
Factors Associated with Non-Attendance at Dental Preventive Care in Slovak High School Students

 , ,
, ,  , and
, and 
Abstract
:1. Introduction
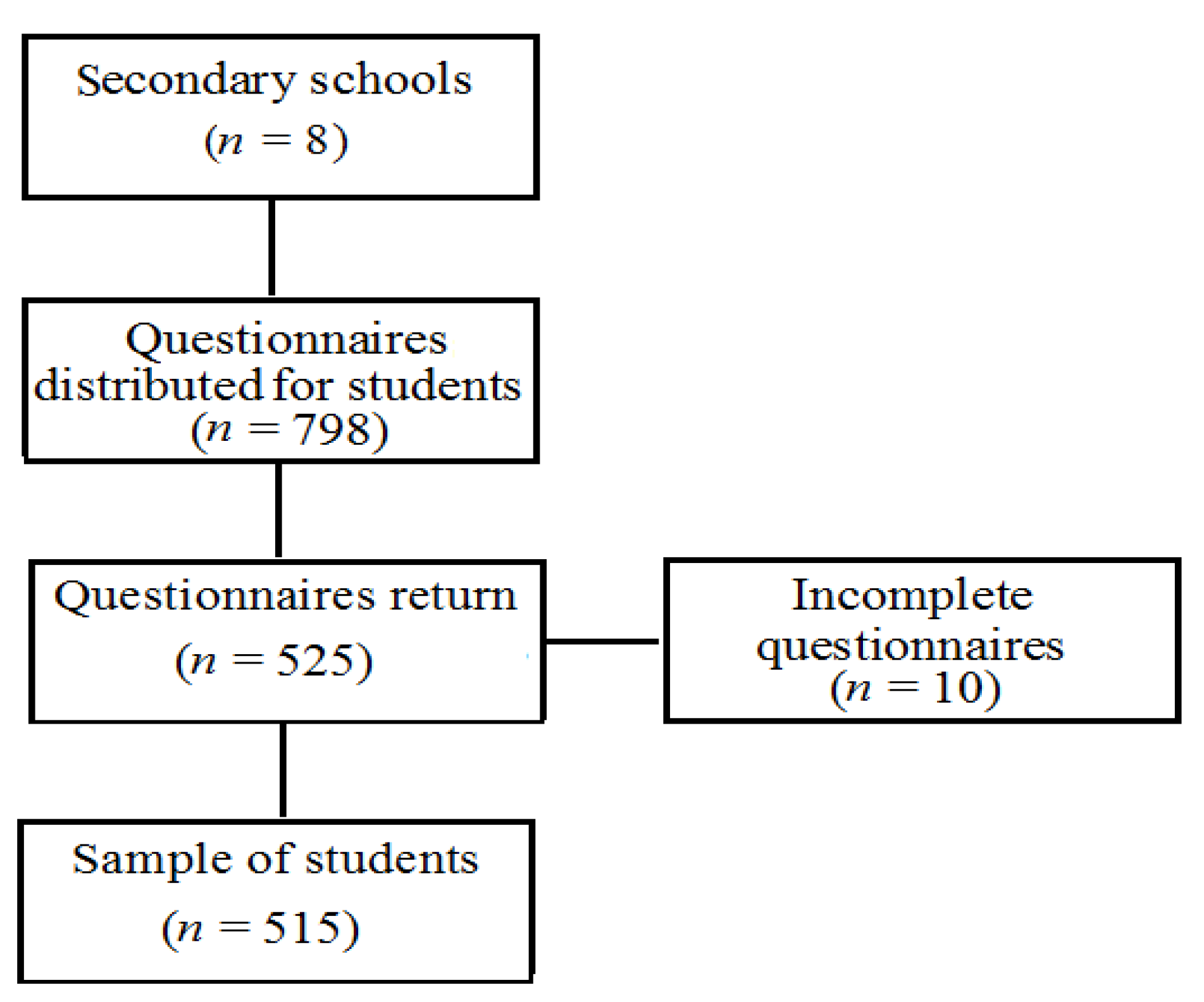
2. Materials and Methods
Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Davidovich, E.; Grender, J.; Zini, A. Factors Associated with Dental Plaque, Gingivitis, and Caries in a Pediatric Population: A Records-Based Cross-Sectional Study. Int. J. Environ. Res. Public Health 2020, 17, 8595. [Google Scholar] [CrossRef] [PubMed]
- Patel, R. The State of Oral Health in Europe. Report Commissioned by the Platform for Better Oral Health in Europe. 2015. Available online: http://www.oralhealthplatform.eu/wp-content/uploads/2015/09/Report-the-State-of-Oral-Health-in-Europe.pdf (accessed on 5 September 2018).
