
Mental Health among Adults during the COVID-19 Pandemic Lockdown: A Cross-Sectional Multi-Country Comparison

 , ,
, ,  ,
,  ,
,  ,
,  , ,
, ,  ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Survey Instrument
2.3. Procedures
2.4. Study Variables and Measures
2.5. Statistical Analysis
3. Results
3.1. Study Participants
3.2. Country-Level COVID-19 Factors and Personal COVID-19 Exposure
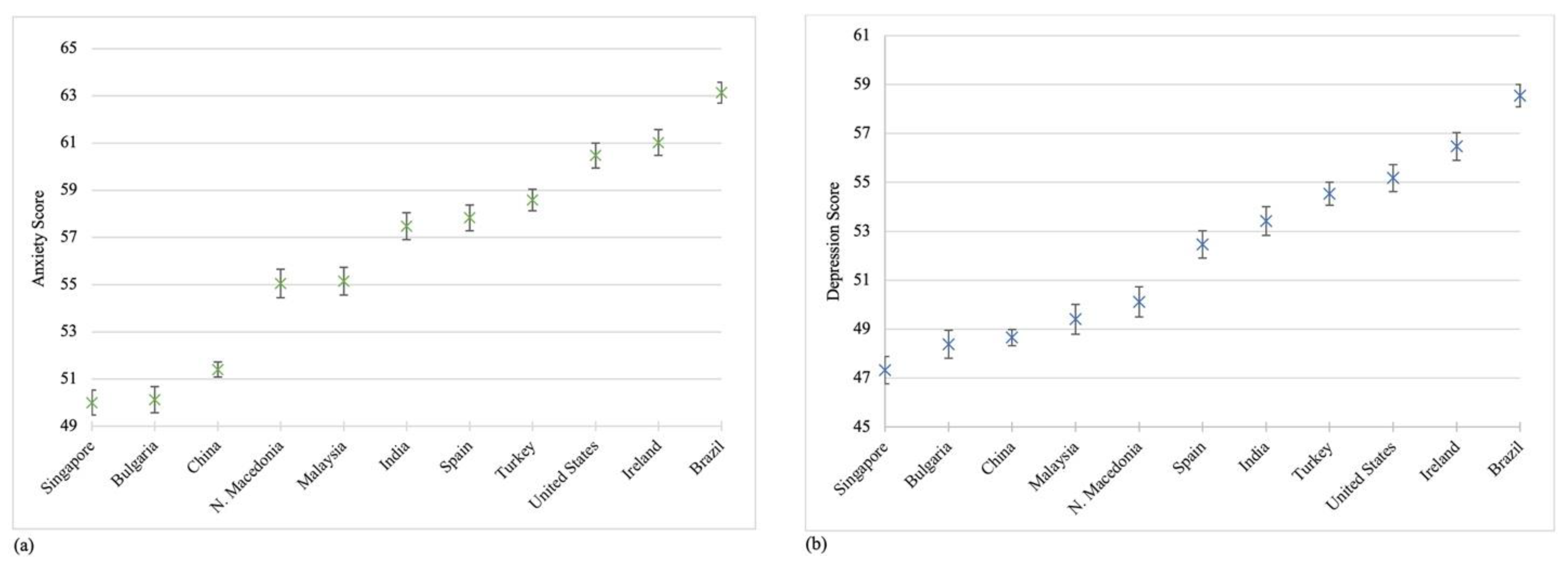
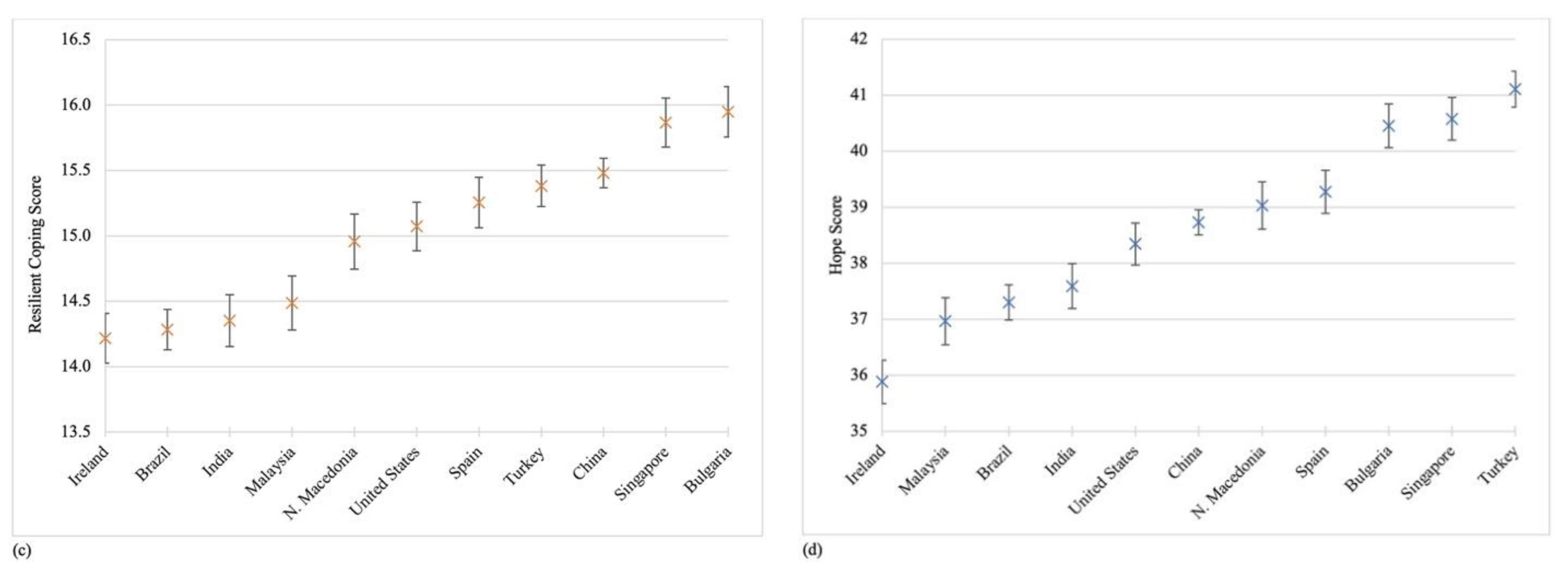
3.3. Mental Health across the 11 Countries
3.4. Associations of Country-Level COVID-19 Factors and Personal COVID-19 Exposure with Anxiety and Depression Symptoms
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Global Community Health–COVID-19 Collaborative Research Team
References
- Cucinotta, D.; Vanelli, M. WHO declares COVID-19 a pandemic. Acta BioMed. 2020, 91, 157–160. [Google Scholar] [PubMed]
- Anderson, R.M.; Heesterbeek, H.; Klinkenberg, D.; Hollingsworth, T.D. How will country-based mitigation measures influence the course of the COVID-19 epidemic? Lancet 2020, 395, 931–934. [Google Scholar] [CrossRef]
- Hsiang, S.; Allen, D.; Annan-Phan, S.; Bell, K.; Bolliger, I.; Chong, T.; Druckenmiller, H.; Huang, L.Y.; Hultgren, A.; Krasovich, E.; et al. The effect of large-scale anti-contagion policies on the COVID-19 pandemic. Nat. Cell Biol. 2020, 584, 262–267. [Google Scholar] [CrossRef] [PubMed]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [Green Version]
- Vindegaard, N.; Benros, M.E. COVID-19 pandemic and mental health consequences: Systematic review of the current evidence. Brain Behav. Immun. 2020, 89, 531–542. [Google Scholar] [CrossRef]
