꚛꚛ○○ | −0.01 (−0.46; 0.43) | 0.98 (0.44; 2.17) |
| Ferritin | 7 | Obs | S * | NS | S | S | Detected | ꚛ○○○ | 0.35 (−0.30; 1.00) | 1.89 (0.58; 6.13) |
| Ferritin (peak) | 1 | Obs | S * | NS | NS | S | Undetect | ꚛꚛ○○ | 0.00 (−0.45–0.45) | 0.99 (0.44–2.25) |
| Fg | 13 | Obs | S * | NS | NS | S | Undetected | ꚛꚛ○○ | −0.02 (−0.16; 0.19) | 0.96 (0.75–1.41) |
| Fg (peak) | 1 | Obs | S * | NS | NS | S | Undetected | ꚛꚛ○○ | −0.23 (−0.73–0.27) | 0.66 (0.26–1.63) |
| IL−6 | 3 | Obs | S * | NS | NS | S | Undetect | ꚛꚛ○○ | −0.28 (−0.55; −0.02) | 0.58 (0.37; 0.97) |
| PCT | 4 | Obs | S * | NS | S | S | Undetect | ꚛ○○○ | 0.53 (0.03; 1.02) | 2.61 (1.05; 6.36) |
| PCT (peak) | 1 | Obs | S * | NS | NS | S | Undetect | ꚛꚛ○○ | 0.41 (−0.0; 0.87) | 2.08 (0.89; 4.87) |
| Haematological parameters | ||||||||||
| Haemoglobin | 8 | Obs | S * | NS | NS | S | Undetect | ꚛꚛ○○ | 0.02 (−0.10; 0.13) | 1.03 (0.83–1.27) |
| Leukocytes | 9 | Obs | S * | NS | S | S | Undetect | ꚛꚛ○○ | 0.34 (−0.03; 0.7) | 1.84 (0.94; 3.59) |
| Lymphocytes | 6 | Obs | S * | NS | S | S | Detected | ꚛ○○○ | −0.23 (−0.52; 0.06) | 0.66 (0.39; 1.11) |
| Neutro/lympho ratio | 3 | Obs | S * | NS | S | NS | Detected | ꚛ○○○ | −0.31 (−1.64; 1.02) | 0.57 (0.05; 6.38) |
| Platelets | 13 | Obs | S * | NS | NS | NS | Undetect | ꚛꚛꚛ○ | 0.04 (−0.07; 0.15) | 1.08 (0.88; 1.32) |
| Platelets (peak) | 1 | Obs | S * | NS | NS | S | Detected | ꚛꚛ○○ | −0.76 (−1.19; −0.33) | 0.25 (0.12; 0.55) |
| Disease severity markers | ||||||||||
| NMB duration | 1 | Obs | S * | NS | NS | NS | Detected | ꚛꚛ○○ | 0.54 (0.25–0.83) | 2.64 (1.57–4.47) |
| PaO2/FiO2 | 4 | Obs | S * | NS | NS | S | Undetect | ꚛꚛ○○ | −0.13 (−0.41; 0.15) | 0.79 (0.48; 1.31) |
| Time factors | ||||||||||
| Disease onset to hospitalization | 2 | Obs | S * | NS | NS | S | Undetect | ꚛꚛ○○ | 0.09 (−0.27–0.44) | 1.18 (0.62–2.23) |
| Disease onset to ICU | 2 | Obs | S * | NS | NS | S | Undetect | ꚛꚛ○○ | −0.20 (−0.57; 0.17) | 0.70 (0.36; 1.36) |
| Time to VTE screening | 2 | Obs | S * | NS | S | S | Undetect | ꚛ○○○ | −0.05 (−0.83; 0.72) | 0.91 (0.22; 3.71) |
| VTE screening in ICU | 2 | Obs | S * | NS | NS | S | Detected | ꚛꚛ○○ | −0.68 (−1.17; −0.19) | 0.29 (0.12; 0.70) |
| Hospital stay duration | 2 | Obs | S * | NS | NS | NS | Undetect | ꚛꚛꚛ○ | 1.08 (0.68–1.48) | 7.09 (3.41–14.73) |
| MV duration | 2 | Obs | S * | NS | NS | S | Undetect | ꚛꚛ○○ | 0.39 (−0.06; 0.84) | 2.02 (0.90; 4.55) |
| ICU stay duration | 3 | Obs | S * | NS | S | S | Detected | ꚛ○○○ | 0.21 (−0.78; 1.20) | 1.46 (0.24; 8.81) |
| Variable | Certainty Assessment Domains | Overall Certainty | OR 95%CI | ||||||
|---|---|---|---|---|---|---|---|---|---|
| N | Study Design | Risk of Bias | Indirectness | Inconsistency | Imprecision | Publication Bias | |||
| Medical history | |||||||||
| Asthma | 2 | Obs | S * | NS | NS | S | Undetected | ꚛꚛ○○ | 0.95 (0.62–1.47) |
| ACE inhibitor use | 2 | Obs | S * | NS | NS | S | Undetected | ꚛꚛ○○ | 0.67 (0.19–2.33) |
| Alcohol use | 1 | Obs | S * | NS | NS | S | Undetected | ꚛꚛ○○ | 0.47 (0.14–1.55) |
| Cancer | 8 | Obs | S * | NS | NS | S | Undetected | ꚛꚛ○○ | 0.84 (0.51–1.38) |
| Cardiovascular disease | 2 | Obs | S * | NS | NS | S | Undetected | ꚛꚛ○○ | 0.32 (0.10–0.99) |
| Cerebrovascular disease | 2 | Obs | S * | NS | NS | S | Undetected | ꚛꚛ○○ | 0.84 (0.26–2.65) |
| Chronic kidney disease | 8 | Obs | S * | NS | NS | S | Undetected | ꚛꚛ○○ | 0.73 (0.50–1.06) |
| Chronic respiratory disease | 7 | Obs | S * | NS | NS | S | Undetected | ꚛꚛ○○ | 0.76 (0.47–1.23) |
