
Development and Evaluation of an Online Education-Entertainment Intervention to Increase Knowledge of HIV and Uptake of HIV Testing among Colombian Men Who Have Sex with Men (MSM)

 , , , , , and
, , , , , and
Abstract
:1. Introduction
Development of an Education-Entertainment Online Video Intervention Using CBPR
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Measures
2.3.1. Acceptability Measures
2.3.2. Efficacy Measures
2.4. Data Analysis
3. Results
3.1. Characteristics of the Baseline Sample (N = 300)
3.2. Randomization and Attrition Analyses
3.3. Acceptability of the Intervention (n = 63)
3.4. Preliminary Efficacy of the Intervention (n = 95)
3.4.1. Recent HIV Testing
3.4.2. HIV-Testing Intentions
3.4.3. HIV Knowledge
3.4.4. Exploratory Moderation Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ministerio de Salud y Proteccion Social; United Nations Population Fund. Comportamiento Sexual y Prevalencia De VIH en Hombres Que Tienen Relaciones Sexuales Con Hombres en Siete Ciudades de Colombia. 2011. Available online: https://www.minsalud.gov.co/salud/Documents/observatorio_vih/documentos/monitoreo_evaluacion/2_evaluacion_respuesta/b_estudios_complementarios/Resultados_Estudio_HSH_final125.pdf (accessed on 20 November 2020).
- Zea, M.C.; Reisen, C.A.; del Río-González, A.M.; Bianchi, F.T.; Ramirez-Valles, J.; Poppen, P.J. HIV Prevalence and Awareness of Positive Serostatus Among Men Who Have Sex With Men and Transgender Women in Bogotá, Colombia. Am. J. Public Health 2015, 105, 1588–1595. [Google Scholar] [CrossRef]
- Reisen, C.A.; Zea, M.C.; Bianchi, F.T.; Poppen, P.J.; del Río-González, A.M.; Aguayo Romero, R.A.; Perez, C. HIV Testing Among MSM in Bogotá, Colombia: The Role of Structural and Individual Characteristics. AIDS Educ. Prev. 2014, 26, 328–344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldman, D.P.; Juday, T.; Seekins, D.; Linthicum, M.T.; Romley, J.A. Early HIV Treatment in the United States Prevented Nearly 13,500 Infections per Year During 1996–2009. Health Aff. (Millwood) 2014, 33, 362–369. [Google Scholar] [CrossRef] [PubMed]
- Romley, J.A.; Juday, T.; Solomon, M.D.; Seekins, D.; Brookmeyer, R.; Goldman, D.P. Early HIV Treatment Led to Life Expectancy Gains Valued at $80 Billion for People Infected in 1996–2009. Health Aff. (Millwood) 2014, 33, 370–377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saag, M.S.; Benson, C.A.; Gandhi, R.T.; Hoy, J.F.; Landovitz, R.J.; Mugavero, M.J.; Sax, P.E.; Smith, D.M.; Thompson, M.A.; Buchbinder, S.P.; et al. Antiretroviral Drugs for Treatment and Prevention of HIV Infection in Adults: 2018 Recommendations of the International Antiviral Society–USA Panel. JAMA 2018, 320, 379–396. [Google Scholar] [CrossRef] [PubMed]
- Andaló, P. Love, Tears, Betrayal... and Health Messages. Perspect. Health Mag. Mag. Pan Am. Health Organ 2003, 8, 8–13. [Google Scholar]
- Sanchez, N.; Sandoval, H.; Siegmeth, T.; Galvez, G.; Rios-Ellis, B. Telenovelas impact on the public health arena and implications for public health messaging and sustainability. In Proceedings of the 141st APHA Annual Meeting, Boston, MA, USA, 2–6 November 2013. Paper number 284192. [Google Scholar]
