
Development and Effects of Cognitive Behavior-Based Healing Programs Using Mobile Apps



Abstract
:1. Introduction
2. Materials and Methods
2.1. App Development Process
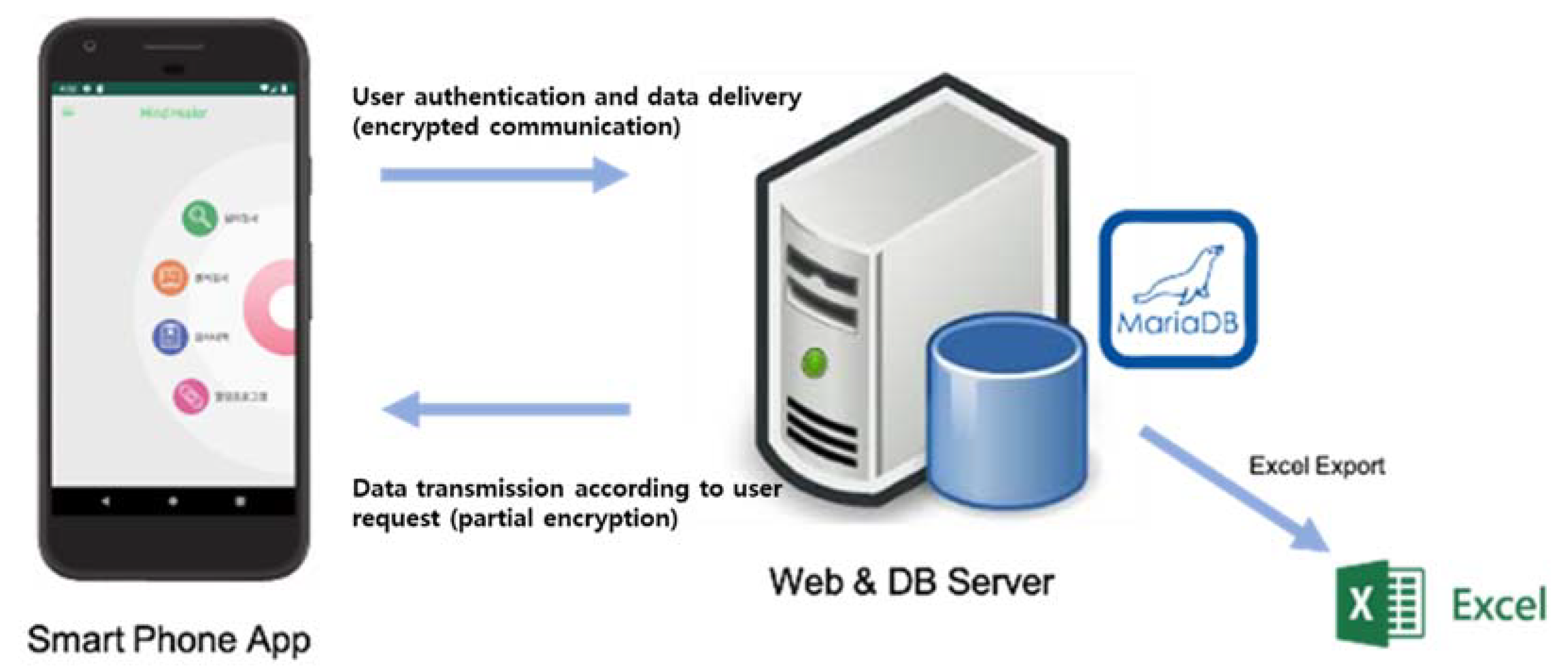
2.1.1. Structural Design
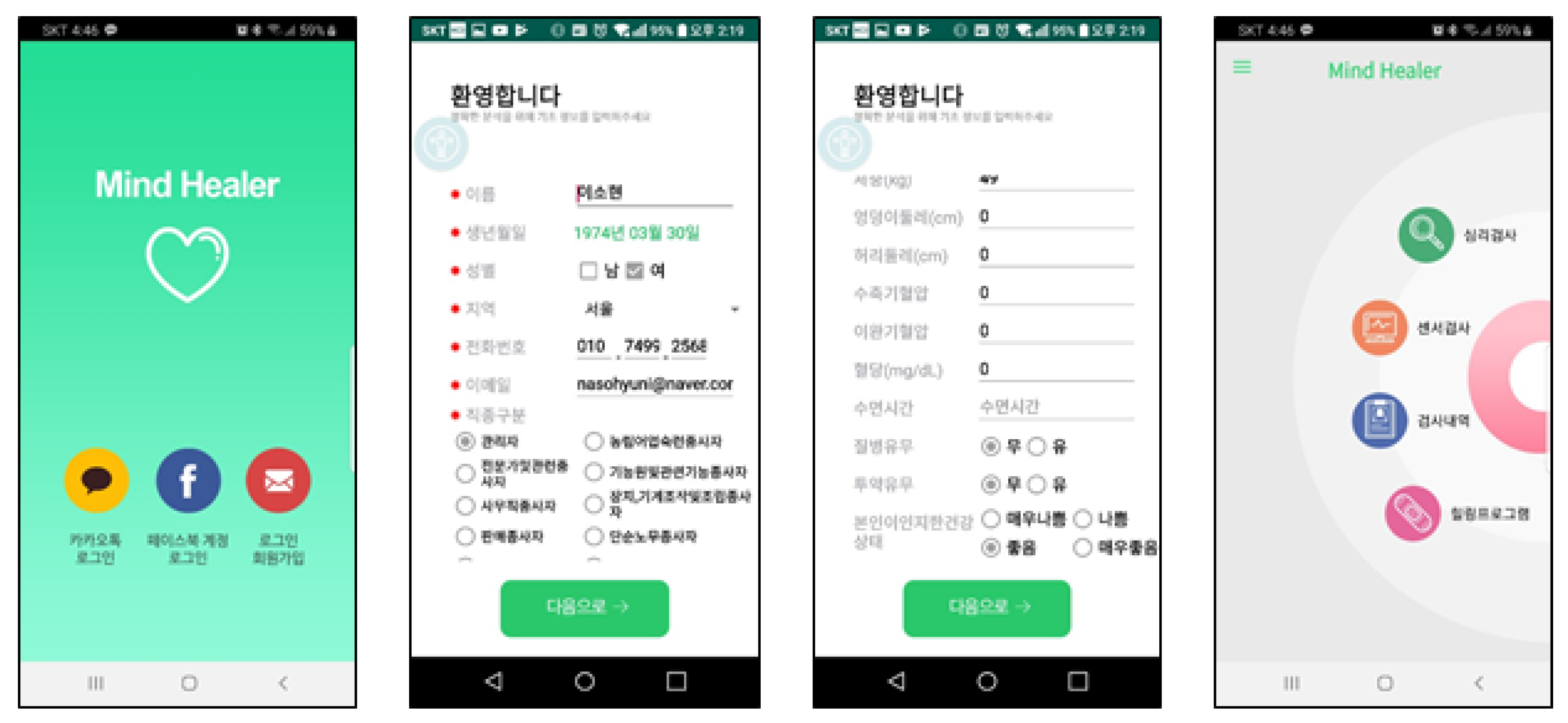
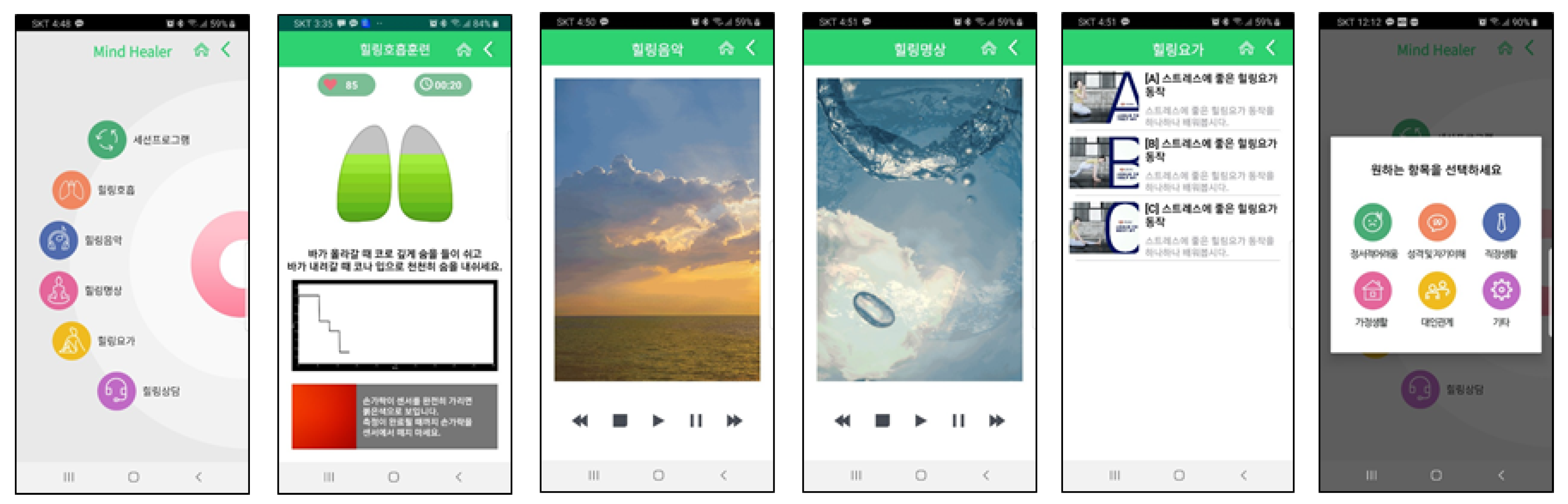
2.1.2. User Interface Design
- Two tools were used for stress. The first was the Perceived Stress Scale (PSS), developed by Cohen, Kamarck, and Mermelstein [16]. It is a Korean version of the PSS (PS-10)—a tool developed to assess the awareness of subjective stress. It comprises six items that measure negative awareness and four items that measure positive awareness. It evaluates the past month and provides a score from 0 to 4 per item (range = 0–40), and higher scores indicate