- Pourat, N.; Choi, M.K.; Chen, X. Evidence of effectiveness of preventive dental care in reducing dental treatment use and related expenditures. J. Public Health Dent. 2018, 78, 203–213. [Google Scholar] [CrossRef] [PubMed]
- Alhabdan, Y.A.; Albeshr, A.G.; Yenugadhati, N.; Jradi, H. Prevalence of dental caries and associated factors among primary school children: A population-based cross-sectional study in Riyadh, Saudi Arabia. Environ. Health Prev. Med. 2018, 23, 60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anil, S.; Anand, P.S. Early childhood caries: Prevalence, risk factors, and prevention. Front. Pediatr. 2017, 5, 157. [Google Scholar] [CrossRef] [Green Version]
- Bhaskar, V.; McGraw, K.A.; Divaris, K. The importance of preventive dental visits from a young age: Systematic review and current perspectives. Clin. Cosmet. Investig. Dent. 2014, 6, 21–27. [Google Scholar] [CrossRef] [Green Version]
- Athavale, P.; Khadka, N.; Roy, S.; Mukherjee, P.; Chandra Mohan, D.; Turton, B.B.; Sokal-Gutierrez, K. Early Childhood Junk Food Consumption, Severe Dental Caries, and Undernutrition: A Mixed-Methods Study from Mumbai, India. Int. J. Environ. Res. Public Health 2020, 17, 8629. [Google Scholar] [CrossRef]
- Birch, S.; Bridgman, C.; Brocklehurst, P.; Elwood, R.; Gomez, J.; Helgeson, M.; Ismail, A.; Macey, R.; Mariotii, A.; Twetman, S.; et al. Prevention in practice—A summary. BMC Oral Health 2015, 15 (Suppl. S1), S12. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Data and Statistics. 2016. Available online: http://www.euro.who.int/en/health-topics/disease-prevention/oral-health/data-and-statistics (accessed on 1 October 2016).
- Center for Disease Control and Prevention. Division of Adolescent and School Health. 2016. Available online: https://www.cdc.gov/healthyyouth/about/pdf/strategic_plan/dash_strategic_plan.pdf (accessed on 1 December 2016).
- Institute of Medicine (US) and National Research Council (US) Committee on the Science of Adolescence. The Science of Adolescent Risk-Taking: Workshop Report; National Academies Press (US): Washington, DC, USA, 2011; p. 144. [Google Scholar]
- Jaworska, N.; MacQueen, G. Adolescence as a unique developmental period. J. Psychiatry Neurosci. 2015, 40, 291–293. [Google Scholar] [CrossRef]
- Vrbič, V.; Vrbič, M.; Petersen, P.E. Epidemiology of dental caries and disease prevention among 12-year-olds in Slovenia over thirty years (1987–2017). Oral Health Prev. Dent. 2020, 18, 185–196. [Google Scholar] [CrossRef]
- European Commission. Special Eurobarometer 330. 2009. Available online: https://www.data.europa.eu/euodp/en/data/dataset/S795_72_3_EBS330 (accessed on 24 September 2009).
- National Center for Health Information. Health Yearbook of the Slovak Republic. 2019. Available online: http://www.nczisk.sk/Documents/rocenky/2018/Zdravotnicka_rocenka_Slovenskej_republiky_2018.pdf (accessed on 30 January 2019). (In Slovak).