- Ahmad, A.; Mueller, C.; Tsamakis, K. COVID-19 pandemic: A public and global mental health opportunity for social transformation? BMJ 2020, 369, m1383. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ettman, C.K.; Abdalla, S.M.; Cohen, G.H.; Sampson, L.; Vivier, P.M.; Galea, S. Prevalence of depression symptoms in us adults before and during the COVID-19 pandemic. JAMA Netw. Open 2020, 3, e2019686. [Google Scholar] [CrossRef] [PubMed]
- Rossi, R.; Socci, V.; Talevi, D.; Mensi, S.; Niolu, C.; Pacitti, F.; Di Marco, A.; Rossi, A.; Siracusano, A.; Di Lorenzo, G. COVID-19 pandemic and lockdown measures impact on mental health among the general population in Italy. Front. Psychiatry 2020, 11, 790. [Google Scholar] [CrossRef]
- Benke, C.; Autenrieth, L.K.; Asselmann, E.; Pané-Farré, C.A. Lockdown, quarantine measures, and social distancing: Associations with depression, anxiety and distress at the beginning of the COVID-19 pandemic among adults from Germany. Psychiatry Res. 2020, 293, 113462. [Google Scholar] [CrossRef]
- Qiu, J.; Shen, B.; Zhao, M.; Wang, Z.; Xie, B.; Xu, Y. A nationwide survey of psychological distress among Chinese people in the COVID-19 epidemic: Implications and policy recommendations. Gen. Psychiatry 2020, 33, e100213. [Google Scholar] [CrossRef] [Green Version]
- Asmundson, G.J.; Taylor, S. Coronaphobia: Fear and the 2019-nCoV outbreak. J. Anxiety Disord. 2020, 70, 102196. [Google Scholar] [CrossRef]
- González-Sanguino, C.; Ausín, B.; Castellanos, M.; Ángel Saiz, J.; López-Gómez, A.; Ugidos, C.; Muñoz, M. Mental health consequences during the initial stage of the 2020 Coronavirus pandemic (COVID-19) in Spain. Brain Behav. Immun. 2020, 87, 172–176. [Google Scholar] [CrossRef]
