
Reduction of Human Mobility Matters during Early COVID-19 Outbreaks: Evidence from India, Japan and China

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources
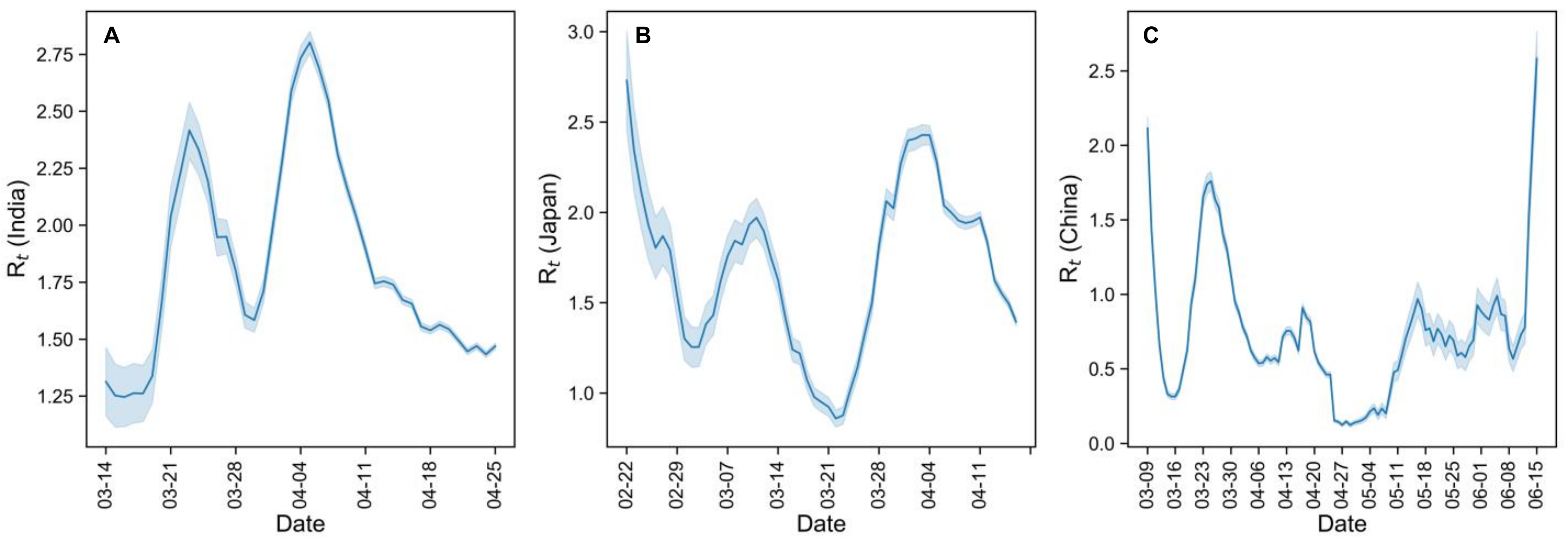
2.2. Estimation of Time-Varying Reproductive Number, Rt
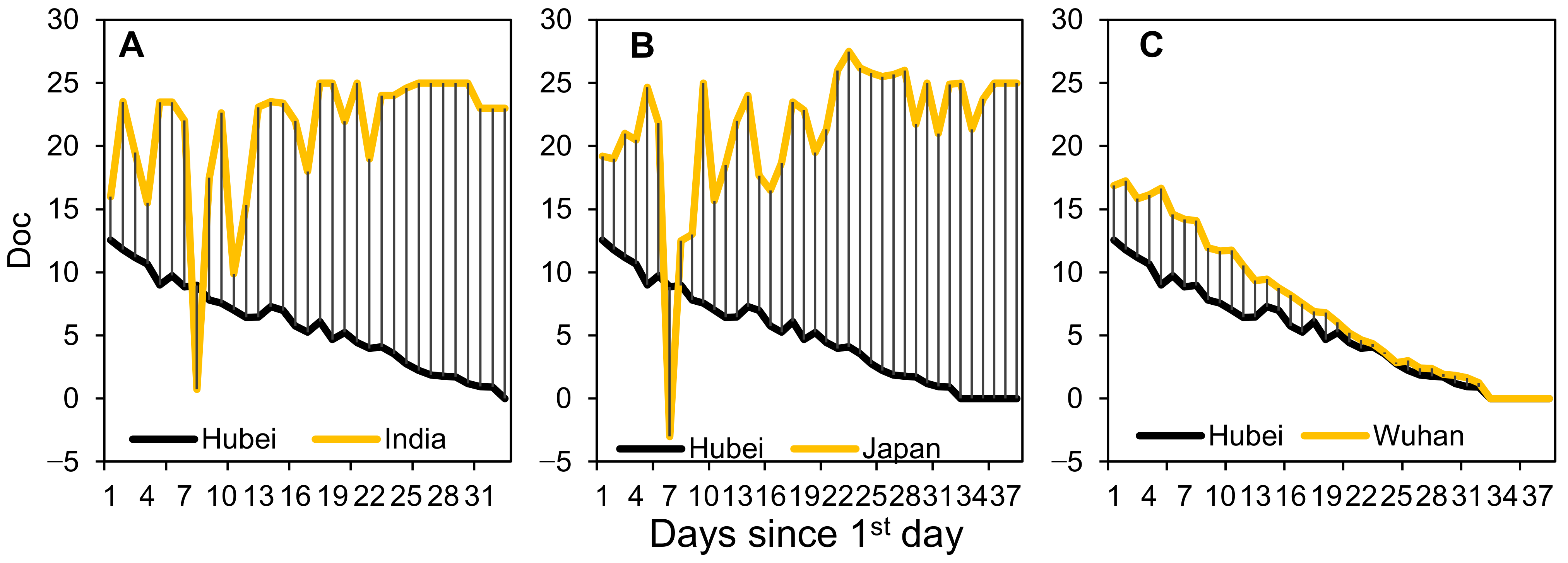
2.3. Estimation of Doc and Epidemic Curves by Illness Onset Date
2.4. Estimation of Bed Shortage
2.5. Critical Period for Imported Case Prevention
3. Results
3.1. Time-Varying Reproductive Number Rt and Doc
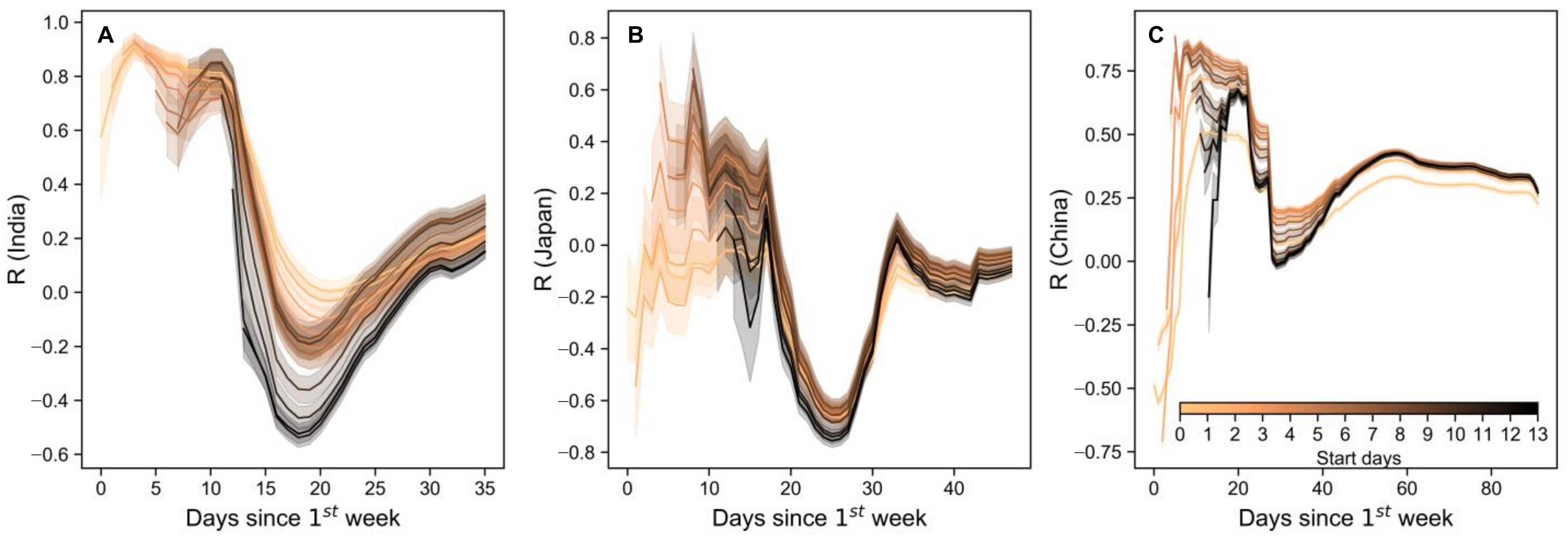
3.2. Critical Period for Controlling Imported Cases
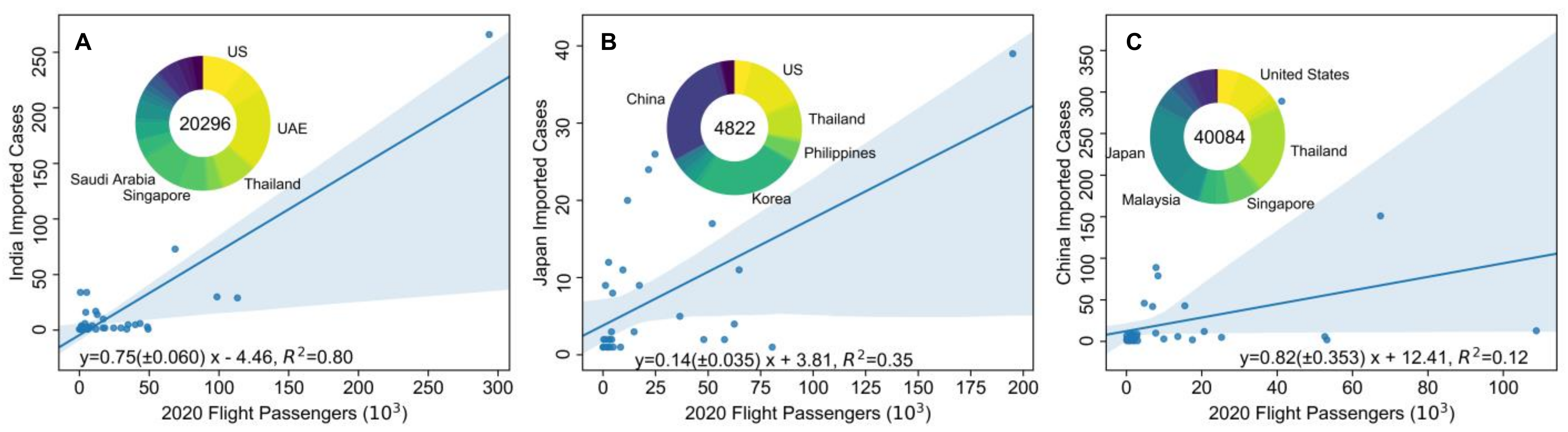
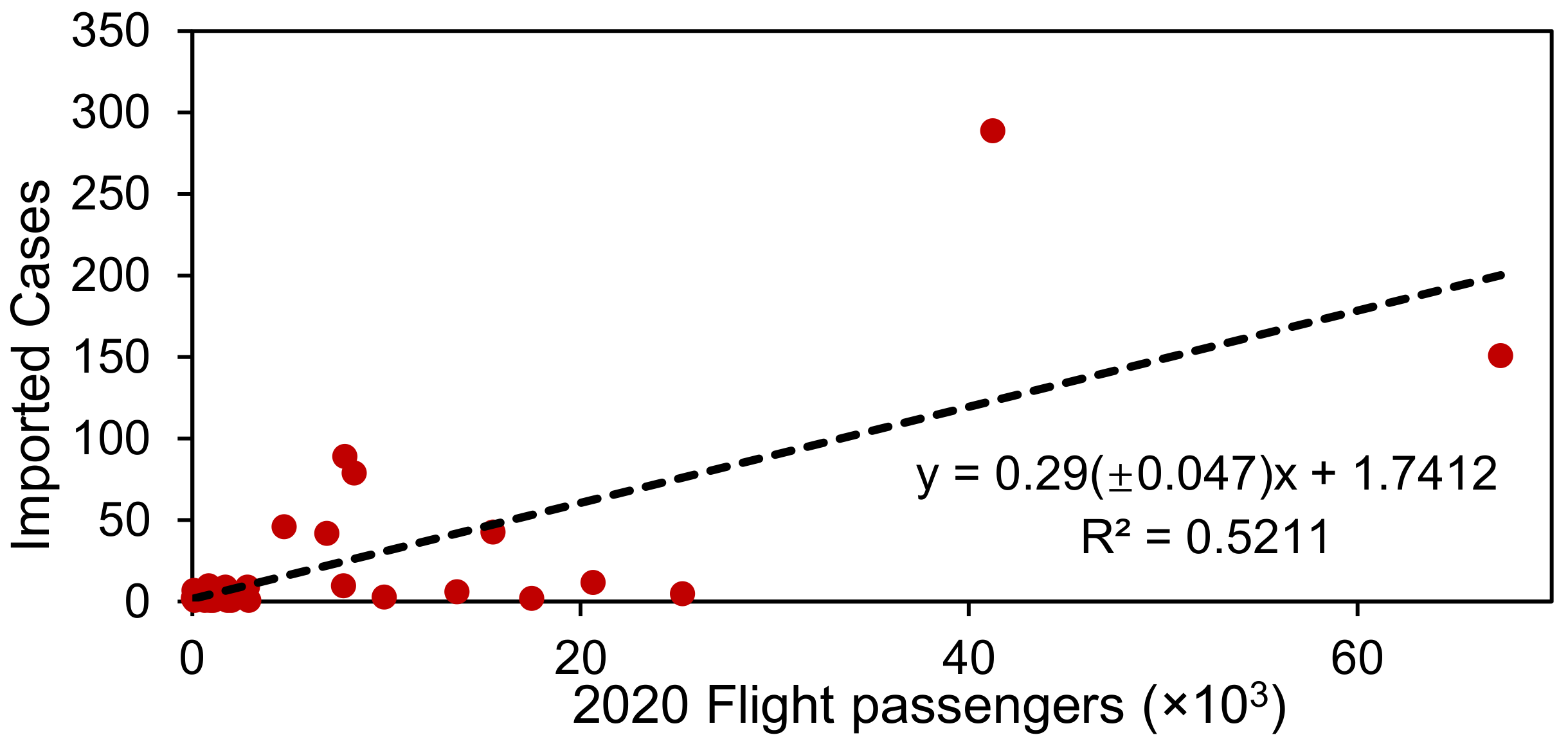
3.3. Effect of Restriction of Inter-Country Mobility on Limiting Case Importation
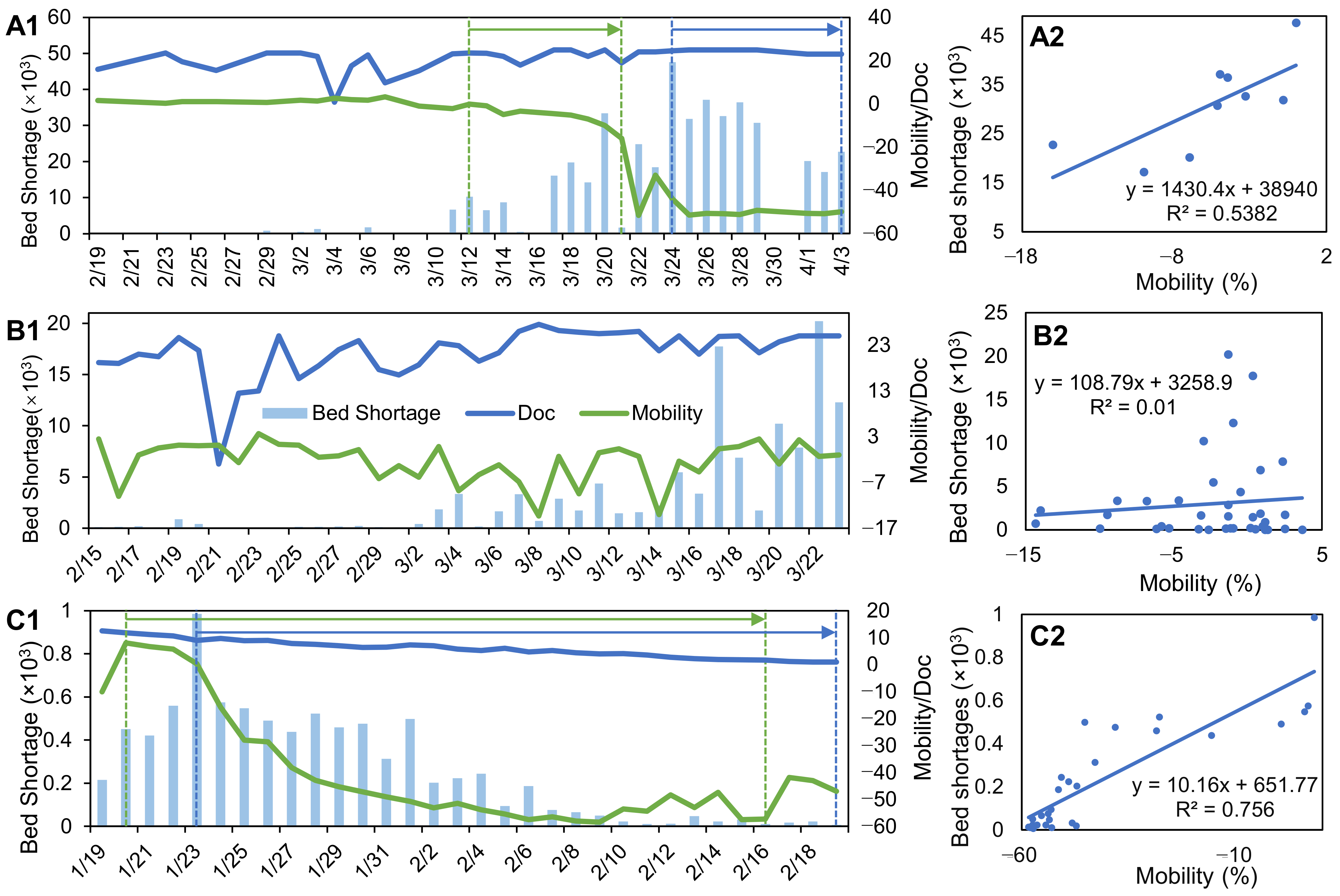
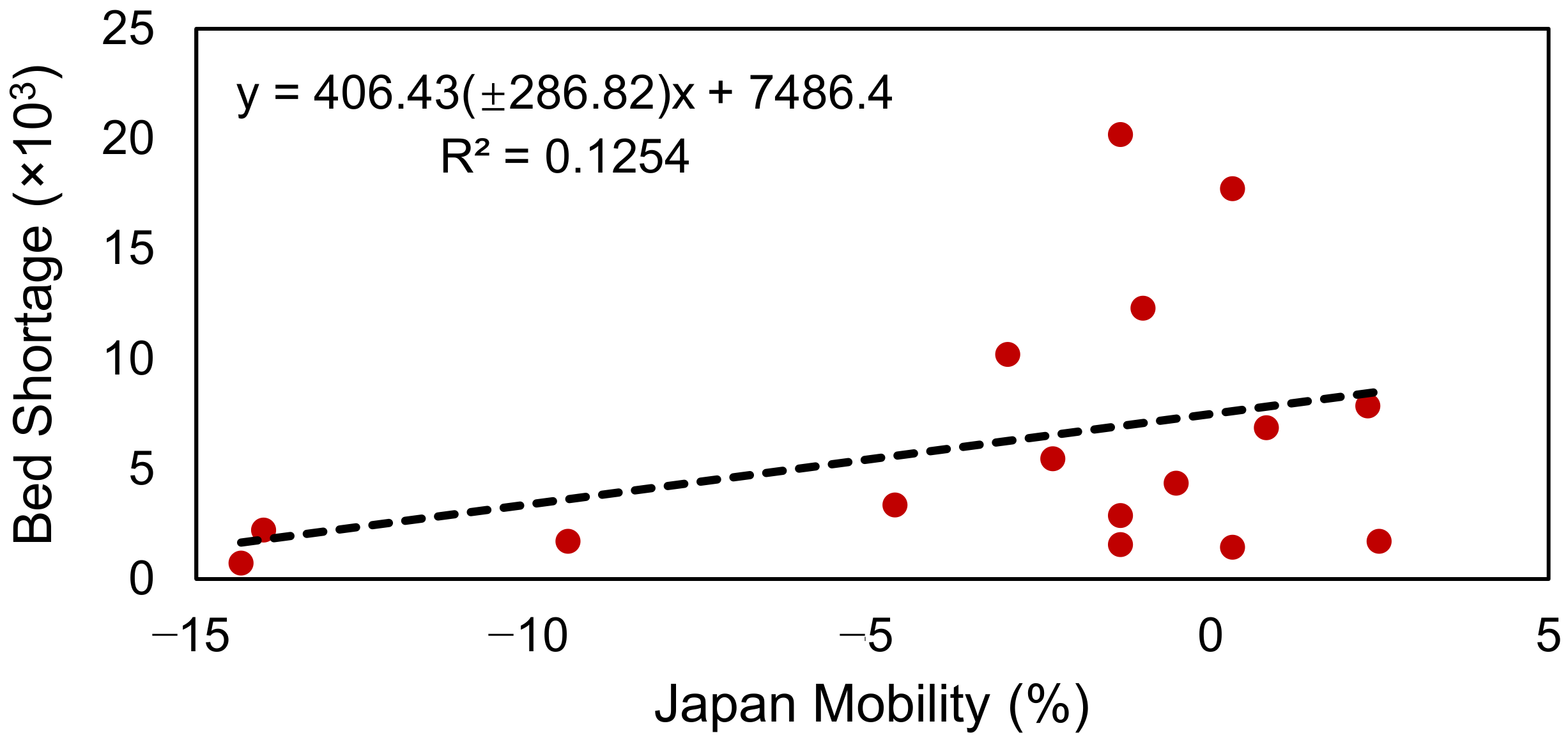
3.4. Effect of Intra-Country Mobility on Hospital Bed Shortages
4. Discussion
4.1. Mobility Restriction Versus Normal Condition
4.2. Prerequisite of Beds Shortage Estimation
4.3. Strengths, Limitations and Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| India | Japan | China | ||||||
|---|---|---|---|---|---|---|---|---|
| Source Country | 2020 Flight Passengers | Imported Cases | Source Country | 2020 Flight Passengers | Imported Cases | Source Country | 2020 Flight Passengers | Imported Cases |
| Australia | 29,673 | 2 | Australia | 47,913 | 2 | Angola | 75 | 3 |
| Bahamas | 20 | 1 | Austria | 3227 | 1 | Austria | 892 | 3 |
| Bahrain | 16,867 | 2 | Belgium | 3020 | 2 | Belgium | 1695 | 5 |
| Bangladesh | 18,229 | 2 | Bolivia | 34 | 1 | Brazil | 1709 | 9 |
