
Effectiveness of a Web-Based Intervention on Parental Psychological Flexibility and Emotion Regulation: A Pilot Open Trial



Abstract
:1. Introduction
2. Materials and Methods
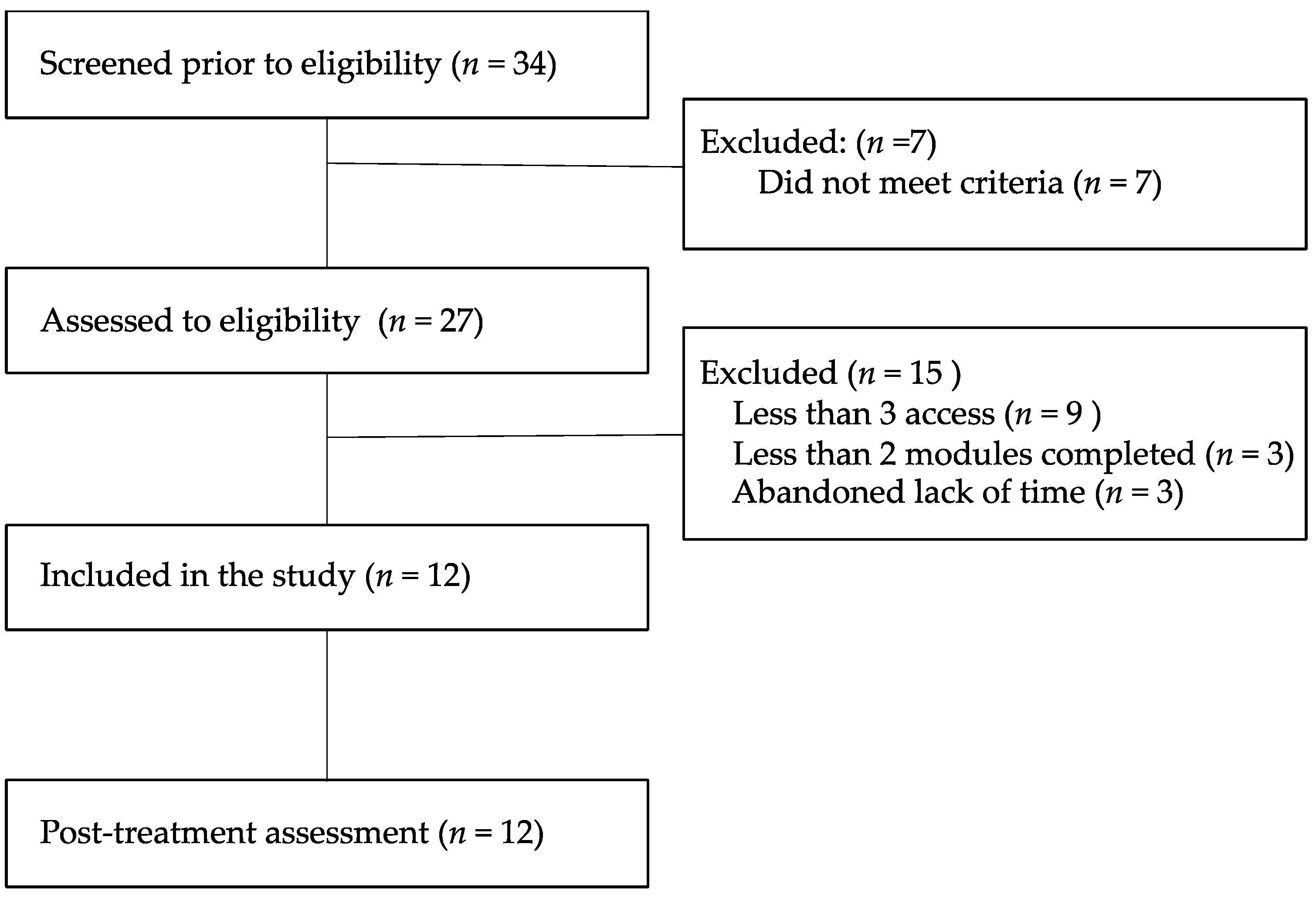
2.1. Design
2.2. Participants
2.3. Intervention

{kind=link}
{kind=link}
{kind=link}
| Module Title | Module Content |
|---|---|
| 1. Welcome to the parenting forest | 1. Introduction to clinical protocol: objectives and sequence. 2. The “Forest Metaphor”: introduction to work on actions towards values. 3. The mind is a lake metaphor: emphasizes that the thoughts and emotions form part of the mind, that they are there and are part of our nature. 4. Explanation of what is mindfulness and first practice of mindfulness to breathing. 5. The garden metaphor [70] values clarification and general goals. 6. Self-evaluation of contents and homework. |
| 2. Emotion regulation with acceptance | 1. Welcome and objectives of the module. 2. The “garden exercise”: Reminder of the contents of the last session. Establishment of specific goals and steps for actions in the direction of values. 3. The “shelter”: exercise of the wise mind [71]. Identify actions involving the emotional mind vs. the rational mind. Establish cohesion with the parenting and look for alternative reactions. 4. Self-evaluation of contents and homework. |
| 3. Walking through the forest | 1. Welcome and objectives of the module. 2. The “garden exercise”: evaluation of the achievement of actions. Identification of barriers and difficulties and alternative actions. 3. “Body scan” mindfulness exercise. Physical sensations related to emotions. 4. “The star observatory”: a defusion exercise to strengthen perspective-taking in private events. 5. Self-evaluation of contents and homework. |
| 4. Allow your emotions to flow | 1. Welcome and objectives of the module. 2. The “garden exercise”: evaluation of the achievement of actions. Identification or barriers. Generalization of parenting skills to goals. 3. “Full attention of sound” mindfulness exercise. 4. The “cascade of emotions”: deliteralization of private events. 5. Self-evaluation of contents and homework. |
| 5. Analyzing your parenting | 1. Welcome and objectives of the module. 2. The “garden exercise”: self-assessment of achievements of actions. Identification or barriers. 3. Functional analysis of parenting for of both parents’ and children’s behavior. Generalization of parenting skills applied to analyzed situation. 4. Thoughts are clouds exercise: deliteralization of private events. 5. The “Connect and Shape” parenting model [72]. 6. Self-evaluation of contents and homework. |
| 6. The other side of the forest | 1. Welcome and objectives of the module. 2. The “garden exercise”: evaluation of the achievement of actions. Empowerment for future goals. 3. Review of the “Connect and Shape” parenting model [72]. 4. Provide behavioral strategies for managing their children’s behavior and emotional problems: modeling, identification of reinforcers, reinforcement, control of antecedent stimuli, differential reinforcement, Premack principle, extinction, overcorrection and timeout. 5. Review skills that have been most useful and relapse prevention. |
2.4. Measuring Instruments
2.4.1. Instruments to Assess Primary Parental Outcomes
2.4.2. Measures of Parent’s Process Outcomes
2.4.3. Instrument to Assess Children Outcomes
2.4.4. Measure of Intervention Satisfaction
2.5. Statistical Analysis
3. Results
3.1. Descriptive Analysis
3.2. Intervention Effects
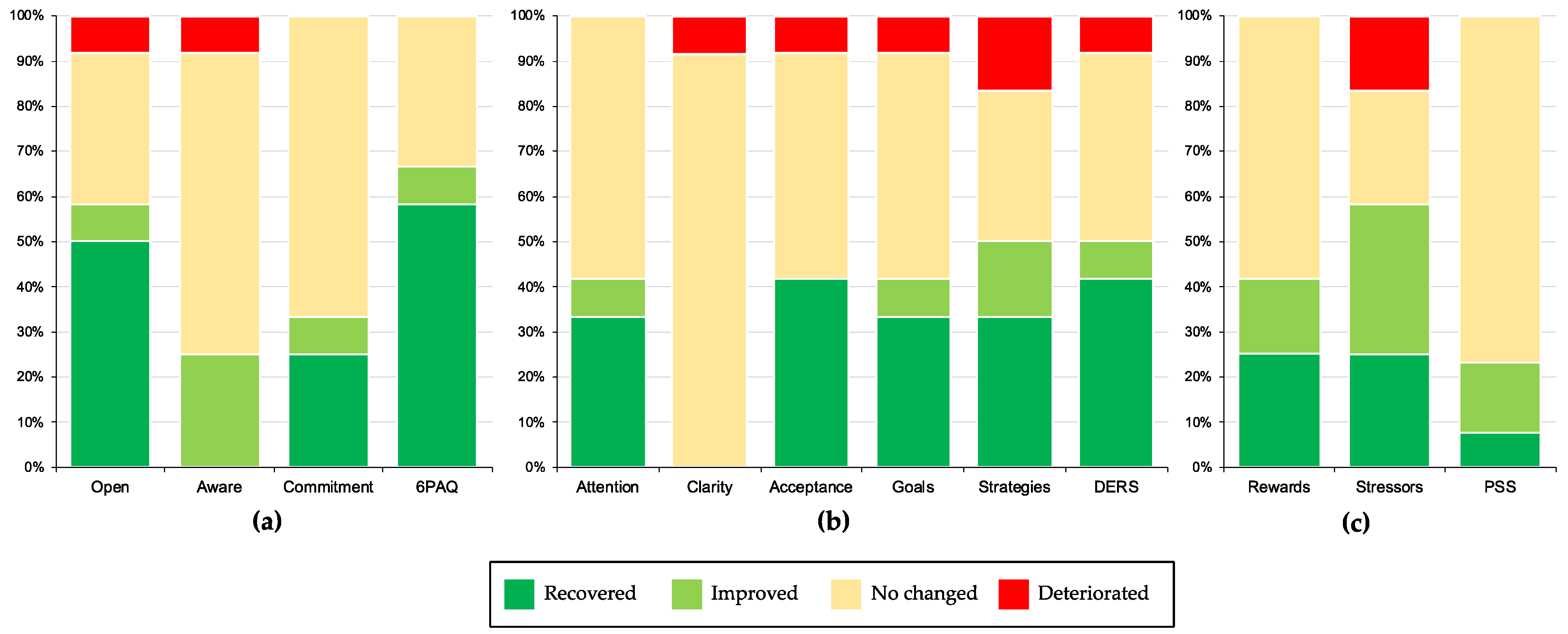
3.3. Significant of Clinical Change
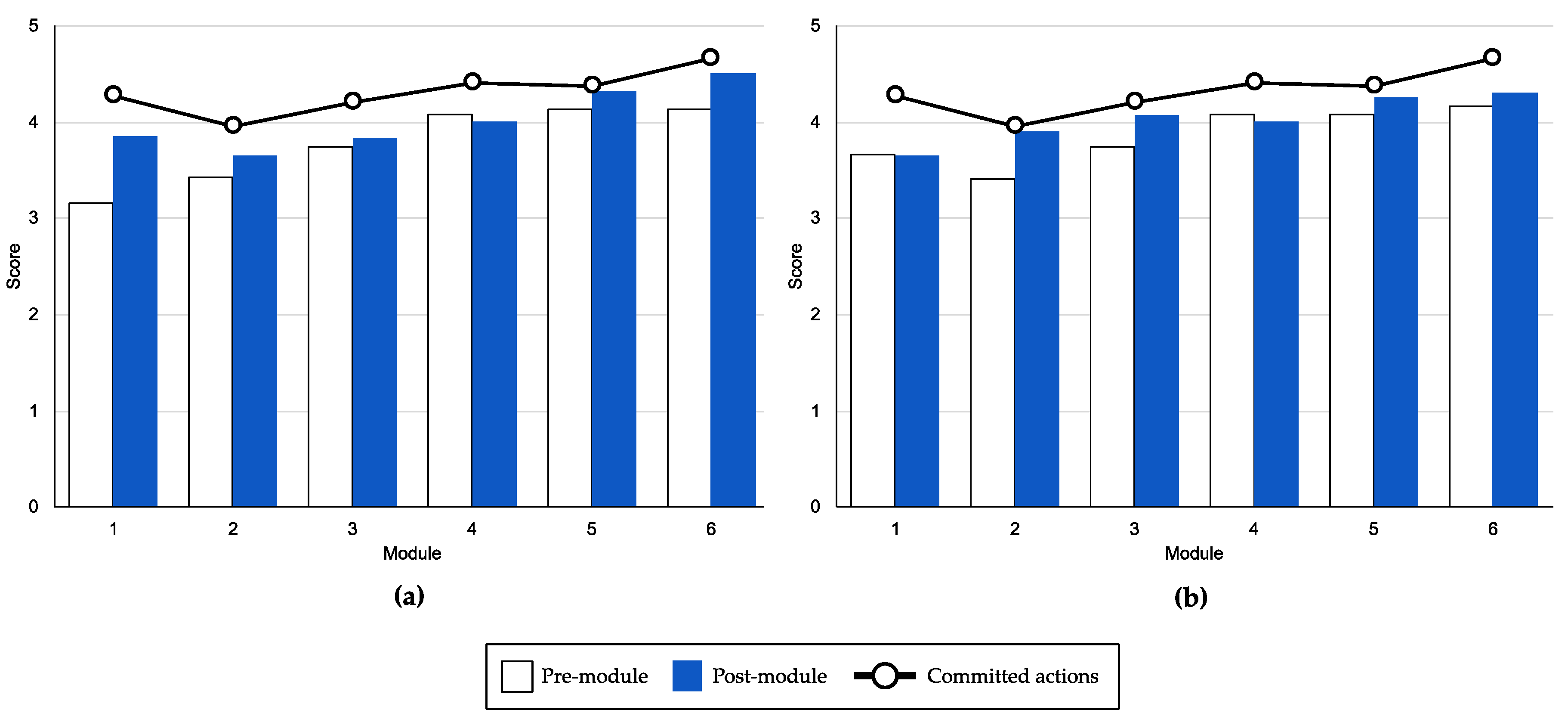
3.4. Process Outcomes
3.5. Measure of Intervention Satisfaction
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kuppens, S.; Ceulemans, E. Parenting Styles: A Closer Look at a Well-Known Concept. J. Child Fam. Stud. 2019, 28, 168–181. [Google Scholar] [CrossRef] [Green Version]
