
Maternal Food and Beverage Consumption Behaviors and Discrepant Phthalate Exposure by Race

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Maternal Urinary Phthalates Analysis
2.3. Study Questionnaire and Covariate Data
2.4. Statistical Analysis
3. Results
3.1. Study Population
3.2. Maternal Urinary Phthalate Concentrations
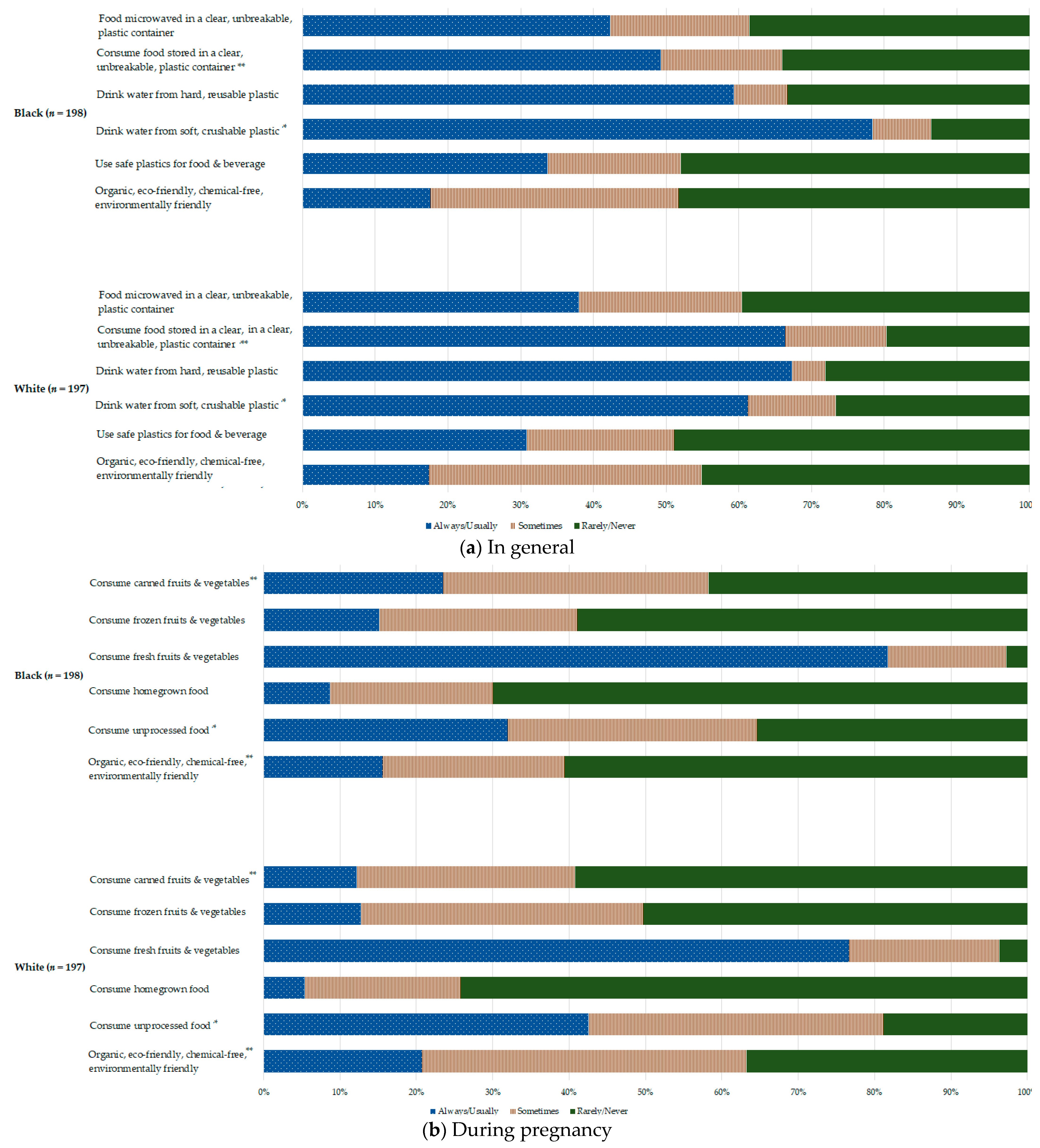
3.3. Food and Beverage Consumption Habits
3.4. Urinary Phthalates Associated with Food and Beverage Consumption Behaviors
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- CDC. Fourth National Report on Human Exposure to Environmental Chemicals-Updated Tables, January 2019; U.S. Centers for Disease Control and Prevention: Atlanta, GA, USA, 2019.