- Yu, S.M.; Bellamy, H.A.; Schwalberg, R.H.; Drum, M.A. Factors associated with use of preventive dental and health services among U.S. adolescents. J. Adolesc. Health 2001, 29, 395–405. [Google Scholar] [CrossRef]
- Ronis, D.L.; Lang, W.P.; Farghaly, M.M.; Passow, E. Tooth brushing, flossing, and preventive dental visits by Detroit-area residents in relation to demographic and socioeconomic factors. J. Public Health Dent. 1993, 53, 138–145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shaban, R.; Kassim, S.; Sabbah, W. Socioeconomic inequality in the provision of specific preventive dental interventions among children in the UK: Children’s Dental Health Survey 2003. Br. Dent. J. 2017, 222, 865–869. [Google Scholar] [CrossRef] [PubMed]
- Fonseca, E.P.D.; Frias, A.C.; Mialhe, F.L.; Pereira, A.C.; Meneghim, M.C. Factors associated with last dental visit or not to visit the dentist by Brazilian adolescents: A population-based study. PLoS ONE 2017, 12, e0183310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Michalak, E.; Łoboda, J.; Chomyszyn-Gajewska, M. Reasons for patients’ visits in the dental offices of Cracow in the years 2005–2006 and 2013–2014. Przegl. Epidemiol. 2015, 69, 787–794. [Google Scholar]
- Timková, S.; Kolarčik, P.; Gecková, A.M. Self-Reported Oral Health Related Behaviour and Gum Bleeding of Adolescents in Slovakia in Relation to Socioeconomic Status of Their Parents: Cross-Sectional Study Based on Representative Data Collection. Int. J. Environ. Res. Public Health 2019, 16, 2484. [Google Scholar] [CrossRef] [Green Version]
- Xu, F.; Mawokomatanda, T.; Flegel, D.; Pierannunzi, C.; Garvin, W.; Chowdhury, P.; Salandy, S.; Crawford, C.; Town, M. Surveillance for certain health behaviors among states and selected local areas—Behavioral risk factor surveillance system, United States, 2011. MMWR Surveill. Summ. 2014, 63, 1–149. [Google Scholar]
- Kann, L.; Kinchen, S.; Shanklin, S.L.; Flint, K.H.; Kawkins, J.; Harris, W.A.; Lowry, R.; Olsen, E.O.; MCManus, T.; Chyen, D.; et al. Youth risk behavior surveillance—The United States, 2013. MMWR Suppl. 2014, 63, 1–168. [Google Scholar]
- Babjakova, J.; Vondrova, D.; Jurkovicova, J.; Samohyl, M.; Filova, A.; Janko, Z.; Stefanikova, Z.; Hirosova, K.; Weitzman, M.; Argalasova, L. Risk behavioral survey in the sample of Slovak adolescents. Bratisl. Lek. Listy 2019, 120, 899–907. [Google Scholar] [CrossRef]
- Argalasova, L.; Vondrova, D.; Babjakova, J.; Hirosova, K.; Filova, A.; Samohyl, M.; Kachutova, I.; Jurkovicova, J.; Weitzman, M. Behavioural, psychosocial and life-style risk factors in a sample of Slovak adolescents. J. Infec. Dis. Treat. 2019, 5, 36. [Google Scholar]
- Aalsma, M.C.; Gilbert, A.L.; Xiao, S.; Rickert, V.I. Parent and adolescent views on barriers to adolescent preventive health care utilization. J. Pediatr. 2016, 169, 140–145. [Google Scholar] [CrossRef]
- Wilkes, M.S.; Anderson, M. A primary care approach to adolescent health care. West. J. Med. 2000, 172, 177–182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salam, R.A.; Das, J.K.; Lassi, Z.S.; Bhutta, Z.A. Adolescent health interventions: Conclusions, evidence gaps, and research priorities. J. Adolesc. Health 2016, 59, S88–S92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krasnik, A.; Sawitz, A.; Keiding, N.; Hansen, E. Determinants of general practice utilization in Denmark. Dan. Med. Bull. 1997, 44, 542–546. [Google Scholar] [PubMed]
- Anderson, J. The impact of family structure on the health of children: Effects of divorce. Linacre Q. 2014, 81, 378–387. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Variables | N (%) | |