- Rekart, K.N.; Mineka, S.; Zinbarg, R.E.; Griffith, J.W. Perceived Family Environment and Symptoms of Emotional Disorders: The Role of Perceived Control, Attributional Style, and Attachment. Cogn Ther Res 2007, 31, 419–436. [Google Scholar] [CrossRef]
- Martínez, I.; Murgui, S.; Garcia, O.F.; Garcia, F. Parenting in the Digital Era: Protective and Risk Parenting Styles for Traditional Bullying and Cyberbullying Victimization. Comput. Hum. Behavior 2019, 90, 84–92. [Google Scholar] [CrossRef]
- Zarra-Nezhad, M.; Viljaranta, J.; Sajaniemi, N.; Aunola, K.; Lerkkanen, M.-K. The Impact of Children’s Socioemotional Development on Parenting Styles: The Moderating Effect of Social Withdrawal. Early Child Dev. Care 2020, 1–13. [Google Scholar] [CrossRef]
- Gorostiaga, A.; Aliri, J.; Balluerka, N.; Lameirinhas, J. Parenting Styles and Internalizing Symptoms in Adolescence: A Systematic Literature Review. Int. J. Envion. Res. Public Health 2019, 16, 3192. [Google Scholar] [CrossRef] [Green Version]
- Mak, M.C.K.; Yin, L.; Li, M.; Cheung, R.Y.; Oon, P.-T. The Relation between Parenting Stress and Child Behavior Problems: Negative Parenting Styles as Mediator. J. Child Fam. Stud. 2020, 29, 2993–3003. [Google Scholar] [CrossRef]
- Fonseca, A.; Moreira, H.; Canavarro, M.C. Uncovering the Links between Parenting Stress and Parenting Styles: The Role of Psychological Flexibility within Parenting and Global Psychological Flexibility. J. Contextual Behav. Sci. 2020, 18, 59–67. [Google Scholar] [CrossRef]
- Burke, K.; Moore, S. Development of the Parental Psychological Flexibility Questionnaire. Child Psychiatry Hum. Dev. 2015, 46, 548–557. [Google Scholar] [CrossRef] [PubMed]
- Emerson, L.-M.; Ogielda, C.; Rowse, G. The Role of Experiential Avoidance and Parental Control in the Association Between Parent and Child Anxiety. Front. Psychol. 2019, 10, 262. [Google Scholar] [CrossRef] [PubMed]
- Moyer, D.N.; Sandoz, E.K. The Role of Psychological Flexibility in the Relationship Between Parent and Adolescent Distress. J. Child Fam. Stud. 2015, 24, 1406–1418. [Google Scholar] [CrossRef]
- Biglan, A.; Gau, J.M.; Jones, L.B.; Hinds, E.; Rusby, J.C.; Cody, C.; Sprague, J. The Role of Experiential Avoidance in the Relationship between Family Conflict and Depression among Early Adolescents. J. Contextual Behav. Sci. 2015, 4, 30–36. [Google Scholar] [CrossRef]
- Murrell, A.R.; Wilson, K.G.; LaBorde, C.T.; Drake, C.E.; Rogers, L.J. Relational Responding in Parents. Behav. Anal. Today 2008, 9, 196–214. [Google Scholar] [CrossRef] [Green Version]
- Coyne, L.W.; Wilson, K.G. The Role of Cognitive Fusion in Impaired Parenting: An RFT Analysis. Int. J. Psychol. Psychol. Ther. 2004, 4, 469–486. [Google Scholar]
- Brown, F.L.; Whittingham, K.; Sofronoff, K. Parental Experiential Avoidance as a Potential Mechanism of Change in a Parenting Intervention for Parents of Children With Pediatric Acquired Brain Injury. J. Pediatric Psychol. 2015, 40, 464–474. [Google Scholar] [CrossRef] [PubMed]
- Whittingham, K. Parenting in Context. J. Contextual Behav. Sci. 2014, 3, 212–215. [Google Scholar] [CrossRef]
- Paulus, D.J.; Vanwoerden, S.; Norton, P.J.; Sharp, C. Emotion Dysregulation, Psychological Inflexibility, and Shame as Explanatory Factors between Neuroticism and Depression. J. Affect. Disord. 2016, 190, 376–385. [Google Scholar] [CrossRef] [PubMed]
- Aldao, A.; Nolen-Hoeksema, S.; Schweizer, S. Emotion-Regulation Strategies across Psychopathology: A Meta-Analytic Review. Clin. Psychol. Rev. 2010, 30, 217–237. [Google Scholar] [CrossRef]
- Duncan, L.G.; Coatsworth, J.D.; Greenberg, M.T. A Model of Mindful Parenting: Implications for Parent-Child Relationships and Prevention Research. Clin. Child Fam. Psychol. Rev. 2009, 12, 255–270. [Google Scholar] [CrossRef] [Green Version]
