
Mediterranean Diet Implementation to Protect against Advanced Lung Cancer Index (ALI) Rise: Study Design and Preliminary Results of a Randomised Controlled Trial

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics
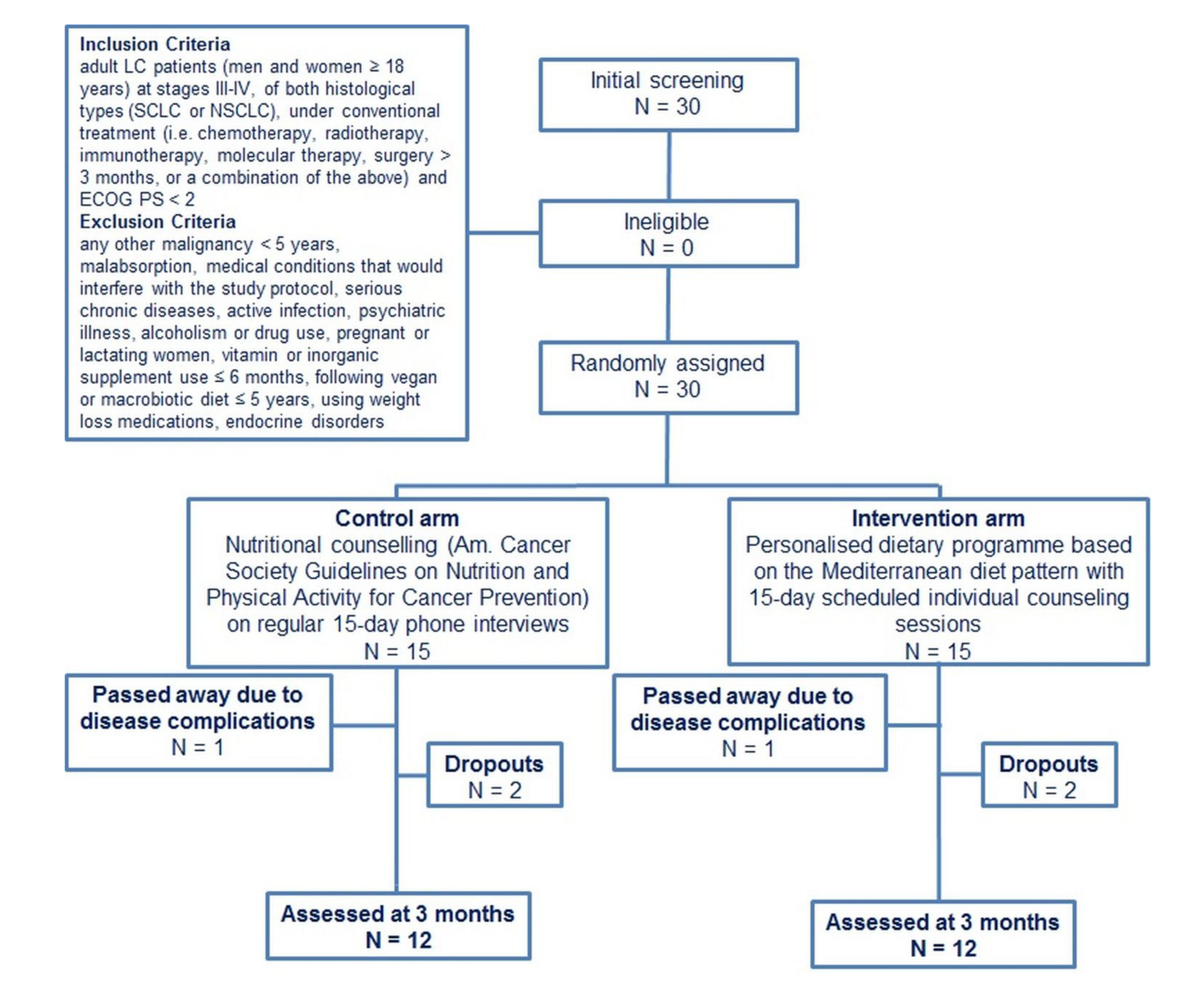
2.2. Participants
2.3. Study Design
2.4. Screening
2.5. Statistical Analysis
3. Results
3.1. Participants
3.2. Anthropometrics and Physical Activity
3.3. Blood Markers
3.4. Dietary Intake and Circulating Vitamins
3.5. Sample Size Calculation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization (WHO). Cancer: Key Facts. Available online: https://www.who.int/news-room/fact-sheets/detail/cancer (accessed on 3 March 2021).
