
A Significant Decrease in the Incidence of Shigellosis in Israel during COVID-19 Pandemic


Abstract
:1. Introduction
2. Materials and Methods
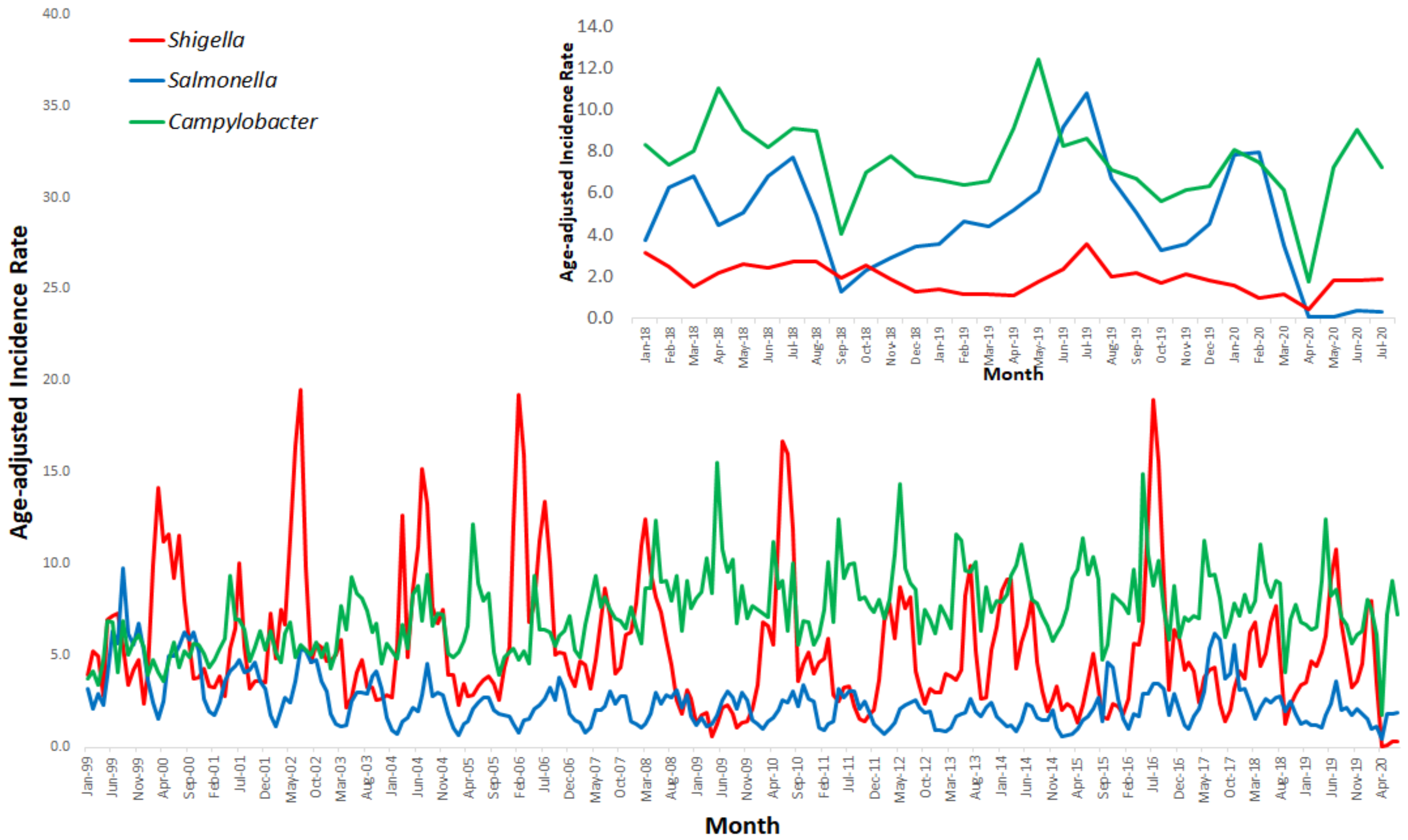
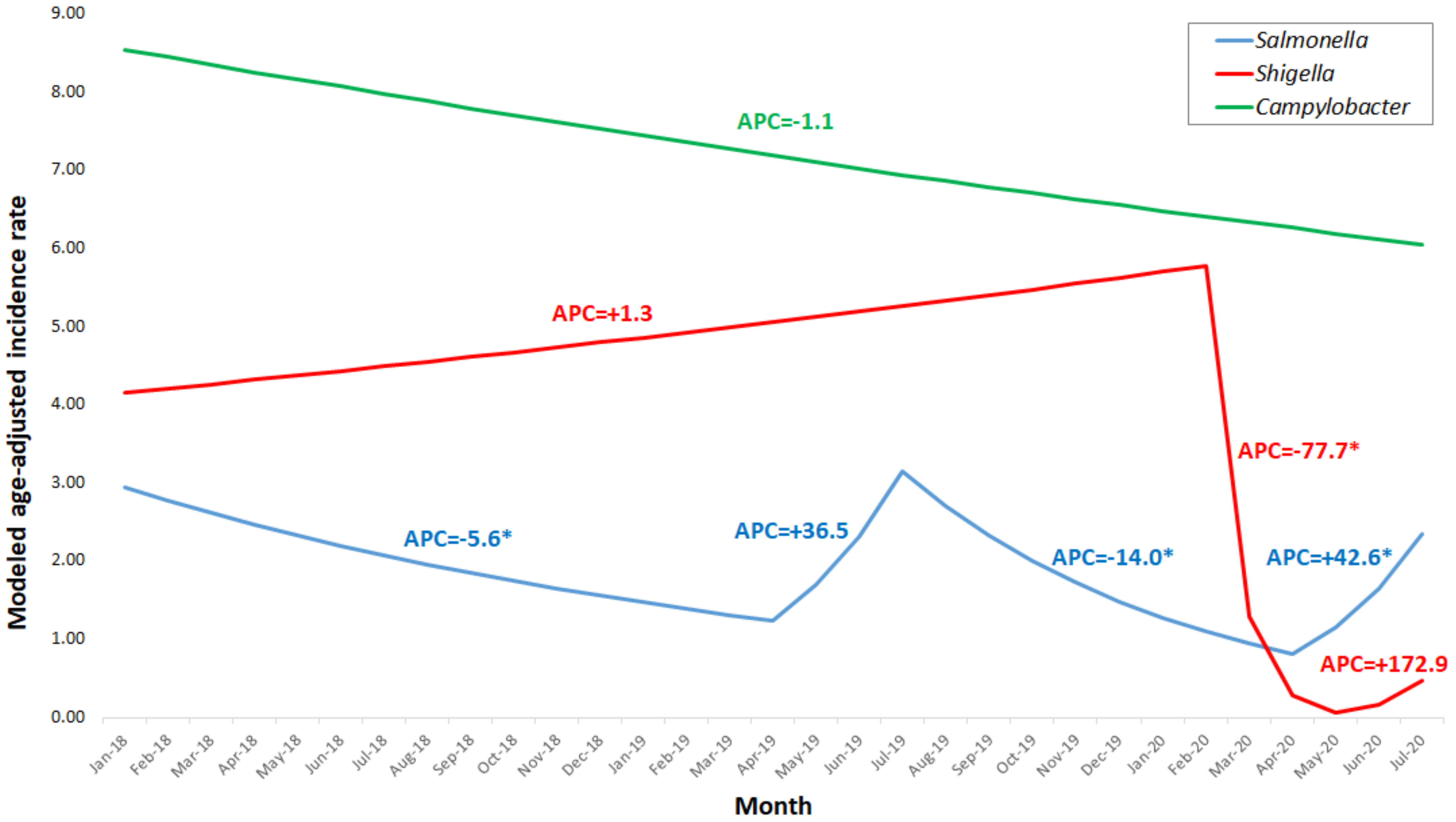
3. Results
4. Discussion
- Social distancing is important in general in reducing the possibility of contact (shaking hands, touching fomites) which can enhance transmission of both respiratory and enteric pathogens such as SARS-CoV-2 and Shigella, respectively.
- Hand hygiene, including washing hands with soap or using alcogel if washing is not possible, may prevent direct and indirect transmission of both SARS-CoV-2 and Shigella [7,8]. Khan et al. and Cohen et al. have shown that hand washing was inversely associated with the occurrence of Shigella, even in insanitary environments [7,8].
- Environmental transmission of Shigella through fomites is highly applicable due to the low infectious dose required. Following the COVID-19 outbreak, the public awareness of fomite and surface sanitation increased dramatically, thus reducing the probability to be contaminated with Shigella.
- Non-coronavirus patients avoided visiting their physician out of fear of contracting COVID-19, either from a healthcare worker or from a patient visiting the clinic. In Canada, a decrease observed in clinic visits due to code strokes was mainly associated with fear of being exposed to the SARS-CoV-2 but also with clinic referrals which were largely explained by hospital policies and the governmental lockdown [9]. The striking decrease observed in the incidence rate of shigellosis cannot be explained solely by the avoidance of visiting the clinic since we could expect a similar quantitative reduction in the incidence rate of both salmonellosis and campylobacteriosis, which was not observed. Thus, the reduction observed seems to reflect a truly lower rate of infection.