- Eisenberg, N.; Losoya, S.; Fabes, R.A.; Guthrie, I.K.; Reiser, M.; Murphy, B.; Shepard, S.A.; Poulin, R.; Padgett, S.J. Parental Socialization of Children’s Dysregulated Expression of Emotion and Externalizing Problems. J. Fam. Psychol. 2001, 15, 183–205. [Google Scholar] [CrossRef] [PubMed]
- Moreira, H.; Canavarro, M.C. Mindful Parenting Is Associated with Adolescents’ Difficulties in Emotion Regulation Through Adolescents’ Psychological Inflexibility and Self-Compassion. J. Youth Adolesc. 2020, 49, 192–211. [Google Scholar] [CrossRef] [PubMed]
- Makriyianis, H.M.; Adams, E.A.; Lozano, L.L.; Mooney, T.A.; Morton, C.; Liss, M. Psychological Inflexibility Mediates the Relationship between Adverse Childhood Experiences and Mental Health Outcomes. J. Contextual Behav. Sci. 2019, 14, 82–89. [Google Scholar] [CrossRef]
- Hayes, S.C.; Villatte, M.; Levin, M.; Hildebrandt, M. Open, Aware, and Active: Contextual Approaches as an Emerging Trend in the Behavioral and Cognitive Therapies. Annu. Rev. Clin. Psychol. 2011, 7, 141–168. [Google Scholar] [CrossRef] [Green Version]
- Lozano-Rodríguez, I.; Valero-Aguayo, L. Una Revisión Sistemática de La Eficacia de Los Programas de Entrenamiento a Padres. Rev. Psicol Clínica Niños Adolesc. 2017, 4, 85–91. [Google Scholar]
- Robles, Z.; Romero, E. Programas de Entrenamiento Para Padres de Niños Con Problemas de Conducta: Una Revisión de Su Eficacia. An. Psicol. 2011, 27, 86–101. [Google Scholar]
- Heinrichs, N.; Bertram, H.; Kuschel, A.; Hahlweg, K. Parent Recruitment and Retention in a Universal Prevention Program for Child Behavior and Emotional Problems: Barriers to Research and Program Participation. Prev. Sci. 2005, 6, 275–286. [Google Scholar] [CrossRef] [PubMed]
- Nix, R.L.; Bierman, K.L.; McMahon, R.J. How Attendance and Quality of Participation Affect Treatment Response to Parent Management Training. J. Consult. Clin. Psychol. 2009, 77, 429–438. [Google Scholar] [CrossRef] [PubMed]
- Prinz, R.J.; Sanders, M.R. Adopting a Population-Level Approach to Parenting and Family Support Interventions. Clin. Psychol. Rev. 2007, 27, 739–749. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flujas-Contreras, J.M.; García-Palacios, A.; Gómez, I. Technology-Based Parenting Interventions for Children’s Physical and Psychological Health: A Systematic Review and Meta-Analysis. Psychol. Med. 2019, 49, 1787–1798. [Google Scholar] [CrossRef]
- Kazdin, A.E. Evidence-Based Treatment Research: Advances, Limitations, and next Steps. Am. Psychol. 2011, 66, 685. [Google Scholar] [CrossRef] [Green Version]
- Mohr, D.C.; Burns, M.N.; Schueller, S.M.; Clarke, G.; Klinkman, M. Behavioral Intervention Technologies: Evidence Review and Recommendations for Future Research in Mental Health. Gen. Hosp. Psychiatry 2013, 35, 332–338. [Google Scholar] [CrossRef] [Green Version]
- Vilardaga, R.; Bricker, J.B.; McDonell, M.G. The Promise of Mobile Technologies and Single Case Designs for the Study of Individuals in Their Natural Environment. J. Contextual Behav. 2014, 3, 148–153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holmes, E.A.; Ghaderi, A.; Harmer, C.J.; Ramchandani, P.G.; Cuijpers, P.; Morrison, A.P.; Roiser, J.P.; Bockting, C.L.H.; O’Connor, R.C.; Shafran, R.; et al. The Lancet Psychiatry Commission on Psychological Treatments Research in Tomorrow’s Science. Lancet Psychiatry 2018, 5, 237–286. [Google Scholar] [CrossRef] [Green Version]
- Funderburk, B.W.; Ware, L.M.; Altshuler, E.; Chaffin, M. Use and Feasibility of Telemedicine Technology in the Dissemination of Parent-Child Interaction Therapy. Child Maltreatment 2008, 13, 377–382. [Google Scholar] [CrossRef]
- Danebakc, C.; Platin, L. Research on Parenthood and the Internet: Themes and Trends. Cyberpsychology 2008, 2, 2. [Google Scholar]
- Nieuwboer, C.C.; Fukkink, R.G.; Hermanns, J.M.A. Online Programs as Tools to Improve Parenting: A Meta-Analytic Review. Child. Youth Serv. Rev. 2013, 35, 1823–1829. [Google Scholar] [CrossRef] [Green Version]