- Silva, M.J.; Reidy, J.A.; Herbert, A.R.; Preau, J.L.; Needham, L.L.; Calafat, A.M. Detection of Phthalate Metabolites in Human Amniotic Fluid. Bull. Environ. Contam. Toxicol. 2004, 72, 1226–1231. [Google Scholar] [CrossRef]
- Gore, A.C.; Chappell, V.A.; Fenton, S.E.; Flaws, J.A.; Nadal, A.; Prins, G.S.; Toppari, J.; Zoeller, R.T. EDC-2: The Endocrine Society’s Second Scientific Statement on Endocrine-Disrupting Chemicals. Endocr. Rev. 2015, 36, E1–E150. [Google Scholar] [CrossRef]
- Kay, V.R.; Bloom, M.S.; Foster, W.G. Reproductive and developmental effects of phthalate diesters in males. Crit. Rev. Toxicol. 2014, 44, 467–498. [Google Scholar] [CrossRef]
- Serrano, S.E.; Braun, J.; Trasande, L.; Dills, R.; Sathyanarayana, S. Phthalates and diet: A review of the food monitoring and epidemiology data. Environ. Health 2014, 13, 43. [Google Scholar] [CrossRef] [Green Version]
- Colacino, J.A.; Harris, T.R.; Schecter, A. Dietary Intake Is Associated with Phthalate Body Burden in a Nationally Representative Sample. Environ. Health Perspect. 2010, 118, 998–1003. [Google Scholar] [CrossRef]
- Zota, A.R.; Calafat, A.M.; Woodruff, T.J. Temporal Trends in Phthalate Exposures: Findings from the National Health and Nutrition Examination Survey, 2001–2010. Environ. Health Perspect. 2014, 122, 235–241. [Google Scholar] [CrossRef] [Green Version]
- Branch, F.; Woodruff, T.J.; Mitro, S.D.; Zota, A.R. Vaginal douching and racial/ethnic disparities in phthalates exposures among reproductive-aged women: National Health and Nutrition Examination Survey 2001–2004. Environ. Health 2015, 14, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Duty, S.M.; Ackerman, R.M.; Calafat, A.M.; Hauser, R. Personal Care Product Use Predicts Urinary Concentrations of Some Phthalate Monoesters. Environ. Health Perspect. 2005, 113, 1530–1535. [Google Scholar] [CrossRef] [Green Version]
- Parlett, L.E.; Calafat, A.M.; Swan, S.H. Women’s exposure to phthalates in relation to use of personal care products. J. Expo. Sci. Environ. Epidemiol. 2012, 23, 197–206. [Google Scholar] [CrossRef]
- Van Tongeren, M.; Nieuwenhuijsen, M.J.; Gardiner, K.; Armstrong, B.; Vrijheid, M.; Dolk, H.; Botting, B. A Job–Exposure Matrix for Potential Endocrine-disrupting Chemicals Developed for a Study into the Association between Maternal Occupational Exposure and Hypospadias. Ann. Occup. Hyg. 2002, 46, 465–477. [Google Scholar] [CrossRef]
- Marie, C.; Vendittelli, F.; Sauvant-Rochat, M.-P. Obstetrical outcomes and biomarkers to assess exposure to phthalates: A review. Environ. Int. 2015, 83, 116–136. [Google Scholar] [CrossRef]
- Pollard, S.H.; Porucznik, C.A. Impact of Periconceptional Exposure to Phthalates on Pregnancy, Birth, and Neonatal Outcomes. Curr. Epidemiol. Rep. 2017, 124, 119–210. [Google Scholar] [CrossRef]
- Swan, S.H.; Main, K.M.; Liu, F.; Stewart, S.L.; Kruse, R.L.; Calafat, A.M.; Mao, C.S.; Redmon, J.B.; Ternand, C.L.; Sullivan, S.; et al. Decrease in Anogenital Distance among Male Infants with Prenatal Phthalate Exposure. Environ. Health Perspect. 2005, 113, 1056–1061. [Google Scholar] [CrossRef] [Green Version]
- Ferguson, K.K.; McElrath, T.F.; Meeker, J.D. Environmental Phthalate Exposure and Preterm Birth. JAMA Pediatr. 2014, 168, 61–67. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Lin, L.; Cao, Y.; Chen, B.; Zheng, L.; Ge, R.-S. Phthalate Levels and Low Birth Weight: A Nested Case-Control Study of Chinese Newborns. J. Pediatr. 2009, 155, 500–504. [Google Scholar] [CrossRef]
