
Client-Centered Breastfeeding-Promotion Strategies: Q Methodology

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Research Setting
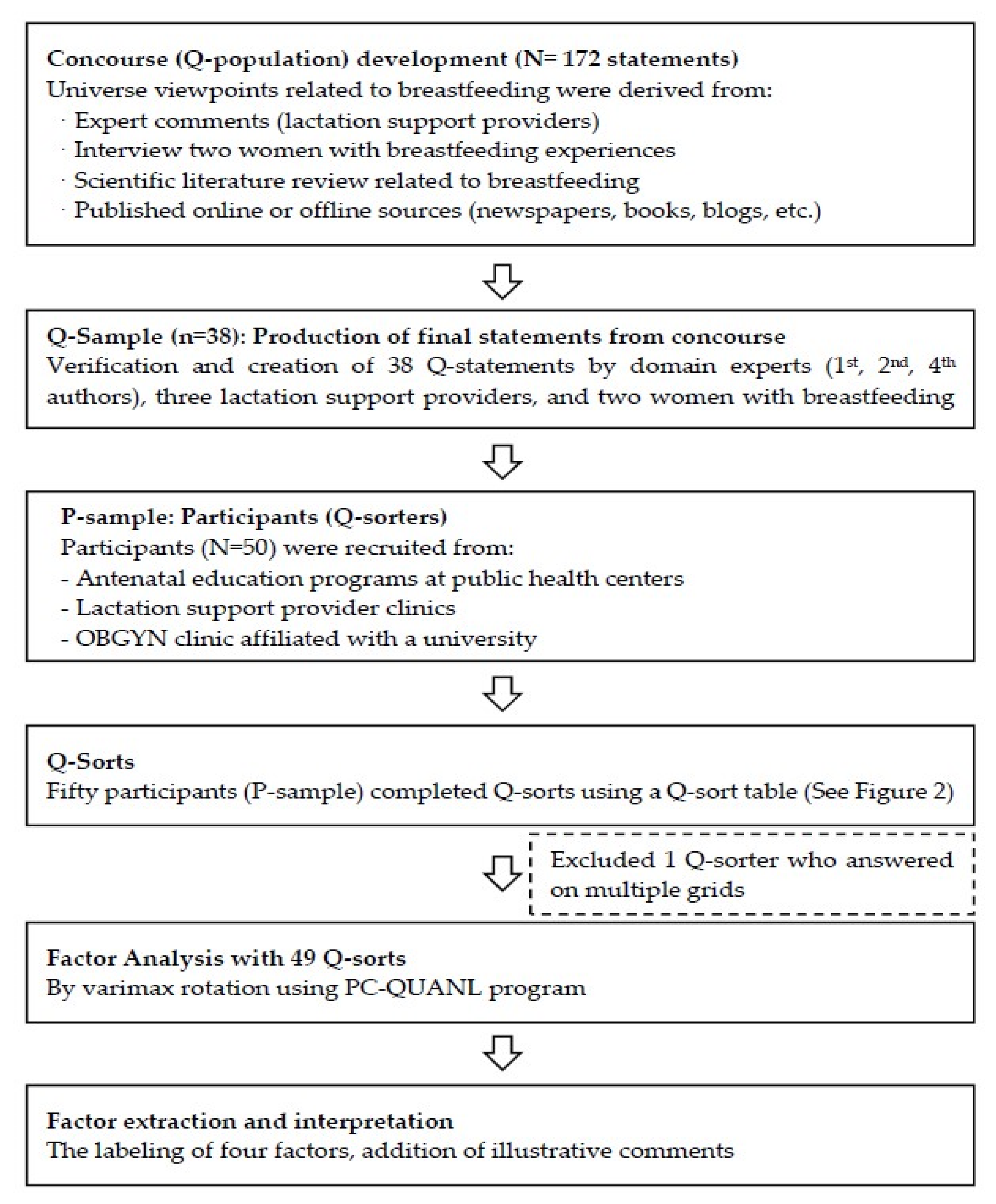
2.3. Research Procedure
2.4. Q Sample
2.5. P Sample
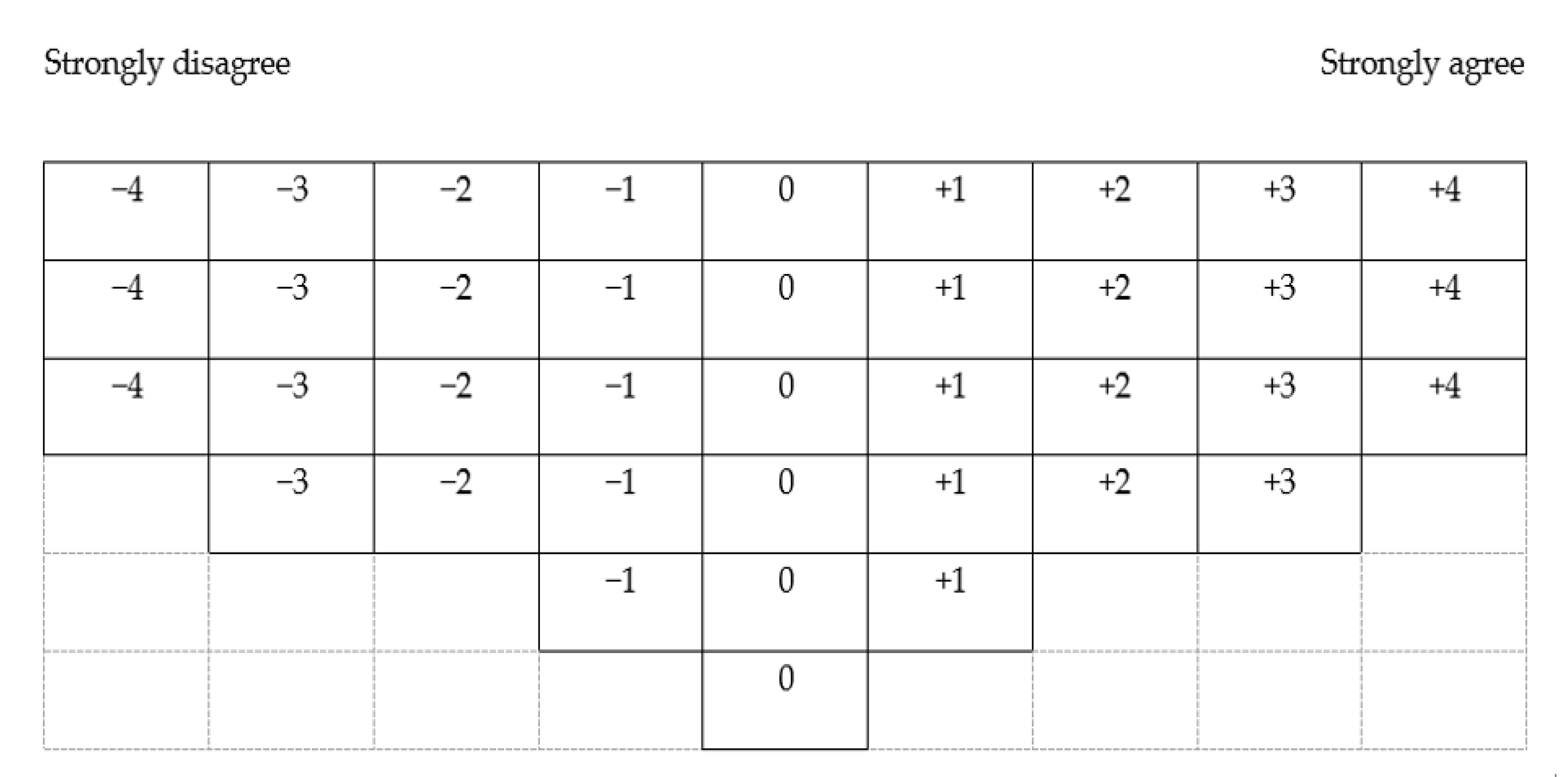
2.6. Data Collection
2.7. Data Analysis
2.8. Ethical Considerations
3. Results
3.1. Patient Characteristics
3.2. Profiles of Each Factor
3.2.1. Factor 1—Maternal Privilege
3.2.2. Factor 2—Option Based on My Emotional Condition
3.2.3. Factor 3—Option if Efficient
3.2.4. Factor 4—Option if I Have Sufficient Problem-Solving Skills
3.3. Comparisons among Factors
3.3.1. Factor 1 vs. Others
3.3.2. Factor 2 vs. Others
3.3.3. Factor 3 vs. Others
3.3.4. Factor 4 vs. Others
3.4. Consensus Items across Factors and Average Z Scores
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Victora, C.G.; Bahl, R.; Barros, A.J.D.; França, G.V.A.; Horton, S.; Krasevec, J.; Murch, S.; Sankar, M.J.; Walker, N.; Rollins, N.C. Breastfeeding in the 21st century: Epidemiology, mechanisms, and lifelong effect. Lancet 2016, 387, 475–490. [Google Scholar] [CrossRef] [Green Version]