- Corralejo, S.M.; Domenech Rodríguez, M.M. Technology in Parenting Programs: A Systematic Review of Existing Interventions. J. Child Fam. Stud. 2018, 27, 2717–2731. [Google Scholar] [CrossRef]
- Breitenstein, S.M.; Gross, D.; Christophersen, R. Digital Delivery Methods of Parenting Training Interventions: A Systematic Review: Digital Delivery of Parent Training. Worldviews Evid. Based Nurs. 2014, 11, 168–176. [Google Scholar] [CrossRef]
- Breitenstein, S.M.; Fehrenbacher, C.; Holod, A.F.; Schoeny, M. A Randomized Trial of Digitally Delivered, Self-Administered Parent Training in Primary Care: Effects on Parenting and Child Behavior. J. Pediatrics 2020. [Google Scholar] [CrossRef] [PubMed]
- Suárez, A.; Byrne, S.; Rodrigo, M.J. Effectiveness of a Universal Web-Based Parenting Program to Promote Positive Parenting: Patterns and Predictors on Program Satisfaction. J. Child Fam. Stud. 2018, 27, 3345–3357. [Google Scholar] [CrossRef]
- Baumel, A.; Faber, K. Evaluating Triple P Online: A Digital Parent Training Program for Child Behavior Problems. Cogn. Behav. Pract. 2018, 25, 538–543. [Google Scholar] [CrossRef]
- Baker, S.; Sanders, M.R.; Turner, K.M.T.; Morawska, A. A Randomized Controlled Trial Evaluating a Low-Intensity Interactive Online Parenting Intervention, Triple P Online Brief, with Parents of Children with Early Onset Conduct Problems. Behav. Res. Ther. 2017, 91, 78–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sim, W.H.; Fernando, L.M.N.; Jorm, A.F.; Rapee, R.M.; Lawrence, K.A.; Mackinnon, A.J.; Yap, M.B.H. A Tailored Online Intervention to Improve Parenting Risk and Protective Factors for Child Anxiety and Depression: Medium-Term Findings from a Randomized Controlled Trial. J. Affect. Disord. 2020, 277, 814–824. [Google Scholar] [CrossRef]
- Ibañez, L.V.; Kobak, K.; Swanson, A.; Wallace, L.; Warren, Z.; Stone, W.L. Enhancing Interactions during Daily Routines: A Randomized Controlled Trial of a Web-Based Tutorial for Parents of Young Children with ASD: A Parenting Tutorial for Daily Routines. Autism Res. 2018, 11, 667–678. [Google Scholar] [CrossRef]
- Phipps, S.; Fairclough, D.L.; Noll, R.B.; Devine, K.A.; Dolgin, M.J.; Schepers, S.A.; Askins, M.A.; Schneider, N.M.; Ingman, K.; Voll, M.; et al. In-Person vs. Web-Based Administration of a Problem-Solving Skills Intervention for Parents of Children with Cancer: Report of a Randomized Noninferiority Trial. EClinicalMedicine 2020, 24, 100428. [Google Scholar] [CrossRef]
- Hayes, S.C.; Strosahl, K.; Wilson, K.G. Acceptance and Commitment Therapy The Process and Practice of Mindful Change; Guilford Press: New York, NY, USA, 2012; ISBN 978-1-60918-962-4. [Google Scholar]
- Linehan, M. Cognitive-Behavioral Treatment of Borderline Personality Disorder; Guilford Press: New York, NY, USA, 1993; ISBN 978-0-89862-183-9. [Google Scholar]
- Segal, Z.V.; Williams, J.M.G.; Teasdale, J.D. Mindfulness-Based Cognitive Therapy for Depression: A New Approach to Preventing Relapse; Guilford Press: New York, NY, USA, 2002; ISBN 1-57230-706-4. [Google Scholar]
- Byrne, G.; Ghráda, Á.N.; O’Mahony, T.; Brennan, E. A Systematic Review of the Use of Acceptance and Commitment Therapy in Supporting Parents. Psychol. Psychother. Theory Res. Pract. 2020, 13, e12282. [Google Scholar] [CrossRef] [PubMed]
- Bögels, S.M.; Hellemans, J.; van Deursen, S.; Römer, M.; van der Meulen, R. Mindful Parenting in Mental Health Care. Mindfulness 2014, 5, 536–551. [Google Scholar] [CrossRef]
- Rayan, A.; Ahmad, M. Mindfulness and Parenting Distress among Parents of Children with Disabilities: A Literature Review. Perspect. Psychiatr. Care 2018, 54, 324–330. [Google Scholar] [CrossRef]