- Whittier, D.K.; Kennedy, M.G.; St. Lawrence, J.S.; Seeley, S.; Beck, V. Embedding Health Messages into Entertainment Television: Effect on Gay Men’s Response to a Syphilis Outbreak. J. Health Commun. 2005, 10, 251–259. [Google Scholar] [CrossRef] [PubMed]
- Wilkin, H.A.; Valente, T.W.; Murphy, S.; Cody, M.J.; Huang, G.; Beck, V. Does Entertainment-Education Work With Latinos in the United States? Identification and the Effects of a Telenovela Breast Cancer Storyline. J. Health Commun. 2007, 12, 455–469. [Google Scholar] [CrossRef]
- Garcia, J.; Perez-Brumer, A.G.; Cabello, R.; Clark, J.L. “And Then Break the Cliché”: Understanding and Addressing HIV Vulnerability Through Development of an HIV Prevention Telenovela with Men Who Have Sex with Men and Transwomen in Lima, Peru. Arch. Sex. Behav. 2018, 47, 1995–2005. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singhal, A.; Rogers, E.M. The status of entertainment-education worldwide. In Entertainment-Education and Social Change: History, Research, and Practice; Singhal, A., Cody, M.J., Rogers, E.M., Sabido, M., Eds.; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 2004; pp. 3–20. [Google Scholar]
- Barker, K.; Connolly, S.; Angelone, C. Creating a brighter future in Rwanda through entertainment education. Crit. Arts 2013, 27, 75–90. [Google Scholar] [CrossRef]
- Cabassa, L.J.; Oh, H.; Humensky, J.L.; Unger, J.B.; Molina, G.B.; Baron, M. Comparing the Impact on Latinos of a Depression Brochure and an Entertainment-Education Depression Fotonovela. Psychiatr. Serv. 2015, 66, 313–316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jibaja-Weiss, M.L.; Volk, R.J.; Granchi, T.S.; Neff, N.E.; Robinson, E.K.; Spann, S.J.; Aoki, N.; Friedman, L.C.; Beck, J.R. Entertainment Education for Breast Cancer Surgery Decisions: A Randomized Trial among Patients with Low Health Literacy. Patient Educ. Couns. 2011, 84, 41–48. [Google Scholar] [CrossRef] [PubMed]
- Moyer-Gusé, E.; Nabi, R.L. Comparing the Effects of Entertainment and Educational Television Programming on Risky Sexual Behavior. Health Commun. 2011, 26, 416–426. [Google Scholar] [CrossRef] [PubMed]
- Tate, J. Laughing All the Way to Tolerance? Mexican Comedic Telenovelas as Vehicles for Lessons Against Homophobia. Latin Am. 2014, 58, 51–65. [Google Scholar] [CrossRef]
- Sabido, M. Evolution of the Sabido Methodology of “Entertainment-Education”. In Using the Media to Achieve Reproductive Health and Gender Equity; UNPFA: New York, NY, USA, 2011; pp. 12–19. Available online: populationmedia.org/wp-content/uploads/2012/02/UNFPA_Best_practices_ENG.pdf (accessed on 20 November 2020).
- Nguyen, L.H.; Tran, B.X.; Rocha, L.E.C.; Nguyen, H.L.T.; Yang, C.; Latkin, C.A.; Thorson, A.; Strömdahl, S. A Systematic Review of eHealth Interventions Addressing HIV/STI Prevention Among Men Who Have Sex With Men. AIDS Behav. 2019, 23, 2253–2272. [Google Scholar] [CrossRef] [Green Version]