- Tull, M.T.; Edmonds, K.A.; Scamaldo, K.M.; Richmond, J.R.; Rose, J.P.; Gratz, K.L. Psychological outcomes associated with stay-at-home orders and the perceived impact of COVID-19 on daily life. Psychiatry Res. 2020, 289, 113098. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; McIntyre, R.S.; Choo, F.N.; Tran, B.; Ho, R.; Sharma, V.K.; et al. A longitudinal study on the mental health of general population during the COVID-19 epidemic in China. Brain Behav. Immun. 2020, 87, 40–48. [Google Scholar] [CrossRef] [PubMed]
- Lai, J.; Ma, S.; Wang, Y.; Cai, Z.; Hu, J.; Wei, N.; Wu, J.; Du, H.; Chen, T.; Li, R.; et al. Factors associated with mental health outcomes among health care workers exposed to coronavirus disease 2019. JAMA Netw. Open 2020, 3, e203976. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Lu, H.; Zeng, H.; Zhang, S.; Du, Q.; Jiang, T.; Du, B. The differential psychological distress of populations affected by the COVID-19 pandemic. Brain Behav. Immun. 2020, 87, 49–50. [Google Scholar] [CrossRef]
- Pilkonis, P.A.; Choi, S.W.; Reise, S.P.; Stover, A.M.; Riley, W.T.; Cella, D. PROMIS Cooperative Group Item Banks for Measuring Emotional Distress From the Patient-Reported Outcomes Measurement Information System (PROMIS®): Depression, Anxiety, and Anger. Assessment 2011, 18, 263–283. [Google Scholar] [CrossRef] [PubMed]
- The PROMIS Health Organization. Obtain & Administer Measures. Available online: https://www.healthmeasures.net/index.php?option=com_content&view=category&layout=blog&id=71&Itemid=817 (accessed on 31 December 2020).
- Sinclair, V.G.; Wallston, K.A. The development and psychometric evaluation of the Brief Resilient Coping Scale. Assessment 2004, 11, 94–101. [Google Scholar] [CrossRef] [PubMed]
- Herth, K. Abbreviated instrument to measure hope: Development and psychometric evaluation. J. Adv. Nurs. 1992, 17, 1251–1259. [Google Scholar] [CrossRef]
- Our World in Data. COVID-19: Stringency Index. Available online: https://ourworldindata.org/grapher/covid-stringency-index (accessed on 31 December 2020).