- Engel, S.M.; Miodovnik, A.; Canfield, R.L.; Zhu, C.; Silva, M.J.; Calafat, A.M.; Wolff, M.S. Prenatal Phthalate Exposure Is Associated with Childhood Behavior and Executive Functioning. Environ. Health Perspect. 2010, 118, 565–571. [Google Scholar] [CrossRef]
- Bloom, M.S.; Wenzel, A.G.; Brock, J.W.; Kucklick, J.R.; Wineland, R.J.; Cruze, L.; Unal, E.R.; Yucel, R.M.; Jiyessova, A.; Newman, R.B. Racial disparity in maternal phthalates exposure; Association with racial disparity in fetal growth and birth outcomes. Environ. Int. 2019, 127, 473–486. [Google Scholar] [CrossRef]
- Wineland, R.J.; Bloom, M.S.; Cruze, L.; Butts, C.D.; Wenzel, A.G.; Unal, E.R.; Kohno, S.; Willan, K.B.; Brock, J.W.; Newman, R.B. In utero effects of maternal phthalate exposure on male genital development. Prenat. Diagn. 2018, 39, 209–218. [Google Scholar] [CrossRef]
- Wenzel, A.G.; Bloom, M.S.; Butts, C.D.; Wineland, R.J.; Brock, J.W.; Cruze, L.; Unal, E.R.; Kucklick, J.R.; Somerville, S.E.; Newman, R.B. Influence of race on prenatal phthalate exposure and anogenital measurements among boys and girls. Environ. Int. 2018, 110, 61–70. [Google Scholar] [CrossRef]
- Wenzel, A.G.; Brock, J.W.; Cruze, L.; Newman, R.B.; Unal, E.R.; Wolf, B.J.; Somerville, S.E.; Kucklick, J.R. Prevalence and predictors of phthalate exposure in pregnant women in Charleston, SC. Chemosphere 2018, 193, 394–402. [Google Scholar] [CrossRef]
- James-Todd, T.M.; Chiu, Y.-H.; Zota, A.R. Racial/Ethnic Disparities in Environmental Endocrine Disrupting Chemicals and Women’s Reproductive Health Outcomes: Epidemiological Examples Across the Life Course. Curr. Epidemiol. Rep. 2016, 3, 161–180. [Google Scholar] [CrossRef] [Green Version]
- Helm, J.S.; Nishioka, M.; Brody, J.G.; Rudel, R.A.; Dodson, R.E. Measurement of endocrine disrupting and asthma-associated chemicals in hair products used by Black women. Environ. Res. 2018, 165, 448–458. [Google Scholar] [CrossRef]
- Polinski, K.J.; Dabelea, D.; Hamman, R.F.; Adgate, J.L.; Calafat, A.M.; Ye, X.; Starling, A.P. Distribution and predictors of urinary concentrations of phthalate metabolites and phenols among pregnant women in the Healthy Start Study. Environ. Res. 2018, 162, 308–317. [Google Scholar] [CrossRef]
- Calafat, A.M. Contemporary Issues in Exposure Assessment Using Biomonitoring. Curr. Epidemiol. Rep. 2016, 3, 145–153. [Google Scholar] [CrossRef] [Green Version]
- National Research Council Phthalates and Cumulative Risk Assessment. Phthalates and Cumulative Risk Assessment; National Academies Press: Washington, DC, USA, 2008. [Google Scholar] [CrossRef]
- Varshavsky, J.R.; Zota, A.R.; Woodruff, T.J. A Novel Method for Calculating Potency-Weighted Cumulative Phthalates Exposure with Implications for Identifying Racial/Ethnic Disparities among U.S. Reproductive-Aged Women in NHANES 2001–2012. Environ. Sci. Technol. 2016, 50, 10616–10624. [Google Scholar] [CrossRef] [Green Version]
- Boeniger, M.F.; Lowry, L.K.; Rosenberg, J. Interpretation of Urine Results Used to Assess Chemical Exposure with Emphasis on Creatinine Adjustments: A Review. Am. Ind. Hyg. Assoc. J. 1993, 54, 615–627. [Google Scholar] [CrossRef]
- Schisterman, E.F.; Vexler, A.; Whitcomb, B.W.; Liu, A. The Limitations due to Exposure Detection Limits for Regression Models. Am. J. Epidemiol. 2006, 163, 374–383. [Google Scholar] [CrossRef] [Green Version]