- Lau, J.T.F.; Lee, A.L.; Tse, W.S.; Mo, P.K.H.; Fong, F.; Wang, Z.; Cameron, L.D.; Sheer, V. A randomized control trial for evaluating efficacies of two online cognitive interventions with and without fear-appeal imagery approaches in preventing unprotected anal sex among Chinese men who have sex with men. AIDS Behav. 2016, 20, 1851–1862. [Google Scholar] [CrossRef]
- Wang, Z.; Lau, J.T.F.; Ip, M.; Ho, S.P.Y.; Mo, P.K.H.; Latkin, C.; Ma, Y.L.; Kim, Y. A Randomized Controlled Trial Evaluating Efficacy of Promoting a Home-Based HIV Self-Testing with Online Counseling on Increasing HIV Testing Among Men Who Have Sex with Men. AIDS Behav. 2018, 22, 190–201. [Google Scholar] [CrossRef] [PubMed]
- Tang, W.; Han, L.; Best, J.; Zhang, Y.; Mollan, K.; Kim, J.; Liu, F.; Hudgens, M.; Bayus, B.; Terris-Prestholt, F.; et al. Crowdsourcing HIV Test Promotion Videos: A Noninferiority Randomized Controlled Trial in China. Clin. Infect. Dis. 2016, 62, 1436–1442. [Google Scholar] [CrossRef]
- Chiasson, M.A.; Shaw, F.S.; Humberstone, M.; Hirshfield, S.; Hartel, D. Increased HIV disclosure three months after an online video intervention for men who have sex with men (MSM). AIDS Care 2009, 21, 1081–1089. [Google Scholar] [CrossRef] [PubMed]
- Hirshfield, S.; Chiasson, M.A.; Joseph, H.; Scheinmann, R.; Johnson, W.D.; Remien, R.H.; Shaw, F.S.; Emmons, R.; Yu, G.; Margolis, A.D. An online randomized controlled trial evaluating HIV prevention digital media interventions for men who have sex with men. PLoS ONE 2012, 7, e46252. [Google Scholar] [CrossRef] [Green Version]
- Starks, T.J.; Dellucci, T.V.; Gupta, S.; Robles, G.; Stephenson, R.; Sullivan, P.S.; Parsons, J.T. A Pilot Randomized Trial of Intervention Components Addressing Drug Use in Couples HIV Testing and Counseling (CHTC) with Male Couples. AIDS Behav. 2019, 23, 2407–2420. [Google Scholar] [CrossRef]
- Blas, M.M.; Alva, I.E.; Carcamo, C.P.; Cabello, R.; Goodreau, S.M.; Kimball, A.M.; Kurth, A.E. Effect of an online video-based intervention to increase HIV testing in men who have sex with men in Peru. PLoS ONE 2010, 5, e10448. [Google Scholar] [CrossRef]
- Tremblay, M.C.; Martin, D.H.; Macaulay, A.C.; Pluye, P. Can we Build on Social Movement Theories to Develop and Improve Community-Based Participatory Research? A Framework Synthesis Review. Am. J. Community Psychol. 2017, 59, 333–362. [Google Scholar] [CrossRef] [Green Version]
- Rhodes, S.D.; Daniel, J.; Alonzo, J.; Duck, S.; García, M.; Downs, M.; Hergenrather, K.C.; Alegría-Ortega, J.; Miller, C.; Allen, A.B.; et al. A Systematic Community-Based Participatory Approach to Refining an Evidence-Based Community-Level Intervention: The HOLA Intervention for Latino Men Who Have Sex With Men. Health Promot. Pract. 2013, 14, 607–616. [Google Scholar] [CrossRef] [PubMed]
- Soul City Institute. Edutainment: Using Stories & Media for Social Action and Behaviour Change. 2013. Available online: https://www.soulcity.org.za/resources/materials/edutainment/edutainment (accessed on 20 November 2020).