- Didkowska, J.; Wojciechowska, U.; Mańczuk, M.; Łobaszewski, J. Lung cancer epidemiology: Contemporary and future challenges worldwide. Ann. Transl. Med. 2016, 4, 150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mouriño, A.; Ruano-Ravina, A.; Lorenzo-González, M.; Rodríguez-Martínez, Á.; Giraldo-Osorio, A.; Varela-Lema, L.; Pereiro-Brea, T.; Barros-Dios, J.M.; Valdés-Cuadrado, L.; Pérez-Ríos, M. Epidemiology of stage III lung cancer: Frequency, diagnostic characteristics, and survival. Casal. Transl. Lung Cancer Res. 2021, 10, 506–518. [Google Scholar] [CrossRef] [PubMed]
- Yang, P. Epidemiology of lung cancer prognosis: Quantity and quality of life. Methods Mol. Biol. 2009, 471, 469–486. [Google Scholar] [PubMed] [Green Version]
- Barta, J.A.; Powell, C.A.; Wisnivesky, J.P. Global epidemiology of lung cancer. Ann. Glob. Health 2019, 85, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peruga, A.; López, M.J.; Martinez, C.; Fernández, E. Tobacco control policies in the 21st century: Achievements and open challenges. Mol. Oncol. 2021, 15, 744–752. [Google Scholar] [CrossRef]
- Thun, M.J.; Carter, B.D.; Feskanich, D.; Freedman, N.D.; Prentice, R.; Lopez, A.D.; Hartge, P.; Gapstur, S.M. 50-year trends in smoking-related mortality in the United States. N. Engl. J. Med. 2013, 368, 351–364. [Google Scholar] [CrossRef] [Green Version]
- Goss, P.E.; Strasser-Weippl, K.; Lee-Bychkovsky, B.L.; Fan, L.; Li, J.; Chavarri-Guerra, Y.; Liedke, P.E.R.; Pramesh, C.S.; Badovinac-Crnjevic, T.; Sheikine, Y.; et al. Challenges to effective cancer control in China, India, and Russia. Lancet Oncol. 2014, 15, 489–538. [Google Scholar] [CrossRef]
- Mele, M.C.; Rinninella, E.; Cintoni, M.; Pulcini, G.; Di Donato, A.; Grassi, F.; Trestini, I.; Pozzo, C.; Tortora, G.; Gasbarrini, A.; et al. Nutritional support in lung cancer patients: The state of the art. Clin. Lung Cancer 2020, S1525–S7304, 30310–30317. [Google Scholar] [CrossRef]
- Kasprzyk, A.; Bilmin, K.; Chmielewska-Ignatowicz, T.; Pawlikowski, J.; Religioni, U.; Merks, P. The role of nutritional support in malnourished patients with lung cancer. In Vivo 2021, 35, 53–60. [Google Scholar] [CrossRef]
- Tanaka, K.; Akechi, T.; Okuyama, T.; Nishiwaki, Y.; Uchitomi, Y. Impact of dyspnea, pain, and fatigue on daily life activities in ambulatory patients with advanced lung cancer. J. Pain Symptom Manag. 2002, 23, 417–423. [Google Scholar] [CrossRef]
- Lemjabbar-Alaoui, H.; Hassan, O.U.I.; Yang, Y.W.; Buchanan, P. Lung cancer: Biology and treatment options. Biochim. Biophys. Acta Rev. Cancer 2015, 1856, 189–210. [Google Scholar] [CrossRef] [Green Version]