- During the COVID-19 outbreak, doctor appointments were mostly performed by phone or video call. It has been shown that remote consultations effectively reduced the burden on hospitals, prevented overcrowding, reduced the risk of cross-infection, relieved patients’ anxiety during the COVID-19 outbreak and played an essential role in pandemic management [10]. However, physicians were less capable to clinically diagnose shigellosis and were less likely to send stool samples to the laboratory for confirmation. Since we count on data received from sentinel laboratories on isolates of Shigella, less available stool samples could have also contributed to the decrease in the incidence rate of culture-proven shigellosis, but this cannot be the sole explanation since a similarly enhanced decrease in culture-proven salmonellosis and campylobacteriosis could also have been expected.
- The clinical laboratories equipment and personnel were all dedicated to testing for SARS-CoV2, and the option of neglecting other specimens testing cannot be ruled out. However, one could expect that the decrease observed in the identification of Shigella should have also been observed in the identification of Salmonella and Campylobacter, which was not the case.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Liu, J.; Liao, X.; Qian, S.; Yuan, J.; Wang, F.; Liu, Y.; Wang, Z.; Wang, F.S.; Liu, L.; Zhang, Z. Community Transmission of Severe Acute Respiratory Syndrome Coronavirus 2, Shenzhen, China, 2020. Emerg. Infect. Dis. 2020, 26, 1320–1323. [Google Scholar] [CrossRef]
- Chan, J.F.; Yuan, S.; Kok, K.H.; To, K.K.; Chu, H.; Yang, J.; Xing, F.; Liu, J.; Yip, C.C.; Poon, R.W.; et al. A familial cluster of pneumonia associated with the 2019 novel coronavirus indicating person-to-person transmission: A study of a family cluster. Lancet 2020, 395, 514–523. [Google Scholar] [CrossRef] [Green Version]
- Modes of Transmission of Virus Causing COVID-19: Implications for IPC Precaution Recommendations. Available online: https://www.who.int/news-room/commentaries/detail/modes-of-transmission-of-virus-causing-covid-19-implications-for-ipc-precaution-recommendations (accessed on 4 February 2021).
- Centers for Disease Control and Prevention, National Center for Zoonotic and Emerging Infectious Diseases, Division of Foodborne, Waterborne, and Environmental Diseases (DFWED). Shigellosis. Available online: https://www.cdc.gov/shigella/index.html (accessed on 4 February 2021).
- The Centers for Disease Control and Prevention (CDC). Shigellosis. In The Yellow Book, Health Information for International Travel 2020; Oxford University Press: Oxford, UK, 2020. [Google Scholar]
- Cohen, D.; Bassal, R.; Goren, S.; Rouach, T.; Taran, D.; Schemberg, B.; Peled, N.; Keness, Y.; Ken-Dror, S.; Vasilev, V.; et al. Recent trends in the epidemiology of shigellosis in Israel. Epidemiol. Infect. 2014, 142, 2583–2594. [Google Scholar] [CrossRef] [Green Version]
- Khan, M.U. Interruption of shigellosis by hand washing. Trans. R Soc. Trop. Med. Hyg. 1982, 76, 164–168. [Google Scholar] [CrossRef]
- Cohen, D.; Korin, H.; Bassal, R.; Perry Markovich, M.; Sivan, Y.; Goren, S.; Muhsen, K. Burden and risk factors of Shigella sonnei shigellosis among children aged 0-59 months in hyperendemic communities in Israel. Int. J. Infect. Dis. 2019, 82, 117–123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bres Bullrich, M.; Fridman, S.; Mandzia, J.L.; Mai, L.M.; Khaw, A.; Vargas Gonzalez, J.C.; Bagur, R.; Sposato, L.A. COVID-19: Stroke Admissions, Emergency Department Visits, and Prevention Clinic Referrals. Can. J. Neurol. Sci. 2020, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Gu, J.; Shao, F.; Liang, X.; Yue, L.; Cheng, Q.; Zhang, L. Application and Preliminary Outcomes of Remote Diagnosis and Treatment During the COVID-19 Outbreak: Retrospective Cohort Study. JMIR Mhealth Uhealth 2020, 8, e19417. [Google Scholar] [CrossRef] [PubMed]