greater stress awareness. Cronbach’s α was 0.89. Second, we used the effort–reward imbalance (ERI), a tool translated by Hwang, Hong, and Kang [17] based on a tool developed by Siegrist [18]. The ERI measures work-related stress, and Cronbach’s α was 0.80.
- Depression was based on the Patient Health Questionnaire-9 (PHQ-9) score, a self-reporting evaluation measure developed by Kroenke, et al. [19]. We used the Korean version of PHQ-9 by Lee, et al. [20]. Participants were to answer the level of symptoms experienced in the past two weeks based on frequency. Scores ranged from 0 to 27, and higher scores indicated higher depression levels. Cronbach’s α was 0.89.
- Anxiety was measured with the General Anxiety Disorder-7 (GAD-7), a seven-item self-reporting assessment tool developed by Spitzer, et al. [21]. The GAD-7 was designed based on Diagnostic and Statistical Manual of Mental Disorders (DSM)-IV diagnosis criteria to enable a GAD diagnosis. Cronbach’s α was 0.92.
- Emotional labor was measured with the Korean Emotional Labor Scale (K-ELS) by Lee, et al. [22]. It was designed to quantitatively and objectively evaluate the level and intensity of emotional labor and the negative emotional responses caused by emotional labor, which reflects the specific nature of Korea’s organizational culture and service industry. The K-ELS consists of 24 questions measured on a 4-point scale. Cronbach’s α was 0.79.
- Well-being was based on the WHO-5 well-being score. This was measured with five questions on a 6-point scale covering the past two weeks. Higher scores indicate better well-being [23].