| COPD | 3 | Obs | S * | NS | NS | S | Undetected | ꚛ○○○ | 0.42 (0.11–1.61) |
| Congestive heart failure | 4 | Obs | S * | NS | NS | S | Undetected | ꚛꚛ○○ | 0.57 (0.35–0.95) |
| Coronary artery disease | 5 | Obs | S * | NS | NS | S | Undetected | ꚛꚛ○○ | 1.00 (0.56–1.77) |
| Diabetes mellitus | 8 | Obs | S * | NS | NS | S | Undetected | ꚛꚛ○○ | 0.76 (0.52–1.11) |
| HIV | 1 | Obs | S * | NS | NS | S | Undetected | ꚛꚛ○○ | 1.75 (0.68–4.46) |
| Hypertension | 10 | Obs | S * | NS | NS | S | Undetected | ꚛꚛ○○ | 0.85 (0.64–1.11) |
| Immunodeficiency | 3 | Obs | S * | NS | NS | S | Undetected | ꚛꚛ○○ | 1.24 (0.56–2.73) |
| Myocarditis | 1 | Obs | S * | NS | NS | S | Undetected | ꚛꚛ○○ | 1.95 (0.50–7.57) |
| Previous VTE | 5 | Obs | S * | NS | NS | S | Undetected | ꚛꚛ○○ | 0.90 (0.27–2.98) |
| Smoker (past or current) | 3 | Obs | S * | NS | NS | S | Undetected | ꚛꚛ○○ | 0.96 (0.60–1.52) |
| Smoker (current) | 2 | Obs | S * | NS | NS | S | Undetected | ꚛꚛ○○ | 0.67 (0.16–2.83) |
| Smoker (past) | 1 | Obs | S * | NS | NS | S | Undetected | ꚛꚛ○○ | 0.92 (0.26–3.17) |
| Disease severity markers and therapeutic management | |||||||||
| Acute kidney injury | 1 | Obs | S * | NS | NS | S | Undetected | ꚛꚛ○○ | 1.73 (0.44–6.81) |
| ECMO | 5 | Obs | S * | NS | NS | S | Undetected | ꚛꚛ○○ | 0.95 (0.46–1.97) |
| Inotrope use | 7 | Obs | S * | NS | NS | S | Undetected | ꚛꚛ○○ | 1.67 (1.15–2.43) |
| Mechanical ventilation | 7 | Obs | S * | NS | NS | NS | Undetected | ꚛꚛꚛ○ | 2.61 (1.94–3.51) |
| Neuromuscular blockers | 2 | Obs | S * | NS | NS | S | Undetected | ꚛꚛ○○ | 1.41 (0.64–3.09) |
| Renal replacement | 5 | Obs | S * | NS | NS | S | Undetected | ꚛꚛ○○ | 1.39 (0.93–2.10) |
| Anticoagulation | |||||||||
| No anticoagulation | 2 | Obs | S * | NS | NS | S | Undetected | ꚛꚛ○○ | 6.32 (0.73–54.58) |
| Prophylactic | 5 | Obs | S * | NS | NS | S | Undetected | ꚛꚛ○○ | 0.73 (0.46–1.17) |
| Intermediate | 1 | Obs | S * | NS | NS | S | Undetected | ꚛꚛ○○ | 0.70 (0.29–1.70) |
| Therapeutic | 7 | Obs | S * | NS | S | S | Undetected | ꚛꚛ○○ | 1.21 (0.61–2.38) |
| Demographic factors | |||||||||
| Male sex | 16 | Obs | S * | NS | NS | S | Undetected | ꚛꚛ○○ | 1.32 (0.84–2.06) |
| Obesity | 4 | Obs | S * | NS | NS | S | Undetected | ꚛꚛ○○ | 1.41 (0.64–3.09) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lobbes, H.; Mainbourg, S.; Mai, V.; Douplat, M.; Provencher, S.; Lega, J.-C. Risk Factors for Venous Thromboembolism in Severe COVID-19: A Study-Level Meta-Analysis of 21 Studies. Int. J. Environ. Res. Public Health 2021, 18, 12944. https://doi.org/10.3390/ijerph182412944
Lobbes H, Mainbourg S, Mai V, Douplat M, Provencher S, Lega J-C. Risk Factors for Venous Thromboembolism in Severe COVID-19: A Study-Level Meta-Analysis of 21 Studies. International Journal of Environmental Research and Public Health. 2021; 18(24):12944. https://doi.org/10.3390/ijerph182412944
Chicago/Turabian StyleLobbes, Hervé, Sabine Mainbourg, Vicky Mai, Marion Douplat, Steeve Provencher, and Jean-Christophe Lega. 2021. "Risk Factors for Venous Thromboembolism in Severe COVID-19: A Study-Level Meta-Analysis of 21 Studies" International Journal of Environmental Research and Public Health 18, no. 24: 12944. https://doi.org/10.3390/ijerph182412944
APA StyleLobbes, H., Mainbourg, S., Mai, V., Douplat, M., Provencher, S., & Lega, J. -C. (2021). Risk Factors for Venous Thromboembolism in Severe COVID-19: A Study-Level Meta-Analysis of 21 Studies. International Journal of Environmental Research and Public Health, 18(24), 12944. https://doi.org/10.3390/ijerph182412944