| Brazil | 1512 | 3 | Brazil | 4121 | 2 | Burkina Faso | 82 | 7 |
| Canada | 24,496 | 2 | Canada | 14,771 | 3 | Cambodia | 52,633 | 6 |
| China | 1403 | 4 | China | 51,970 | 17 | Canada | 20,638 | 12 |
| Congo | 162 | 1 | Congo | 0 | 1 | Denmark | 642 | 1 |
| Denmark | 2352 | 1 | Cote d’Ivoire | 0 | 1 | Egypt | 1818 | 1 |
| Egypt | 4438 | 1 | Czech | 1787 | 1 | Ethiopia | 2024 | 1 |
| Finland | 1118 | 1 | Egypt | 2622 | 12 | France | 8352 | 79 |
| France | 12,690 | 14 | Ethiopia | 252 | 2 | Germany | 13,638 | 6 |
| Germany | 16,993 | 10 | Finland | 3951 | 3 | Greece | 1097 | 1 |
| Greece | 943 | 1 | France | 24,718 | 26 | Hungary | 722 | 4 |
| Guyana | 14 | 1 | Germany | 17,248 | 9 | Iceland | 127 | 1 |
| Indonesia | 11,687 | 17 | Holland | 4512 | 8 | Indonesia | 9901 | 3 |
| Iran | 688 | 34 | India | 8327 | 1 | Iran | 2829 | 9 |
| Ireland | 3841 | 2 | Indonesia | 36,538 | 5 | Ireland | 940 | 5 |
| Italy | 5146 | 34 | Ireland | 1137 | 9 | Italy | 4736 | 46 |
| Japan | 7318 | 2 | Italy | 9411 | 11 | Japan | 53,170 | 2 |
| Kenya | 5844 | 1 | Korea | 80,459 | 1 | Malaysia | 25,231 | 5 |
| Malaysia | 33,847 | 1 | Mexico | 4849 | 1 | Netherlands | 2717 | 6 |
| Mexico | 508 | 1 | Morocco | 1858 | 1 | Niger | 60 | 2 |
| Netherlands | 5761 | 3 | New Caledonia | 2372 | 1 | Nigeria | 845 | 10 |
| New Zealand | 5714 | 1 | Philippines | 64,747 | 11 | Norway | 443 | 2 |
| Oman | 49,183 | 1 | Portugal | 1220 | 2 | Pakistan | 1444 | 8 |
| Philippines | 3900 | 6 | Spain | 11,619 | 20 | Philippines | 15,501 | 43 |
| Portugal | 1051 | 1 | Switzerland | 3045 | 2 | Russian Federation | 6923 | 42 |
