
Analysis of Factors Related to Working Status of Dental Hygienists in Japan



Abstract
:1. Introduction
2. Subjects and Methods
2.1. Study Setting
2.2. Selection of Subjects and Research Design
2.3. Survey Items
2.4. Analysis Methods
2.5. Ethical Approval
3. Results
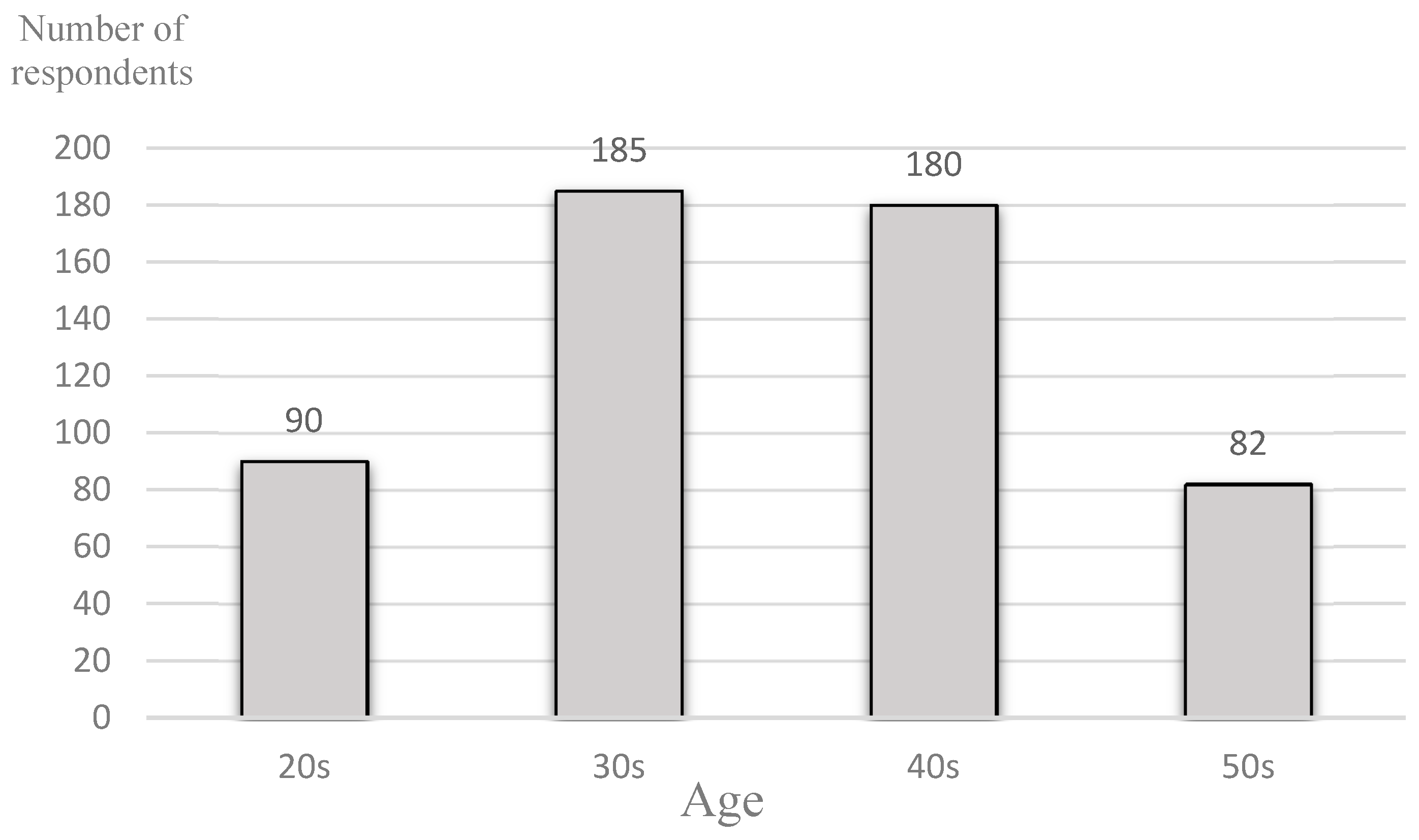
3.1. Respondents’ Demographic Information
3.2. Analysis of the Priority of Working
3.3. Analysis of Factors Related to Employment Status (1): Bivariate Analysis
3.4. Analysis of Factors Related to Employment Status (2): Multivariate Analysis
4. Discussion
4.1. Trends in Employment Rate and Other Factors by Age Group
4.2. Analysis of Factors Related to Employment
4.2.1. Bivariate Analysis
4.2.2. Multivariate Analysis
4.3. Professional Education for Dental Hygienists
4.4. Provision of Oral Health Services in Japan
4.5. Limitation of This Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Tada, A.; Miura, H. Systematic review of the association with food and nutrient intake in the dependent elderly. Arch. Gerontol. Geriatr. 2014, 59, 497–505. [Google Scholar] [CrossRef] [PubMed]
- Hakeen, F.; Bernabe, E.; Sabbah, W. Association between oral health and frailty: A systematic review of longitudinal studies. Gerodontology 2019, 36, 205–215. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Ageing and Health; WHO: Geneva, Switzerland, 2015; pp. 3–13.