- Heckathorn, D.D. Respondent-Driven Sampling: A New Approach to the Study of Hidden Populations. Soc. Probl. 1997, 44, 174–199. [Google Scholar] [CrossRef]
- Heckathorn, D.D. Respondent-Driven Sampling II: Deriving Valid Population Estimates from Chain-Referral Samples of Hidden Populations. Soc. Probl. 2002, 49, 11–34. [Google Scholar] [CrossRef]
- Ramirez-Valles, J.; Heckathorn, D.D.; Vázquez, R.; Diaz, R.M.; Campbell, R.T. From Networks to Populations: The Development and Application of Respondent-Driven Sampling Among IDUs and Latino Gay Men. AIDS Behav. 2005, 9, 387–402. [Google Scholar] [CrossRef] [PubMed]
- Niederdeppe, J.; Kim, H.K.; Lundell, H.; Fazili, F.; Frazier, B. Beyond Counterarguing: Simple Elaboration, Complex Integration, and Counterelaboration in Response to Variations in Narrative Focus and Sidedness. J. Commun. 2012, 62, 758–777. [Google Scholar] [CrossRef]
- Igartua, J.-J.; Vega Casanova, J. Identification With Characters, Elaboration, and Counterarguing in Entertainment-Education Interventions Through Audiovisual Fiction. J. Health Commun. 2016, 21, 293–300. [Google Scholar] [CrossRef] [PubMed]
- Arrivillaga, M.; Hoyos, P.A.; Tovar, L.M.; Varela, M.T.; Correa, D.; Zapata, H. HIV Testing and Counselling in Colombia: Evidence from a National Health Survey and Recommendations for Health-care Services. Int. J. STD AIDS 2012, 23, 815–821. [Google Scholar] [CrossRef]
- Lundgren, J.D.; Borges, A.H.; Neaton, J.D. Serious Non-AIDS Conditions in HIV: Benefit of Early ART. Curr. HIV/AIDS Rep. 2018, 15, 162–171. [Google Scholar] [CrossRef]
- Yombi, J.C.; Jonckheere, S.; Vincent, A.; Wilmes, D.; Vandercam, B.; Belkhir, L. Late Presentation for Human Immunodeficiency Virus HIV Diagnosis: Results of a Belgian Single Centre. Acta Clin. Belg. 2014, 69, 33–39. [Google Scholar] [CrossRef] [PubMed]
- The Temprano ANRS 12136 Study Group. A Trial of Early Antiretrovirals and Isoniazid Preventive Therapy in Africa. N. Engl. J. Med. 2015, 373, 808–822. [Google Scholar] [CrossRef] [Green Version]
- The INSIGHT START Study Group. Initiation of Antiretroviral Therapy in Early Asymptomatic HIV Infection. N. Engl. J. Med. 2015, 373, 795–807. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ministerio de la Protección Social. Cobertura de Servicios de Salud y la Obligatoriedad para la Realización de las Pruebas Diagnósticas y Confirmatorias para VIH (Circular No. 0063). 2006. Available online: https://www.minsalud.gov.co/sites/rid/Lists/BibliotecaDigital/RIDE/DE/DIJ/Circular_0063_de_2006.pdf (accessed on 5 December 2020).
- Ramirez-Valles, J.; Fergus, S.; Reisen, C.A.; Poppen, P.J.; Zea, M.C. Confronting Stigma: Community Involvement and Psychological Well-Being Among HIV-Positive Latino Gay Men. Hisp. J. Behav. Sci. 2005, 27, 101–119. [Google Scholar] [CrossRef]
- Diaz, R.M.; Ayala, G. Love, passion and rebellion: Ideologies of HIV risk among Latino gay men in the USA. Cult. Health Sex. 1999, 1, 277–293. [Google Scholar] [CrossRef]