| Qatar | 39,981 | 5 | Thailand | 62,414 | 4 | Saudi Arabia | 585 | 4 |
| Russian Federation | 11,748 | 1 | UK | 21,669 | 24 | Serbia | 1223 | 4 |
| Saudi Arabia | 98,599 | 30 | US | 194,938 | 39 | Singapore | 17,491 | 2 |
| Singapore | 48,595 | 3 | Vietnam | 57,775 | 2 | Spain | 7846 | 89 |
| South Africa | 5942 | 1 | Sweden | 906 | 1 | |||
| Spain | 4512 | 16 | Switzerland | 1522 | 8 | |||
| Sri Lanka | 34,801 | 5 | Thailand | 108,739 | 13 | |||
| Sweden | 1651 | 3 | Turkey | 1291 | 2 | |||
| Switzerland | 4050 | 2 | UAE | 7785 | 10 | |||
| Thailand | 43,419 | 6 | UK | 41,216 | 289 | |||
| Trinidad | 16 | 1 | US | 67,375 | 151 | |||
| Turkey | 9125 | 4 | Vietnam | 2923 | 1 | |||
| UAE | 293,587 | 266 | ||||||
| UK | 68,504 | 73 | ||||||
| US | 113,165 | 29 | ||||||
References
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Eng. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- WHO. Statement on the Second Meeting of the International Health Regulations (2005) Emergency Committee Regarding the Outbreak of Novel Coronavirus (2019-nCoV). Available online: https://www.who.int/news-room/detail/30-01-2020-statement-on-the-second-meeting-of-the-international-health-regulations-(2005)-emergency-committee-regarding-the-outbreak-of-novel-coronavirus-(2019-ncov) (accessed on 8 April 2020).
- Anderson, R.M.; Heesterbeek, H.; Klinkenberg, D.; Hollingsworth, T.D. How will country-based mitigation measures influence the course of the COVID-19 epidemic? Lancet 2020, 395, 931–934. [Google Scholar] [CrossRef]
