
Attachment Security and Suicide Ideation and Behaviour: The Mediating Role of Reflective Functioning



Abstract
:1. Introduction
2. Materials and Methods
2.1. Sampling and Procedure
2.2. Inclusion Criteria
2.3. Measures
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organisation. Suicide Data. 2018. Available online: http://www.who.int/mental_health/prevention/suicide/suicideprevent/en/ (accessed on 17 March 2021).
- Office of National Statistics. Suicides in the UK: 2019 Registrations. 2020. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths/bulletins/suicidesintheunitedkingdom/2019registrations (accessed on 17 March 2021).
- O’Connor, R.C.; Nock, M.K. The psychology of suicidal behaviour. Lancet Psychiatry 2014, 1, 73–85. [Google Scholar] [CrossRef]
- Durkheim, E. Le Suicide: Étude de Sociologie: Alcan; Alcan, F., Ed.; Le suicide: étude de sociologie: Paris, France, 1897. [Google Scholar]
- Baumeister, R.F. Suicide as Escape from Self. Psychol. Rev. 1990, 97, 90–113. [Google Scholar] [CrossRef] [PubMed]
- Johnson, J.; Gooding, P.; Tarrier, N. Suicide risk in schizophrenia: Explanatory models and clinical implications, The Schematic Appraisal Model of Suicide (SAMS). Psychol. Psychother. Theory Res. Pract. 2008, 81, 55–77. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, R.C. The integrated motivational-volitional model of suicidal behavior. Crisis 2011, 32, 295–298. [Google Scholar] [CrossRef] [PubMed]
- Schotte, D.E.; Clum, G.A. Problem-solving skills in psychiatric patients. J. Consult. Clin. Psychol. 1987, 55, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Williams, J.M.G. Cry of Pain: Understanding Suicide and Self-Harm; Penguin Group USA: London, UK, 1997. [Google Scholar]
- Williams, J.M.G. Suicide and Attempted Suicide; Penguin: London, UK, 2001. [Google Scholar]
- Klonsky, E.D.; May, A.M. Differentiating suicide attempters from suicide ideators: A critical frontier for suicidology research. Suicide Life Threat. Behav. 2014, 1, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Joiner, T. Why People Die by Suicide; Harvard University Press: Cambridge, MA, USA, 2005. [Google Scholar]
- Van Orden, K.A.; Witte, T.K.; Cukrowicz, K.C.; Braithwaite, S.R.; Selby, E.A.; Joiner, T.E., Jr. The interpersonal theory of suicide. Psychol. Rev. 2010, 117, 575–600. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chu, C.; Buchman-Schmitt, J.M.; Stanley, I.H.; Hom, M.A.; Tucker, R.P.; Hagan, C.R.; Rogers, M.L.; Podlogar, M.C.; Chiurliza, B.; Ringer, F.B.; et al. The interpersonal theory of suicide: A systematic review and meta-analysis of a decade of cross-national research. Psychol. Bull. 2017, 143, 1313–1345. [Google Scholar] [CrossRef] [PubMed]