- Richardson, D.B. Effects of Exposure Measurement Error When an Exposure Variable Is Constrained by a Lower Limit. Am. J. Epidemiol. 2003, 157, 355–363. [Google Scholar] [CrossRef] [Green Version]
- Fasano, E.; Bono-Blay, F.; Cirillo, T.; Montuori, P.; Lacorte, S. Migration of phthalates, alkylphenols, bisphenol A and di(2-ethylhexyl)adipate from food packaging. Food Control. 2012, 27, 132–138. [Google Scholar] [CrossRef] [Green Version]
- McNeal, T.P.; Biles, J.E.; Begley, T.H.; Craun, J.C.; Hopper, M.L.; Sack, C.A. Determination of Suspected Endocrine Disruptors in Foods and Food Packaging. Anal. Environ. Endocr. Disrupt. 1999, 747, 33–52. [Google Scholar]
- Martino-Andrade, A.J.; Liu, F.; Sathyanarayana, S.; Barrett, E.S.; Redmon, J.B.; Nguyen, R.H.N.; Levine, H.; Swan, S.H. The TIDES Study Team Timing of prenatal phthalate exposure in relation to genital endpoints in male newborns. Andrology 2016, 4, 585–593. [Google Scholar] [CrossRef]
- Sathyanarayana, S.; Grady, R.; Barrett, E.S.; Redmon, B.; Nguyen, R.H.; Barthold, J.S.; Bush, N.R.; Swan, S.H. First trimester phthalate exposure and male newborn genital anomalies. Environ. Res. 2016, 151, 777–782. [Google Scholar] [CrossRef]
- Koo, H.J.; Lee, B.M. Estimated Exposure to Phthalates in Cosmetics and Risk Assessment. J. Toxicol. Environ. Health Part A 2004, 67, 1901–1914. [Google Scholar] [CrossRef]
- Pak, V.M.; McCauley, L.A. Risks of phthalate exposure among the general population: Implications for occupational health nurses. AAOHN J. 2007, 55, 12–17. [Google Scholar]
- Galobardes, B. Indicators of socioeconomic position (part 1). J. Epidemiol. Community Health 2006, 60, 7–12. [Google Scholar] [CrossRef] [Green Version]
- Buckley, J.P.; Doherty, B.T.; Keil, A.P.; Engel, S.M. Statistical Approaches for Estimating Sex-Specific Effects in Endocrine Disruptors Research. Environ. Health Perspect. 2017, 125, 067013. [Google Scholar] [CrossRef]
- Martínez, M.E.; Marshall, J.R.; Sechrest, L. Invited Commentary: Factor Analysis and the Search for Objectivity. Am. J. Epidemiol. 1998, 148, 17–19. [Google Scholar] [CrossRef] [Green Version]
- DiStefano, C.; Zhu, M.; Miîndrilaã, D. Understanding and Using Factor Scores: Considerations for the Applied Researcher. In Practical Assessment, Research, and Evaluation; 2009; Volume 14, ISSN 1531-7714. [Google Scholar]
- Woodruff, T.J.; Zota, A.R.; Schwartz, J.M. Environmental Chemicals in Pregnant Women in the United States: NHANES 2003–2004. Environ. Health Perspect. 2011, 119, 878–885. [Google Scholar] [CrossRef] [Green Version]
- Hoepner, L.A.; Whyatt, R.M.; Just, A.C.; Calafat, A.M.; Perera, F.P.; Rundle, A.G. Urinary concentrations of bisphenol A in an urban minority birth cohort in New York City, prenatal through age 7 years. Environ. Res. 2013, 122, 38–44. [Google Scholar] [CrossRef] [Green Version]
- Cantonwine, D.E.; Cordero, J.F.; Rivera-González, L.O.; Del Toro, L.V.A.; Ferguson, K.K.; Mukherjee, B.; Calafat, A.M.; Crespo, N.; Jiménez-Vélez, B.; Padilla, I.Y.; et al. Urinary phthalate metabolite concentrations among pregnant women in Northern Puerto Rico: Distribution, temporal variability, and predictors. Environ. Int. 2014, 62, 1–11. [Google Scholar] [CrossRef]
- Casas, L.; Fernández, M.F.; Llop, S.; Guxens, M.; Ballester, F.; Olea, N.; Irurzun, M.B.; Rodríguez, L.S.M.; Riaño, I.; Tardón, A.; et al. Urinary concentrations of phthalates and phenols in a population of Spanish pregnant women and children. Environ. Int. 2011, 37, 858–866. [Google Scholar] [CrossRef]