- Bassal, R.; Reisfeld, A.; Andorn, N.; Yishai, R.; Nissan, I.; Agmon, V.; Peled, N.; Block, C.; Keller, N.; Kenes, Y.; et al. Recent trends in the epidemiology of non-typhoidal Salmonella in Israel, 1999–2009. Epidemiol. Infect. 2012, 140, 1446–1453. [Google Scholar] [CrossRef] [PubMed]
- Bassal, R.; Lerner, L.; Valinsky, L.; Agmon, V.; Peled, N.; Block, C.; Keller, N.; Keness, Y.; Taran, D.; Shainberg, B.; et al. Trends in the Epidemiology of Campylobacteriosis in Israel (1999–2012). Foodborne Pathog. Dis. 2016, 13, 448–455. [Google Scholar] [CrossRef] [PubMed]
- Yu, X.; Wei, D.; Chen, Y.; Zhang, D.; Zhang, X. Retrospective detection of SARS-CoV-2 in hospitalized patients with influenza-like illness. Emerg. Microbes Infect. 2020, 9, 1470–1473. [Google Scholar] [CrossRef] [PubMed]
- Mutnal, M.B.; Arroliga, A.C.; Walker, K.; Mohammad, A.; Brigmon, M.M.; Beaver, R.M.; Midturi, J.K.; Rao, A. Early trends for SARS-CoV-2 infection in central and north Texas and impact on other circulating respiratory viruses. J. Med. Virol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Angoulvant, F.; Ouldali, N.; Yang, D.D.; Filser, M.; Gajdos, V.; Rybak, A.; Guedj, R.; Soussan-Banini, V.; Basmaci, R.; Lefevre-Utile, A.; et al. COVID-19 pandemic: Impact caused by school closure and national lockdown on pediatric visits and admissions for viral and non-viral infections, a time series analysis. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Salmonellosis | Shigellosis | Campylobacteriosis | |||||
|---|---|---|---|---|---|---|---|
| 95%CI € | 95%CI € | 95%CI € | |||||
| March–July 2018–2019 | aaIR £ | 2.1 | 1.6–2.7 | 6.7 | 5.2–8.2 | 9.0 | 7.9–10.2 |
| March–July 2020 | aaIR £ | 1.4 | 0.6–2.2 | 0.9 | 0.0–2.7 | 6.3 | 2.9–9.7 |
| RR | 0.67 | 0.08–5.66 | 0.13 | 0.01–1.21 | 0.70 | 0.25–1.94 | |
| RRR ¥ (%) | 33.0 | 86.6 | 30.0 | ||||
| Period No. | Start Month | MAAIR ¥ per 100,000 | End Month | MAAIR ¥ per 100,000 | APC £ | p-Value |
|---|---|---|---|---|---|---|
| Salmonellosis | ||||||
| 1 | January 2018 | 2.94 | April 2019 | 1.24 | −5.6 | 0.000252 |
| 2 | April 2019 | 1.24 | July 2019 | 3.15 | 36.5 | 0.321872 |
| 3 | July 2019 | 3.15 | April 2020 | 0.81 | −14.0 | 0.000212 |
| 4 | April 2020 | 0.81 | July 2020 | 2.35 | 42.6 | 0.031211 |
| Shigellosis | ||||||
| 1 | January 2018 | 4.15 | February 2020 | 5.77 | 1.3 | 0.318416 |
| 2 | February 2020 | 5.77 | May 2020 | 0.06 | −77.7 | 0.032693 |
| 3 | May 2020 | 0.06 | July 2020 | 0.47 | 172.9 | 0.142301 |
| Campylobacteriosis | ||||||
| 1 | January 2018 | 8.54 | July 2020 | 6.04 | −1.1 | 0.086214 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bassal, R.; Keinan-Boker, L.; Cohen, D. A Significant Decrease in the Incidence of Shigellosis in Israel during COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 3070. https://doi.org/10.3390/ijerph18063070
Bassal R, Keinan-Boker L, Cohen D. A Significant Decrease in the Incidence of Shigellosis in Israel during COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2021; 18(6):3070. https://doi.org/10.3390/ijerph18063070
Chicago/Turabian StyleBassal, Ravit, Lital Keinan-Boker, and Dani Cohen. 2021. "A Significant Decrease in the Incidence of Shigellosis in Israel during COVID-19 Pandemic" International Journal of Environmental Research and Public Health 18, no. 6: 3070. https://doi.org/10.3390/ijerph18063070
APA StyleBassal, R., Keinan-Boker, L., & Cohen, D. (2021). A Significant Decrease in the Incidence of Shigellosis in Israel during COVID-19 Pandemic. International Journal of Environmental Research and Public Health, 18(6), 3070. https://doi.org/10.3390/ijerph18063070