- Hjelmeland, H.; Knizek, B.L. The emperor’s new clothes? A critical look at the interpersonal theory of suicide. Death Stud. 2020, 44, 168–178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, J.; Batterham, P.J.; Calear, A.L.; Han, J. A systematic review of the pre-dictions of the Interpersonal Psychological Theory of Suicidal Behavior. Clin. Psychol. Rev. 2016, 46, 34–45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bowlby, J. Attachment and Loss; Basic Books: New York, NY, USA, 1969; Volume 1. [Google Scholar]
- Main, M.; Kaplan, N.; Cassidy, J. Security in infancy, childhood, and adulthood: A move to the level of representation. Monogr. Soc. Res. Child Dev. 1985, 66–104. [Google Scholar] [CrossRef]
- Ainsworth, M.D.S.; Bell, S.M.; Stayton, D.J. Individual differences in strange- situation behavior of one-year-olds. In The Origins of Human Social Relations; Schaffer, H.R., Ed.; Academic Press: London, UK; New York, NY, USA, 1971; pp. 17–58. [Google Scholar]
- Ainsworth, M.D.S.; Blehar, M.C.; Waters, E.; Wall, S. Patterns of Attachment: A Psychological Study of the Strange Situation; Erlbaum: Hillside, NJ, USA, 1978. [Google Scholar]
- Fraley, R.C. Attachment stability from Infancy to Adulthood: Meta-analysis and Dynamic Modeling of Developmental Mechanisms. Personal. Soc. Psychol. Rev. 2002, 6, 123–151. [Google Scholar] [CrossRef]
- Hazan, C.; Shaver, P. Romantic Love Conceptualised as an Attachment Process. J. Personal. Soc. Psychol. 1987, 62, 511–524. [Google Scholar] [CrossRef]
- Bartholomew, K.; Horowitz, L.M. Attachment Styles Amoung Young Adults: A test of a four category model. J. Pers. Soc. Psychol. 1991, 61, 226–244. [Google Scholar] [CrossRef] [PubMed]
- Brennan, K.A.; Clark, C.L.; Shaver, P.R. Self-report measurement of adult romantic attachment: An integrative overview. In Attachment Theory and Close Relationships; Simpson, J.A., Rholes, W.S., Eds.; Guilford Press: New York, NY, USA, 1998; pp. 46–76. [Google Scholar]
- Adams, K.S. Suicidal behaviour and attachment: A developmental model. In Suicide over the Life Cycle: Risk Factors, Assessment and Treatment of Suicidal Patients; Blumenthal, S.J., Kupfer, D.J., Eds.; Guilford Press: New York, NY, USA, 1994; pp. 39–96. [Google Scholar]
- Miniati, M.; Callari, A.; Pini, S. Adult Attachment Style and Suicidality. Psychiatr. Danub. 2017, 29, 250–259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mickelson, K.D.; Kessler, R.C.; Shaver, P.R. Adult Attachment in a Nationally Representative Sample. J. Personal. Soc. Psychol. 1997, 73, 1092–1106. [Google Scholar] [CrossRef]
- Mikulincer, M.; Shaver, P.R. Attachment in Adulthood: Structure, Dynamics, and Change; Guilford Press: New York, NY, USA, 2007. [Google Scholar]
- Green, J.; Berry, K.; Danquah, A.; Pratt, D. The Role of Psychological and Social Factors in the Relationship between Attachment and Suicide: A Systematic Review. Clin. Psychol. Psychother. 2020, 27, 463–488. [Google Scholar] [CrossRef] [Green Version]