- Chabowski, M.; Polański, J.; Jankowska-Polańska, B.; Janczak, D.; Rosińczuk, J. Is nutritional status associated with the level of anxiety, depression and pain in patients with lung cancer? J. Thorac. Dis. 2018, 10, 2303–2310. [Google Scholar] [CrossRef] [Green Version]
- Jain, R.; Coss, C.; Whooley, P.; Phelps, M.; Owen, D.H. The role of malnutrition and muscle wasting in advanced lung cancer. Curr. Oncol. Rep. 2020, 22, 54. [Google Scholar] [CrossRef]
- Arends, J.; Bachmann, P.; Baracos, V.; Barthelemy, N.; Bertz, H.; Bozzetti, F.; Fearon, K.; Hütterer, E.; Isenring, E.; Kaasa, S.; et al. ESPEN guidelines on nutrition in cancer patients. Clin. Nutr. 2017, 36, 11–48. [Google Scholar] [CrossRef] [Green Version]
- Winther-Larsen, A.; Aggerholm-Pedersen, N.; Sandfeld-Paulsen, B. Inflammation scores as prognostic biomarkers in small cell lung cancer: A systematic review and meta-analysis. Syst. Rev. 2021, 10, 40. [Google Scholar] [CrossRef]
- Skouroliakou, M.; Grosomanidis, D.; Massara, P.; Kostara, C.; Papandreou, P.; Ntountaniotis, D.; Xepapadakis, G. Serum antioxidant capacity, biochemical profile and body composition of breast cancer survivors in a randomised Mediterranean dietary intervention study. Eur. J. Nutr. 2018, 57, 2133–2145. [Google Scholar] [CrossRef]
- Matalas, A.L. Disparities within traditional Mediterranean food patterns: An historical approach of the Greek diet. Int. J. Food Sci. Nutr. 2006, 57, 529–536. [Google Scholar] [CrossRef]
- UNESCO Representative List of the Intangible Cultural Heritage of Humanity. Available online: www.unesco.org/culture/ich/index.php?lg=en&pg=00011&RL=00394 (accessed on 20 October 2017).
- Hawrysz, I.; Wadolowska, L.; Slowinska, M.A.; Czerwinska, A.; Golota, J.J. Adherence to prudent and Mediterranean dietary patterns is inversely associated with lung cancer in moderate but not heavy male polish smokers: A case-control study. Nutrients 2020, 12, 3788. [Google Scholar] [CrossRef]
- Hodge, A.M.; Bassett, J.K.; Shivappa, N.; Hébert, J.R.; English, D.R.; Giles, G.G.; Severi, G. Dietary inflammatory index, Mediterranean diet score, and lung cancer: A prospective study. Cancer Causes Control 2016, 27, 907–917. [Google Scholar] [CrossRef] [Green Version]
- Lilenbaum, R.C.; Cashy, J.; Hensing, T.A.; Young, S.; Cella, D. Prevalence of poor performance status in lung cancer patients: Implications for research. J. Thorac. Oncol. 2008, 3, 125–129. [Google Scholar] [CrossRef] [Green Version]