- Van der Oord, S.; Bögels, S.M.; Peijnenburg, D. The Effectiveness of Mindfulness Training for Children with ADHD and Mindful Parenting for Their Parents. J. Child Fam. Stud. 2012, 21, 139–147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harnett, P.H.; Dawe, S. The Contribution of Mindfulness-Based Therapies for Children and Families and Proposed Conceptual Integration. Child Adolesc. Ment. Health 2012, 17, 195–208. [Google Scholar] [CrossRef] [PubMed]
- Zalewski, M.; Maliken, A.C.; Lengua, L.J.; Gamache Martin, C.; Roos, L.E.; Everett, Y. Integrating Dialectical Behavior Therapy with Child and Parent Training Interventions: A Narrative and Theoretical Review. Clin. Psychol. Sci. Pract. 2020, e12363. [Google Scholar] [CrossRef]
- MacPherson, H.A.; Cheavens, J.S.; Fristad, M.A. Dialectical Behavior Therapy for Adolescents: Theory, Treatment Adaptations, and Empirical Outcomes. Clin. Child Fam. Psychol. Rev. 2013, 16, 59–80. [Google Scholar] [CrossRef] [PubMed]
- Perepletchikova, F.; Nathanson, D.; Axelrod, S.R.; Merrill, C.; Walker, A.; Grossman, M.; Rebeta, J.; Scahill, L.; Kaufman, J.; Flye, B.; et al. Randomized Clinical Trial of Dialectical Behavior Therapy for Preadolescent Children With Disruptive Mood Dysregulation Disorder: Feasibility and Outcomes. J. Am. Acad. Child Adolesc. Psychiatry 2017, 56, 832–840. [Google Scholar] [CrossRef] [PubMed]
- Sairanen, E.; Lappalainen, R.; Lappalainen, P.; Kaipainen, K.; Carlstedt, F.; Anclair, M.; Hiltunen, A. Effectiveness of a Web-Based Acceptance and Commitment Therapy Intervention for Wellbeing of Parents Whose Children Have Chronic Conditions: A Randomized Controlled Trial. J. Contextual Behav. Sci. 2019, 13, 94–102. [Google Scholar] [CrossRef]
- Pennefather, J.; Hieneman, M.; Raulston, T.J.; Caraway, N. Evaluation of an Online Training Program to Improve Family Routines, Parental Well-Being, and the Behavior of Children with Autism. Res. Autism Spectr. Disord. 2018, 54, 21–26. [Google Scholar] [CrossRef]
- Yang, M.; Jia, G.; Sun, S.; Ye, C.; Zhang, R.; Yu, X. Effects of an Online Mindfulness Intervention Focusing on Attention Monitoring and Acceptance in Pregnant Women: A Randomized Controlled Trial. J. Midwifery Women’s Health 2019, 64, 68–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flujas-Contreras, J.M.; García-Palacios, A.; Gómez, I. Intervención en flexibilidad parental a través de una intervención grupal en familias. Behav. Psychol. 2020, 28, 25–57. [Google Scholar]
- Eldridge, S.M.; Chan, C.L.; Campbell, M.J.; Bond, C.M.; Hopewell, S.; Thabane, L.; Lancaster, G.A. CONSORT 2010 Statement: Extension to Randomised Pilot and Feasibility Trials. BMJ 2016, 355, i5239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lancaster, G.A.; Thabane, L. Guidelines for Reporting Non-Randomised Pilot and Feasibility Studies. Pilot Feasibility Stud. 2019, 5, 114. [Google Scholar] [CrossRef]
- Flujas-Contreras, J.M.; García-Palacios, A.; Gómez, I. Spanish Validation of the Parental Acceptance Questionnaire (6-PAQ). Int. J. Clin. Health Psychol. 2020, 20, 163–172. [Google Scholar] [CrossRef]
- Español-Martín, G.; Pagerols, M.; Prat, R.; Rivas, C.; Sixto, L.; Valero, S.; Artigas, M.S.; Ribasés, M.; Ramos-Quiroga, J.A.; Casas, M.; et al. Strengths and Difficulties Questionnaire: Psychometric Properties and Normative Data for Spanish 5- to 17-Year-Olds. Assessment 2020. [Google Scholar] [CrossRef]
- Whitehead, A.L.; Julious, S.A.; Cooper, C.L.; Campbell, M.J. Estimating the Sample Size for a Pilot Randomised Trial to Minimise the Overall Trial Sample Size for the External Pilot and Main Trial for a Continuous Outcome Variable. Stat. Methods Med. Res. 2016, 25, 1057–1073. [Google Scholar] [CrossRef] [PubMed]
- Julious, S.A. Sample Size of 12 per Group Rule of Thumb for a Pilot Study. Pharm. Stat. 2005, 4, 287–291. [Google Scholar] [CrossRef]
- LabPsiTec Psicología y Tecnología. Available online: https://psicologiaytecnologia.labpsitec.es/ (accessed on 24 December 2020).