- Adams, K.S.; Sheldon-Keller, A.E.; West, M. Attachment organisation and history of suicidal behaviour in clinical adolescents. J. Consult. Clin. Psychol. 1996, 64, 264–272. [Google Scholar] [CrossRef]
- de Jong, M.L. Attachment, Individuation, and Risk of Suicide in Late Adolescence. J. Youth Adolesc. 1992, 21, 357–373. [Google Scholar] [CrossRef]
- Sheftall, A.H.; Mathias, C.W.; Furr, R.M.; Dougherty, D.M. Adolescent attachment security, family functioning, and suicide attempts. Attach Hum. Dev. 2013, 15, 368–383. [Google Scholar] [CrossRef] [Green Version]
- McKeown, A.; Clarbour, J.; Heron, R.; Thomson, N.D. Attachment, Coping, and Suicidal Behavior in Male Prisoners. Crim. Justice Behav. 2016, 44, 566–588. [Google Scholar] [CrossRef]
- Palitsky, D.; Mota, N.; Afifi, T.O.; Downs, A.C.; Sareen, J. The association between adult attachment style, mental disorders, and suicidality: Findings from a population-based study. J. Nerv. Ment. Dis. 2013, 201, 579–586. [Google Scholar] [CrossRef] [PubMed]
- Davaji, R.B.O.; Valizadeh, S.; Nikamal, M. The relationship between attachment styles and suicide ideation: The study of Turkmen students, Iran. Procedia Soc. Behav. Sci. 2010, 5, 1190–1194. [Google Scholar] [CrossRef] [Green Version]
- Lessard, J.C.; Moretti, M.M. Suicidal ideation in an adolescent clinical sample: Attachment patterns and clinical implications. Adolescence 1998, 21, 383–395. [Google Scholar] [CrossRef] [PubMed]
- Grunebaum, M.F.; Galfalvy, H.C.; Mortenson, L.Y.; Burke, A.K.; Oquendo, M.A.; Mann, J.J. Attachment and social adjustment: Relationships to suicide attempt and major depressive episode in a prospective study. J. Affect. Disord. 2010, 123, 123–130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lizardi, D.; Grunebaum, M.F.; Burke, A.; Stanley, B.; Mann, J.J.; Harkavy-Friedman, J.; Oquendo, M. The effect of social adjustment and attachment style on suicidal behaviour. Acta Psychiatr. Scand. 2011, 124, 295–300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sheftall, A.H.; Schoppe-Sullivan, S.J.; Bridge, J.A. Insecure attachment and suicidal behavior in adolescents. Crisis 2014, 35, 426–430. [Google Scholar] [CrossRef] [PubMed]
- Stepp, S.D.; Morse, J.Q.; Yaggi, K.E.; Reynolds, S.K.; Reed, L.I.; Pilkonis, P.A. The role of attachment styles and interpersonal problems in suicide-related behaviors. Suicide Life Threat. Behav. 2008, 38, 592–607. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Falgares, G.; Marchetti, D.; De Santis, S.; Carrozzino, D.; Kopala-Sibley, D.C.; Fulcheri, M.; Verrocchio, M.C. Attachment Styles and Suicide-Related Behaviors in Adolescence: The Mediating Role of Self-Criticism and Dependency. Front. Psychiatry 2017, 8, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levi-Belz, Y.; Gvion, Y.; Horesh, N.; Apter, A. Attachment patterns in medically serious suicide attempts: The mediating role of self-disclosure and loneliness. Suicide Life Threat. Behav. 2013, 43, 511–522. [Google Scholar] [CrossRef] [PubMed]