- Kushi, L.H.; Doyle, C.; McCullough, M.; Rock, C.L.; Demark-Wahnefried, W.; Bandera, E.V.; Gapstur, S.; Patel, A.V.; Andrews, K.; Gansler, T.; et al. American Cancer Society 2010 Nutrition and Physical Activity Guidelines Advisory Committee. American Cancer Society Guidelines on nutrition and physical activity for cancer prevention: Reducing the risk of cancer with healthy food choices and physical activity. CA Cancer J. Clin. 2012, 62, 30–67. [Google Scholar]
- Kogiannou, D.A.A.; Kalogeropoulos, N.; Kefalas, P.; Polissiou, M.G.; Kaliora, A.C. Herbal infusions; their phenolic profile, antioxidant and anti-inflammatory effects in HT29 and PC3 cells. Food Chem. Toxicol. 2013, 61, 152–159. [Google Scholar] [CrossRef]
- Harasym, J.; Oledzki, R. Effect of fruit and vegetable antioxidants on total antioxidant capacity of blood plasma. Nutrition 2014, 30, 511–517. [Google Scholar] [CrossRef]
- Mourouti, N.; Papavagelis, C.; Psaltopoulou, T.; Aravantinos, G.; Samantas, E.; Filopoulos, E.; Manousou, A.; Plytzanopoulou, P.; Vassilakou, T.; Malamos, N.; et al. Aims, design and methods of a case-control study for the assessment of the role of dietary habits, eating behaviors and environmental factors, on the development of breast cancer. Maturitas 2013, 74, 31–36. [Google Scholar] [CrossRef]
- Panagiotakos, D.B.; Pitsavos, C.; Arvaniti, F.; Stefanadis, C. Adherence to the Mediterranean food pattern predicts the prevalence of hypertension, hypercholesterolemia, diabetes and obesity, among healthy adults, the accuracy of the MedDietScore. Prev. Med. 2007, 44, 335–340. [Google Scholar] [CrossRef]
- Papathanasiou, G.; Georgoudis, G.; Papandreou, M.; Spyropoulos, P.; Georgakopoulos, D.; Kalfakakou, V.; Evangelou, A. Reliability measures of the short International Physical Activity Questionnaire (IPAQ) in Greek young adults. Hellenic J. Cardiol. 2009, 50, 283–294. [Google Scholar] [PubMed]
- Jafri, S.H.; Shi, R.; Mills, G. Advance lung cancer inflammation index (ALI) at diagnosis is a prognostic marker in patients with metastatic non-small cell lung cancer (NSCLC): A retrospective review. BMC Cancer 2013, 13, 158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nierenberg, D.W.; Lester, D.C. Determination of vitamins A and E in serum and plasma using a simplified clarification method and high-performance liquid chromatography. J. Chromatogr. 1985, 345, 275–284. [Google Scholar] [CrossRef]
- Liau, L.S.; Lee, B.L.; New, A.L.; Ong, C.N. Determination of plasma ascorbic acid by high-performance liquid chromatography with ultraviolet and electrochemical detection. J. Chromatogr. 1993, 612, 63–70. [Google Scholar] [CrossRef]