- American Academy of Pediatrics. Breastfeeding and the use of human milk. Pediatrics 2012, 129, e827–e841. [Google Scholar] [CrossRef] [Green Version]
- United Nations Children’s Fund (UNICEF). Breastfeeding: A Mother’s Gift, for Every Child; UNICEF: New York, NY, USA, 2018. [Google Scholar]
- Binns, C.; Lee, M.; Low, W.Y. The Long-Term Public Health Benefits of Breastfeeding. Asia Pac. J. Public Health 2016, 28, 7. [Google Scholar] [CrossRef] [Green Version]
- U.S. Department of Health and Human Services. The Surgeon General’s Call to Action to Support Breastfeeding; U.S. Department of Health and Human Services: Washington, DC, USA, 2011.
- Brummelte, S.; Galea, L.A. Postpartum depression: Etiology, treatment and consequences for maternal care. Horm. Behav. 2016, 77, 153–166. [Google Scholar] [CrossRef] [PubMed]
- Del Ciampo, L.A.; Del Ciampo, I.R.L. Breastfeeding and the Benefits of Lactation for Women’s Health. Rev. Bras. Ginecol. Obstet. 2018, 40, 354–359. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Global Breastfeeding Scorecard 2018. Available online: https://www.who.int/nutrition/publications/infantfeeding/global-bf-scorecard-2018.pdf?ua=1 (accessed on 31 January 2021).