- Cohen, L.J.; Ardalan, F.; Yaseen, Z.; Galynker, I. Suicide Crisis Syndrome Mediates the Relationship between Long-term Risk Factors and Lifetime Suicidal Phenomena. Suicide Life Threat. Behav. 2017. epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Galynker, I.I.; Briggs, J.; Duffy, M.; Frechette-Hagan, A.; Kim, H.J.; Yaseen, Z.S. Attachment style and suicide behaviors in high risk psychiatric inpatients following hospital discharge: The mediating role of entrapment. Psychiatry Res. 2017, 257, 309–314. [Google Scholar] [CrossRef] [PubMed]
- Fonagy, P.; Bateman, A. Adversity, attachment, and mentalizing. Compr. Psychiatry 2016, 64, 59–66. [Google Scholar] [CrossRef] [PubMed]
- Fonagy, P.; Gergely, G.; Jurist, E.L.; Target, M. Affect Regulation, Mentalization, and the Development of the Self; Other Press: New York, NY, USA, 2002. [Google Scholar]
- Fonagy, P.; Target, M. Attachment and Reflective Function: The role in self-organisation. Dev. Psychopathol. 1997, 9, 679–700. [Google Scholar] [CrossRef] [PubMed]
- Katznelson, H. Reflective functioning: A review. Clin. Psychol. Rev. 2014, 34, 107–117. [Google Scholar] [CrossRef]
- Meins, E.; Fernyhough, C.; Wainwright, R.; Das Gupta, M.; Fradley, E.; Tuckey, M. Maternal mind–mindedness and attachment security as predictors of theory of mind understanding. Child Dev. 2002, 73, 1715–1726. [Google Scholar] [CrossRef] [PubMed]
- Fonagy, P.; Luyten, P. A developmental, mentalization-based approach to the understanding and treatment of borderline personality disorder. Dev. Psychopathol. 2009, 21, 1355–1381. [Google Scholar] [CrossRef] [PubMed]
- Klonsky, E.D.; May, A. Rethinking impulsivity in suicide. Suicide Life Threat. Behav. 2010, 40, 612–619. [Google Scholar] [CrossRef] [PubMed]
- Troister, T.; Holden, R.R. A two-year prospective study of psychache and its relationship to suicidality among high-risk undergraduates. J. Clin. Psychol. 2012, 68, 1019–1027. [Google Scholar] [CrossRef] [PubMed]
- Weinberg, A.; Klonsky, E.D. Measurement of emotion dysregulation in adolescents. Psychol. Assess. 2009, 21, 616. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bateman, A.; Fonagy, P. 8-Year Follow-Up of Patients Treated for Borderline Personality Disorder: Mentalization-based Treatment verus Treatment as Usual. Am. J. Psychiatry 2008, 165, 631–638. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duno, R.; Pousa, E.; Miguelez, M.; Montalvo, I.; Suarez, D.; Tobena, A. Suicidality connected with mentalizing anomalies in schizophrenia: A study with stabilized outpatients. Ann. N. Y. Acad. Sci. 2009, 1167, 207–211. [Google Scholar] [CrossRef] [PubMed]
- George, C.; Kaplan, N.; Main, M. Adult Attachment Interview, 3rd ed.; University of California: Berkley, CA, USA, 1996. [Google Scholar]