- Johnston, C.S.; Corte, C. People with marginal vitamin C status are at high risk of developing vitamin C deficiency. J. Am. Diet Assoc. 1999, 99, 854–856. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Serum Retinol Concentrations for Determining the Prevalence of Vitamin A Deficiency in Populations. Vitamin and Mineral Nutrition Information System. Geneva, World Health Organization, 2011 (WHO/NMH/NHD/MNM/11.3). Available online: http://www.who.int/vmnis/indicators/retinol.pdf (accessed on 1 March 2021).
- Traber, M.G. Vitamin E inadequacy in humans: Causes and consequences. Adv. Nutr. 2014, 5, 503–514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peebles, K.A.; Lee, J.M.; Mao, J.T.; Hazra, S.; Reckamp, K.L.; Krysan, K.; Dohadwala, M.; Heinrich, E.L.; Walser, T.C.; Cui, X.; et al. Inflammation and lung carcinogenesis: Applying findings in prevention and treatment. Expert Rev. Anticancer Ther. 2007, 7, 1405–1421. [Google Scholar] [CrossRef] [PubMed]
- Yu, D.; Liu, B.; Zhang, L.; Du, K. Platelet count predicts prognosis in operable non-small cell lung cancer. Exp. Ther. Med. 2013, 5, 1351–1354. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tomita, M.; Ayabe, T.; Maeda, R.; Nakamura, K. Comparison of inflammation-based prognostic scores in patients undergoing curative resection for non-small cell lung cancer. World J. Oncol. 2018, 9, 85–90. [Google Scholar] [CrossRef] [Green Version]
- Hu, Z.; Wu, W.; Zhang, X.; Li, P.; Zhang, H.; Wang, H.; Xue, W.; Chen, Z.; Zhao, Q.; Duan, G. Advanced lung cancer inflammation index is a prognostic factor of patients with small-cell lung cancer following surgical resection. Cancer Manag. Res. 2021, 13, 2047–2055. [Google Scholar] [CrossRef]
- Zhang, Y.; Chen, B. Prognostic value of the advanced lung cancer inflammation index in patients with lung cancer: A meta-analysis. Dis. Markers 2019, 2019, 2513026. [Google Scholar] [CrossRef] [Green Version]
- MacDonald, N. Cancer cachexia and targeting chronic inflammation: A unified approach to cancer treatment and palliative/supportive care. J. Support Oncol. 2007, 5, 157–162. [Google Scholar]
- Yong, L.C.; Brown, C.C.; Schatzkin, A.; Dresser, C.M.; Slesinski, M.J.; Cox, C.S.; Taylor, P.R. Intake of vitamins E, C, and A and risk of lung cancer. The NHANES I epidemiologic follow up study. First National Health and Nutrition Examination Survey. Am. J. Epidemiol. 1997, 146, 231–243. [Google Scholar] [CrossRef] [Green Version]
- Rahman, Q.; Abidi, P.; Afaq, F.; Schiffmann, D.; Mossman, B.T.; Kamp, D.W.; Athar, M. Glutathione redox system in oxidative lung injury. Crit. Rev. Toxicol. 1999, 29, 543–568. [Google Scholar] [CrossRef]