- Our World in Data. Daily confirmed cases per million people. Available online: https://ourworldindata.org/covid-cases?country=IND~USA~GBR~CAN~DEU~FRA#daily-confirmed-cases-per-million-people (accessed on 31 December 2020).
- Merlo, J.; Yang, M.; Chaix, B.; Lynch, J.; Rastam, L. A brief conceptual tutorial on multilevel analysis in social epidemiology: Investigating contextual phenomena indifferent groups of people. J. Epidemiol. Community Health 2005, 59, 729–736. [Google Scholar] [CrossRef] [Green Version]
- Holmes, E.A.; O’Connor, R.C.; Perry, V.H.; Tracey, I.; Wessely, S.; Arseneault, L.; Ballard, C.; Christensen, H.; Silver, R.C.; Everall, I.; et al. Multidisciplinary research priorities for the COVID-19 pandemic: A call for action for mental health science. Lancet Psychiatry 2020, 7, 547–560. [Google Scholar] [CrossRef]
- World Health Organization. Depression and Other Common Mental Disorders: Global Health Estimates; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Lau, H.; Khosrawipour, V.; Kocbach, P.; Mikolajczyk, A.; Schubert, J.; Bania, J.; Khosrawipour, T. The positive impact of lockdown in Wuhan on containing the COVID-19 outbreak in China. J. Travel Med. 2020, 27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aquino, E.M.L.; Silveira, I.H.; Pescarini, J.M.; Aquino, R.; de Souza-Filho, J.A.; dos Santos Rocha, A.; Ferreira, A.; Victor, A.; Teixeira, C.; Pilecco, F.; et al. Social distancing measures to control the COVID-19 pan-demic: Potential impacts and challenges in Brazil. Cienc. Saude Coletiva 2020, 25 (Suppl. 1), 2423–2446. [Google Scholar] [CrossRef]
- Pung, R.; Chiew, C.J.; Young, B.E.; Chin, S.; Chen, M.I.; Clapham, H.E.; Cook, A.R.; Mark, T.M.; Lin, R.V.; Singapore 2019 Novel Coronavirus Outbreak Research Team; et al. Investigation of three clusters of COVID-19 in Singapore: Implications for surveillance and response measures. Lancet 2020, 395, 1039–1046. [Google Scholar] [CrossRef]
- U. S. Department of Health and Human Services. Mental Health: Culture, Race, and Ethnicity—A Supplement to Mental Health: A Report of the Surgeon General; Department of Health and Human Services, Substance Abuse and Mental Health Services Administration, Center for Mental Health Services: Rockville, MD, USA, 2001. [Google Scholar]
- Reger, M.A.; Stanley, I.H.; Joiner, T.E. Suicide mortality and coronavirus disease 2019—A perfect storm? JAMA Psychiatry 2020, 77, 1093–1094. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palgi, Y.; Shrira, A.; Ring, L.; Bodner, E.; Avidor, S.; Bergman, Y.; Cohen-Fridel, S.; Keisari, S.; Hoffman, Y. The loneliness pandemic: Loneliness and other concomitants of depression, anxiety and their comorbidity during the COVID-19 outbreak. J. Affect. Disord. 2020, 275, 109–111. [Google Scholar] [CrossRef]
- Chen, Q.; Liang, M.; Li, Y.; Guo, J.; Fei, D.; Wang, L.; He, L.; Sheng, C.; Cai, Y.; Li, X.; et al. Mental health care for medical staff in China during the COVID-19 outbreak. Lancet Psychiatry 2020, 7, e15–e16. [Google Scholar] [CrossRef]