- Fonagy, P.; Luyten, P.; Moulton-Perkins, A.; Lee, Y.W.; Warren, F.; Howard, S.; Lowyck, B. Development and Validation of a Self-Report Measure of Mentalizing: The Reflective Functioning Questionnaire. PLoS ONE 2016, 11, e0158678. [Google Scholar] [CrossRef] [PubMed]
- Nock, M.K.; Borges, G.; Bromet, E.J.; Alonso, J.; Angermeyer, M.; Beautrais, A.; Bruffaerts, R.; Chiu, W.T.; de Girolamo, G.; Gluzman, S.; et al. Cross-national prevalence and risk factors for suicidal ideation, plans and attempts. Br. J. Psychiatry 2008, 192, 98–105. [Google Scholar] [CrossRef] [PubMed]
- Brown, G.K.; Beck, A.T.; Steer, R.A.; Grisham, J.R. Risk Factors for Suicide in Psychiatric Outpatients: A 20-year Prospective Study. J. Couns. Clin. Psychol. 2000, 68, 371–377. [Google Scholar] [CrossRef]
- Lewinsohn, P.M.; Rohde, P.; Seeley, J.R. Adolescent suicidal ideation and attempts: Prevalence, risk factors, and clinical implications. Clin. Psychol. Sci. Pract. 1996, 3, 25–46. [Google Scholar] [CrossRef]
- Steinhausen, H.C.; Winkler Metzke, C.W. The impact of suicidal ideation in preadolescence, adolescence, and young adulthood on psychosocial functioning and psychopathology in young adulthood. Acta Psychiatr. Scand. 2004, 110, 438–445. [Google Scholar] [CrossRef] [PubMed]
- Branley-Bell, D.; O’Connor, D.B.; Green, J.A.; Ferguson, E.; O’Carroll, R.E.; O’Connor, R.C. Distinguishing suicide ideation from suicide attempts: Further test of the Integrated Motivational-Volitional Model of Suicidal Behaviour. J. Psychiatr. Res. 2019, 117, 100–107. [Google Scholar] [CrossRef]
- Beck, A.T.; Kovacs, M.; Weissman, A. Assessment of suicidal intention: The Scale for Suicide Ideation. J. Consult. Clin. Psychol. 1979, 47, 343–352. [Google Scholar] [CrossRef]
- Beck, A.T.; Steer, R.A.; Ranieri, W.F. Scale for Suicide Ideation: Psychometric properties of a self-report version. J. Clin. Psychol. 1988, 44, 499–505. [Google Scholar] [CrossRef]
- Fraley, R.C.; Waller, N.G.; Brennan, K.A. An item response theory analysis of self-report measures of adult attachment. J. Personal. Soc. Psychol. 2000, 78, 350–365. [Google Scholar] [CrossRef]
- Mikulincer, M.; Shaver, P.R. Measurement of attachment-related constructs in adulthood. In Attachment in Adulthood; Mikulincer, M., Shaver, P.R., Eds.; Guilford Press: New York, NY, USA, 2007; pp. 81–115. [Google Scholar]
- Sibley, C.G.; Fischer, R.; Liu, J.H. Reliability and validity of the revised experiences in close relationships (ECR-R) self-report measure of adult romantic attachment. Pers. Soc. Psychol. Bull. 2005, 31, 1524–1536. [Google Scholar] [CrossRef] [PubMed]
- Beck, A.T.; Weissman, A.; Lester, D.; Trexler, L. The measurement of pessimism: The Hopelessness Scale. J. Consult. Clin. Psychol. 1974, 42, 861–865. [Google Scholar] [CrossRef] [PubMed]
