
Whether Prolyl Hydroxylase Blocker—Roxadustat—In the Treatment of Anemia in Patients with Chronic Kidney Disease Is the Future?



Abstract
:1. Introduction
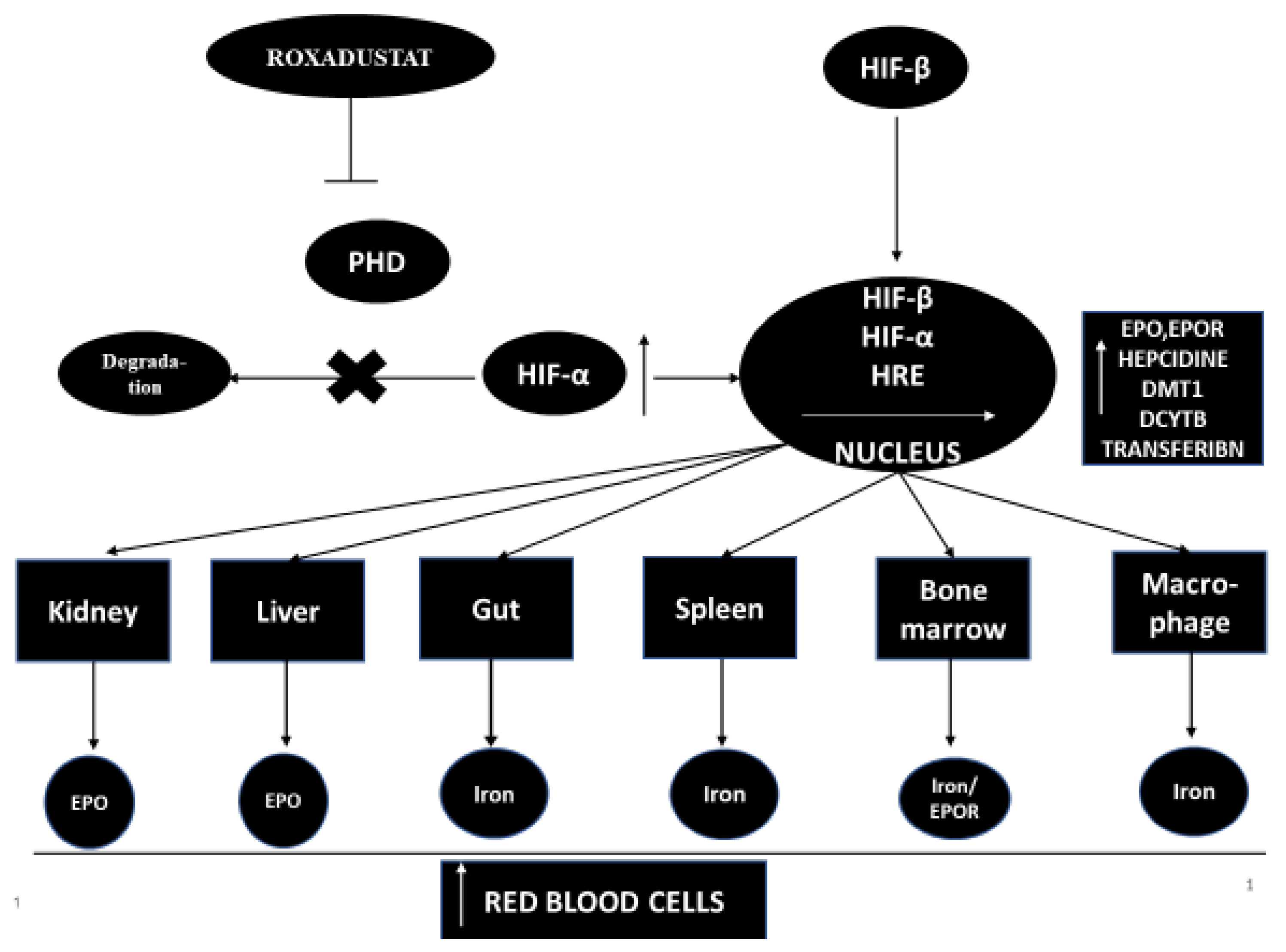
1.1. A Little Information about Roxadustat
1.2. Pharmacokinetics of Roxadustat
2. Roxadustat—Phase 1 Studies
3. Roxadustat—Phase 2 Studies
3.1. Roxadustat in Patients with Terminal Renal Failure Not Treated by Dialysis
3.2. Roxadustat in Patients with Terminal Renal Failure Treated by Dialysis
3.3. Summary
4. Roxadustat—Phase 3 Studies
4.1. Roxadustat in Patients with Terminal Renal Failure, Not Treated by Dialysis
4.1.1. The First Stage of the Study
4.1.2. The Second Stage of the Study
4.2. Roxadustat in Patients with Terminal Renal Failure, Treated by Hemodialysis or Peritoneal Dialysis
5. Additional Assessed Parameters
5.1. Hepcidin
5.2. Lipids
5.3. C-Reactive Protein (CRP)
6. Summary
6.1. Adverse Events after Roxadustat
6.2. Potential Benefits of Roxadustat, Assumed after Clinical Trials with CKD Patients, Both Non-Dialyzed and Dialyzed
6.3. Roxadustat Effects in Patients with Diabetes and Obesity
6.4. New Clinical Trials of Roxadustat in Patients with CKD
- DOLOMITES study (NCT02021318). It is a randomized, open-label, Phase 3 study that compares the anemia control efficacy and safety of roxadustat versus darberythropoietin in 616 patients with non-dialyzed CKD.
- In a randomized, open-label, phase 3 trial by Japanese authors (NCT02988973), the observation of CKD patients was not treated with renal replacement therapy, comparing the efficacy and safety of roxadustat versus darberythropoietin. Subjects were previously treated with recombinant human EPO or darberythropoietin alfa. Another study to be enrolled in 325 will evaluate the efficacy of anemia correction and the safety of roxadustat in patients who have previously been treated with beta erythropoietin. The primary endpoint of this study will be the ocean of change in Hb levels after 18–24 weeks of treatment.
- An open-label, phase 2/3 extension study (NCT01630889) assesses the long-term efficacy of anemia control and the safety of roxadustat in patients with CKD not treated and treated with dialysis.
- Preparations are underway to start a randomized, double-blind, placebo-controlled, phase III study (NCT03263091). The aim of the research is to assess the efficacy and safety of roxadustat in the treatment of anemia in patients at low risk of myelodysplastic syndrome MDS and not receiving frequent blood transfusions. The authors plan to include 184 patients with CKD in the study. The authors set the main goal of the study as not to transfuse blood for ≥56 days.