- Alberg, A. The influence of cigarette smoking on circulating concentrations of antioxidant micronutrients. Toxicology 2002, 180, 121–137. [Google Scholar] [CrossRef]
- Dev, R.; Bruera, E.; Dalal, S. Insulin resistance and body composition in cancer patients. Ann. Oncol. 2018, 29, ii18–ii26. [Google Scholar] [CrossRef]
- Wagner, E.F.; Petruzzelli, M. Cancer metabolism: A waste of insulin interference. Nature 2015, 521, 430–431. [Google Scholar] [CrossRef]
- Staudacher, H.M.; Irving, P.M.; Lomer, M.C.E.; Whelan, K. The challenges of control groups, placebos and blinding in clinical trials of dietary interventions. Proc. Nutr. Soc. 2017, 76, 203–212. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Characteristics | Enrolled Patients (N = 30) | Control Group (N = 15) | MD Group (N = 15) | p-Value |
|---|---|---|---|---|
| Sex Males Females | 16 14 | 8 7 | 8 7 | - |
| Age (years) | 52.2 ± 27.3 | 52.9 ± 27.8 | 51.5 ± 27.7 | 0.891 |
| BMI (kg/m2) <18.5 18.5–24.9 25–29.9 >30 | 26.8 ± 5.5 2 9 12 7 | 27.4 ± 4.1 0 5 7 3 | 26.2 ± 6.6 2 4 5 4 | 0.550 - |
| BFM (Kg) | 27.8 ± 10.7 | 28.6 ± 9.1 | 26.9 ± 12.3 | 0.688 |
| % BFM | 37.0 ± 9.2 | 37.4 ± 7.3 | 36.7 ± 11.0 | 0.864 |
| LC type SCLC NSCLC | 3 27 | 2 13 | 1 15 | - |
| LC stage III IV | 5 25 | 2 13 | 3 12 | - |
| Smoking Yes In the past Never | 13 16 1 | 6 8 1 | 7 8 0 | - |
| Cigarettes per day by current smokers 1–5 6–14 15–24 25–34 | 13 4 4 3 2 | 2 2 1 1 | 2 2 2 1 | - |
| LC treatment Surgery (>3 months) Unoperated Combined chemo- radiotherapy Chemotherapy Immunotherapy Combined chemo- immunotherapy Molecular therapy | 7 23 12 3 4 3 1 | 2 13 5 1 3 3 1 | 5 10 7 2 1 0 0 | - |
| ECOG performance status Score 0 Score 1 | 25 5 | 13 2 | 12 3 | - |
| METS-min/week | 288.6 ± 106.7 | 287.1 ± 90.8 | 290.1 ± 123.8 | 0.940 |
| Hematocrit (%) | 38.2 ± 5.0 | 38.9 ± 5.3 | 37.4 ± 4.8 | 0.447 |
| Hemoglobin (g/dL) | 12.4 ± 1.8 | 12.7 ± 1.8 | 12.2 ± 1.7 | 0.438 |
| White blood cell (K/μL) | 5.3 × 103 ± 3.4 × 103 | 5.5 × 103 ± 3.3 × 103 | 5.1 × 103 ± 3.6 × 103 | 0.766 |
| Neutrophils (%) | 62.4 ± 12.6 | 64.3 ± 13.2 | 60.3 ± 11.9 | 0.398 |
| Lymphocytes (%) | 25.6 ± 10.8 | 23.6 ± 11.4 | 27.8 ± 10.0 | 0.301 |
| NLR | 3.2 ± 2.1 | 3.8 ± 2.6 | 2.5 ± 1.1 | 0.100 |
| Platelets (K/μL) | 241.5 × 103 ± 94.9 × 103 | 256.1 × 103 ± 76.1 × 103 | 226.8 × 103 ± 111.4 × 103 | 0.407 |
| Glucose (mg/dL) | 103.8 ± 20.6 | 99.9 ± 16.4 | 107.9 ± 24.2 | 0.304 |
| Total cholesterol (mg/dL) | 201.5 ± 40.1 | 209.1 ± 42.0 | 193.4 ± 37.6 | 0.300 |
| HDL (mg/dL) | 53.3 ± 17.5 | 55.2 ± 20.5 | 51.3 ± 14.1 | 0.562 |
| LDL (mg/dL) | 126.8 ± 33.3 | 134.9 ± 31.1 | 118.1 ± 34.4 | 0.179 |