- McMillan, D.; Gilbody, S.; Beresford, E.; Neilly, L. Can we predict suicide and non-fatal self-harm with the Beck Hopelessness Scale? A meta-analysis. Psychol. Med. 2007, 37, 769–778. [Google Scholar] [CrossRef] [PubMed]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.W. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Int. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef] [PubMed]
- Field, A. Discovering Statistics Using IBM SPSS Statistics, 4th ed.; Sage: London, UK, 2014. [Google Scholar]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach; Guilford Press: New York, NY, USA, 2013. [Google Scholar]
- Funder, D.C.; Ozer, D.J. Evaluating effect size in psychological research: Sense and nonsense. Adv. Methods Pract. Psychol. Sci. 2019, 2, 156–168. [Google Scholar] [CrossRef]
- Hayes, A.F.; Rockwood, N.J. Regression-based statistical mediation and moderation analysis in clinical research: Observations, recommendations, and implementation. Behav. Res. 2017, 98, 39–57. [Google Scholar] [CrossRef]
- Baron, R.M.; Kenny, D.A. The moderator–mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. J. Pers. Soc. Psychol. 1986, 51, 1173–1182. [Google Scholar] [CrossRef] [PubMed]
- Riggs, S.A.; Jacobvitz, D. Expectant parents’ representations of early attachment relationships: Associations with mental health and family history. J. Consult. Clin. Psychol. 2002, 70, 195–204. [Google Scholar] [CrossRef] [PubMed]
- Fossati, A.; Feeney, J.; Maffei, C.; Borroni, S. Thinking about feelings: Affective state mentalization, attachment styles, and borderline personality disorder features among Italian nonclinical adolescents. Psychoanal. Psychol. 2014, 31, 41–67. [Google Scholar] [CrossRef]
- Levesque, C.; Lafontaine, M.-F.; Bureau, J.-F.; Cloutier, P.; Dandurand, C. The influence of romantic attachment and intimate partner violence on non-suicidal self-injury in young adults. J. Youth Adolesc. 2010, 39, 474–483. [Google Scholar] [CrossRef] [PubMed]
- Fonagy, P.; Bateman, A. The development of borderline personality disorder-A mentalizing model. J. Personal. Disord. 2008, 22, 4. [Google Scholar] [CrossRef]
- Ravitz, P.; Maunder, R.; Hunter, J.; Sthankiya, B.; Lancee, W. Adult attachment measures: A 25-year review. J. Psychosom. Res. 2010, 69, 419–432. [Google Scholar] [CrossRef] [PubMed]
- Paetzold, R.L.; Rholes, W.S.; Kohn, J.L. Disorganized attachment in adulthood: Theory, measurement, and implications for romantic relationships. Rev. Gen. Psychol. 2015, 19, 146–156. [Google Scholar] [CrossRef]
- Main, M.; Hesse, E. Parents’ unresolved traumatic experiences are related to infant disorganized attachment status: Is frightened and/or frightening parental behavior the linking mechanism? In Attachment in the Preschool Years: Theory, Research, and Intervention; Greenberg, M.T., Cicchetti, D., Cummings, E.M., Eds.; University of Chicago Press: Chigago, IL, USA, 1990; pp. 161–182. [Google Scholar]