- The Academy of Breastfeeding Medicine Korea. Breastfeeding and Exclusive Breastfeeding Rates of Korea. Available online: http://www.bfmed.co.kr/subView.html?cate=1&cate=1&idx=936 (accessed on 31 January 2021).
- Centers for Disease Control and Prevention. Facts: Key Breastfeeding Indicators. Available online: https://www.cdc.gov/breastfeeding/data/facts.html (accessed on 11 March 2021).
- Lee, S.; Kim, E.; Park, J.; Byeon, S.; Oh, M.; Lee, S.; Lee, J. The 2018 National Survey on Fertility and Family Health and Welfare in Korea; Korea Institue for Health and Social Affairs: Sejong, Korea, 2018. [Google Scholar]
- Lee, S.; Bai, Y.K.; You, S.-B. Ecological Factors Influencing Breastfeeding Decisions among Korean Immigrant Mothers in America. J. Child Fam. Stud. 2018, 27, 928–943. [Google Scholar] [CrossRef]
- Park, H.; Ryu, K.; Piao, Y.; Li, P.; Hong, J.; Kim, H.; Chung, H.; Hoh, J.; Kim, Y. Positive Effect of Baby-Friendly Hospital Initiatives on Improving Mothers’ Intention for Successful Breastfeeding in Korea. J. Korean Med. Sci. 2018, 33, e272. [Google Scholar] [CrossRef] [PubMed]
- UNICEF KOREA. Child Friendly Initiative. Available online: https://www.unicef.or.kr/child-rights/initiative/bfhi-information.asp (accessed on 8 August 2020).