- González-Robles, A.; Díaz-García, A.; García-Palacios, A.; Roca, P.; Ramos-Quiroga, J.A.; Botella, C. Effectiveness of a Transdiagnostic Guided Internet-Delivered Protocol for Emotional Disorders Versus Treatment as Usual in Specialized Care: Randomized Controlled Trial. J. Med. Internet Res. 2020, 22, e18220. [Google Scholar] [CrossRef] [PubMed]
- Ben-Porath, D.D. Dialectical Behavior Therapy Applied to Parent Skills Training: Adjunctive Treatment for Parents with Difficulties in Affect Regulation. Cog. Behav. Pract. 2010, 17, 458–465. [Google Scholar] [CrossRef]
- Gómez, I.; Hódar, J.C.; Barranco, M.R.G. Intervención en valores con familias de riesgo social desde la Terapia de Aceptación y Compromiso. Análisis Modif. Conducta 2012, 38, 20. [Google Scholar] [CrossRef] [Green Version]
- Hayes, S.C.; Strosahl, K.D.; Wilson, K.G. Acceptance and Commitment Therapy: An Experiential Approach to Behavior Change; Guilford Press: New York, NY, USA, 1999. [Google Scholar]
- Linehan, M. DBT Skills Training Manual; Guilford Press: New York, NY, USA, 2014; ISBN 978-1-4625-1699-5. [Google Scholar]
- Whittingham, K. Connect and Shape: A Parenting Meta-Strategy. J. Contextual Behav. Sci. 2015, 4, 103–106. [Google Scholar] [CrossRef]
- Gómez, I.; de Salazar, A.M.; Barranco, R.G.; Cobos, L.; Filippo, C. Validación Del Cuestionario de Estilos Educativos Parentales: Estudio Piloto. In Proceedings of the II Symposium Nacional de Psicología Clínica y de la Salud con Niños y Adolescentes, Elche, Spain, 21 November 2012. [Google Scholar]
- Greene, R.L.; Field, C.E.; Fargo, J.D.; Twohig, M.P. Development and Validation of the Parental Acceptance Questionnaire (6-PAQ). J. Contextual Behav. Sci. 2015, 4, 170–175. [Google Scholar] [CrossRef]
- Bond, F.W.; Hayes, S.C.; Baer, R.A.; Carpenter, K.M. Preliminary Psychometric Properties of the Acceptance and Action Questionnaire–II: A Revised Measure of Psychological Inflexibility and Experiential Avoidance. Behav. Ther. 2001, 42, 676–688. [Google Scholar] [CrossRef] [Green Version]
- Ruiz, F.J.; Herrera, A.I.L.; Luciano, C.; Cangas, A.J.; Beltran, I. Measuring Experiential Avoidance and Psychological Inflexibility: The Spanish Version of the Acceptance and Action Questionnaire—II. Psicothema 2013, 25, 123–129. [Google Scholar] [CrossRef] [PubMed]
- Gratz, K.L.; Roemer, L. Multidimensional Assessment of Emotion Regulation and Dysregulation: Development, Factor Structure, and Initial Validation of the Difficulties in Emotion Regulation Scale. J. Psychopathol. Beh. Assess. 2004, 26, 41–54. [Google Scholar] [CrossRef]
- Hervás, G.; Jódar, R. Adaptación al Castellano de La Escala de Dificultades En La Regulación Emocional The Spanish Version of the Difficulties in Emotion Regulation Scale. Clínica Salud 2008, 19, 139–156. [Google Scholar] [CrossRef] [Green Version]
- Berry, J.O.; Jones, W.H. The Parental Stress Scale: Initial Psychometric Evidence. J. Soc. Pers. Relatsh. 1995, 12, 463–472. [Google Scholar] [CrossRef]
- Oronoz, B.; Alonso-Arbiol, I.; Balluerka, N. A Spanish Adaptation of the Parental Stress Scale. Psicothema 2007, 19, 687–692. [Google Scholar] [PubMed]
- Diener, E.; Emmons, R.A.; Larsem, R.J.; Griffin, S. The Satisfaction With Life Scale. J. Pers. Assess. 1985, 49, 71–75. [Google Scholar] [CrossRef] [PubMed]
- Vázquez, C.; Duque, A.; Hervás, G. Satisfaction with Life Scale in a Representative Sample of Spanish Adults: Validation and Normative Data. Span. J. Psychol. 2013, 16, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Palacios, A.; Herrero, R.; Belmonte, M.A.; Castilla, D.; Guixeres, J.; Molinari, G.; Baños, R.M.; Botella, C. Ecological Momentary Assessment for Chronic Pain in Fibromyalgia Using a Smartphone: A Randomized Crossover Study. Eur. J. Pain 2014, 18, 862–872. [Google Scholar] [CrossRef] [Green Version]
- Goodman, R. Psychometric Properties of the Strengths and Difficulties Questionnaire. J. Am. Acad. Child Adolesc. Psychiatry 2001, 40, 1337–1345. [Google Scholar] [CrossRef] [PubMed]
- Larsen, D.L.; Attkisson, C.C.; Hargreaves, W.A.; Nguyen, T.D. Assessment of Client/Patient Satisfaction: Development of a General Scale. Eval. Program Plan. 1979, 2, 197–207. [Google Scholar] [CrossRef]
- Roberts, R.E.; Attkisson, C.C. Assessing Client Satisfaction among Hispanics. Eval. Program Plan. 1983, 6, 401–413. [Google Scholar] [CrossRef]
- Jamovi. Available online: https://www.jamovi.org/ (accessed on 26 December 2020).