- De Renzy-Martin, K.T.; Frederiksen, H.; Christensen, J.S.; Kyhl, H.B.; Andersson, A.-M.; Husby, S.; Barington, T.; Main, K.M.; Jensen, T.K. Current exposure of 200 pregnant Danish women to phthalates, parabens and phenols. Reproduction 2014, 147, 443–453. [Google Scholar] [CrossRef] [Green Version]
- Lin, S.; Ku, H.-Y.; Su, P.-H.; Chen, J.-W.; Huang, P.-C.; Angerer, J.; Wang, S.-L. Phthalate exposure in pregnant women and their children in central Taiwan. Chemosphere 2011, 82, 947–955. [Google Scholar] [CrossRef]
- Rudel, R.A.; Gray, J.M.; Engel, C.L.; Rawsthorne, T.W.; Dodson, R.E.; Ackerman, J.M.; Rizzo, J.; Nudelman, J.L.; Brody, J.G. Food Packaging and Bisphenol A and Bis(2-Ethyhexyl) Phthalate Exposure: Findings from a Dietary Intervention. Environ. Health Perspect. 2011, 119, 914–920. [Google Scholar] [CrossRef]
- Kobrosly, R.W.; Parlett, L.E.; Stahlhut, R.W.; Barrett, E.S.; Swan, S.H. Socioeconomic factors and phthalate metabolite concentrations among United States women of reproductive age. Environ. Res. 2012, 115, 11–17. [Google Scholar] [CrossRef]
- Meeker, J.D.; Sathyanarayana, S.; Swan, S.H. Phthalates and other additives in plastics: Human exposure and associated health outcomes. Philos. Trans. R. Soc. B Biol. Sci. 2009, 364, 2097–2113. [Google Scholar] [CrossRef] [Green Version]
- Koch, H.M.; Lorber, M.; Christensen, K.L.; Pälmke, C.; Koslitz, S.; Brüning, T. Identifying sources of phthalate exposure with human biomonitoring: Results of a 48h fasting study with urine collection and personal activity patterns. Int. J. Hyg. Environ. Health 2013, 216, 672–681. [Google Scholar] [CrossRef]
- Martina, C.A.; Weiss, B.; Swan, S.H. Lifestyle behaviors associated with exposures to endocrine disruptors. NeuroToxicology 2012, 33, 1427–1433. [Google Scholar] [CrossRef] [Green Version]
- Pacyga, D.C.; Sathyanarayana, S.; Strakovsky, R.S. Dietary Predictors of Phthalate and Bisphenol Exposures in Pregnant Women. Adv. Nutr. 2019, 10, 803–815. [Google Scholar] [CrossRef]
- Sathyanarayana, S.; Alcedo, G.; Saelens, B.E.; Zhou, C.; Dills, R.L.; Yu, J.; Lanphear, B.P. Unexpected results in a randomized dietary trial to reduce phthalate and bisphenol A exposures. J. Expo. Sci. Environ. Epidemiol. 2013, 23, 378–384. [Google Scholar] [CrossRef]
- Chen, M.-L.; Chen, J.-S.; Tang, C.-L.; Mao, I.-F. The internal exposure of Taiwanese to phthalate—An evidence of intensive use of plastic materials. Environ. Int. 2008, 34, 79–85. [Google Scholar] [CrossRef]
- Serrano, S.E.; Karr, C.J.; Seixas, N.S.; Nguyen, R.H.N.; Barrett, E.S.; Janssen, S.; Redmon, B.; Swan, S.H.; Sathyanarayana, S. Dietary Phthalate Exposure in Pregnant Women and the Impact of Consumer Practices. Int. J. Environ. Res. Public Health 2014, 11, 6193–6215. [Google Scholar] [CrossRef] [Green Version]
- Koo, J.-W.; Parham, F.; Kohn, M.C.; Masten, S.A.; Brock, J.W.; Needham, L.L.; Portier, C.J. The association between biomarker-based exposure estimates for phthalates and demographic factors in a human reference population. Environ. Health Perspect. 2002, 110, 405–410. [Google Scholar] [CrossRef] [Green Version]
- Ford, C.L.; Airhihenbuwa, C.O. Critical Race Theory, Race Equity, and Public Health: Toward Antiracism Praxis. Am. J. Public Health 2010, 100, S30–S35. [Google Scholar] [CrossRef]