2.2. Assessment of App Effectiveness
2.2.1. Research Design
2.2.2. Participants
2.3. Research Procedure
2.3.1. Ethical Aspects
2.3.2. App Development
2.4. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Ministry of Health & Welfare. The Survey of Mental Disorders in Korea; Series The Survey of Mental Disorders in Korea; Ministry of Health & Welfare: Sejong, Korea, 2016. [Google Scholar]
- Park, E.; Kim, J.-H.; Mirihae, K. The Impact of Well-Being Cognition Technique Using the Smartphone APP on the Job Stress and Subjective Well-Being of Employees. Korean J. Health Psychol. 2020, 25, 57–74. [Google Scholar] [CrossRef]
- Taouk, Y.; Spittal, M.J.; LaMontagne, A.D.; Milner, A.J. Psychosocial work stressors and risk of all-cause and coronary heart disease mortality: A systematic review and meta-analysis. Scand. J. Work Environ. Health 2020, 46, 19–31. [Google Scholar] [CrossRef] [Green Version]
- Hwang, W.J.; Jo, H.H. Evaluation of the Effectiveness of Mobile App-Based Stress-Management Program: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2019, 16, 4270. [Google Scholar] [CrossRef] [Green Version]
- Bakker, D.; Kazantzis, N.; Rickwood, D.; Rickard, N. Mental health smartphone apps: Review and evidence-based recommendations for future developments. JMIR Ment. Health 2016, 3, e7. [Google Scholar] [CrossRef] [Green Version]
- ICT(Information and Communication Technology), M.O.S.A. 2019 Survery on the Internet Usage. Korea Internet & Security Agency (KISA). 2020. Available online: http://eiec.kdi.re.kr/policy/materialView.do?num=198051 (accessed on 2 November 2020).
- Kim, S.; Shin, H.; Kim, Y. Study on Relation Between Education Level and Overdependence on Smartphone for Middle-aged and Elderly People: Focused on Mediator Effect of Willingness to Participate in Smartphone Overdependence Prevention Program. J. Soc. Sci. 2020, 31, 31–46. [Google Scholar] [CrossRef]
- Meeker, M.; Wu, L. Internet trends D11 conference. Kleiner Perkins Caufld. Byers. Retrieved 2013, 2, 14. [Google Scholar]
- Oulasvirta, A.; Rattenbury, T.; Ma, L.; Raita, E. Habits make smartphone use more pervasive. Pers. Ubiquitous Comput. 2012, 16, 105–114. [Google Scholar] [CrossRef]
- Wang, C.; Lee, M.K. Why We Cannot Resist Our Smartphones: Investigating Compulsive Use of Mobile SNS from a Stimulus-Response-Reinforcement Perspective. J. Assoc. Inf. Syst. 2020, 21, 4. [Google Scholar] [CrossRef] [Green Version]
- East, M.L.; Havard, B.C. Mental health mobile apps: From infusion to diffusion in the mental health social system. JMIR Ment. Health 2015, 2, e10. [Google Scholar] [CrossRef] [PubMed]
- Lee, R.A.; Jung, M.E. Evaluation of an mhealth app (destressify) on university students’ mental health: Pilot trial. JMIR Ment. Health 2018, 5, e2. [Google Scholar] [CrossRef] [PubMed]
- Hwang, W.J.; Ha, J.S.; Kim, M.J. Research trends on mobile mental health application for general population: A scoping review. Int. J. Environ. Res. Public Health 2021, 18, 2459. [Google Scholar] [CrossRef]
- An, S. Use of Mobile Mental Health Application for Mental Health Promotion: Based on the Information-Motivation-Behavioral Skills Model. Korean J. Commun. Stud. 2018, 62, 167–194. [Google Scholar] [CrossRef]
- Yun, G. The 2021 outlook for Healthcare Policy. Health Welf. Policy Forum 2021, 2021, 9–22. [Google Scholar]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef] [PubMed]
- Hwang, W.J.; Hong, O.; Kang, D.R. Psychometric Testing of the Effort-Reward Imbalance-Short Form Among Blue-Collar Workers Employed in Small Industrial Settings in Korea. Workplace Health Saf. 2018, 66, 597–605. [Google Scholar] [CrossRef] [PubMed]
- Siegrist, J. Effort-reward imbalance at work and cardiovascular diseases. Int. J. Occup. Med. Environ. Health 2010, 23, 279–285. [Google Scholar] [CrossRef] [Green Version]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Lee, S.; Huh, Y.; Kim, J. Finding Optimal Cut Off Points of the Korean Version of the Patient Health Questionnaire-9 (PHQ-9) for Screening Depressive Disorders. Mood Emot 2014, 12, 32–36. [Google Scholar]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.; Löwe, B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.; Han, E.-m.; Hong, H.; Lee, I. Validation of the Korean Version of the Emotional Labor Scale (ELS). Korean Psychol. Assoc. 2016, 21, 243–256. [Google Scholar]
- WHO. Mental Health: A State of Well-Being. 2014. Available online: http://www.who.int/features/factfiles/mental_health/en/ (accessed on 11 December 2020).