- Fang, Z.; Liu, Y.; Wang, H.; Tang, K. The Patterns and Social Determinants of Breastfeeding in 12 Selected Regions in China: A Population-Based Cross-Sectional Study. J. Hum. Lact. 2019, 36, 436–447. [Google Scholar] [CrossRef]
- Mosca, F.; Roggero, P.; Garbarino, F.; Morniroli, D.; Bracco, B.; Morlacchi, L.; Mallardi, D.; Gianni, M.L.; Consonni, D. Determinants of breastfeeding discontinuation in an Italian cohort of mother-infant dyads in the first six months of life: A randomized controlled trial. Ital. J. Pediatrics 2018, 44, 134. [Google Scholar] [CrossRef] [Green Version]
- Lauer, E.; Armenti, K.; Henning, M.; Sirois, L. Identifying Barriers and Supports to Breastfeeding in the Workplace Experienced by Mothers in the New Hampshire Special Supplemental Nutrition Program for Women, Infants, and Children Utilizing the Total Worker Health Framework. Int. J. Environ. Res. Public Health 2019, 16, 529. [Google Scholar] [CrossRef] [Green Version]
- Theurich, M.A.; Davanzo, R.; Busck-Rasmussen, M.; Diaz-Gomez, N.M.; Brennan, C.; Kylberg, E.; Baerug, A.; McHugh, L.; Weikert, C.; Abraham, K.; et al. Breastfeeding Rates and Programs in Europe: A Survey of 11 National Breastfeeding Committees and Representatives. J. Pediatric Gastroenterol. Nutr. 2019, 68, 400–407. [Google Scholar] [CrossRef]
- Eram, U. A review Article: Myths, Beliefs and Malpractices relating to Breastfeeding and Complementary Feeding Practices. Int. J. Pharm. Sci. Invent. 2017, 6, 14–16. [Google Scholar]
- Zhu, Y.; Zhang, Z.; Ling, Y.; Wan, H. Impact of intervention on breastfeeding outcomes and determinants based on theory of planned behavior. Women Birth 2017, 30, 146–152. [Google Scholar] [CrossRef] [PubMed]
- Radzyminski, S.; Callister, L.C. Mother’s Beliefs, Attitudes, and Decision Making Related to Infant Feeding Choices. J. Perinat. Educ. 2016, 25, 18–28. [Google Scholar] [CrossRef] [Green Version]
- Arora, A.; Manohar, N.; Hayen, A.; Bhole, S.; Eastwood, J.; Levy, S.; Scott, J.A. Determinants of breastfeeding initiation among mothers in Sydney, Australia: Findings from a birth cohort study. Int. Breastfeed. J. 2017, 12, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Nasrabadi, M.; Vahedian-Shahroodi, M.; Esmaily, H.; Tehrani, H.; Gholian-Aval, M. Factors affecting Exclusive breastfeeding in the first six months of birth: An Exploratory-Descriptive Study. J. Midwifery Reprod. Health 2019, 7, 1749. [Google Scholar]
- Dall’Oglio, I.; Marchetti, F.; Mascolo, R.; Amadio, P.; Gawronski, O.; Clemente, M.; Dotta, A.; Ferro, F.; Garofalo, A.; Salvatori, G.; et al. Breastfeeding Protection, Promotion, and Support in Humanitarian Emergencies: A Systematic Review of Literature. J. Hum. Lact. Off. J. Int. Lact. Consult. Assoc. 2020. [Google Scholar] [CrossRef] [PubMed]
- Parkinson, J.; Russell-Bennett, R.; Previte, J. Challenging the planned behavior approach in social marketing: Emotion and experience matter. Eur. J. Mark. 2018, 52, 837. [Google Scholar] [CrossRef]
- Zabala, A.; Sandbrook, C.; Mukherjee, N. When and how to use Q methodology to understand perspectives in conservation research. Conserv. Biol. 2018, 32, 1185–1194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zabala, A.; Pascual, U. Bootstrapping Q Methodology to Improve the Understanding of Human Perspectives. PLoS ONE 2016, 11, e0148087. [Google Scholar] [CrossRef]