- Currently, 175 patients with CKD are enrolled in the Phase 2/3 study (NCT03303066), which aims to assess the efficacy (percentage of people with an Hb increase that allows life without transfusion) and the safety of roxadustat in a lower risk of MDS. The study is to be completed by the end of 2020.
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Podolak-Dawidziak, M. Anemia, Internal Medicine Szczeklik; Practical Medicine Krakow: Krakow, Poland, 2018; p. 1719. [Google Scholar]
- Bright, R. Cases and Observations Illustrative of Renal Disease, Accompanied with the Secretion of Albuminous Urine. Med. Chir. Rev. 1836, 49, 23–35. [Google Scholar]
- Becker, K.; Saad, M. A new approach to the management of anemia in CKD patients: A review on roxadustat. Adv. Ther. 2017, 34, 848–853. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Locatelli, F.; Fishbane, S.; Block, G.A.; Macdougall, I.C. Targeting hypoxia-inducible factors for the treatment of anemia in CKD patients. Am. J. Nephrol. 2017, 5, 187–199. [Google Scholar] [CrossRef] [PubMed]
- Semenza, G.L. Oxygen sensing, hypoxia-inducible factors, and disease pathophysiology. Annu. Rev. Pathol. 2014, 9, 47–71. [Google Scholar] [CrossRef] [PubMed]
- Haase, V.H. HIF-prolyl hydroxylases as therapeutic targets in erythropoiesis and iron metabolism. Hemodial. Int. 2017, 21 (Suppl. 1), S110–S124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bernhardt, W.M.; Wiesener, M.S.; Scigalla, P.; Chou, J.; Schmieder, R.; Gumzler, V.; Eckardt, K. Inhibition of prolyl hydroxylases increases erythropoietin production in ESRD. J. Am. Soc. Nephrol. 2010, 21, 2151–2156. [Google Scholar] [CrossRef]
- Provenzano, R.; Besarab, A.; Wright, S.; Dua, S.; Zeig, S.; Nguyen, P.; Poole, L.; Saikali, K.G.; Saha, G.; Hemmerich, S.; et al. Roxadustat (FG-4592) versus epoetin alfa for anemia in patients receiving maintenance hemodialysis: A phase 2, randomise, 6- to 19-week, open-Label, active-comparator, dose-ranging, safety and exploratory efficacy study. Am. J. Kidney Dis. 2016, 67, 912–924. [Google Scholar] [CrossRef] [Green Version]
- Provenzano, R.; Besarab, A.; Sun, C.H.; Diamond, S.A.; Durham, J.H.; Cangiano, J.L.; Aiello, J.R.; Novak, J.E.; Lee, T.; Leong, R.; et al. Oral hypoxia-inducible factor prolyl hydroxylase inhibitor roxadustat (FG-4592) for the treatment of anemia in patients with CKD. Clin. J. Am. Soc. Nephrol. 2016, 11, 982–991. [Google Scholar] [CrossRef]