- Shechter, A.; Diaz, F.; Moise, N.; Anstey, D.E.; Ye, S.; Agarwal, S.; Birk, J.L.; Brodie, D.; Cannone, D.E.; Chang, B.; et al. Psychological distress, coping behaviors, and preferences for support among New York healthcare workers during the COVID-19 pandemic. Gen. Hosp. Psychiatry 2020, 66, 1–8. [Google Scholar] [CrossRef]
- Hofmann, S.G.; Gómez, A.F. Mindfulness-based interventions for anxiety and depression. Psychiatr. Clin. N. Am. 2017, 40, 739–749. [Google Scholar] [CrossRef]
- Dominguez-Rodriguez, A.; De La Rosa-Gómez, A.; Hernández Jiménez, M.J.; Arenas-Landgrave, P.; Martínez-Luna, S.C.; Silva, J.A.; Acosta Guzmán, V.; Alvarez Silva, J.; García Hernándedz, J.; Arzola-Sánchez, C.; et al. A self-administered multicomponent web-based mental health intervention for the Mexican population during the COVID-19 pandemic: protocol for a randomized controlled trial. JMIR Res. Protoc. 2020, 16, e23117. [Google Scholar] [CrossRef] [PubMed]
- Valdez, D.; Thij, M.T.; Bathina, K.; A Rutter, L.; Bollen, J. Social media insights into US mental health during the COVID-19 pandemic: Longitudinal analysis of twitter data. J. Med. Internet Res. 2020, 22, e21418. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n | % | ||
|---|---|---|---|
| Country | |||
| China | 2850 | 21.5 | |
| Brazil | 1500 | 11.3 | |
| Turkey | 1400 | 10.6 | |
| United States | 1027 | 7.7 | |
| Singapore | 997 | 7.5 | |
| Spain | 981 | 7.4 | |
| Ireland | 980 | 7.4 | |
| Bulgaria | 952 | 7.2 | |
| India | 935 | 7.1 | |
| Malaysia | 831 | 6.3 | |
| North Macedonia | 810 | 6.1 | |
| Sex | |||
| Female | 8332 | 62.8 | |
| Male | 4801 | 36.2 | |
| Other | 130 | 1.0 | |
| Age a | |||
| 18–24 | 4072 | 30.7 | |
| 25–34 | 2785 | 21.0 | |
| 35–44 | 2624 | 19.8 | |
| 45–54 | 1949 | 14.7 | |
| 55–64 | 1195 | 9.0 | |
| 65 years or older | 625 | 4.7 | |
| Education a | |||
| Less than a high school degree | 873 | 6.6 | |
| High school degree | 2321 | 17.5 | |
| Associate degree | 2043 | 15.4 | |
| Bachelor’s degree | 4744 | 35.8 | |
| Graduate degree | 3258 | 24.6 | |
| Marital status | |||
| Single | 6465 | 48.7 | |
| Married | 5858 | 44.2 | |
| Other | 885 | 6.7 | |
| History of a mental disorder | |||
| Yes | 2022 | 15.3 | |
| No | 11,241 | 84.8 | |
| Number of people co-habiting during the lockdown a | |||
| 0 | 1891 | 14.3 | |
| 1 | 2351 | 17.8 | |
| 2 | 3252 | 24.6 | |
| 3 | 2941 | 22.2 | |
| 4+ | 2794 | 21.1 | |
| Employment and income changes since COVID-19 b | |||
| Employment changed and income decreased | 1135 | 8.6 | |
| Employment changed but no change in income | 559 | 4.2 | |
| No change in employment but income decreased | 2122 | 16.0 | |
| No changes in employment nor income | 4904 | 37.0 | |
| Other | 4543 | 34.3 | |
| Personal COVID-19 exposure c | |||
| Went out less than once a month | 1075 | 8.1 | |
| Went out at least once a month | 1351 | 10.2 | |
| Went out at least once a week | 5991 | 45.2 | |
| Had a contact with COVID-19 patient or had to quarantine for 14 days | 2939 | 22.2 | |