|---|---|---|
| Gender | Male | 195 (37.9) |
| Female | 320 (62.1) | |
| Age groups (yrs) | 15–16 | 106 (20.6) |
| 16–17 | 157 (30.5) | |
| 17–18 | 119 (23.1) | |
| 18–19 | 79 (15.3) | |
| 19+ | 59 (10.5) | |
| Nationality * | Slovak | 469 (91.1) |
| Other | 46 (8.9) | |
| Type of school | Grammar | 209 (40.5) |
| Vocational | 126 (24.3) | |
| Secondary | 182 (35.2) | |
| Siblings | Yes | 425 (82.5) |
| No | 90 (17.5) | |
| Residence | Urban | 306 (59.4) |
| Rural | 209 (40.6) | |
| Family | Complete | 363 (71.3) |
| Incomplete | 146 (28.7) | |
| Father’s education † | Primary | 8 (2.8) |
| Secondary | 186 (64.1) | |
| University degree | 96 (33.1) | |
| Mother’s education † | Primary | 9 (2.3) |
| Secondary | 243 (62.5) | |
| University degree | 137 (35.2) | |
| Employment status father † | Employed | 454 (93.8) |
| Unemployed | 30 (6.2) | |
| Employment status mother † | Employed | 470 (91.3) |
| Unemployed | 45 (8.7) | |
| Variables | Study Group 1 | Control Group 2 | p-Value | |
|---|---|---|---|---|
| N (%) † (n = 57) | N (%) † (n = 458) | |||
| Gender | Male | 31 (54.4) | 164 (35.8) | 0.010 |
| Female | 26 (45.6) | 294 (64.2) | ||
| Age groups (yrs) | x ± SD | 17.2 ± 1.5 | 16.6 ± 1.3 | 0.004 |
| 15–16 | 5 (9.1) | 100 (22.1) | 0.025 | |
| 16–17 | 16 (29.1) | 140 (30.9) | ||
| 17–18 | 11 (20) | 107 (23.6) | 0.018 4 | |
| 18–19 | 12 (21.8) | 65 (14.3) | ||
| 19+ | 11 (20) | 41 (9.1) | 0.011 | |
| Type of school | Grammar | 18 (31.6) | 191 (41.7) | 0.309 |
| Vocational | 18 (31.6) | 106 (23.1) | ||
| Secondary | 21 (36.8) | 161 (35.2) | ||
| Residence | Urban | 35 (61.4) | 271 (59.2) | 0.747 |
| Rural | 22 (38.6) | 187 (40.8) | ||
| Family | Complete | 25 (43.9) | 338 (74.8) | <0.001 |
| Incomplete | 32 (56.1) | 114 (25.2) | ||
| Stress at home | Yes | 10 (17.5) | 29 (6.5) | 0.037 |
| No | 47 (82.5) | 420 (93.5) | ||
| Stress at school | Yes | 31 (54.4) | 223 (48.7) | 0.422 |
| No | 26 (45.6) | 235 (51.3) | ||
| Healthy feeling | Yes | 38 (67.9) | 397 (86.9) | 0.005 |
| No | 18 (32.1) | 60 (13.1) | ||
| Pediatric preventive care 3 | Yes | 36 (65.5) | 421 (91.5) | <0.001 |
| No | 19 (34.5) | 39 (8.5) | ||
| Selected Variables in Mothers | Study Group 1 | Control Group 2 | p-Value | |
|---|---|---|---|---|
| N (%) † (n = 35) | N (%) † (n = 355) | |||
| Age groups (yrs) | x ± SD | 42.4 ± 4.4 | 43.6 ± 5.1 | 0.183 |
| 30–50 | 33 (94.3) | 321 (90.4) | 0.371 | |
| 51–71 | 2 (5.7) | 34 (9.6) | ||
| Mother’s educational level | Primary school | 2 (5.7) | 7 (2.0) | 0.259 |
| High school | 23 (65.7) | 220 (62.1) | ||
| University | 10 (28.6) | 127 (35.9) | ||
| Marital status | Single | 4 (11.4) | 25 (7.0) | 0.034 |
| Married | 16 (45.7) | 263 (74.1) | ||
| Divorced | 13 (37.1) | 58 (16.3) | ||
| Widow | 2 (5.8) | 9 (2.6) | ||
| Residence | Urban | 22 (62.9) | 217 (61.1) | 0.843 |
| Rural | 13 (37.1) | 138 (38.9) | ||
| Employment | Yes | 30 (88.2) | 317 (89.8) | 0.789 |
| No | 4 (11.8) | 36 (10.2) | ||
| Household income (EUR) | ≤900 | 19 (55.9) | 115 (35.6) | 0.031 |
| >900 | 15 (44.1) | 208 (64.4) | ||
| Stress at work | Yes | 24 (75.0) | 244 (73.5) | 0.854 |
| No | 8 (25.0) | 88 (26.5) | ||
| Healthy feeling | Yes | 29 (82.9) | 291 (84.3) | 0.826 |
| No | 6 (17.1) | 54 (15.7) | ||
| Preventive care 3 | Yes | 23 (67.6) | 309 (88.5) | 0.017 |
| No | 11 (32.4) | 40 (11.5) | ||
| Dental preventive care | Yes | 17 (73.9) | 293 (95.1) | 0.034 |
| No | 6 (26.1) | 15 (4.9) | ||
| Variables | AOR | 95%CI | ||
|---|---|---|---|---|
| Selected variables in students | Gender | Female | 1 | - |
| Male | 2.11 | 1.09, 4.03 * | ||
| Age groups (yrs) | 15–18 | 1 | - | |