- Carvalho, J.; Rocha, A.; Junqueira, L.; Neto, J.S.; Santos, I.; Nascimento, F. A tool for time-frequency analysis of heart rate variability. In Proceedings of the 25th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (IEEE Cat. No. 03CH37439), Cancun, Mexico, 17–21 September 2003; pp. 2574–2577. [Google Scholar]
- Mohan, P.M.; Nagarajan, V.; Das, S.R. Stress measurement from wearable photoplethysmographic sensor using heart rate variability data. In Proceedings of the 2016 International Conference on Communication and Signal Processing (ICCSP), Melmaruvathur, India, 6–8 April 2016; pp. 1141–1144. [Google Scholar]
- Yoo, K.-S.; Lee, W.-H. Mental stress assessment based on pulse photoplethysmography. In Proceedings of the 2011 IEEE 15th International Symposium on Consumer Electronics (ISCE), Singapore, 14–17 June 2011; pp. 323–326. [Google Scholar]
- Blumenstein, B.; Breslav, I.; Bar-Eli, M.; Tenenbaum, G.; Weinstein, Y. Regulation of mental states and biofeedback techniques: Effects on breathing pattern. Biofeedback Self-Regul. 1995, 20, 169–183. [Google Scholar] [CrossRef]
- Jerath, R.; Barnes, V.A. Augmentation of mind-body therapy and role of deep slow breathing. J. Complement. Integr. Med. 2009, 6. [Google Scholar] [CrossRef] [Green Version]
- Song, H.-S. A Study on the Relation between Emotion and Color. in Healing Video Art. Treatise Plast. Media 2011, 14, 79–86. [Google Scholar]
- NIMH. Technology and the Future of Mental Health Treatment. Available online: https://www.nimh.nih.gov/health/topics/technology-and-the-future-of-mental-health-treatment/index.shtml (accessed on 3 December 2020).
- Villani, D.; Grassi, A.; Cognetta, C.; Toniolo, D.; Cipresso, P.; Riva, G. Self-help stress management training through mobile phones: An experience with oncology nurses. Psychol. Serv. 2013, 10, 315. [Google Scholar] [CrossRef]
- Shen, N.; Levitan, M.-J.; Johnson, A.; Bender, J.L.; Hamilton-Page, M.; Jadad, A.A.R.; Wiljer, D. Finding a depression app: A review and content analysis of the depression app marketplace. JMIR mHealth uHealth 2015, 3, e16. [Google Scholar] [CrossRef] [PubMed]
- Birney, A.J.; Gunn, R.; Russell, J.K.; Ary, D.V. MoodHacker mobile web app with email for adults to self-manage mild-to-moderate depression: Randomized controlled trial. JMIR mHealth uHealth 2016, 4, e8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donker, T.; Petrie, K.; Proudfoot, J.; Clarke, J.; Birch, M.-R.; Christensen, H. Smartphones for Smarter Delivery of Mental Health Programs: A Systematic Review. J. Med. Internet Res. 2013, 15, e247. [Google Scholar] [CrossRef] [Green Version]
- de Santos Sierra, A.; Ávila, C.S.; Casanova, J.G.; del Pozo, G.B. A stress-detection system based on physiological signals and fuzzy logic. IEEE Trans. Ind. Electron. 2011, 58, 4857–4865. [Google Scholar] [CrossRef] [Green Version]
- Hammen, C.; Kim, E.Y.; Eberhart, N.K.; Brennan, P.A. Chronic and acute stress and the prediction of major depression in women. Depress. Anxiety 2009, 26, 718–723. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harkness, K.L.; Monroe, S.M. The assessment and measurement of adult life stress: Basic premises, operational principles, and design requirements. J. Abnorm. Psychol. 2016, 125, 727. [Google Scholar] [CrossRef]
- Kim, W.; Rhee, K.Y.; Lee, G. Work Environment and Stress of Emotional Laborers. Korean Sociol. Assoc. 2012, 46, 123–149. [Google Scholar]
- KOSHA, K.O.S.H.A. Korean Emotional Labor Guideline. 2019. Available online: http://www.moel.go.kr/local/seoulseobu/info/dataroom/view.do?bbs_seq=20200101192 (accessed on 11 December 2020).