- Li, R.; Chen, B.; Zhang, T.; Ren, Z.; Song, Y.; Xiao, Y.; Hou, L.; Cai, J.; Xu, B.; Li, M.; et al. Global COVID-19 pandemic demands joint interventions for the suppression of future waves. Proc. Natl. Acad. Sci. USA 2020, 117, 26151–26157. [Google Scholar] [CrossRef]
- Tashiro, A.; Shaw, R. COVID-19 Pandemic response in Japan: What is behind the initial flattening of the Curve? Sustainability 2020, 12, 5250. [Google Scholar] [CrossRef]
- Weill, J.A.; Stigler, M.; Deschenes, O.; Springborn, M.R. Social distancing responses to COVID-19 emergency declarations strongly differentiated by income. Proc. Natl. Acad. Sci. USA 2020, 117, 19658. [Google Scholar] [CrossRef] [PubMed]
- Chinazzi, M.; Davis, J.T.; Ajelli, M.; Gioannini, C.; Litvinova, M.; Merler, S.; Piontti, A.P.; Mu, K.; Rossi, L.; Sun, K.; et al. The effect of travel restrictions on the spread of the 2019 novel coronavirus (COVID-19) outbreak. Science 2020, 368, 395–400. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, R.; Pei, S.; Chen, B.; Song, Y.; Zhang, T.; Yang, W.; Shaman, J. Substantial undocumented infection facilitates the rapid dissemination of novel coronavirus (SARS-CoV-2). Science 2020, 368, 489. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gatto, M.; Bertuzzo, E.; Mari, L.; Miccoli, S.; Carraro, L.; Casagrandi, R.; Rinaldo, A. Spread and dynamics of the COVID-19 epidemic in Italy: Effects of emergency containment measures. Proc. Natl. Acad. Sci. USA 2020, 117, 10484. [Google Scholar] [CrossRef] [Green Version]
- Badr, H.S.; Du, H.; Marshall, M.; Dong, E.; Squire, M.M.; Gardner, L.M. Association between mobility patterns and COVID-19 transmission in the USA: A mathematical modelling study. Lancet Infect. Dis. 2020, 20, 1247–1254. [Google Scholar] [CrossRef]