- Flamme, I.; Oehme, F.; Ellinghaus, P.; Jeske, M.; Keldenich, J.; Thuss, U. Mimicking hypoxia to treat anemia: HIF-stabilizer BAY 85-3934 (Molidustat) stimulates erythropoietin production without hypertensive effects. PLoS ONE 2014, 9, e111838. [Google Scholar]
- Besarab, A.; Provenzano, R.; Hertel, J.; Zabaneh, R.; Klaus, S.; Lee, T.; Leong, R.; Hemmerich, S.; Peony Yu, K.-H.; Neff, T. Randomise placebo controlled dose-ranging and pharmacodynamics study of roxadustat (FG-4592) to treat anemia in nondialysis-dependent CKD (NDD-CKD) patients. Nephrol. Dial. Transplant. 2015, 30, 1665–1673. [Google Scholar] [CrossRef]
- FibroGen. FibroGen Announces Positive Topline Results from Three Global Phase 3 Trials of Roxadustat for Treatment of Anemia in Patients with CKD: Primary Efficacy Endpoints Met in All Three Studies, Non-Dialysis, Incident Dialysis, and Stable Dialysis Studies [Media Release]. 20 December 2018. Available online: http://investor.fibrogen.com/phoenix.zhtml?c=253783&p=irol-newsArticle_print&ID=2381297 (accessed on 20 December 2018).
- Groenendaal-van de Meent, D.; Adel, M.D.; Noukens, J.; Rijnders, S.; Krebs-Brown, A.; Mateva, L.; Alexiev, A.; Schaddelee, M. Effect of moderate hepatic impairment on the pharmacokinetics and pharmacodynamics of roxadustat, an oral hypoxia-inducible factor prolyl hydroxylase inhibitor. Clin. Drug Investig. 2016, 36, 743–751. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haase, V.H. Hypoxic regulation of erythropoiesis and iron metabolism. Am. J. Physiol. Renal. Physiol. 2010, 299, F1–F13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- AstraZeneca. Phase III OLYMPUS and ROCKIES Trials for Roxadustat Met Their Primary Endpoints in CKD Patients with Anaemia [Media Release]. 2018. Available online: https://www.astrazeneca.com/media-centre/pressreleases/2018/phase-iii-olympusand-rockies-trials-for-roxadustat-met-their-primary-endpoints-inchronic-kidney-disease-patients-with-anaemia20122018.html (accessed on 20 December 2018).
- Chen, N.; Hao, C.; Peng, X.; Lin, H.; Yin, A.; Hao, L.; Tao, Y.; Liang, X.; Liu, Z.; Xing, C.; et al. Roxadustat for anemia in patients with kidney disease not receiving dialysis. N. Engl. J. Med. 2019, 381, 1001–1010. [Google Scholar] [CrossRef] [PubMed]
- Astellas Pharma. Astellas Announces Positive Topline Results for Global Phase 3 Trial of Roxadustat in CKD (CKD) Patients with Anemia Not on Dialysis [Media Release]. 20 September 2018. Available online: https://www.astellas.com/system/files/news/2018-09/180920_eg.pdf (accessed on 20 September 2018).