- Parker, R.G.; Perez-Brumer, A.; Garcia, J.; Gavigan, K.; Ramirez, A.; Milnor, J.; Terto, V., Jr. Prevention literacy: Community-based advocacy for access and ownership of the HIV prevention toolkit. J. Int. AIDS Soc. 2016, 19, 21092. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Major Activity | Specific Objectives | Significant Results/Key Outcomes |
|---|---|---|
| Step 1: Background Research on the Target Population, the Message Topic, and the Communication Environment. | ||
| Three in-person CBPR team meetings. | To share our previous research findings in Colombia with the edu-entertainment team. To carry out new formative research on the target population and the message topic to inform the webnovela message. To find a common ground with CBPR regarding communication for social and behavioral change. To understand the communication environment in Colombia. | Formative research to inform the webnovela development and message. |
| Two focus groups with young MSM (n = 15). | To enrich formative research findings and assess current knowledge, attitudes, practices and social norms among young MSM regarding sexual life, HIV, HIV testing and communication. | Input for Message Brief. |
| Step 2: Development of the Message Brief. | ||
| Message brief workshop (CBPR team and PI). | Based on formative research, to identify the crucial messages to bring about the desired changes in the target community. | Draft of Message Brief. |
| Two focus groups with young MSM (n = 15) & Key-informant interviews (N = 5) | Obtain feedback on the clarity and suitability of the Message Brief. | Feedback for Message Brief. |
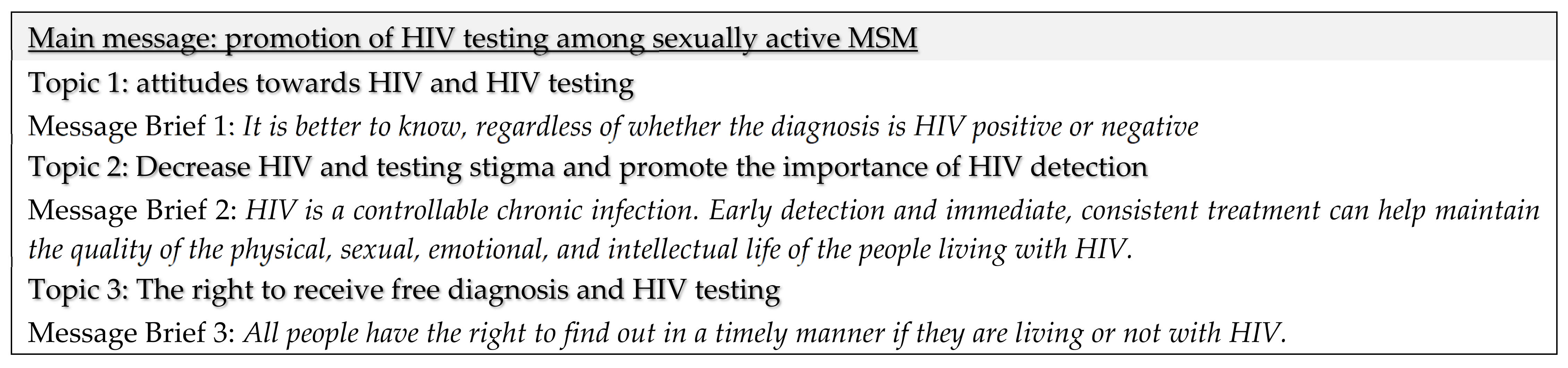
| Message brief adjustment workshop (CBPR team and PI). | Examine feedback from focus groups and key-informant interviews, and revise the Message Brief accordingly. | Final Message Brief (See Figure 1). |
| Step 3: Development of broad story outline and characters. | ||
| Recruitment of Creative team | Identify Producer, Director, Assistant Director and scriptwriters for film and production. | Creative team. |
| Creative workshop I (CBPR, PI, and Creative teams). | Discuss possible characters, setting, plot, and actions. | Findings were used for development of Draft Story Outline. |
| Creative team meetings. | Integrate the Message Brief into a drama, achieving the appropriate balance between entertainment and education. | Draft Story Outline. |
| Creative workshop II (CBPR, PI, and Creative teams). | Create the arc of the story and characters. Discuss Draft Story Outline and revise accordingly. | |
| Three focus groups with young MSM (n = 30)/Key informants interviews (N = 5). | Obtain feedback on the story, characters, and messages in the Draft Story Outline. Validation of the universe, treatment and summary of 13 chapters. | Feedback for Story Outline. |
| Creative workshop III (CBPR, PI, and Creative teams). | Examine feedback and determine aspects that need further changes. | Final Story Outline. |
| Step 4: Development of the script. | ||
| Draft script (Creative team). | Based on final story outline, develop detailed story lines, character sketches, scripts, and scenes | Draft Script. |
| Three focus groups with young MSM (n = 51)/Key informants interviews (N = 5). | Obtain feedback on draft scripts | |