- Brown, S.R. Subjectivity in the Human Sciences. Psychol. Rec. 2019, 69, 565–579. [Google Scholar] [CrossRef]
- Andreasen, A.R. Marketing Social Changes: Changing Behavior to Promote Health, Social Development and the Environment; Jossey-Bass: San Francisco, CA, USA, 1995. [Google Scholar]
- Choi, E.J. Breastfeeding-related Social Environmental Factors and Their Policy Implications. Health Soc. Aff. Forum 2017, 249, 72–81. [Google Scholar]
- McKeown, B.; Thomas, D.B. Q Methodology, 2nd ed.; Sage: Thousand Oaks, CA, USA, 2013. [Google Scholar]
- Watts, S.; Stenner, P. Doing Q Metodological Research: Theory, Method and Interpretation; Sage Publication: London, UK, 2012. [Google Scholar]
- Van Tubergen, N. QUANL User’s Guide, a Computer Program Providing a Single Execution Method for Handling All Phases of Stephenson’s Q Analysis Offset; Department of Communication, University of Kentucky: Lexington, KY, USA, 1975. [Google Scholar]
- Chon, M.; Yeun, E.; Jung, K.; Jo, Y.; Lee, K. Perceptions of resilience in patients undergoing peritoneal dialysis: A Q-methodology study. Nurs. Health Sci. 2020, 22, 108. [Google Scholar] [CrossRef]
- UNICEF. Adopting Optimal Feeding Practices Is Fundamental to a Child’s Survival, Growth and Development, But Too Few Children Benefit. Available online: https://data.unicef.org/topic/nutrition/infant-and-young-child-feeding/ (accessed on 11 March 2021).
- Odeniyi, A.; Embleton, N.; Ngongalah, L.; Akor, W.; Rankin, J. Breastfeeding beliefs and experiences of African immigrant mothers in high-income countries: A systematic review. Matern. Child Nutr. 2020, 16, 1. [Google Scholar] [CrossRef] [PubMed]
- Yi, H. Discourse of child and childhood in the Korean society reflected in baby contests and sports meetings. J. Child Educ. 2012, 21, 267–280. [Google Scholar]
- Choi, E.; Park, E.; Kim, H.; Lee, N.; Choi, J. A Report on the Breastfeeding Survey of 2016; Korea Institute of Health and Social Affairs: Sejong, Korea, 2016. [Google Scholar]
- Almeida, R.; Alvarez Gutierrez, S.; Whaley, S.E.; Ventura, A.K. A Qualitative Study of Breastfeeding and Formula-Feeding Mothers’ Perceptions of and Experiences in WIC. J. Nutr. Educ. Behav. 2020, 52, 615–625. [Google Scholar] [CrossRef]
- Kendall-Tackett, K. The new paradigm for depression in new mothers: Current findings on maternal depression, breastfeeding and resiliency across the lifespan. Breastfeed. Rev. Prof. Publ. Nurs. Mothers’ Assoc. Aust. 2015, 23, 7–10. [Google Scholar]
- Webber, E.; Benedict, J. Postpartum depression: A multi-disciplinary approach to screening, management and breastfeeding support. Arch. Psychiatr. Nurs. 2019, 33, 284–289. [Google Scholar] [CrossRef] [PubMed]
- Weaver, J.M.; Schofield, T.J.; Papp, L.M. Breastfeeding duration predicts greater maternal sensitivity over the next decade. Dev. Psychol. 2018, 54, 220–227. [Google Scholar] [CrossRef]
- Anstey, E.H.; Coulter, M.; Jevitt, C.M.; Perrin, K.M.; Dabrow, S.; Klasko-Foster, L.B.; Daley, E.M. Lactation Consultants’ Perceived Barriers to Providing Professional Breastfeeding Support. J. Hum. Lact. 2018, 34, 51. [Google Scholar] [CrossRef]