- Chen, N.; Hao, C.; Liu, B.; Lin, H.; Wang, C.; Xing, C.; Liang, X.; Jiang, G.; Liu, Z.; Li, X.; et al. Roxadustat Treatment for Anemia in Patients Undergoing Long-Term Dialysis. N. Engl. J. Med. 2019, 381, 1011–1020. [Google Scholar] [CrossRef] [PubMed]
- Groenendaal-van de Meent, D.; den Adel, M.; Rijnders, S.; Krebs- Brown, A.; Kerbusch, V.; Golor, G.; Schaddelee, M. The hypoxia-inducible factor prolyl-hydroxylase inhibitor roxadustat (FG-4592) and warfarin in healthy volunteers: A pharmacokinetic and pharmacodynamic drug-drug interaction study. Clin. Ther. 2016, 38, 918–928. [Google Scholar] [CrossRef] [PubMed]
- Akizawa, T.; Otsuka, T.; Reusch, M.; Ueno, M. Intermittent Oral Dosing of Roxadustat in Peritoneal Dialysis Chronic Kidney Disease Patients with Anemia: A Randomized, Phase 3, Multicenter, Open-Label Study. Ther. Apheresis Dial. 2020, 24, 115–125. [Google Scholar] [CrossRef] [Green Version]
- Akizawa, T.; Iwasaki, T.; Otsuka, T. Roxadustat Treatment of Chronic Kidney Disease Associated Anemia in Japanese Patients Not on Dialysis: A Phase 2, Randomized, Double-Blind, Placebo-Controlled Trial. Adv. Ther. 2019, 36, 1438–1454. [Google Scholar] [CrossRef] [Green Version]
- Dhillon, S. Roxadustat: First Global Approval. Drugs 2019, 79, 563–572. [Google Scholar] [CrossRef]
- Besarab, A.; Chernyavskaya, E.; Motylev, I.; Shutov, E.; Kumbar, L.; Gurevich, K.; Tak Mao Chan, M.; Leong, R.; Poole, L.; Zhong, M.; et al. Roxadustat (FG4592): Correction of anemia in incident dialysis patients. J. Am. Soc. Nephrol. 2016, 27, 1225–1233. [Google Scholar] [CrossRef] [Green Version]
- Rabinowitz, M.H. Inhibition of hypoxia-inducible factor prolyl hydroxylase domain oxygen sensors: Tricking the body into mounting orchestrated survival and repair responses. J. Med. Chem. 2013, 56, 9369–9402. [Google Scholar] [CrossRef]
- Li, Z.; Tu, Y.; Liu, B. Treatment of renal anemia with roxadustat: Advantages and achievement. Kidney Dis. 2020, 6, 65–73. [Google Scholar] [CrossRef] [PubMed]
- Del Balzo, U.; Signore, P.E.; Walkinshaw, G.; Seeley, T.; Brenner, M.; Wang, Q.; Guo, G.; Arend, M.; Flippin, L.; Chow, A.; et al. Nonclinical Characterization of the HIF-Prolyl Hydroxylase Inhibitor Roxadustat, a Novel Treatment for Anemia of Chronic Kidney Disease Fast Forward. J. Pharmacol. Exp. Ther. 2020. [Google Scholar] [CrossRef] [PubMed]
- Noonan, M.; Clinkenbeard, E.; Ni, P.; Swallow, E.; Tippen, S.; Agoro, R.; Allen, M.; White, K. Erythropoietin and a hypoxia-inducible factor prolyl hydroxylase inhibitor (HIF-PHDi) lowers FGF23 in a model of chronic kidney disease (CKD). Physiol. Rep. 2020, 8, e14434. [Google Scholar] [CrossRef]
- Akizawa, T.; Yamagushi, Y.; Otsuka, T. A Phase 3, Multicenter, Randomized, Two-Arm, Open-Label Study of Intermittent Oral Dosing of Roxadustat for the Treatment of Anemia in Japanese Erythropoiesis-Stimulating Agent-Naïve Chronic Kidney Disease Patients Not on Dialysis. Nephron 2020, 144, 372–382. [Google Scholar] [CrossRef]