| Diagnosed with COVID-19 or experienced COVID-19 symptoms | 1907 | 14.4 |
| Governmental Policy Responses | Personal COVID-19 Exposure | Anxiety | Depression | Resilient Coping | Hope | ||
|---|---|---|---|---|---|---|---|
| Increase in confirmed cases per million people a | 0.087 ** | 0.175 ** | 0.311 ** | 0.255 ** | −0.068 ** | −0.048 | |
| Governmental policy response a | 0.030 ** | 0.152 ** | 0.135 ** | −0.099 ** | −0.121 | ||
| Personal COVID-19 exposure b | 0.144 ** | 0.132 ** | −0.021 * | −0.070 | |||
| Anxiety | 0.765 ** | −0.254 ** | −0.344 | ||||
| Depression | −0.307 ** | −0.449 | |||||
| Resilient coping | 0.601 | ||||||
| Anxiety | Depression | |||||
|---|---|---|---|---|---|---|
| Model 2 (n = 12,671) β (95%CI) | Model 3 (n = 12,583) β (95%CI) | Model 4 (n = 12,524) β (95%CI) | Model 2 (n = 12,951) β (95%CI) | Model 3 (n = 12,872) β (95%CI) | Model 4 (n = 12,824) β (95%CI) | |
| Country-level COVID-19 factors | ||||||
| Increase in confirmed cases per million people | 0.06 (0.00, 0.13) | 0.06(0.00, 0.12) * | 0.05 (0.00, 0.10) | 0.05 (0.00, 0.11) | 0.05(0.00, 0.10) | 0.04 (−0.01, 0.10) |
| Governmental policy response | 0.21 (−0.08, 0.51) | 0.16 (−0.09, 0.41) | 0.13 (−0.09, 0.36) | 0.17 (−0.09, 0.42) | 0.11 (−0.12, 0.34) | 0.07 (−0.16, 0.30) |
| Personal COVID-19 exposure | ||||||
| Went out less than once a month | Reference | Reference | Reference | Reference | Reference | Reference |
| Went out at least once a month | 0.41 (−0.26, 1.08) | 0.69 (0.09, 1.30) * | 0.59 (−0.01, 1.17) | 0.86 (0.15, 1.57) * | 1.34 (0.71, 1.97) ** | 1.40 (0.79, 2.01) ** |
| Went out at least once a week | 0.00 (−0.56, 0.55) | 0.57 (0.07, 1.07) * | 0.65 (0.15, 1.14) * | −0.16 (−0.75, 0.43) | 0.66 (0.14, 1.18) ** | 1.03 (0.52, 1.54) ** |
| Had contact with a COVID-19 patient or had to quarantine for14 days | 1.16 (0.57, 1.74) ** | 1.34 (0.81, 1.87) ** | 1.35 (0.83, 1.86) ** | 1.09 (0.47, 1.71) ** | 1.34 (0.80, 1.90) ** | 1.33 (0.79, 1.86) ** |
| Diagnosed with COVID-19 or experienced COVID-19 symptoms | 3.02 (2.37, 3.66) ** | 2.49 (1.91, 3.07) ** | 2.18 (1.61, 2.75) ** | 2.74 (2.06, 3.42) ** | 2.29 (1.69, 2.89) ** | 2.16 (1.57, 2.75) ** |
| Resilient coping | −0.15 (−0.20, −0.10) ** | −0.13 (−0.18, −0.08) ** | −0.06 (−0.11, 0.00) * | −0.03 (−0.09, 0.02) | ||
| Hope | −0.56 (−0.59, −0.54) ** | −0.54 (−0.57, −0.51) ** | −0.67 (−0.69, −0.64) ** | −0.61 (−0.64, −0.58) ** | ||
| Demographic variables | ||||||
| Sexa | ||||||
| Female | 2.31 (2.04, 2.58) ** | 1.81 (1.54, 2.09) ** | ||||
| Male | Reference | Reference | ||||
| Age | ||||||
| 18–24 | 2.78 (2.03, 3.53) ** | 3.33 (2.56, 4.10) ** | ||||
| 25–34 | 2.46 (1.76, 3.16) ** | 2.74 (2.01, 3.46) ** | ||||
| 35–44 | 1.95 (1.28, 2.62) ** | 1.96 (1.27, 2.66) ** | ||||
| 45–54 | 1.35 (0.67, 2.02) ** | 1.19 (0.49, 1.89) ** | ||||
| 55–64 | 0.82 (0.09, 1.54) * | 0.46 (−0.29, 1.21) | ||||
| 65 years or older | Reference | Reference | ||||
| Education | ||||||
| Less than a high school degree | Reference | Reference | ||||