| Creative workshop III (CBPR, PI, and Creative teams). | Identify areas in need of modification and make recommendations to the creative team to revise the story lines, characters, and scripts. | Final Script. |
| Step 5: Production. | ||
| Casting and hiring of production and direction teams | Pre-production | |
| Three focus groups with young MSM (n = 40) | Provide feedback on casting and final scripts. | |
| Filming and editing | Finalize product | Decision to use a feature film format, rather than a webnovela with 5 episodes. Final version of “Bondage It is better to know”. |
| Characteristic | Baseline Survey (N = 300) % (95% CI) | Post-Viewing Acceptability Survey (n = 63) % (95% CI) | Follow-Up Survey (n = 95) | |
|---|---|---|---|---|
| Intervention Group (n = 48) % (95% CI) | Control Group (n = 47) % (95% CI) | |||
| Age (Mean ± SD) | 23.18 ± 3.40 | 22.65 ± 3.32 | 22.29 ± 3.12 | 21.85 ± 3.01 |
| Gender identity a | ||||
| Cisgender men | 95.0 (91.9–97.2) | 98.4 (91.5–100) | 100 (92.6–100) | 93.6 (82.5–98.7) |
| Transgender women | 3.7 (1.8–6.5) | 1.6 (0.0–8.5) | 0.0 (0.0–7.4) | 4.3 (0.5–14.5) |
| Transgender men | 1.3 (0.4–3.4) | 0.0 (0.0–5.7) | 0.0 (0.0–7.4) | 2.1 (0.1–11.3) |
| Sexual orientation | ||||
| Gay | 66.3 (60.7–71.7) | 96.8 (57.0–80.8) | 77.1 (62.7–88.0) | 44.7 (30.2–59.9) |
| Bisexual | 26.3 (21.4–31.7) | 22.2 (12.7–34.5) | 16.7 (7.5–30.2) | 40.4 (26.4–55.7) |
| Heterosexual | 4.3 (2.3–7.3) | 7.9 (2.6–17.6) | 6.3 (1.3–17.2) | 12.8 (4.8–25.7) |
| Don’t know | 3.0 (1.4–5.6) | 0.0 (0.0–5.7) | 0.0 (0.0–7.4) | 2.1 (0.1–11.3) |
| Socio-economic strata b | ||||
| Low | 37.8 (32.1–43.8) | 32.3 (20.9–45.3) | 39.6 (25.8–54.7) | 43.2 (28.3–59.0) |
| Medium | 60.0 (53.9–65.8) | 67.7 (54.7–79.1) | 60.4 (45.3–74.2) | 56.8 (41.0–71.7) |
| High | 2.2 (0.8–4.7) | 0.0 (0.0–5.8) | 0.0 (0.0–7.4) | 0.0 (0.0–8.0) |
| Education | ||||
| Less than high school | 6.3 (3.9–9.7) | 0.0 (0.0–5.7) | 0.0 (0.0–7.4) | 6.4 (1.3–17.5) |
| High school | 20.7 (16.2–25.7) | 15.9 (7.9–27.3) | 16.7 (7.5–30.2) | 21.3 (10.7–35.7) |
| Some college | 52.7 (46.8–58.4) | 63.5 (50.4–75.3) | 60.4 (45.3–74.2) | 57.4 (42.2–71.7) |
| College or more | 20.3 (15.9–25.3) | 20.6 (11.5–32.7) | 22.9 (12.0–37.3) | 14.9 (6.2–28.3) |
| Self-reported HIV status (At each time point) | ||||
| Positive | 8.3 (5.5–12.1) | 7.9 (2.6–17.6) | 12.5 (4.7–25.2) | 4.3 (0.5–14.5) |
| Negative | 62.3 (56.6–67.8) | 61.9 (48.8–73.9) | 43.8 (29.5–58.8) | 42.6 (28.3–57.8) |
| Unknown | 29.3 (24.2–34.8) | 30.2 (19.2–43.0) | 43.8 (29.5–58.8) | 53.2 (38.1–67.9) |
| Scale/Item | Mean | SD | Range | α |
|---|---|---|---|---|
| How much did you enjoy Bondage? | 3.79 | 1.02 | 1–5 | |
| How informative did you find Bondage? | 4.21 | 0.94 | 1–5 | |
| How much do you think your MSM friends would enjoy the film Bondage? | 3.81 | 1.13 | 1–5 | |
| Would you recommend Bondage to a friend? | 2.54 | 0.64 | 1–3 | |
| Narrative engagement | 3.47 | 0.73 | 1.3–4.9 | 0.83 |
| Sometimes it was hard for me to understand what was going on in the film (Rev) | 3.45 | 1.14 | 1–5 | |
| Sometimes my mind wandered while I was watching the film (Rev) | 3.37 | 1.28 | 1–5 | |