- Toniazzo, M.P.; Amorim, P.; Muniz, F.; Weidbh, P. Relationship of nutritional status and oral health in elderly. Systematic review with meta-analysis. Clin. Nutr. 2018, 37, 824–830. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, Y.; Okada, K.; Kondo, M.; Matsushita, T.; Nakazawa, S.; Yamazaki, Y. Oral health for achieving longevity. Geriatr. Gerontol. Int. 2020, 20, 526–538. [Google Scholar] [CrossRef] [PubMed]
- Yokoyama, T. National Health Promotion Measures in Japan: Health Japan 21 (the second term). J. Natl. Inst. Public Health 2020, 69, 14–24. [Google Scholar]
- Oral Health for an Ageing Population. Available online: https://www.fdiworlddental.org/what-we-do/projects/oral-health-for-an-ageing-population (accessed on 5 October 2020).
- Usui, Y.; Miura, H.; Tamaki, Y. Survey on future needs and agendas related to promoting dental and oral health of super aging society among influential experts. Jpn. J. Gerontol. 2013, 28, 304–309. [Google Scholar]
- Yoneyama, T.; Yoshida, M.; Ohrui, T.; Mukaiyama, H.; Okamoto, H.; Sasaki, H. Oral care reduces pneumonia in older patients in nursing home. J. Am. Geriatr. Soc. 2002, 50, 430–433. [Google Scholar] [CrossRef] [PubMed]
- Adachi, M.; Ishihara, K.; Abe, S.; Okuda, K. Professional oral health care by dental hygienists reduced respiratory infections in elderly persons requiring nursing care. Int. J. Dent. Hyg. 2007, 5, 69–74. [Google Scholar] [CrossRef] [PubMed]
- Kanazawa, N. Prospects and subjects of dental hygienists: Aiming at coordination with medical care and elderly care. Ann. Jpn. Prosthodont. Soc. 2014, 6, 267–272. [Google Scholar] [CrossRef]
- Usui, Y.; Miura, H. Workforce re-entry for Japanese unemployed dental hygienist. Int. J. Dent. Hyg. 2014, 13, 74–78. [Google Scholar] [CrossRef] [PubMed]
- Miura, H.; Kariyasu, M.; Yamasaki, K.; Sumi, Y. Physical, mental and social factors affecting self-rated verbal communication among elderly individuals. Geriatr. Gerontol. Int. 2004, 4, 100–104. [Google Scholar] [CrossRef]
- Japan Dental Hygienists Association. Report on the Study Group on Securing Human Resources for Dental Hygienists and Support for Return to Work; Japan Dental Hygienists Association: Tokyo, Japan, 2017; p. 31. [Google Scholar]
- Summary of the Survey of Employment of Young People in Japan. Available online: https://www.mhlw.go.jp/tukei/list/dl/4-21-iyakurenkoyou-h30.gaikyo.pdf (accessed on 5 October 2020).
- Labour Force Survey. Available online: https://www.stat.go.jp/data/roudou (accessed on 5 October 2020).
- University Training Center for Dental Hygienists Returning to Work. Available online: https://www2.Jdha.or.jp/info/info_training.html (accessed on 5 October 2020).
- Johns, G.H.; Gutmann, M.E.; Dewald, J.P.; Nunn, M.E. Career retention in the dental hygiene workforce in Texas. J. Dent. Hyg. 2001, 75, 135–148. [Google Scholar] [PubMed]
- Inukai, J.; Sakurai, M.; Nakagaki, H.; Matsui, K.; Matsuda, H.; Tamura, K.; Danielsen, B.; Rowbothan, J.; Kosaka, T. Comparison of clinical practice education in dental hygiene schools in eight countries. Int. Dent. J. 2012, 62, 122–126. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, N.; Endo, K.; Komaki, M. Dental hygiene education in Japan: Present status and future directions. Int. J. Dent. Hyg. 2004, 2, 179–184. [Google Scholar] [CrossRef] [PubMed]
- Muroga, R.; Tsuruta, J.; Morio, I. Disparity in perception of the working condition of dental hygienists between dentists and dental hygiene students in Japan. Int. J. Dent. Hyg. 2015, 13, 213–221. [Google Scholar] [CrossRef] [PubMed]
- Nagatani, Y.; Imafuku, R.; Takemoto, T.; Waki, T.; Obayashi, T.; Ogawa, T. Dental hygienists’ perceptions of professionalism are multi-dimensional and context-dependent: A qualitative study in Japan. BMC Med Educ. 2017, 17, 267. [Google Scholar] [CrossRef] [PubMed]