| Triacylglycerols (mg/dL) | 132.8 ± 96.3 | 141.3 ± 116.6 | 122.8 ± 69.3 | 0.622 |
| Albumin (g/dL) | 4.2 ± 0.4 | 4.1 ± 0.3 | 4.2 ± 0.4 | 0.630 |
| Vitamin A (mg/L) | 0.5 ± 0.3 | 0.5 ± 0.2 | 0.6 ± 0.3 | 0.579 |
| Vitamin C (mg/L) | 6.0 ± 2.4 | 5.5 ± 2.7 | 6.5 ± 2.0 | 0.258 |
| Vitamin E (mg/L) | 13.1 ± 4.8 | 13.2 ± 4.5 | 13.1 ± 5.3 | 0.977 |
| CRP (mg/L) | 11.2 ± 13.6 | 12.3 ± 13.4 | 10.1 ± 14.3 | 0.667 |
| ALI | 47.2 ± 29.9 | 45.0 ± 31.8 | 49.3 ± 28.9 | 0.704 |
| MD score | 30.8 ± 4.8 | 31.7 ± 4.8 | 29.9 ± 4.7 | 0.311 |
| Sugars (g/day) | 60.8 ± 23.1 | 56.5 ± 24.5 | 65.2 ± 21.5 | 0.314 |
| SFAs (g/day) | 30.5 ± 9.5 | 27.6 ± 7.2 | 33.3 ±10.8 | 0.101 |
| PUFAs (g/day) | 13.6 ± 8.0 | 13.7 ± 5.9 | 13.6 ± 9.8 | 0.975 |
| MUFAs (g/day) | 24.3 ± 10.2 | 27.2 ± 12.1 | 21.5 ± 7.2 | 0.127 |
| Fibers (g/day) | 4.0 ± 2.7 | 4.4 ± 3.1 | 3.5 ± 2.2 | 0.385 |
| Vitamin C (mg/day) | 80.5 ± 42.6 | 88.4 ± 37.7 | 72.6 ± 46.8 | 0.319 |
| Vitamin A RAE (mcg/day) | 596.8 ± 698.6 | 590.1 ± 566.9 | 603.5 ± 830.3 | 0.959 |
| alpha-tocopherol (mcg/day) | 7.4 ± 2.7 | 7.4 ± 2.5 | 7.3 ± 3.0 | 0.968 |
| Parameter | Group | Baseline (N = 12) | 3 Months (N = 12) | p-Value | * p-Value |
|---|---|---|---|---|---|
| Mean ± SD | Mean ± SD | ||||
| BMI (kg/m2) <18.5 18.5–24.99 25–30 >30 | control | 27.5 ± 4.7 0 5 4 3 | 25.7 ± 3.1 0 5 5 2 | 0.133 - - - - | 0.138 |
| MD | 26.3 ± 6.9 1 (8.3) 4 (33.3) 4 (33.3) 3 (25) | 26.4 ± 6.4 1 (8.3) 5 (41.7) 4 (33.3) 2 (16.7) | 0.916 - - - - | ||
| Body fat mass (kg) | control | 26.2 ± 7.3 | 26.7 ± 8.1 | 0.446 | 0.401 |
| MD | 26.0 ± 12.8 | 26.2 ± 11.2 | 0.818 | ||
| % body fat mass | control | 36.4 ± 7.4 | 36.8 ± 7.2 | 0.514 | 0.366 |
| MD | 34.7 ± 10.5 | 35.4 ± 8.0 | 0.665 | ||
| METS-min/week | control | 283.8 ± 97.5 | 323.0 ± 84.2 | 0.128 | 0.711 |
| MD | 298.2 ± 112.4 | 350.0 ± 109.6 | 0.053 | ||
| Current smokers | control | 5 (41.7) | 3 25.0) | - | - |
| MD | 6 (50) | 2 (16.7) | - | - | |
| Hematocrit (%) | control | 39.4 ± 4.2 | 39.2 ± 4.4 | 0.795 | 0.477 |
| MD | 37.0 ± 5.0 | 38.0 ± 3.1 | 0.509 | ||
| Hemoglobin (g/dL) | control | 12.8 ± 1.4 | 12.7 ± 1.5 | 0.545 | 0.311 |
| MD | 12.0 ± 1.7 | 12.3 ± 1.2 | 0.422 | ||
| White blood cell (K/μL) | control | 4.6 × 103 ± 3.0 × 103 | 3.4 × 103 ± 2.8 × 103 | 0.124 | 0.144 |
| MD | 5.2 × 103 ± 3.9 × 103 | 6.0 × 103 ± 3.2 × 103 | 0.482 | ||
| Neutrophils (%) | control | 61.1 ± 12.7 | 58.8 ± 13.0 | 0.460 | 0.158 |
| MD | 62.2 ± 9.4 | 65.0 ± 9.9 | 0.150 | ||
| Lymphocytes (%) | control | 26.8 ± 10.6 | 29.9 ± 13.0 | 0.299 | 0.088 |
| MD | 26.8 ± 8.8 | 24.2 ± 9.8 | 0.090 | ||
| NLR | control | 2.9 ± 2.1 | 2.8 ± 2.2 | 0.723 | 0.174 |
| MD | 2.6 ± 1.0 | 3.2 ± 1.6 | 0.071 | ||