- Shiffman, S.; Stone, A.A.; Hufford, M.R. Ecological momentary assessment. Annu. Rev. Clin. Psychol. 2008, 4, 1–32. [Google Scholar] [CrossRef] [PubMed]
- Kirschbaum, C.; Pirke, K.-M.; Hellhammer, D.H. The ‘Trier Social Stress Test’—A tool for investigating psychobiological stress responses in a laboratory setting. Neuropsychobiology 1993, 28, 76–81. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Total N = 65 | |
|---|---|
| Sociodemographic Variables | N (%) |
| Gender | |
| Male | 20 (30.8) |
| Female | 45 (69.2) |
| Ethnicity | |
| White British | 54 (83.1) |
| White Other | 4 (6.2) |
| Other | 7 (10.8) |
| Educational Attainment, highest level | |
| None | 4 (6.2) |
| GCSEs or equivalent | 12 (18.5) |
| A Levels or equivalent | 26 (40.0) |
| Undergraduate degree | 9 (13.8) |
| Postgraduate degree | 6 (12.3) |
| Other | 8 (12.3) |
| Current Relationship Status | |
| Single | 44 (67.7) |
| In a relationship | 8 (12.3) |
| Cohabiting | 5 (7.7) |
| Married | 8 (12.3) |
| Employment Status | |
| Unemployed | 9 (13.8) |
| Unable to work (due to disability, mental health, sickness) | 19 (29.2) |
| Employed | 17 (26.2) |
| Student | 19 (29.2) |
| Retired | 1 (1.5) |
| Self-reported Psychiatric Diagnosis a | |
| None/Not stated | 11 (16.9) |
| Anxiety Disorder | 24 (39.6) |
| Mood Disorder | 37 (56.9) |
| Personality Disorder | 14 (21.5) |
| Psychotic Disorder | 10 (15.4) |
| Other | 4 (6.2) |
| Self-reported Disability a | |
| None | 41 (63.1) |
| Physical | 10 (15.4) |
| Learning Disability/Difficulty | 4 (6.2) |
| Autistic Spectrum Disorder | 4 (6.2) |
| Mental Health | 11 (16.9) |
| Other | 1 (1.5) |
| Kolmogorov–Smirnov Test | Cronbach’s Alpha | ||||
|---|---|---|---|---|---|
| Mean (SD) | Range | Statistic | Sig. Level | α | |
| Suicidal Ideation | 14.23 (9.87) | 0–35.00 | 0.13 | 0.01 | 0.94 |
| Depression | 15.87 (7.38) | 0–27.00 | 0.13 | 0.01 | 0.89 |
| Hopelessness | 12.09 (6.49) | 0–20.29 | 0.15 | 0.01 | 0.94 |
| Attachment Security: | |||||
| Anxious Attachment a | 4.21 (1.42) | 1.06–6.61 | 0.08 | 0.20 | 0.93 |
| Avoidant Attachment a | 3.80 (1.44) | 1.11–6.67 | 0.09 | 0.20 | 0.94 |
| Reflective Functioning: | |||||
| Certainty a | 0.66 (0.74) | 0–2.83 | 0.19 | <0.001 | 0.78 |
| Uncertainty a | 1.36 (0.88) | 0–3.00 | 0.11 | 0.04 | 0.80 |
| Hopelessness | Depression a | Anxious Attachment | Avoidant Attachment | Certainty of Mental State/Hypermentalising | Uncertainty of Mental State/Hypomentalising | |
|---|---|---|---|---|---|---|
| Suicidal Ideation | 0.71 ** [0.59, 0.82] | 0.48 ** [0.31, 0.63] | 0.22 [−0.08, 0.50] | 0.36 ** [0.13, 0.58] | −0.09 [−0.36, 0.17] | 0.24 [−0.04, 0.48] |
| Hopelessness | 0.60 ** [0.41, 0.74] | 0.27 * [0.03, 0.49] | 0.32 * [0.11, 0.53] | −0.12 [−0.39, 0.14] | 0.23 [−0.03, 0.45] | |
| Depression a | 0.26 * [0.03, 0.45] | 0.25 [−0.01, 0.47] | −0.13 [−0.35, 0.10] | 0.23 [−0.01, 0.45] | ||