- McKinney, C.H.; Honig, T.J. Health Outcomes of a Series of Bonny Method of Guided Imagery and Music Sessions: A Systematic Review. J. Music Ther. 2017, 54, 1–34. [Google Scholar] [CrossRef]
- Sayres, S.; Visentin, L. Breastfeeding: Uncovering barriers and offering solutions. Curr. Opin. Pediatr. 2018, 30, 591–596. [Google Scholar] [CrossRef] [PubMed]
- Friedman, D.; Hechter, M. The Contribution of Rational Choice Theory to Macrosociological Research. Sociol. Theory 1988, 6, 201–218. [Google Scholar] [CrossRef]
- Goodman, J.H. Perinatal depression and infant mental health. Arch. Psychiatr. Nurs. 2019, 33, 217–224. [Google Scholar] [CrossRef]
- Regina Alves, Y.; Leontina do Couto, L.; Mateus Barreto, A.C.; Baptista Quitete, J. Breastfeeding under the umbrella of support networks: A facilitative strategy. Anna Nery Sch. J. Nurs. Esc. Anna Nery Rev. Enferm. 2020, 24, 1. [Google Scholar]
- Fahey, J.O.; Shenassa, E. Understanding and meeting the needs of women in the postpartum period: The Perinatal Maternal Health Promotion Model. J. Midwifery Womens Health 2013, 58, 613–621. [Google Scholar] [CrossRef]
- Mercer, R.T. Becoming a mother versus maternal role attainment. J. Nurs. Scholarsh. 2004, 36, 226–232. [Google Scholar] [CrossRef] [PubMed]
- Francis, J.; Mildon, A.; Stewart, S.; Underhill, B.; Tarasuk, V.; Di Ruggiero, E.; Sellen, D.; O’Connor, D. Vulnerable mothers’ experiences breastfeeding with an enhanced community lactation support program. Matern. Child Nutr. 2020, 16, 1. [Google Scholar] [CrossRef] [PubMed]
- Bandura, A. Self-efficacy: Toward a unifying theory of behavioral change. Psychol. Rev. 1977, 84, 191–215. [Google Scholar] [CrossRef] [PubMed]
- Stenner, P.; Watts, S.; Worrell, M. Q Methodology; Sage: Thousand Oaks, CA, USA, 2008. [Google Scholar]
- Bronfenbrenner, U. The Ecology of Human Development: Experiments by Nature and Design; Harvard University Press: Cambridge, MA, USA, 1979. [Google Scholar]
- Ajzen, I.; Fishbein, M. The prediction of behavior from attitudinal and normative variables. J. Exp. Soc. Psychol. 1970, 6, 466–487. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | Factor 1 (n = 23) | Factor 2 (n = 13) | Factor 3 (n = 11) | Factor 4 (n = 2) | Total Sample (N = 49) |
|---|---|---|---|---|---|
| Eigenvalues (% of total variance) | 17.90 (36.5%) | 4.31 (8.8%) | 1.92 (3.9%) | 1.81 (3.7%) | N/A |
| Age (years), n (%) | |||||
| 20–30 | 3 (13.0%) | 2 (15.4%) | 3 (27.3%) | 1 (50.0%) | 9 (18.4%) |
| 31–40 | 19 (82.6%) | 11 (84.6%) | 7 (63.6%) | 1 (50.0%) | 38 (77.6%) |
| ≥ 41 | 1 (4.3%) | 0 (0.0%) | 1 (9.1%) | 0 (0.0%) | 2 (4.0%) |
| Mean age ± SD | 33.8 ± 0.49 | 33.4 ± 3.52 | 32.7 ± 4.81 | 33.0 ± 4.24 | 33.4 ± 3.49 |
| Pregnancy history | |||||
| Yes | 16 (69.6%) | 9 (69.2%) | 9 (81.8%) | 2 (100%) | 36 (73.5%) |
| No | 7 (30.4%) | 4 (30.8%) | 2 (18.2%) | 0 (0.0%) | 13 (26.5%) |
| Breastfeeding history | |||||
| Yes | 14 (60.9%) | 7 (53.8%) | 9 (81.8%) | 2 (100%) | 32 (65.3%) |
| No | 9 (39.1%) | 6 (46.2%) | 2 (18.2%) | 0 (0.0%) | 17 (34.7%) |
| Currently pregnant | |||||