- Adamkiewicz, G.; Zota, A.R.; Fabian, M.P.; Chahine, T.; Julien, R.; Spengler, J.D.; Levy, J.I. Moving Environmental Justice Indoors: Understanding Structural Influences on Residential Exposure Patterns in Low-Income Communities. Am. J. Public Health 2011, 101, S238–S245. [Google Scholar] [CrossRef]
- Zota, A.R.; Shamasunder, B. The environmental injustice of beauty: Framing chemical exposures from beauty products as a health disparities concern. Am. J. Obstet. Gynecol. 2017, 217, 418.e1–418.e6. [Google Scholar] [CrossRef] [Green Version]
- Hauser, R.; Calafat, A. Phthalates and human health. Occup. Environ. Med. 2005, 62, 806–818. [Google Scholar] [CrossRef] [Green Version]
- James-Todd, T.M.; Meeker, J.D.; Huang, T.; Hauser, R.; Seely, E.W.; Ferguson, K.K.; Rich-Edwards, J.W.; McElrath, T.F. Racial and ethnic variations in phthalate metabolite concentration changes across full-term pregnancies. J. Expo. Sci. Environ. Epidemiol. 2017, 27, 160–166. [Google Scholar] [CrossRef] [Green Version]
- James-Todd, T.; Senie, R.; Terry, M.B. Racial/Ethnic Differences in Hormonally-Active Hair Product Use: A Plausible Risk Factor for Health Disparities. J. Immigr. Minor. Health 2011, 14, 506–511. [Google Scholar] [CrossRef]
- Kelley, K.E.; Hernández-Díaz, S.; Chaplin, E.L.; Hauser, R.; Mitchell, A.A. Identification of Phthalates in Medications and Dietary Supplement Formulations in the United States and Canada. Environ. Health Perspect. 2012, 120, 379–384. [Google Scholar] [CrossRef]
- Gao, H.; Zhu, Y.-D.; Xu, Y.-Y.; Zhang, Y.-W.; Yao, H.-Y.; Sheng, J.; Jin, Z.-X.; Ren, L.-L.; Huang, K.; Hao, J.-H.; et al. Season-dependent concentrations of urinary phthalate metabolites among Chinese pregnant women: Repeated measures analysis. Environ. Int. 2017, 104, 110–117. [Google Scholar] [CrossRef]
- Gibson, R.S.; Charrondiere, U.R.; Bell, W. Measurement Errors in Dietary Assessment Using Self-Reported 24-Hour Recalls in Low-Income Countries and Strategies for Their Prevention. Adv. Nutr. 2017, 8, 980–991. [Google Scholar] [CrossRef] [Green Version]
- Hays, S.M.; Aylward, L.L.; Blount, B.C. Variation in Urinary Flow Rates According to Demographic Characteristics and Body Mass Index in NHANES: Potential Confounding of Associations between Health Outcomes and Urinary Biomarker Concentrations. Environ. Health Perspect. 2015, 123, 293–300. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Characteristic | Overall (n = 395) | White (n = 197) | Black (n = 198) | p Value | |||
|---|---|---|---|---|---|---|---|
| Age, mean (SD) a | 27.4 | 5.6 | 29.0 | 5.2 | 25.9 | 5.6 | <0.0001 |
| BMI, mean (SD) b | 29.3 | 7.4 | 27.6 | 6.3 | 30.9 | 8.1 | <0.0001 |
| Education, n (%) c | <0.0001 | ||||||
| < High school | 41 | 11.0% | 12 | 6.4% | 29 | 15.7% | - |
| High school | 80 | 21.4% | 19 | 23.8% | 61 | 33.0% | - |
| Some college | 96 | 25.7% | 40 | 21.2% | 56 | 30.3% | - |
| Finish college | 101 | 27.0% | 73 | 38.6% | 28 | 15.1% | |
| Graduate work | 56 | 15.0% | 45 | 23.8% | 11 | 6.0% | - |
| Annual household income, n (%) d | <0.0001 | ||||||
| <$25k | 93 | 34.3% | 20 | 12.7% | 73 | 64.6% | - |
| $25k–$65k | 87 | 32.1% | 52 | 32.9% | 35 | 31.0% | - |
| >$65k | 91 | 33.4% | 86 | 54.4% | 5 | 4.4% | - |
| Marital status, n (%) e,f | <0.0001 | ||||||
| Married | 202 | 53.9% | 156 | 82.5% | 46 | 24.7% | - |
| Single | 173 | 46.1% | 33 | 17.5% | 140 | 75.3% | - |
| Job, n (%) g,h | 0.36 | ||||||
| High risk | 101 | 34.8% | 58 | 37.2% | 43 | 32.1% | - |
| Low risk | 189 | 65.2% | 98 | 62.8% | 91 | 67.9% | - |
| Housing, n(%) i | |||||||