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Academic Press: New York, NY, USA, 1988. [Google Scholar]
- Jacobson, N.S.; Truax, P. Clinical Significance: A Statistical Approach to Defining Meaningful Change in Psychotherapy Research. J. Consult. Clin. Psychol. Psychology 1991, 59, 12–19. [Google Scholar] [CrossRef]
- Cederberg, J.T.; Cernvall, M.; Dahl, J.; von Essen, L.; Ljungman, G. Acceptance as a Mediator for Change in Acceptance and Commitment Therapy for Persons with Chronic Pain? Int. J. Behav. Med. 2016, 23, 21–29. [Google Scholar] [CrossRef] [PubMed]
- Hesser, H.; Westin, V.Z.; Andersson, G. Acceptance as a Mediator in Internet-Delivered Acceptance and Commitment Therapy and Cognitive Behavior Therapy for Tinnitus. J. Behav. Med. 2014, 37, 756–767. [Google Scholar] [CrossRef]
- Weiss, J.A.; Cappadocia, M.C.; MacMullin, J.A.; Viecili, M.; Lunsky, Y. The Impact of Child Problem Behaviors of Children with ASD on Parent Mental Health: The Mediating Role of Acceptance and Empowerment. Autism 2012, 16, 261–274. [Google Scholar] [CrossRef] [Green Version]
- Martin, C.G.; Roos, L.E.; Zalewski, M.; Cummins, N. A Dialectical Behavior Therapy Skills Group Case Study on Mothers With Severe Emotion Dysregulation. Cogn. Behav. Pract. 2017, 24, 405–415. [Google Scholar] [CrossRef]
- Gershy, N.; Meehan, K.B.; Omer, H.; Papouchis, N.; Sapir, I.S. Randomized Clinical Trial of Mindfulness Skills Augmentation in Parent Training. Child Youth Care Forum 2017, 46, 783–803. [Google Scholar] [CrossRef]
- Haydicky, J.; Wiener, J.; Shecter, C. Mechanisms of Action in Concurrent Parent-Child Mindfulness Training: A Qualitative Exploration. Mindfulness 2017, 8, 1018–1035. [Google Scholar] [CrossRef]
- Anderson, S.; Guthery, A. Mindfulness-Based Psychoeducation for Parents of Children with Attention-Deficit/Hyperactivity Disorder: An Applied Clinical Project. J. Child Adolesc. Psychiatr. Nurs. 2015, 28, 43–49. [Google Scholar] [CrossRef] [PubMed]
- Bazzano, A.; Wolfe, C.; Zylowska, L.; Wang, S.; Schuster, E.; Barrett, C.; Lehrer, D. Mindfulness Based Stress Reduction (MBSR) for Parents and Caregivers of Individuals with Developmental Disabilities: A Community-Based Approach. J. Child Fam. Stud. 2015, 24, 298–308. [Google Scholar] [CrossRef]
- Dykens, E.M.; Fisher, M.H.; Taylor, J.L.; Lambert, W.; Miodrag, N. Reducing Distress in Mothers of Children With Autism and Other Disabilities: A Randomized Trial. Pediatrics 2014, 134, e454–e463. [Google Scholar] [CrossRef] [Green Version]
- Hwang, Y.S.; Kearney, P.; Klieve, H.; Lang, W.; Roberts, J. Cultivating Mind: Mindfulness Interventions for Children with Autism Spectrum Disorder and Problem Behaviours, and Their Mothers. J. Child Fam. Stud. 2015, 24, 3093–3106. [Google Scholar] [CrossRef]
- Sairanen, E.; Lappalainen, R.; Lappalainen, P.; Hiltunen, A. Mediators of Change in Online Acceptance and Commitment Therapy for Psychological Symptoms of Parents of Children with Chronic Conditions: An Investigation of Change Processes. J. Contextual Behav. Sci. 2020, 15, 123–130. [Google Scholar] [CrossRef]
- Jones, S.H.; Jovanoska, J.; Calam, R.; Wainwright, L.D.; Vincent, H.; Asar, O.; Diggle, P.J.; Parker, R.; Long, R.; Sanders, M.; et al. Web-Based Integrated Bipolar Parenting Intervention for Parents with Bipolar Disorder: A Randomised Controlled Pilot Trial. J. Child Psychol. Psychiatr. 2017, 58, 1033–1041. [Google Scholar] [CrossRef]
- Bögels, S.; Hoogstad, B.; van Dun, L.; de Schutter, S.; Restifo, K. Mindfulness Training for Adolescents with Externalizing Disorders and Their Parents. Behav. Cogn. Psychother. 2008, 36, 193–209. [Google Scholar] [CrossRef] [Green Version]
- Coatsworth, J.D.; Duncan, L.G.; Greenberg, M.T.; Nix, R.L. Changing Parent’s Mindfulness, Child Management Skills and Relationship Quality with Their Youth: Results from a Randomized Pilot Intervention Trial. J. Child Fam. Stud. 2010, 19, 203–217. [Google Scholar] [CrossRef] [Green Version]
- Uliaszek, A.A.; Wilson, S.; Mayberry, M.; Cox, K.; Maslar, M. A Pilot Intervention of Multifamily Dialectical Behavior Group Therapy in a Treatment-Seeking Adolescent Population: Effects on Teens and Their Family Members. Fam. J. 2014, 22, 206–215. [Google Scholar] [CrossRef]
- Gómez-Becerra, I.; Flujas, J.M.; Andrés, M.; Sánchez-López, P. Evolución del estado psicológico y el miedo en la infancia y adolescencia durante el confinamiento por la COVID-19. Rev. Psicol. Clínica Niños Adolesc. 2020, 7, 11–18. [Google Scholar]
- Heifetz, M.; Dyson, A. Mindfulness-Based Group for Teens with Developmental Disabilities and Their Parents: A Pilot Study. Mindfulness 2017, 8, 444–453. [Google Scholar] [CrossRef]
- Gould, E.R.; Tarbox, J.; Coyne, L. Evaluating the Effects of Acceptance and Commitment Training on the Overt Behavior of Parents of Children with Autism. J. Contextual Behav. Sci. 2018, 7, 81–88. [Google Scholar] [CrossRef]
- Chase, J.A.; Houmanfar, R.; Hayes, S.C.; Ward, T.A.; Vilardaga, J.P.; Follette, V. Values Are Not Just Goals: Online ACT-Based Values Training Adds to Goal Setting in Improving Undergraduate College Student Performance. J. Contextual Behav. Sci. 2013, 2, 79–84. [Google Scholar] [CrossRef]