- Bonaccorsi, G.; Pierri, F.; Cinelli, M.; Flori, A.; Galeazzi, A.; Porcelli, F.; Schmidt, A.L.; Valensise, C.M.; Scala, A.; Quattrociocchi, W.; et al. Economic and social consequences of human mobility restrictions under COVID-19. Proc. Natl. Acad. Sci. USA 2020, 117, 15530. [Google Scholar] [CrossRef] [PubMed]
- Guan, D.; Wang, D.; Hallegatte, S.; Davis, S.J.; Huo, J.; Li, S.; Bai, Y.; Lei, T.; Xue, Q.; Coffman, D.M.; et al. Global supply-chain effects of COVID-19 control measures. Nat. Hum. Behav. 2020, 4, 577–587. [Google Scholar] [CrossRef]
- Nicola, M.; Alsafi, Z.; Sohrabi, C.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C.; Agha, M.; Agha, R. The socio-economic implications of the coronavirus pandemic (COVID-19): A review. Int. J. Surg. 2020, 78, 185–193. [Google Scholar] [CrossRef]
- Hâncean, M.-G.; Perc, M.; Lerner, J. Early spread of COVID-19 in Romania: Imported cases from Italy and human-to-human transmission networks. R. Soc. Open Sci. 2020, 7, 200780. [Google Scholar] [CrossRef] [PubMed]
- Hellewell, J.; Abbott, S.; Gimma, A.; Bosse, N.I.; Jarvis, C.I.; Russell, T.W.; Munday, J.D.; Kucharski, A.J.; Edmunds, W.J.; Sun, F.; et al. Feasibility of controlling COVID-19 outbreaks by isolation of cases and contacts. Lancet Glob. Health 2020, 8, e488–e496. [Google Scholar] [CrossRef] [Green Version]
- Chakraborty, I.; Sen, I.K.; Mondal, S.; Bar, H.; Nayak, A.; Bhanja, S.K.; Maity, P. Traveler as a risk factor for migration of COVID-19 in India. J. Transp. Health 2020, 18, 100915. [Google Scholar] [CrossRef] [PubMed]