- Shim, S.J. Determinants of Subjective Well-being in Korea. J. Korean Off. Stat. 2016, 21, 25–47. [Google Scholar]
- Ki, Y.-S.; Ahn, S.-M.; Cho, M.-G.; Choi, B. An Analysis on Affecting Factors of Healthcare Applications Continuous Usage Intention and their Relationships. J. Soc. E-Bus. Stud. 2019, 24, 49–86. [Google Scholar] [CrossRef]
- Lee, L.-S.; Lee, S.-H.; Jeong, J.-S.; Noh, K.-Y. Psychological Factors Influencing Continuous Use of Mobile Healthcare Applications. J. Digit. Converg. 2017, 15, 445–456. [Google Scholar] [CrossRef]
- Chandrashekar, P. Do mental health mobile apps work: Evidence and recommendations for designing high-efficacy mental health mobile apps. Mhealth 2018, 4, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yuan, S.; Ma, W.; Kanthawala, S.; Peng, W. Keep using my health apps: Discover users’ perception of health and fitness apps with the UTAUT2 model. Telemed. e-Health 2015, 21, 735–741. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.; Han, M. The Convergence Effect of the Willingness to use Smartphone Application on Therapeutic Lifestyle Change among People with Mental Illness. J. Korea Converg. Soc. 2018, 9, 325–335. [Google Scholar] [CrossRef]
- Kay, M.; Santos, J.; Takane, M. mHealth: New horizons for health through mobile technologies. World Health Organ. 2011, 64, 66–71. [Google Scholar]
- Carissoli, C.; Villani, D.; Riva, G. Does a meditation protocol supported by a mobile application help people reduce stress? Suggestions from a controlled pragmatic trial. Cyberpsychol. Behav. Soc. Netw. 2015, 18, 46–53. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Category | n (%) | Mean ± SD | ||
|---|---|---|---|---|
| Gender | Male | 22 (25.9) | ||
| Female | 63 (74.1) | |||
| Age (yr) | 30 and younger | 11 (12.9) | ||
| 31–40 | 28 (32.9) | |||
| 41–50 | 36 (42.4) | |||
| 51 and older | 6 (11.8) | |||
| Marriage | Unmarried | 24 (28.2) | ||
| Married | 61 (71.8) | |||
| Education | High shcool | 7 (8.2) | ||
| College | 58 (68.2) | |||
| Beyond college | 20 (23.5) | |||
| Income (millon Won) | <200 | 8 (9,.4) | ||
| 200 ~ <400 | 22 (25.9) | |||
| ≥400 | 55 (64.7) | |||
| BMI | Low weight | 1 (1.2) | 23.17 ± 2.71 | |
| Normal | 51 (60.0) | |||
| Overweight | 9 (10.6)) | |||
| Obesity | 24 (28.2) | |||
| Height | 164.47 ± 7.06 | |||
| Weight | 62.97 ± 10.04 | |||
| Working time | 8.25 ± 1.85 | |||
| Blood pressure | DBP | 118.53 ± 11.76 | ||
| SBP | 77.42 ± 9.37 | |||
| Health Status | Physical health | Not good | 10(11.8) | 3.3.4 ± 0.76 |
| Average | 41(48.2) | |||
| Good | 34(40.0) | |||
| Mental health | Not good | 8(9.4) | 3.46 ± 0.74 | |
| Average | 35(41.2) | |||
| Good | 42(49.5) | |||
| Variables | Pre-Test (M ± SD) | Post-Test (M ± SD) | t | p | |