| Detached single family home | 172 | 46.4% | 119 | 63.4% | 53 | 28.7% | <0.0001 |
| Attached single family home | 36 | 9.7% | 17 | 9.1% | 19 | 10.3% | - |
| Apartment | 107 | 28.8% | 25 | 13.4% | 82 | 44.3% | - |
| Mobile home/trailer | 36 | 9.7% | 17 | 9.1% | 19 | 10.3% | - |
| Condminium | 7 | 1.9% | 5 | 2.7% | 2 | 1.1% | - |
| Other | 13 | 3.5% | 3 | 1.6% | 10 | 5.4% | - |
| Season enrolled, n(%) j | |||||||
| Winter | 36 | 18.0% | 36 | 18.3% | 35 | 17.7% | 0.78 |
| Spring | 44 | 23.5% | 44 | 22.3% | 49 | 24.8% | - |
| Summer | 62 | 32.7% | 62 | 31.5% | 67 | 33.8% | - |
| Fall | 55 | 25.8% | 55 | 27.9% | 47 | 23.7% | - |
| Phthalate Metabolite | Overall (n = 380) | White (n = 193) | Black (n = 187) | p Value a |
|---|---|---|---|---|
| GM (95% CI) | GM (95% CI) | GM (95% CI) | ||
| MBP | 17.4 (16.0, 19.0) | 13.2 (11.7, 14.8) | 23.0 (20.4, 25.8) | <0.0001 |
| MiBP | 12.4 (11.3, 13.5) | 8.9 (7.9, 9.9) | 17.1 (15.2, 19.1) | <0.0001 |
| MBzP | 13.4 (11.9, 15.0) | 9.2 (7.7, 10.9) | 19.2 (16.7, 22.0) | <0.0001 |
| MEHP | 3.9 (3.5, 4.3) | 3.4 (2.9, 4.0) | 4.4 (3.8, 5.0) | 0.02 |
| MEOHP | 6.6 (6.1, 7.2) | 6.5 (5.8, 7.3) | 6.7 (6.0, 7.5) | 0.72 |
| MEHHP | 8.3 (7.6, 9.0) | 8.0 (7.1, 9.0) | 8.6 (7.6, 9.7) | 0.39 |
| MEP | 59.6 (51.6, 68.6) b | 39.5 (32.5, 47.8) | 90.4 (74.3, 109.9) b | <0.0001 b |
| MMP | 2.9 (2.5, 3.3) b | 2.1 (1.6, 2.7) | 3.8 (3.3, 4.3) b | <0.0001 b |
| ΣDEHP | 61.1 (56.4, 66.2) | 58.5 (52.3, 65.4) | 63.8 (56.8, 71.6) | 0.29 |
| ΣDBP | 133.5 (122.8, 145.1) | 97.9 (87.7, 109.1) | 183.5 (164.4, 204.9) | <0.0001 |
| ΣRPF | 41.7 (38.6, 45.0) b | 32.8 (29.4, 36.5) | 53.3 (48.1, 58.9) b | <0.0001 b |
| Phthalate Metabolite | PC Factor 1: | PC Factor 2: | PC Factor 3: | |||
|---|---|---|---|---|---|---|
| % Difference (95% CI) | p Value | % Difference (95% CI) | p Value | % Difference (95% CI) | p Value | |
| MBP | 0.50 (0.20, 1.01) | 0.01 | 1.01 (−1.00, 3.05) | 0.23 | −1.98 (−6.76, 3.05) | 0.37 |
| MiBP | 1.01 (1.01, 1.01) | <0.0001 | 1.01 (−0.10, 2.02) | 0.07 | −2.96 (−6.76, 2.02) | 0.22 |
| MBzP | 0.20 (−0.20, 1.01) | 0.26 | 1.01 (−1.00, 3.05) | 0.36 | −7.69 (−13.06, −1.98) | 0.01 |
| MEHP | 1.01 (1.01, 2.02) | <0.0001 | 2.02 (1.01, 3.05) | <0.0001 | 2.02 (−1.98, 6.18) | 0.41 |
| MEOHP | 1.02 (0.30, 1.01) | <0.0001 | 2.02 (1.01, 3.05) | <0.0001 | 0.40 (−3.92, 4.08) | 0.84 |
| MEHHP | 0.40 (0.10, 1.01) | 0.01 | 2.02 (1.01, 3.05) | <0.0001 | 1.01 (−3.92, 6.18) | 0.66 |
| MEP b | 3.05 (3.05, 4.08) | <0.0001 | 1.01 (−2.96, 5.13) | 0.75 | −10.42 (−19.75, −0.30) | 0.04 |
| MMP b | 0.40 (0.10, 1.01) | 0.01 | 0.50 (−1.00, 2.02) | 0.58 | −4.88 (−9.52, 1.01) | 0.09 |
| ∑DEHP | 2.02 (1.01, 3.05) | <0.0001 | 5.13 (3.05, 7.25) | <0.0001 | 2.02 (−4.88, 9.42) | 0.57 |
| ∑DBP | 1.01 (0.40, 1.01) | <0.0001 | 1.01 (−0.40, 2.02) | 0.17 | −2.96 (−7.69, 2.02) | 0.21 |
| ΣRPF b | 1.01 (1.01, 1.01) | <0.0001 | 2.02 (0.03, 3.05) | 0.05 | −1.98 (−5.82, 2.02) | 0.35 |
| Phthalate Metabolite | PC Factor 1: | PC Factor 2: | PC Factor 3: | |||
|---|---|---|---|---|---|---|
| % Difference (95% CI) | p Value | % DiFference (95% CI) | p Value | % Difference (95% CI) | p Value | |
| MBP | −1.00 (−1.00, 0.00) | 0.05 | 5.13 (1.01, 8.33) | 0.01 | 2.02 (−1.00, 5.13) | 0.22 |
| MiBP | −1.00 (−1.00, −0.20) | 0.01 | 3.05 (−0.30, 6.18) | 0.07 | 1.01 (−2.96, 5.13) | 0.74 |
| MBzP | −0.10 (−2.96, 3.05) | 0.93 | 4.08 (−2.96, 10.52) | 0.24 | −1.98 (−6.76, 3.05) | 0.52 |