| High school degree | −0.42 (−1.04, 0.21) | −0.88 (−1.52, −0.23) ** | ||||
| Associate degree | −0.45 (−1.05, 0.16) | −1.57 (−2.20, −0.94) ** | ||||
| Bachelor’s degree | 0.35 (−0.23, 0.92) | −1.07 (−1.66, −0.47) ** | ||||
| Graduate degree | 0.95 (0.33, 1.56) ** | −1.05 (−1.68, −0.42) ** | ||||
| Marital statusa | ||||||
| Single | −0.60 (−0.98, −0.23) ** | −0.04 (−0.43, 0.35) | ||||
| Married | Reference | Reference | ||||
| History of a mental disorder | ||||||
| Yes | 3.04 (2.66, 3.42) ** | 3.62 (3.22, 4.01) ** | ||||
| No | Reference | Reference | ||||
| Employment and income changes since COVID-19a,b | ||||||
| Employment changed and income decreased | 1.39 (0.91, 1.86) ** | 1.89 (1.40, 2.38) ** | ||||
| No change in employment but income decreased | 0.39 (0.01, 0.76) * | 0.87 (0.48, 1.26) ** | ||||
| Employment changed but no change in income | 0.77 (0.13, 1.41) * | 1.19 (0.53, 1.85) ** | ||||
| No changes in employment status nor income | Reference | Reference | ||||
| Number of people co-habiting during the lockdown | 0.33 (0.25, 0.42) ** | 0.10 (0.01, 0.19) * | ||||
| ICC b Country | 0.140 | 0.1299 | 0.1125 | 0.096 | 0.104 | 0.105 |
| AIC b | 89,000.8 | 85,665.1 | 84,456.0 | 92,701.8 | 88,861.0 | 87,683.4 |
| BIC b | 89,001.6 | 85,665.9 | 84,456.8 | 92,702.6 | 88,861.8 | 87,684.2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ding, K.; Yang, J.; Chin, M.-K.; Sullivan, L.; Demirhan, G.; Violant-Holz, V.; Uvinha, R.R.; Dai, J.; Xu, X.; Popeska, B.; et al. Mental Health among Adults during the COVID-19 Pandemic Lockdown: A Cross-Sectional Multi-Country Comparison. Int. J. Environ. Res. Public Health 2021, 18, 2686. https://doi.org/10.3390/ijerph18052686
Ding K, Yang J, Chin M-K, Sullivan L, Demirhan G, Violant-Holz V, Uvinha RR, Dai J, Xu X, Popeska B, et al. Mental Health among Adults during the COVID-19 Pandemic Lockdown: A Cross-Sectional Multi-Country Comparison. International Journal of Environmental Research and Public Health. 2021; 18(5):2686. https://doi.org/10.3390/ijerph18052686
Chicago/Turabian StyleDing, Kele, Jingzhen Yang, Ming-Kai Chin, Lindsay Sullivan, Giyasettin Demirhan, Veronica Violant-Holz, Ricardo R. Uvinha, Jianhui Dai, Xia Xu, Biljana Popeska, and et al. 2021. "Mental Health among Adults during the COVID-19 Pandemic Lockdown: A Cross-Sectional Multi-Country Comparison" International Journal of Environmental Research and Public Health 18, no. 5: 2686. https://doi.org/10.3390/ijerph18052686
APA StyleDing, K., Yang, J., Chin, M. -K., Sullivan, L., Demirhan, G., Violant-Holz, V., Uvinha, R. R., Dai, J., Xu, X., Popeska, B., Mladenova, Z., Khan, W., Kuan, G., Balasekaran, G., Smith, G. A., & on behalf of Global Community Health–COVID-19 Collaborative Research Team. (2021). Mental Health among Adults during the COVID-19 Pandemic Lockdown: A Cross-Sectional Multi-Country Comparison. International Journal of Environmental Research and Public Health, 18(5), 2686. https://doi.org/10.3390/ijerph18052686