|---|---|---|---|---|---|
| Stress | PSS | 15.56 ± 3.56 | 16.80 ± 3.67 | −3.431 | 0.001 |
| ERI | 35.49 ± 4.55 | 35.67 ± 4.4.4 | −0.423 | 0.673 | |
| Depression | 5.65 ± 4.53 | 4.80 ± 4.00 | 2.052 | 0.043 | |
| Anxiety | 3.92 ± 3.69 | 2.76 ± 2.85 | 3.037 | 0.003 | |
| Emotional labor | 55.77 ± 11.65 | 55.37 ± 11.82 | 0.343 | 0.732 | |
| Well-being | 51.62 ± 22.99 | 49.93 ± 22.92 | 0.689 | 0.493 | |
| PPG | 73.46 ± 5.43 | 64.83 ± 10.07 | 3.415 | 0.002 | |
| Question | Strongly Disagree | Disagree | Agree | Strongly Agree |
|---|---|---|---|---|
| Recognize the need for mental health management | 2(2.4) | 7(8.2) | 57(67.1) | 12(14.1) |
| Increased mental health management knowledge | 2(2.4) | 16(18.8) | 49(57.9) | 11(12.9) |
| Improving your attitude toward mental health | 3(3.5) | 13(15.3) | 54(63.5) | 8(9.4) |
| Motivation for stress management | 1(1.2) | 13(15.3) | 52(61.2) | 12(14.1) |
| Request for help | 2(2.4) | 18(21.2) | 45(52.9) | 13(15.3) |
| Behavior change | 3(3.5) | 23(27.1) | 46(54.1) | 6(7.1) |
| Question | Item | n (%) | |
|---|---|---|---|
| Satisfaction with app | Dissatisfied | 6(7.1) | |
| Usually | 38(44.7) | ||
| Satisfied | 34(40.0) | ||
| Would you recommend the app to others? | Nobody at all | 1(1.2) | |
| Few people | 18(21.2) | ||
| To a few people | 43(50.6) | ||
| To many people | 11(12.9) | ||
| To almost everyone | 5(5.9) | ||
| Subjective opinion | Benefits | Instant inspection result confirmation and interpretation Healing program that can be applied quickly and in a short time Various programs Easy to use, available anywhere | |
| Suggestions | Simplified survey Added alarm function for continuous use and interest Continuous content update Clarity of the user manual | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hwang, W.J.; Jo, H.H. Development and Effects of Cognitive Behavior-Based Healing Programs Using Mobile Apps. Int. J. Environ. Res. Public Health 2021, 18, 3334. https://doi.org/10.3390/ijerph18073334
Hwang WJ, Jo HH. Development and Effects of Cognitive Behavior-Based Healing Programs Using Mobile Apps. International Journal of Environmental Research and Public Health. 2021; 18(7):3334. https://doi.org/10.3390/ijerph18073334
Chicago/Turabian StyleHwang, Won Ju, and Hyun Hee Jo. 2021. "Development and Effects of Cognitive Behavior-Based Healing Programs Using Mobile Apps" International Journal of Environmental Research and Public Health 18, no. 7: 3334. https://doi.org/10.3390/ijerph18073334
APA StyleHwang, W. J., & Jo, H. H. (2021). Development and Effects of Cognitive Behavior-Based Healing Programs Using Mobile Apps. International Journal of Environmental Research and Public Health, 18(7), 3334. https://doi.org/10.3390/ijerph18073334