- Provenzano, R.; Tumlin, J.; Zabaneh, R.; Chou, J.; Hemmerich, S.; Neff, T.B.; Yu, K.P. Oral Hypoxia-Inducible Factor Prolyl Hydroxylase Inhibitor Roxadustat (FG-4592) for Treatment of Anemia in Chronic Kidney Disease: A Placebo-Controlled Study of Pharmacokinetic and Pharmacodynamic Profiles in Hemodialysis Patients. J. Clin. Pharmacol. 2020. [Google Scholar] [CrossRef]
- Pirri, D.; Fragiadaki, M.; Evans, P. Diabetic atherosclerosis: Is there a role for the hypoxia-inducible factors? Biosci. Rep. 2020, 40. [Google Scholar] [CrossRef]
- Chen, N.; Hao, C.; Peng, X.; Lin, H.; Yin, A.; Hao, L.; Tao, Y.; Liang, X.; Liu, Z.; Xing, C.; et al. A phase 3, randomise, doubleblind, placebo-controlled study of efficacy and safety of roxadustat (FG-4592) for treatment of anemia in subjects with CKD not on dialysis (abstract no. TH-PO1153). J. Am. Soc. Nephrol. 2018, 29, B5. [Google Scholar]
- Akizawa, T.; Iwasaki, M.; Yamaguchi, Y.; Majikawa, Y.; Reusch, M. Phase 3, randomise, double-blind, active-comparator (darberythropoietin alfa) conversion study of oral roxadustat in CKD patients with anemia on hemodialysis in Japan. J. Am. Soc. Nephrol. 2020, 31, 1628–1639. [Google Scholar] [CrossRef]
- Chen, N.; Qian, J.; Chen, J.; Yu, X.; Mei, C.; Hao, C.; Jiang, G.; Lin, H.; Zhang, X.; Zuo, L.; et al. Phase 2 studies of oral hypoxiainducible factor prolyl hydroxylase inhibitor FG-4592 for treatment of anemia in China. Nephrol. Dial. Transplant. 2017, 32, 1373–1386. [Google Scholar] [CrossRef] [PubMed]
- Riopel, M.; Moon, J.; Bandyopadhyay, G.; You, S.; Lam, K.; Liu, X.; Kisseleva, T.; Brenner, D.; Lee, S. Inhibition of prolyl hydroxylases increases hepatic insulin and decreases glucagon sensitivity by an HIF-2a-dependent mechanism. Mol. Metab. 2020, 41, 101039. [Google Scholar] [CrossRef] [PubMed]
- Rahtu-Korpela, L.; Karsikas, S.; Horkko, S.; Sequeiros, R.; Lammentausa, E.; Makela, K.; Herzig, K.; Walkinshaw, G.; Kivirikko, K.; Myllyharju, J.; et al. HIF Prolyl 4-Hydroxylase-2 Inhibition Improves Glucose and Lipid Metabolism and Protects Against Obesity and Metabolic Dysfunction. Diabetes 2014, 63, 3324–3333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dallas, A.; Trotsyuk, A.; Ilves, H.; Bonham, C.; Rodrigues, M.; Engel, K.; Barrera, J.; Kosaric, N.; Stern-Buchbnder, Z.; White, A.; et al. Acceleration of Diabetic Wound Healing with PHD2- and miR-210-Targeting Oligonucleotides. Tissue Eng. 2019, 25, 44–54. [Google Scholar] [CrossRef] [PubMed]
- Laitakari, A.; Tapio, J.; Makela, K.; Herzig, K.; Dengler, F.; Gylling, H.; Walkinshaw, G.; Myllyharju, J.; Dimova, E.; Serpi, R.; et al. HIF-P4H-2 inhibition enhances intestinal fructose metabolism and induces thermogenesis protecting against NAFLD. J. Mol. Med. 2020, 98, 719–731. [Google Scholar] [CrossRef] [Green Version]
- Saito, H.; Tanaka, T.; Sugahara, M.; Tanaka, S.; Fukui, K.; Wakashima, T.; Nangaku, M. Inhibition of prolyl hydroxylase domain (PHD) by JTZ-951 reduces obesity-related diseases in the liver, white adipose tissue, and kidney in mice with a high-fat diet. Lab. Investig. 2019, 99, 1217–1232. [Google Scholar] [CrossRef] [PubMed]