| During the film, my body was in the room but my mind was in the world created by the story. | 3.24 | 1.18 | 1–5 | |
| The story affected me emotionally | 2.81 | 1.16 | 1–5 | |
| I felt sorry for some of the film characters | 3.53 | 1.16 | 1–5 | |
| I felt the whole time that I wanted to know how the story would end | 3.92 | 1.01 | 1–5 | |
| The story’s events are relevant for my daily life | 3.18 | 1.17 | 1–5 | |
| I could picture myself in the events shown in the film | 3.48 | 1.24 | 1–5 | |
| I reflected on the topics covered in the film | 4.06 | 0.99 | 1–5 | |
| I thought about the situations and motivations of the characters | 3.68 | 1.08 | 1–5 | |
| Counterarguing | 2.62 | 0.96 | 1–4.75 | 0.76 |
| I felt like criticizing my disagreement with what was happening or was being said | 2.79 | 1.23 | 1–5 | |
| I thought that the information on some topics was imprecise or wrong | 1.90 | 1.20 | 1–5 | |
| I considered different ways in which the story could have been different | 3.23 | 1.31 | 1–5 | |
| I tried to identify problems with the information around some topics | 2.55 | 1.28 | 1–5 | |
| Identification with the main character (Gabriel) | 3.43 | 1.10 | 1–5 | 0.88 |
| I felt as if I were GABRIEL | 2.92 | 1.51 | 1–5 | |
| I imagined how I would act if I were in GABRIEL’s place | 3.79 | 1.37 | 1–5 | |
| I worried about what was happening to GABRIEL | 3.56 | 1.20 | 1–5 | |
| I understood GABRIEL’s feelings or emotions | 3.66 | 1.25 | 1–5 | |
| I tried to see things from GABRIEL’s perspective | 3.61 | 1.24 | 1–5 | |
| I identified with GABRIEL | 3.07 | 1.48 | 1–5 |
| Characteristic | Baseline Survey e (N = 300) Mean ± SD/ % (95% CI) | Post-Viewing Acceptability Survey (n = 63) Mean ± SD/ % (95% CI) | Follow-Up Survey (n = 95) | |
|---|---|---|---|---|
| Intervention Group (n = 48) Mean ± SD/ % (95% CI) | Control Group (n = 47) Mean ± SD/ % (95% CI) | |||
| HIV Testing a (% [95% CI]) | ||||
| Yes | 74.7 (69.3–79.5) | 79.3 (66.6–88.8) | 56.3 (41.2–70.5) | 46.8 (29.5–58.8) |
| No | 25.3 (20.5–30.7) | 20.7 (11.2–33.4) | 43.8 (32.1–61.9) | 53.2 (38.1–67.9) |
| HIV testing intentions b (Mean ± SD) | 4.32 ± 0.89 | 4.19 ± 0.91 | 4.46 ± 0.61 | 4.41 ± 1.03 |
| I plan to get an HIV test within the next 6 months | 4.33 ± 0.97 | 4.20 ± 0.96 | 4.50 ± 0.67 | 4.42 ± 1.05 |
| From now on, I plan to get tested for HIV on a regular basis | 4.32 ± 0.95 | 4.18 ± 0.94 | 4.42 ± 0.63 | 4.40 ± 1.05 |
| Knowledge about HIV transmission dynamics c (Mean ± SD) | 2.45 ± 1.29 | 3.27 ± 1.26 | 3.40 ± 1.14 | 2.96 ± 1.32 |
| There is a medication that, when taken properly, reduces HIV levels in blood and semen [True] | 0.36 ± 0.48 | 0.58 ± 0.49 | 0.66 ± 0.47 | 0.51 ± 0.50 |
| It is possible to know if a person is infected with HIV from how he/she looks (his/her appearance) [False] | 0.54 ± 0.49 | 0.72 ± 0.44 | 0.66 ± 0.47 | 0.57 ± 0.49 |
| A person can be infected with HIV and not have AIDS [True] | 0.61 ± 0.48 | 0.83 ± 0.37 | 0.83 ± 0.37 | 0.70 ± 0.46 |
| If a person has HIV but gets treatment on time he/she can live a normal life with a normal life span [True] | 0.78 ± 0.41 | 0.91 ± 0.27 | 0.91 ± 0.27 | 0.87 ± 0.33 |