- Jia, J.S.; Lu, X.; Yuan, Y.; Xu, G.; Jia, J.; Christakis, N.A. Population flow drives spatio-temporal distribution of COVID-19 in China. Nature 2020, 582, 389–394. [Google Scholar] [CrossRef] [PubMed]
- Sokadjo, Y.M.; Atchadé, M.N. The influence of passenger air traffic on the spread of COVID-19 in the world. Transp. Res. Interdiscip. Perspect. 2020, 8, 100213. [Google Scholar] [CrossRef]
- WHO. Updated WHO Recommendations for International Traffic in Relation to COVID-19 Outbreak. Available online: https://www.who.int/news-room/articles-detail/updated-who-recommendations-for-international-traffic-in-relation-to-covid-19-outbreak (accessed on 27 January 2020).
- Wells, C.R.; Sah, P.; Moghadas, S.M.; Pandey, A.; Shoukat, A.; Wang, Y.; Wang, Z.; Meyers, L.A.; Singer, B.H.; Galvani, A.P. Impact of international travel and border control measures on the global spread of the novel 2019 coronavirus outbreak. Proc. Natl. Acad. Sci. USA 2020, 117, 7504–7509. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yabe, T.; Tsubouchi, K.; Fujiwara, N.; Wada, T.; Sekimoto, Y.; Ukkusuri, S.V. Non-compulsory measures sufficiently reduced human mobility in Tokyo during the COVID-19 epidemic. Sci. Rep. 2020, 10, 18053. [Google Scholar] [CrossRef]
- Wu, J.T.; Leung, K.; Leung, G.M. Nowcasting and forecasting the potential domestic and international spread of the 2019-nCoV outbreak originating in Wuhan, China: A modelling study. Lancet 2020, 395, 689–697. [Google Scholar] [CrossRef] [Green Version]