- Firestone, J.; Cardaciotto, L.; Levin, M.E.; Goldbacher, E.; Vernig, P.; Gambrel, L.E. A Web-Based Self-Guided Program to Promote Valued-Living in College Students: A Pilot Study. J. Contextual Behav. Sci. 2019, 12, 29–38. [Google Scholar] [CrossRef]
- Sveen, J.; Andersson, G.; Ekselius, L.; Sjöberg, F.; Buhrman, B.; Willebrand, M. Internet-Based Information and Self-Help Program for Parents of Children with Burns: Study Protocol for a Randomized Controlled Trial. Internet Interv. 2015, 2, 367–371. [Google Scholar] [CrossRef] [Green Version]
- Gonzalez, C.; Morawska, A.; Haslam, D.M. A Model of Intention to Participate in Parenting Interventions: The Role of Parent Cognitions and Behaviours. Behav. Ther. 2020. [Google Scholar] [CrossRef]



| Parent | Children | 6-PAQ Parents Characteristics at Pre-Test | SDQ Children Characteristics at Pre-Test | |
|---|---|---|---|---|
| 1 | 42 (f) | 10 (f) 7 (f) | ↑ parental psychological inflexibility; ↓ acceptance; ↓ commitment | ↑ SDQ score; ± emotional, ↑behavioral, ± hyperactivity, ↑peer, ↓ prosocial |
| 2 | 37 (f) | 8 (f) | ↑ parental psychological inflexibility; ↓ acceptance; ↓commitment | ↑ SDQ score; ↑ behavioral, ±hyperactivity, ↑ peer, ↓ prosocial |
| 3 | 43 (f) | 10 (m) 7 (f) | ↑ parental psychological inflexibility; ↓ acceptance; ↓awareness | ↑ SDQ score; ↑ emotional, ↑behavioral, ↑ hyperactivity, ↑peer, ↓ prosocial |
| 4 | 37 (f) | 3 (m) | ± parental psychological inflexibility; ↓ acceptance; ↓awareness | ↑ SDQ score; ± emotional, ↑behavioral, ± hyperactivity, ↑peer, ± prosocial |
| 5 | 42 (f) | 9 (m) 6 (m) | ↑ parental psychological inflexibility; ↓ acceptance; ↓commitment | ↑ SDQ score; ± emotional, ±peer./ADHD diagnosis < 6 months |
| 6 | 36 (f) | 9 (f) 13 (m) | ↑ parental psychological inflexibility; ↓ acceptance; ↓awareness | ↑ SDQ score; ↑ emotional, ↑behavioral, ↑ hyperactivity ADHD diagnosis > 1 year |
| 7 | 40 (f) | 7 (m) 3 (m) | - | ↑ SDQ score; ± behavioral, ↑ peer |
| 8 | 45 (m) | 10 (m) 7 (m) | ↑ parental psychological inflexibility | ↑ SDQ score; ↑ emotional, ↑behavioral, ± prosocial |
| 9 | 43 (m) | 8 (m) 5 (m)/5 (f) | - | ↑ SDQ score; ↑ emotional, ↑behavioral, ↑ peer |
| 10 | 50 (f) | 15 (m) 13 (m) | - | ↑ SDQ score; ↑ emotional |
| 11 | 42 (f) | 10 (f) | - | ↑ SDQ score; ↑ emotional, ±behavioral, ± peer, ± prosocial |
| 12 | 36 (f) | 8 (m) 4 (f) | ↑ parental psychological inflexibility; ↓ awareness | ↑ SDQ score; ↑ emotional, ↑behavioral, ± hyperactivity, ↓prosocial |
| Pre-Treatment (n = 12) | Post-Treatment (n = 12) | Wilcoxon Z | p | Cohen’s d | |||
|---|---|---|---|---|---|---|---|
| M | SD | M | SD | ||||
| Primary parental outcomes | |||||||
| 6-PAQ | 32.50 | 6.69 | 26.92 | 5.32 | 78.0 | 0.002 * | 1.43 |
| Open | 11.17 | 3.13 | 8.67 | 1.92 | 50.5 | 0.021 * | 0.91 |
| Aware | 12.42 | 3.00 | 10.00 | 2.73 | 45.0 | 0.009 ** | 1.39 |
| Commitment | 8.92 | 1.83 | 8.25 | 2.67 | 33.5 | 0.208 | 0.29 |
| AAQ-II | 23.17 | 7.87 | 19.33 | 8.76 | 49.5 | 0.154 | 0.49 |
| DERS | 66.00 | 24.73 | 57.33 | 18.33 | 53.5 | 0.272 | 0.38 |
| Attention | 8.58 | 3.92 | 8.58 | 2.50 | 24.0 | 0.905 | 0.00 |
| Clarity | 7.50 | 2.24 | 7.42 | 2.47 | 38.0 | 0.684 | 0.03 |
| Acceptance | 18.58 | 8.46 | 14.25 | 6.59 | 62.0 | 0.076 † | 0.57 |
| Goals | 11.17 | 4.32 | 9.92 | 4.68 | 45.0 | 0.304 | 0.29 |
| Strategies | 20.17 | 9.01 | 17.17 | 6.16 | 36.0 | 0.414 | 0.33 |
| PSS | 32.75 | 7.21 | 30.67 | 8.07 | 50.0 | 0.141 | 0.27 |
| Rewards | 8.92 | 3.40 | 7.83 | 2.82 | 44.5 | 0.089 † | 0.56 |
| Stressors | 23.83 | 5.57 | 22.83 | 5.77 | 34.0 | 0.540 | 0.15 |
| SWL | 23.25 | 7.94 | 25.08 | 5.58 | 27.0 | 0.365 | 0.31 |
| Children outcomes (reported by parents) | |||||||
| SDQ | 23.75 | 6.97 | 23.25 | 6.82 | 23.5 | 0.478 | 0.16 |
| Emotional sx. | 4.00 | 2.41 | 3.58 | 2.27 | 28.0 | 0.545 | 0.24 |
| Behavior prob. | 4.83 | 2.72 | 3.75 | 2.80 | 28.0 | 0.018 * | 0.71 |
| Hyperactivity | 4.75 | 3.14 | 5.25 | 3.49 | 15.5 | 0.433 | 0.28 |
| Peers prob. | 3.50 | 3.29 | 3.08 | 3.34 | 16.0 | 0.281 | 0.35 |
| Prosocial | 6.67 | 2.93 | 7.58 | 2.68 | .003 | 0.034 * | 0.84 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Flujas-Contreras, J.M.; García-Palacios, A.; Gómez, I. Effectiveness of a Web-Based Intervention on Parental Psychological Flexibility and Emotion Regulation: A Pilot Open Trial. Int. J. Environ. Res. Public Health 2021, 18, 2958. https://doi.org/10.3390/ijerph18062958
Flujas-Contreras JM, García-Palacios A, Gómez I. Effectiveness of a Web-Based Intervention on Parental Psychological Flexibility and Emotion Regulation: A Pilot Open Trial. International Journal of Environmental Research and Public Health. 2021; 18(6):2958. https://doi.org/10.3390/ijerph18062958
Chicago/Turabian StyleFlujas-Contreras, Juan M., Azucena García-Palacios, and Inmaculada Gómez. 2021. "Effectiveness of a Web-Based Intervention on Parental Psychological Flexibility and Emotion Regulation: A Pilot Open Trial" International Journal of Environmental Research and Public Health 18, no. 6: 2958. https://doi.org/10.3390/ijerph18062958
APA StyleFlujas-Contreras, J. M., García-Palacios, A., & Gómez, I. (2021). Effectiveness of a Web-Based Intervention on Parental Psychological Flexibility and Emotion Regulation: A Pilot Open Trial. International Journal of Environmental Research and Public Health, 18(6), 2958. https://doi.org/10.3390/ijerph18062958