| Anxious Attachment | 0.36 ** [0.12, 0.56] | −0.22 [−0.47, 0.02] | 0.60 * [0.40, 0.75] | |||
| Avoidant Attachment | 0.09 [−0.18, 0.30] | 0.20 [−0.07, 0.45] | ||||
| Certainty of Mental State/Hypermentalising | −0.61 ** [−0.74, −0.46] |
| Independent Variable (Attachment Dimension) | Path a | Path b | Total Effect (c): | Direct Effect (c’) | Indirect Effect | Sobel Test: z-Score (p Value) |
|---|---|---|---|---|---|---|
| Anxious | 0.36 [0.23, 0.48] | 1.87 [−0.1.71, 5.46] | 1.51 [−0.20, 3.22] | 0.84 [−1.30, 2.98] | 0.69 [−0.64, 1.93] | 1.01 (0.31) |
| (controlling for depression) a | 0.34 [0.22, 0.47] | 1.26 [−2.00, 4.52] | 0.72 [−0.87, 2.32] | 0.29 [−1.67, 2.25] | 0.43 [−0.99, 1.50] | 0.75 (0.45) |
| Avoidant | 0.12 [−0.03, 0.26] | 1.95 [−0.83, 4.73] | 2.39 [0.81, 3.96] | 2.16 [0.56, 3.75] | 0.23 [−0.08, 1.02] | 0.96 (0.34) |
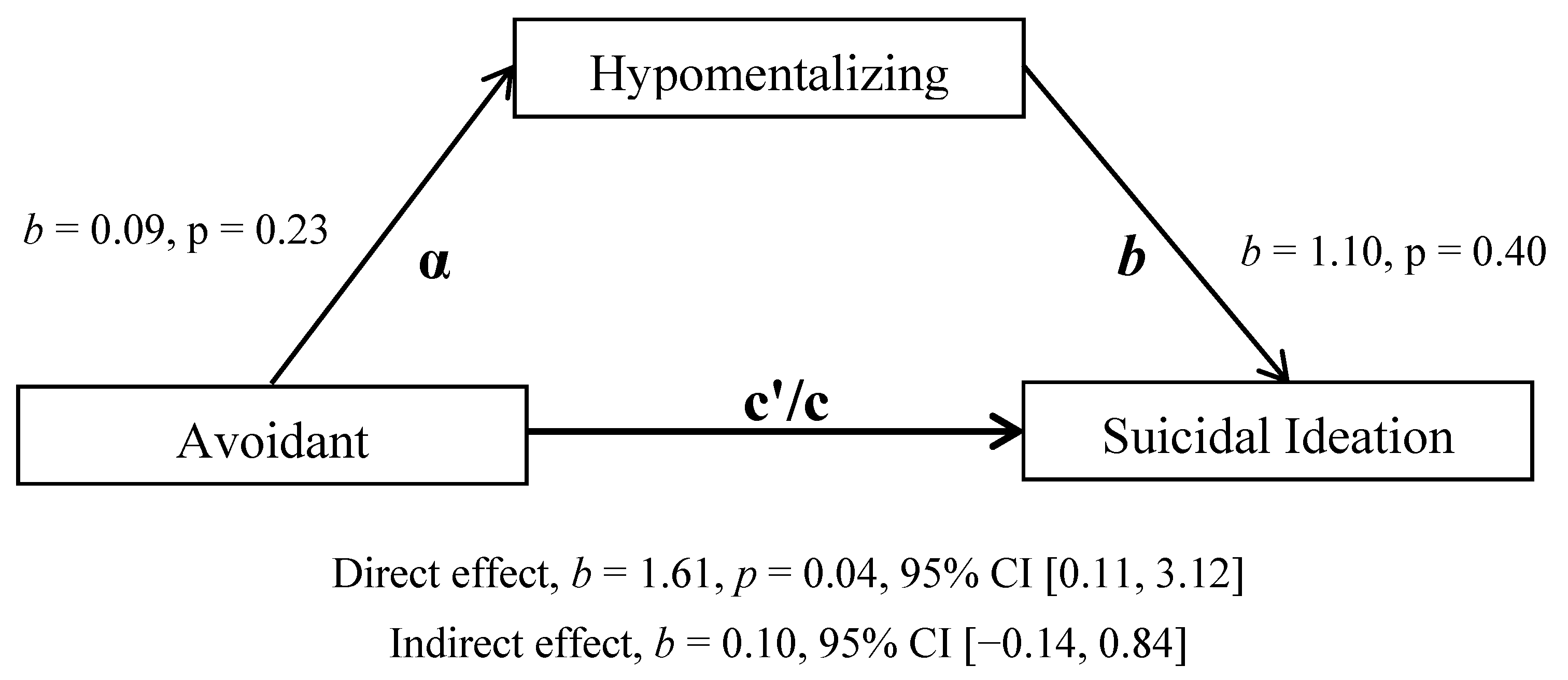
| (controlling for depression) a | 0.09 [−0.06, 0.24] | 1.10 [−1.50, 3.71] | 1.71 [0.23, 3.19] | 1.61 [0.11, 3.12] | 0.10 [−0.14, 0.84] | 0.57 (0.57) |
| Descriptive Statistics | Kruskal–Wallis Test | Pairwise Comparisons | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Never (n = 17) | Once (n = 19) | Multiple (n = 29) | H Statistic | Sig. | Never: Once | Never: Multiple | Once: Multiple | ||
| Attachment a | |||||||||
| Anxious | 3.32 (1.16) | 4.38 (1.18) | 4.64 (1.50) | 10.37 | 0.01 | −0.37 | −0.47 ** | −0.11 | |
| Avoidant | 3.03 (1.02) | 3.71 (1.51) | 4.23 (1.42) | 5.39 | 0.07 | - | - | - | |
| Reflective Functioning a | |||||||||
| Certainty | 0.59 (0.49) | 0.69 (0.73) | 0.47 (0.62) | 1.59 | 0.45 | - | - | - | |
| Uncertainty | 0.82 (0.49) | 1.34 (0.89) | 1.63 (0.91) | 6.431 | 0.04 | −0.22 | −0.38 * | −0.16 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Green, J.; Berry, K.; Danquah, A.; Pratt, D. Attachment Security and Suicide Ideation and Behaviour: The Mediating Role of Reflective Functioning. Int. J. Environ. Res. Public Health 2021, 18, 3090. https://doi.org/10.3390/ijerph18063090
Green J, Berry K, Danquah A, Pratt D. Attachment Security and Suicide Ideation and Behaviour: The Mediating Role of Reflective Functioning. International Journal of Environmental Research and Public Health. 2021; 18(6):3090. https://doi.org/10.3390/ijerph18063090
Chicago/Turabian StyleGreen, Jessica, Katherine Berry, Adam Danquah, and Daniel Pratt. 2021. "Attachment Security and Suicide Ideation and Behaviour: The Mediating Role of Reflective Functioning" International Journal of Environmental Research and Public Health 18, no. 6: 3090. https://doi.org/10.3390/ijerph18063090
APA StyleGreen, J., Berry, K., Danquah, A., & Pratt, D. (2021). Attachment Security and Suicide Ideation and Behaviour: The Mediating Role of Reflective Functioning. International Journal of Environmental Research and Public Health, 18(6), 3090. https://doi.org/10.3390/ijerph18063090