- Gilbert, M.; Pullano, G.; Pinotti, F.; Valdano, E.; Poletto, C.; Boëlle, P.-Y.; D’Ortenzio, E.; Yazdanpanah, Y.; Eholie, S.P.; Altmann, M.; et al. Preparedness and vulnerability of African countries against importations of COVID-19: A modelling study. Lancet 2020, 395, 871–877. [Google Scholar] [CrossRef] [Green Version]
- Ku, B.S.; Druss, B.G. Associations Between Primary Care Provider Shortage Areas and County-Level COVID-19 Infection and Mortality Rates in the USA. J. Gen. Intern. Med. 2020, 35, 3404–3405. [Google Scholar] [CrossRef] [PubMed]
- Beitler, J.R.; Mittel, A.M.; Kallet, R.; Kacmarek, R.; Hess, D.; Branson, R.; Olson, M.; Garcia, I.; Powell, B.; Wang, D.S.; et al. Ventilator Sharing during an Acute Shortage Caused by the COVID-19 Pandemic. Am. J. Respir. Crit. Care Med. 2020, 202, 600–604. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.W.; Lee, K.S.; Kim, K.; Lee, J.J.; Kim, J.Y.; Daegu Medical Association. A Brief Telephone Severity Scoring System and Therapeutic Living Centers Solved Acute Hospital-Bed Shortage during the COVID-19 Outbreak in Daegu, Korea. J. Korean Med. Sci. 2020, 35, e152. [Google Scholar] [CrossRef] [Green Version]
- de Nardo, P.; Gentilotti, E.; Mazzaferri, F.; Cremonini, E.; Hansen, P.; Goossens, H.; Tacconelli, E.; The Members of the COVID-19MCDA Group. Multi-Criteria Decision Analysis to prioritize hospital admission of patients affected by COVID-19 in low-resource settings with hospital-bed shortage. Int. J. Infect. Dis. 2020, 98, 494–500. [Google Scholar] [CrossRef] [PubMed]
- The Global Aviation Data Management (GADM) program from International Air Transport Association. Available online: https://www.iata.org/en/services/statistics/gadm/ (accessed on 8 April 2020).