- Sofue, T.; Nakagawa, N.; Kanda, E.; Nagasu, H.; Matsushita, K.; Nangaku, M.; Maruyama, S.; Wada, T.; Terada, Y.; Yamagata, K.; et al. Prevalence of anemia in patients with chronic kidney disease in Japan: A nationwide, cross-sectional cohort study using data from the Japan Chronic Kidney Disease Database (JCKD-DB). PLoS ONE 2020, 15, e0236132. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| NCT | Patients | Basal Hb (g/dg/dL) | S/R/C | Effect—Change Hemoglobin Level (g/dg/dL) | Adverse Events (%) | Serious Adverse Events (%) | Reference |
|---|---|---|---|---|---|---|---|
| 01599507 | NDD/Placebo | <10.0 | 156/91/82 | After 8 weeks: Low dose roxa—1.82+/−0.21 High dose roxa—2.59+/−0.26 Placebo—0.65+/−0.13 | Roxa—59 Placebo—63 | Roxa—13.1 Placebo—13.3 | [9] |
| 00761657 | NDD/Placebo | NDD treated roxa: | 293/88/28 | After 6 weeks therapy: | Roxa—59.1 Placebo—59.1 | Roxa—5 Placebo—4 | [13] |
| 0.7 mg/kg—10.3 | 0.7 mg/kg—+0.4 | ||||||
| 1.0 mg/kg—10.4 | 1.0 mg/kg—+0.4 | ||||||
| 1.5 mg/kg—10.3 | 1.5 mg/kg—+1.2 | ||||||
| 2.0 mg/kg—10.3 | 2.0 mg/kg—+1.8 | ||||||
| Placebo—10.3 | Placebo—0.1 | ||||||
| 01244763 | NDD | <10.5 | 357/145 | After 16(A and B) and after 24 weeks roxa therapy: A (1 mg/kg)—1.71+/−0.21 B (1.7 mh/kg)—1.09+/−0.21 C 50 mg—0.57+/−0.21 D 100 mg—1.53+/−0.20 E 70/100/150—0.77+/−0.20 F 70 mg—0.61+/−0.20 | 80.0 | 24.1 | [11] |
| 01964196 | NDD/Placebo | <10.0 | 190/80/27 | After 6 weeks. Rate of rise (g/dg/dL/week) compare to placebo | Placebo 70.4 | Placebo 7.4 | [21] |
| Roxa 50 mg/TIW—+0.254 | Roxa 50 mg/TIW—74.1 | Roxa 50 mg/TI—22.2 | |||||
| Roxa 70 g/TIW—+0.508 | Roxa 70 mg/TIW—88.5 | Roxa 70 mg/TIW—0 | |||||
| Roxa 100 g/TIW—+0.623 | Roxa 100 mg/TIW—74.1 | Roxa 100 mg/TIW—74.1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grzeszczak, W.; Szczyra, D.; Śnit, M. Whether Prolyl Hydroxylase Blocker—Roxadustat—In the Treatment of Anemia in Patients with Chronic Kidney Disease Is the Future? Int. J. Environ. Res. Public Health 2021, 18, 1612. https://doi.org/10.3390/ijerph18041612
Grzeszczak W, Szczyra D, Śnit M. Whether Prolyl Hydroxylase Blocker—Roxadustat—In the Treatment of Anemia in Patients with Chronic Kidney Disease Is the Future? International Journal of Environmental Research and Public Health. 2021; 18(4):1612. https://doi.org/10.3390/ijerph18041612
Chicago/Turabian StyleGrzeszczak, Władysław, Dariusz Szczyra, and Mirosław Śnit. 2021. "Whether Prolyl Hydroxylase Blocker—Roxadustat—In the Treatment of Anemia in Patients with Chronic Kidney Disease Is the Future?" International Journal of Environmental Research and Public Health 18, no. 4: 1612. https://doi.org/10.3390/ijerph18041612
APA StyleGrzeszczak, W., Szczyra, D., & Śnit, M. (2021). Whether Prolyl Hydroxylase Blocker—Roxadustat—In the Treatment of Anemia in Patients with Chronic Kidney Disease Is the Future? International Journal of Environmental Research and Public Health, 18(4), 1612. https://doi.org/10.3390/ijerph18041612