| 19+ | 1.19 | 0.51, 2.78 | ||
| Type of school | Grammar | 1 | - | |
| Secondary/Vocational | 1.32 | 0.65, 2.70 | ||
| Residence | Rural | 1 | - | |
| Urban | 0.77 | 0.08, 7.64 | ||
| Family | Complete | 1 | - | |
| Incomplete | 3.26 | 1.68, 6.30 *** | ||
| Stress at home | No | 1 | - | |
| Yes | 1.71 | 0.62, 4.68 | ||
| Stress at school | No | 1 | - | |
| Yes | 1.18 | 0.61, 2.28 | ||
| Healthy feeling | Yes | 1 | - | |
| No | 1.13 | 0.49, 2.60 | ||
| Pediatric preventive care 1 | Yes | 1 | - | |
| No | 5.14 | 2.40, 10.99 *** | ||
| Selected variables in mothers | Age group (yrs) | 30–50 | 1 | - |
| 51–71 | 0.40 | 0.05, 3.21 | ||
| Mother’s educational level | High school diploma/University | 1 | - | |
| Primary/High school without a diploma | 1.20 | 0.40, 3.62 | ||
| Marital status | Married/in relationship | 1 | - | |
| Single/divorced/widowed | 2.20 | 0.91, 5.32 | ||
| Residence | Rural | 1 | - | |
| Urban | 1.10 | 0.45, 2.66 | ||
| Employment | Yes | 1 | - | |
| No | 0.42 | 0.04, 4.41 | ||
| Household income (EUR) | >900 | 1 | - | |
| ≤ 900 | 1.51 | 0.63, 3.63 | ||
| Stress at work | No | 1 | - | |
| Yes | 0.97 | 0.67, 2.54 | ||
| Healthy feeling | Yes | 1 | - | |
| No | 0.86 | 0.25, 2.98 | ||
| Preventive care 2 | Yes | 1 | - | |
| No | 1.95 | 0.69, 5.46 | ||
| Dental preventive care | Yes | 1 | - | |
| No | 4.19 | 1.50, 11.71 ** | ||
| Selected variables in fathers | Age group (yrs) | 32–44 | 1 | - |
| 45–76 | 0.50 | 0.19, 1.27 | ||
| Father’s educational level | High school diploma/University | 1 | - | |
| Primary/High school without a diploma | 1.50 | 0.56, 4.02 | ||
| Marital status | Married/in relationship | 1 | - | |
| Single/divorced/widowed | 3.73 | 1.21, 11.54 * | ||
| Residence | Rural | 1 | - | |
| Urban | 0.91 | 0.34, 2.46 | ||
| Employment | Yes | 1 | - | |
| No | - | - | ||
| Household income (EUR) | >900 | 1 | - | |
| ≤900 | 0.48 | 0.14, 1.57 | ||
| Stress at work | No | 1 | - | |
| Yes | 0.47 | 0.18, 1.24 | ||
| Healthy feeling | Yes | 1 | - | |
| No | 1.98 | 0.56, 6.98 | ||
| Preventive care 3 | Yes | 1 | - | |
| No | 1.23 | 0.43, 3.50 | ||
| Dental preventive care | Yes | 1 | - | |
| No | 3.41 | 1.24, 9.32 * | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Samohyl, M.; Babjakova, J.; Vondrova, D.; Jurkovicova, J.; Stofko, J.; Kollar, B.; Hirosova, K.; Filova, A.; Argalasova, L. Factors Associated with Non-Attendance at Dental Preventive Care in Slovak High School Students. Int. J. Environ. Res. Public Health 2021, 18, 1295. https://doi.org/10.3390/ijerph18031295
Samohyl M, Babjakova J, Vondrova D, Jurkovicova J, Stofko J, Kollar B, Hirosova K, Filova A, Argalasova L. Factors Associated with Non-Attendance at Dental Preventive Care in Slovak High School Students. International Journal of Environmental Research and Public Health. 2021; 18(3):1295. https://doi.org/10.3390/ijerph18031295
Chicago/Turabian StyleSamohyl, Martin, Jana Babjakova, Diana Vondrova, Jana Jurkovicova, Juraj Stofko, Branislav Kollar, Katarina Hirosova, Alexandra Filova, and Lubica Argalasova. 2021. "Factors Associated with Non-Attendance at Dental Preventive Care in Slovak High School Students" International Journal of Environmental Research and Public Health 18, no. 3: 1295. https://doi.org/10.3390/ijerph18031295
APA StyleSamohyl, M., Babjakova, J., Vondrova, D., Jurkovicova, J., Stofko, J., Kollar, B., Hirosova, K., Filova, A., & Argalasova, L. (2021). Factors Associated with Non-Attendance at Dental Preventive Care in Slovak High School Students. International Journal of Environmental Research and Public Health, 18(3), 1295. https://doi.org/10.3390/ijerph18031295