- Thompson, R.N.; Stockwin, J.E.; van Gaalen, R.D.; Polonsky, J.A.; Kamvar, Z.N.; Demarsh, P.A.; Dahlqwist, E.; Li, S.; Miguel, E.; Jombart, T.; et al. Improved inference of time-varying reproduction numbers during infectious disease outbreaks. Epidemics 2019, 29, 100356. [Google Scholar] [CrossRef] [PubMed]
- Cori, A.; Ferguson, N.M.; Fraser, C.; Cauchemez, S. A new framework and software to estimate time-varying reproduction numbers during epidemics. Am. J. Epidemiol. 2013, 178, 1505–1512. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, S.; Zhang, Z.; Yang, J.; Wang, J.; Zhai, X.; Bärnighausen, T.; Wang, C. Fangcang shelter hospitals: A novel concept for responding to public health emergencies. Lancet 2020, 395, 1305–1314. [Google Scholar] [CrossRef]
- Rocklöv, J.; Sjödin, H. High population densities catalyse the spread of COVID-19. J. Travel Med. 2020, 27. [Google Scholar] [CrossRef]
- Travel Advisory. Available online: https://www.china-airlines.com/us/en/discover/news/travel-advisory?travelAlert=36257-7030# (accessed on 25 January 2021).
- Schlosser, F.; Maier, B.F.; Jack, O.; Hinrichs, D.; Zachariae, A.; Brockmann, D. COVID-19 lockdown induces disease-mitigating structural changes in mobility networks. Proc. Natl. Acad. Sci. USA 2020, 117, 32883–32890. [Google Scholar] [CrossRef] [PubMed]
- Kraemer, M.U.G.; Yang, C.-H.; Gutierrez, B.; Wu, C.-H.; Klein, B.; Pigott, D.M.; du Plessis, L.; Faria, N.R.; Li, R.; Hanage, W.P.; et al. The effect of human mobility and control measures on the COVID-19 epidemic in China. Science 2020, 368, 493–497. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amagasa, S.; Kojin, H.; Inoue, S. Mobility Trends Reports Revealed “Self-isolation Fatigue” in Japan: Use of Mobility Data for Coronavirus Disease Control. JMA J. 2020, 3, 272–273. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, T.; Uchiumi, C.; Suzuki, N.; Yoshimoto, J.; Murillo-Rodriguez, E. The Psychological Impact of ‘Mild Lockdown’ in Japan during the COVID-19 Pandemic: A Nationwide Survey under a Declared State of Emergency. Int. J. Environ. Res. Public Health 2020, 17, 9382. [Google Scholar] [CrossRef] [PubMed]





| Data Source | Country | Duration |
|---|---|---|
| https://www.covid19india.org/ | India | 2 February 2020–26 April 2020 |
| https://github.com/reustle/covid19japan-data/tree/master/docs/patient_data | Japan | 15 January 2020–17 April 2020 |
| https://github.com/beoutbreakprepared/nCoV2019 | China | 1 January 2020–16 June 2020 |
| https://github.com/Juan-ZJ/COVID-19-line-list |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ren, Z.; Li, R.; Zhang, T.; Chen, B.; Wang, C.; Li, M.; Song, S.; Xiao, Y.; Xu, B.; Liu, Z.; et al. Reduction of Human Mobility Matters during Early COVID-19 Outbreaks: Evidence from India, Japan and China. Int. J. Environ. Res. Public Health 2021, 18, 2826. https://doi.org/10.3390/ijerph18062826
Ren Z, Li R, Zhang T, Chen B, Wang C, Li M, Song S, Xiao Y, Xu B, Liu Z, et al. Reduction of Human Mobility Matters during Early COVID-19 Outbreaks: Evidence from India, Japan and China. International Journal of Environmental Research and Public Health. 2021; 18(6):2826. https://doi.org/10.3390/ijerph18062826
Chicago/Turabian StyleRen, Zhehao, Ruiyun Li, Tao Zhang, Bin Chen, Che Wang, Miao Li, Shuang Song, Yixiong Xiao, Bo Xu, Zhaoyang Liu, and et al. 2021. "Reduction of Human Mobility Matters during Early COVID-19 Outbreaks: Evidence from India, Japan and China" International Journal of Environmental Research and Public Health 18, no. 6: 2826. https://doi.org/10.3390/ijerph18062826
APA StyleRen, Z., Li, R., Zhang, T., Chen, B., Wang, C., Li, M., Song, S., Xiao, Y., Xu, B., Liu, Z., Shen, C., Guan, D., Hou, L., Deng, K., Bai, Y., Gong, P., & Xu, B. (2021). Reduction of Human Mobility Matters during Early COVID-19 Outbreaks: Evidence from India, Japan and China. International Journal of Environmental Research and Public Health, 18(6), 2826. https://doi.org/10.3390/ijerph18062826