| Yes | 8 (34.8%) | 6 (46.2%) | 5 (45.5%) | 0 (0.0%) | 19 (38.8%) |
| No | 15 (65.2%) | 7 (53.8%) | 6 (54.5%) | 2 (100%) | 30 (61.2%) |
| Marital status | |||||
| Married | 23 (100%) | 13 (100%) | 11(100%) | 2 (100%) | 49 (100.0%) |
| Unmarried | 0 | 0 | 0 | 0 | 0 (0.0%) |
| Education | |||||
| Completed high school | 5 (21.7%) | 1 (7.7%) | 1 (9.1%) | 1 (50%) | 8 (16.3%) |
| Completed college or university | 16 (69.6%) | 11 (84.6%) | 10 (90.9%) | 1 (50%) | 38 (77.6%) |
| Completed grad program | 2 (8.7%) | 1 (7.7%) | 0 | 0 | 3 (6.1%) |
| Item | Z Scores | |||
|---|---|---|---|---|
| Factor 1 | Factor 2 | Factor 3 | Factor 4 | |
| 1. Breastfeeding is a woman’s responsibility. | 0.11 | −2.03 | −0.62 | 0.32 |
| 2. Breastfeeding is something only I can do for my baby. | 2.02 | 1.03 | 1.01 | 1.17 |
| 3. It is difficult for me to adhere to the baby’s breastfeeding schedule. | −0.03 | 0.34 | 0.77 | 1.17 |
| 4. If it causes stress, I’d rather not breastfeed. | 0.50 | 2.17 | 0.95 | 0.85 |
| 5. If it causes pain, I’d rather not breastfeed. | −0.27 | 0.50 | 0.02 | −0.02 |
| 6. Although the doctor has prescribed me to take medicines, I am worried that they will affect my baby through breastfeeding. | 0.96 | 0.93 | 0.93 | 0.90 |
| 7. Healthcare professionals’ opinions on breastfeeding affect my decision making. | 0.67 | 0.39 | 0.37 | 2.03 |
| 8. Information related to breastfeeding from the Internet, blogs, friends, and peers affects my decision making. | −0.12 | 0.55 | −0.82 | −1.52 |
| 9. Breastfeeding makes me feel like a cow. | −1.65 | −0.79 | −1.29 | −0.99 |
| 10. I do not mind breastfeeding in front of my husband. | 1.31 | 0.84 | 1.31 | 1.38 |
| 11. I will stop breastfeeding after 6 months because it does not help with the baby’s growth. | −0.92 | 0.30 | −1.36 | −1.71 |
| 12. If the baby does not gain weight during breastfeeding, I would lose confidence, thinking that it is not helping. | 0.37 | 0.18 | 1.30 | −1.04 |
| 13. Breastfeeding restricts my physical freedom. | −1.49 | −0.48 | 0.79 | 0.19 |
| 14. Putting out my breast to breastfeed in public is embarrassing. | −0.38 | 1.18 | 0.96 | 0.51 |
| 15. I would become the perfect woman through breastfeeding. | 0.03 | −1.95 | −1.25 | −0.85 |
| 16. Breastfeeding makes me sexually unattractive. | −1.67 | −1.77 | −1.43 | 1.36 |
| 17. Breastfeeding is time-saving compared to bottle-feeding. | 1.28 | −0.88 | 1.00 | 0.19 |
| 18. When I go out, breastfeeding is more convenient than bottle-feeding. | 1.50 | −0.93 | 1.50 | −0.48 |
| 19. Breastfeeding endears my child to me even further. | 1.91 | 0.59 | 0.62 | 1.04 |
| 20. Breastfeeding brings me closer to my husband. | 0.54 | 0.04 | −1.41 | −0.85 |
| 21. I avoid breastfeeding since it restricts medical treatment. | −0.86 | −0.39 | −0.90 | −0.90 |
| 22. I avoid breastfeeding since it puts restrictions on my diet. | −0.61 | −0.50 | −0.11 | −0.32 |
| 23. I am worried that increasing my food intake to facilitate breastfeeding would make me obese. | −0.24 | 0.07 | −0.82 | 0.48 |
| 24. I’d rather bottle-feed my baby instead of turning my back on him/her because breastfeeding upsets/annoys me. | 0.15 | 1.54 | 0.10 | −0.35 |