- Nomura, Y.; Okada, A.; Miyoshi, J.; Mukaida, M.; Akasaka, E.; Saigo, K.; Daikoku, H.; Maekawa, H.; Sato, T.; Hanada, N. Willingness to work and the working environment of Japanese dental hygienists. Int. J. Dent. 2018, 2018, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kodama, T.; Ida, Y.; Miura, H. A Nationwide survey on working hours and working environment among hospital dentists in Japan. Int. J. Environ. Res. Public Health 2020, 17, 9048. [Google Scholar] [CrossRef] [PubMed]
- Virtanen, J.I.; Pellikka, E.; Singh, S.; Widstrom, E. The professional role of a dental hygienist in Finland: Educators’ view. Int. J. Dent. Hyg. 2016, 14, 231–238. [Google Scholar] [CrossRef] [PubMed]
- Jokiaho, T.-L.; Kaakinen, P.; Virtanen, J.I. Dose dental hygienist professional education meet the needs of working life? Educators’ view. Int. J. Dent. Hyg. 2018, 16, 134–143. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | Age | χ2-Value | p-Value | |||
|---|---|---|---|---|---|---|
| 20s | 30s | 40s | 50s | |||
| Employment rate (%) | 85.55 | 67.56 | 68.33 | 50.62 | 20.93 | <0.01 |
| Marriage rate (%) | 23.33 | 70.81 | 76.67 | 81.48 | 38.56 | <0.01 |
| Subjects with children (%) | 14.77 | 65.76 | 71.51 | 76.83 | 36.30 | <0.01 |
| Training participation rate (%) | 60.00 | 43.78 | 34.63 | 31.71 | 16.82 | <0.01 |
| Subjects seeking full-time work (%) | 80.00 | 44.32 | 47.22 | 32.93 | 21.57 | <0.01 |
| Variable | % |
|---|---|
| Working hours | 80.82 |
| Human relations at the workplace | 80.07 |
| Wages | 73.37 |
| Working location | 60.89 |
| Job description | 52.33 |
| (A) Chi-square Test | ||||
|---|---|---|---|---|
| Variable | Employed (N = 366) | Unemployed (N = 171) | χ2-Value | p-Value |
| Marriage rate (%) | 58.47 | 82.46 | 32.27 | <0.001 |
| Subjects with children (%) | 54.10 | 73.68 | 18.32 | <0.001 |
| Training participation rate (%) | 54.92 | 12.87 | 83.5 | <0.001 |
| Subjects seeking full-time work (%) | 60.38 | 12.87 | 102.44 | <0.001 |
| (B) Unpaired t-test | ||||
| Variable | Employed (N = 366) | Unemployed (N = 171) | t-Value | p-Value |
| Age (years) | 37.99 ± 8.95 | 41.31 ± 8.37 | 4.07 | <0.01 |
| Variable | Employed (%) | Unemployed (%) | χ2-Value | p-Value |
|---|---|---|---|---|
| Working hours | 83.61 | 74.85 | 5.21 | <0.001 |
| Human relations at workplace | 80.33 | 79.53 | 0.01 | NS |
| Wages | 80.05 | 59.06 | 25.40 | <0.001 |
| Working location | 62.57 | 57.31 | 1.18 | NS |
| Job description | 54.10 | 48.54 | 1.30 | NS |
| Independent Variable | β | SE | Wald | p-Value | OR | 95% CI |
|---|---|---|---|---|---|---|
| Participation in training programs | 1.87 | 0.27 | 47.62 | <0.001 | 6.50 | 3.82–11.07 |
| Desired for full-time work | 1.20 | 0.19 | 40.34 | <0.001 | 0.30 | 0.21–0.44 |
| Priority assigned to wages | 0.75 | 0.24 | 9.55 | <0.01 | 2.12 | 1.32–3.42 |
| Priority assigned to working hours | 0.65 | 0.29 | 5.11 | <0.05 | 1.91 | 1.09–3.34 |
| Constant | 1.14 | 0.43 | 6.97 | <0.01 | 3.13 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Miura, H.; Tano, R.; Oshima, K.; Usui, Y. Analysis of Factors Related to Working Status of Dental Hygienists in Japan. Int. J. Environ. Res. Public Health 2021, 18, 1025. https://doi.org/10.3390/ijerph18031025
Miura H, Tano R, Oshima K, Usui Y. Analysis of Factors Related to Working Status of Dental Hygienists in Japan. International Journal of Environmental Research and Public Health. 2021; 18(3):1025. https://doi.org/10.3390/ijerph18031025
Chicago/Turabian StyleMiura, Hiroko, Rumi Tano, Katsuo Oshima, and Yoshie Usui. 2021. "Analysis of Factors Related to Working Status of Dental Hygienists in Japan" International Journal of Environmental Research and Public Health 18, no. 3: 1025. https://doi.org/10.3390/ijerph18031025
APA StyleMiura, H., Tano, R., Oshima, K., & Usui, Y. (2021). Analysis of Factors Related to Working Status of Dental Hygienists in Japan. International Journal of Environmental Research and Public Health, 18(3), 1025. https://doi.org/10.3390/ijerph18031025