| MEHP | 1.01 (−1.98, 3.05) | 0.59 | −0.30 (−2.96, 2.02) | 0.83 | −3.92 (−6.76, −1.00) | 0.01 |
| MEOHP | 1.01 (−1.98, 3.05) | 0.68 | 0.00 (−2.96, 3.05) | 1.00 | −1.98 (−6.76, 2.02) | 0.34 |
| MEHHP | 1.01 (−1.98, 3.05) | 0.49 | −1.00 (−3.92, 2.02) | 0.48 | −2.96 (−6.76, 2.02) | 0.28 |
| MEP | −1.00 (−2.96, 1.01) | 0.48 | 5.13 (−3.92, 15.03) | 0.28 | −1.00 (−12.19, 11.63) | 0.88 |
| MMP | −1.98 (−3.92, −0.04) | 0.05 | 3.05 (−3.92, 10.52) | 0.36 | 3.05 (−2.96, 8.33) | 0.33 |
| ∑DEHP | 1.01 (−1.98, 5.13) | 0.56 | −1.00 (−4.88, 3.05) | 0.64 | −5.82 (−8.61, −1.98) | 0.01 |
| ∑DBP | −1.00 (−1.98, −0.30) | 0.01 | 5.13 (1.01, 9.42) | 0.01 | 2.02 (−1.98, 7.25) | 0.34 |
| ΣRPF | 0.10 (−1.00, 2.02) | 0.86 | 3.05 (−0.50, 6.18) | 0.10 | −1.00 (−4.88, 2.02) | 0.48 |
| Phthalate Metabolite | PC Factor 1: | PC Factor 2: | PC Factor 3: | |||
|---|---|---|---|---|---|---|
| % Difference (95% CI) | p Value | % Difference (95% CI) | p Value | % Difference (95% CI) | p Value | |
| MBP | 2.02 (−1.00, 5.13) | 0.29 | 0.30 (−2.96, 4.08) | 0.87 | 2.02 (−7.69, 12.75) | 0.70 |
| MiBP | 1.01 (0.30, 2.02) | 0.01 | 0.30 (−1.98, 3.05) | 0.81 | −2.96 (−11.31, 6.18) | 0.51 |
| MBzP | 1.01 (−1.00, 2.02) | 0.31 | −1.00 (−4.88, 3.05) | 0.67 | 5.13 (−4.88, 17.35) | 0.32 |
| MEHP | 1.01 (0.10, 3.05) | 0.03 | 2.02 (−0.10, 5.13) | 0.05 | −1.98 (−10.42, 6.18) | 0.60 |
| MEOHP | 1.01 (0.10, 1.01) | 0.03 | 2.02 (1.01, 4.08) | 0.01 | −1.00 (−8.61, 7.25) | 0.78 |
| MEHHP | 0.30 (−0.30, 1.01) | 0.32 | 3.05 (1.01, 5.13) | 0.01 | −1.98 (−10.42, 6.18) | 0.68 |
| MEP b | 4.08 (3.05, 6.18) | <0.0001 | −1.00 (−7.69, 6.18) | 0.81 | 15.03 (−4.88, 39.10) | 0.14 |
| MMP b | 0.50 (0.00, 1.01) | 0.05 | −1.00 (−2.96, 2.02) | 0.66 | 4.08 (−2.96, 12.75) | 0.25 |
| ∑DEHP | 1.01 (−0.10, 2.02) | 0.08 | 4.08 (1.01, 7.25) | 0.01 | −1.00 (−12.19, 11.63) | 0.86 |
| ∑DBP | 2.02 (−1.00, 4.08) | 0.17 | 0.30 (−2.96, 4.08) | 0.89 | 0.30 (−10.42, 11.63) | 0.95 |
| ΣRPF b | 2.02 (−0.20, 4.08) | 0.07 | 1.01 (−3.92, 6.18 | 0.64 | 2.02 (−7.69, 11.63) | 0.73 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sterrett, M.E.; Bloom, M.S.; Jamro, E.L.; Wenzel, A.G.; Wineland, R.J.; Unal, E.R.; Brock, J.; Kucklick, J.; Garcia, K.; Newman, R.B. Maternal Food and Beverage Consumption Behaviors and Discrepant Phthalate Exposure by Race. Int. J. Environ. Res. Public Health 2021, 18, 2190. https://doi.org/10.3390/ijerph18042190
Sterrett ME, Bloom MS, Jamro EL, Wenzel AG, Wineland RJ, Unal ER, Brock J, Kucklick J, Garcia K, Newman RB. Maternal Food and Beverage Consumption Behaviors and Discrepant Phthalate Exposure by Race. International Journal of Environmental Research and Public Health. 2021; 18(4):2190. https://doi.org/10.3390/ijerph18042190
Chicago/Turabian StyleSterrett, Mary E., Michael S. Bloom, Erica L. Jamro, Abby G. Wenzel, Rebecca J. Wineland, Elizabeth R. Unal, John Brock, John Kucklick, Kelly Garcia, and Roger B. Newman. 2021. "Maternal Food and Beverage Consumption Behaviors and Discrepant Phthalate Exposure by Race" International Journal of Environmental Research and Public Health 18, no. 4: 2190. https://doi.org/10.3390/ijerph18042190
APA StyleSterrett, M. E., Bloom, M. S., Jamro, E. L., Wenzel, A. G., Wineland, R. J., Unal, E. R., Brock, J., Kucklick, J., Garcia, K., & Newman, R. B. (2021). Maternal Food and Beverage Consumption Behaviors and Discrepant Phthalate Exposure by Race. International Journal of Environmental Research and Public Health, 18(4), 2190. https://doi.org/10.3390/ijerph18042190