| When a person living with HIV has an undetectable viral load, he can still transmit HIV to another person [False] | 0.14 ± 0.35 | 0.20 ± 0.41 | 0.31 ± 0.46 | 0.29 ± 0.46 |
| Knowledge about HIV-related rights d (Mean ± SD) | 2.71 ± 1.06 | 3.11 ± 1.14 | 3.14 ± 0.87 | 2.85 ± 0.97 |
| All Colombian citizens have the right to get treatment for HIV/AIDS [True] | 0.80 ± 0.39 | 0.77 ± 0.42 | 0.79 ± 0.41 | 0.80 ± 0.39 |
| Employers can demand their employees to get tested for HIV before hiring them [False] | 0.37 ± 0.48 | 0.59 ± 0.49 | 0.62 ± 0.48 | 0.36 ± 0.48 |
| HIV test results should be confidential [True] | 0.84 ± 0.36 | 0.88 ± 0.31 | 0.95 ± 0.20 | 0.87 ± 0.33 |
| By law, health-providing organizations must approve HIV tests, up to twice per year, to any member who requests it [True] | 0.70 ± 0.45 | 0.85 ± 0.35 | 0.77 ± 0.42 | 0.80 ± 0.39 |
| Outcome Variable | Time-Point | Group | |
|---|---|---|---|
| Intervention (n = 48) Mean (SD) | Control (n = 47) Mean (SD) | ||
| Recent HIV testing a | Baseline | 0.48 (0.50) | 0.43 (0.50) |
| Follow-up | 0.56 (0.50) | 0.47 (0.50) | |
| HIV testing intentions b | Baseline | 4.33 (0.93) | 4.41 (0.65) |
| Follow-up | 4.46 (0.62) | 4.41 (1.03) | |
| Knowledge of HIV transm. Dynamics c | Baseline | 2.88 (1.25) | 2.23 (1.17) |
| Follow-up | 3.40 (1.14) | 2.96 (1.32) | |
| Knowledge of HIV-related rights d | Baseline | 2.75 (1.16) | 2.70 (0.86) |
| Follow-up | 3.15 (0.88) | 2.85 (0.98) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
del Río-González, A.M.; Zea, M.C.; Calabrese, S.K.; Betancourt, F.; Pacheco-Cabrales, J.; Estrada-Santiago, Y.; Poppen, P.J. Development and Evaluation of an Online Education-Entertainment Intervention to Increase Knowledge of HIV and Uptake of HIV Testing among Colombian Men Who Have Sex with Men (MSM). Int. J. Environ. Res. Public Health 2021, 18, 1811. https://doi.org/10.3390/ijerph18041811
del Río-González AM, Zea MC, Calabrese SK, Betancourt F, Pacheco-Cabrales J, Estrada-Santiago Y, Poppen PJ. Development and Evaluation of an Online Education-Entertainment Intervention to Increase Knowledge of HIV and Uptake of HIV Testing among Colombian Men Who Have Sex with Men (MSM). International Journal of Environmental Research and Public Health. 2021; 18(4):1811. https://doi.org/10.3390/ijerph18041811
Chicago/Turabian Styledel Río-González, Ana María, Maria Cecilia Zea, Sarah K. Calabrese, Fabián Betancourt, Jorge Pacheco-Cabrales, Yacid Estrada-Santiago, and Paul J. Poppen. 2021. "Development and Evaluation of an Online Education-Entertainment Intervention to Increase Knowledge of HIV and Uptake of HIV Testing among Colombian Men Who Have Sex with Men (MSM)" International Journal of Environmental Research and Public Health 18, no. 4: 1811. https://doi.org/10.3390/ijerph18041811
APA Styledel Río-González, A. M., Zea, M. C., Calabrese, S. K., Betancourt, F., Pacheco-Cabrales, J., Estrada-Santiago, Y., & Poppen, P. J. (2021). Development and Evaluation of an Online Education-Entertainment Intervention to Increase Knowledge of HIV and Uptake of HIV Testing among Colombian Men Who Have Sex with Men (MSM). International Journal of Environmental Research and Public Health, 18(4), 1811. https://doi.org/10.3390/ijerph18041811