| 25. Breastfeeding takes up too much of my energy, and thus it difficult to pay other family members an adequate amount of attention. | −0.65 | −0.09 | 0.18 | −1.36 |
| 26. I consider family members’ opinions when I make breastfeeding decisions. | −0.89 | −1.10 | −1.65 | −0.64 |
| 27. The pumping makes me feel like an animal. | −1.32 | −0.77 | −0.86 | −0.53 |
| 28. I do not want to breastfeed if my family views it negatively. | −0.68 | 0.37 | −1.27 | 1.68 |
| 29. Breastfeeding is good for my health. | 1.12 | 0.03 | 0.08 | 0.35 |
| 30. Bottle-feeding with breast milk is better than direct breastfeeding since it helps to check the amount of milk the baby has consumed. | −0.91 | 0.05 | −0.49 | −0.51 |
| 31. If the amount of colostrum is small, I lose confidence about breastfeeding. | −0.32 | −0.31 | 0.81 | 0.64 |
| 32. Breastfeeding should be continued despite the deficiency of breastmilk. | 0.81 | −1.15 | 0.54 | −1.01 |
| 33. My emotional state during breastfeeding affects the baby’s health. | 1.47 | 1.12 | 1.29 | 0.51 |
| 34. The baby’s lactation schedule affects my daily routine. | 1.19 | 1.35 | 1.19 | 0.56 |
| 35. If I breastfeed, family members should endure various inconvenience such as my unavailability to attend to the need of other family members. | −0.72 | 0.13 | 0.21 | −0.35 |
| 36. I avoid breastfeeding since it costs a lot of money for breast care during breastfeeding. | −0.89 | −1.12 | −1.21 | −1.68 |
| 37. The shape of my nipple affects my decision regarding breastfeeding. | 0.11 | 0.26 | 0.43 | 1.54 |
| 38. Continuation of breastfeeding depends on my will. | 1.16 | 1.97 | 1.77 | 1.01 |
| Item | Z Score |
|---|---|
| 38. Whether to continue breastfeeding relies on my will. | 1.48 |
| 33. During breastfeeding, my emotional state affects the baby’s health. | 1.10 |
| 34. The baby’s lactation habit affects my daily life. | 1.07 |
| 9. I feel like a cow when I breastfeed my baby. | −1.18 |
| 10. I do not mind breastfeeding in front of my husband. | 1.21 |
| 36. I avoid breastfeeding since it costs a lot of money for breast care during breastfeeding. | −1.23 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cha, E.; Shin, M.H.; Braxter, B.J.; Park, I.S.; Jang, H.; Kang, B.H. Client-Centered Breastfeeding-Promotion Strategies: Q Methodology. Int. J. Environ. Res. Public Health 2021, 18, 2955. https://doi.org/10.3390/ijerph18062955
Cha E, Shin MH, Braxter BJ, Park IS, Jang H, Kang BH. Client-Centered Breastfeeding-Promotion Strategies: Q Methodology. International Journal of Environmental Research and Public Health. 2021; 18(6):2955. https://doi.org/10.3390/ijerph18062955
Chicago/Turabian StyleCha, EunSeok, Myoung Hwan Shin, Betty J. Braxter, In Sook Park, Hyesun Jang, and Byung Hun Kang. 2021. "Client-Centered Breastfeeding-Promotion Strategies: Q Methodology" International Journal of Environmental Research and Public Health 18, no. 6: 2955. https://doi.org/10.3390/ijerph18062955
APA StyleCha, E., Shin, M. H., Braxter, B. J., Park, I. S., Jang, H., & Kang, B. H. (2021). Client-Centered Breastfeeding-Promotion Strategies: Q Methodology. International Journal of Environmental Research and Public Health, 18(6), 2955. https://doi.org/10.3390/ijerph18062955