| Platelets (K/μL) | control | 252.7 × 103 ± 74.8 × 103 | 214.0 × 103 ± 164.8 × 103 | 0.372 | 0.441 |
| MD | 256.9 × 103 ± 96.1 × 103 | 175.3 × 103 ± 133.1 × 103 | 0.044 | ||
| Glucose (mg/dL) | control | 100.3 ± 17.1 | 114.6 ± 34.5 | 0.059 | 0.017 |
| MD | 108.7 ± 26.2 | 104.4 ± 18.1 | 0.368 | ||
| Cholesterol (mg/dL) | control | 207.8 ± 42.8 | 209.3 ± 38.5 | 0.898 | 0.394 |
| MD | 185.7 ± 34.5 | 200.7 ± 32.7 | 0.183 | ||
| HDL (mg/dL) | control | 58.1 ± 21.5 | 51.6 ± 17.7 | 0.066 | 0.093 |
| MD | 50.8 ± 15.1 | 52.8 ± 14.3 | 0.600 | ||
| LDL (mg/dL) | control | 132.8 ± 26.0 | 130.1 ± 26.7 | 0.753 | 0.302 |
| MD | 110.4 ± 29.4 | 119.3 ± 25.7 | 0.229 | ||
| Triacylglycerols (mg/dL) | control | 108.7 ± 43.4 | 148.6 ± 113.1 | 0.113 | 0.409 |
| MD | 125.9 ± 71.4 | 143.3 ± 85.7 | 0.225 | ||
| Albumin (g/dl) | control | 4.2 ± 0.3 | 4.1 ± 0.4 | 0.435 | 0.095 |
| MD | 4.2 ± 0.4 | 4.4 ± 0.6 | 0.142 | ||
| Vitamin A (mg/L) | control | 0.5 ± 0.1 | 0.5 ± 0.2 | 0.886 | 0.274 |
| MD | 0.6 ± 0.3 | 0.5 ± 0.1 | 0.223 | ||
| Vitamin C (mg/L) | control | 5.9 ± 2.8 | 5.2 ± 4.4 | 0.693 | 0.442 |
| MD | 6.4 ± 2.0 | 7.2 ± 3.8 | 0.402 | ||
| Vitamin E (mg/L) | control | 13.5 ± 4.8 | 14.9 ± 3.2 | 0.402 | 0.630 |
| MD | 13.3 ± 5.4 | 13.7 ± 5.7 | 0.768 | ||
| CRP (mg/L) | control | 9.4 ± 11.7 | 11.9 ± 18.3 | 0.687 | 0.193 |
| MD | 11.6 ± 14.9 | 3.8 ± 4.1 | 0.116 | ||
| ALI | control | 55.0 ± 27.1 | 78.4 ± 30.6 | 0.025 | 0.003 |
| MD | 48.2 ± 20.9 | 45.2 ± 18.7 | 0.542 | ||
| MD score | control | 31.6 ± 3.2 | 33.1 ± 5.1 | 0.163 | 0.031 |
| MD | 29.2 ± 5.9 | 34.7 ± 3.7 | 0.004 | ||
| Sugars (g/d) | control | 56.8 ± 25.8 | 55.0 ± 22.9 | 0.835 | 0.980 |
| MD | 69.0 ± 21.2 | 67.5 ± 18.2 | 0.848 | ||
| SFAs (g/d) | control | 27.6 ± 7.1 | 23.1 ± 8.7 | 0.172 | 0.279 |
| MD | 35.0 ± 11.3 | 26.2 ± 11.5 | 0.006 | ||
| PUFAs (g/d) | control | 13.4 ± 6.5 | 11.7 ± 6.7 | 0.398 | 0.838 |
| MD | 15.0 ± 11.1 | 14.2 ± 8.1 | 0.832 | ||
| MUFAs (g/d) | control | 27.1 ± 14.2 | 27.9 ± 13.9 | 0.858 | 0.102 |
| MD | 21.4 ± 8.5 | 30.4 ± 5.8 | 0.002 | ||
| Fibers (g/d) | control | 3.9 ± 3.3 | 3.8 ± 2.5 | 0.930 | 0.025 |
| MD | 4.1 ± 2.3 | 8.5 ± 4.0 | 0.005 | ||
| Vitamin C (mg/day) | control | 85.2 ± 44.1 | 50.7 ± 33.3 | 0.097 | 0.004 |
| MD | 67.6 ± 52.4 | 139.2 ± 63.7 | 0.024 | ||
| Vitamin A RAE (mcg/day) | control | 789.2 ± 906.3 | 356.1 ± 663.9 | 0.655 | 0.872 |
| MD | 490.5 ± 646.0 | 581.3 ± 430.3 | 0.559 | ||
| alpha-tocopherol (mcg/day) | control | 7.7 ± 3.4 | 6.2 ± 2.4 | 0.124 | 0.497 |
| MD | 7.8 ± 2.6 | 7.5 ± 5.2 | 0.898 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gioxari, A.; Tzanos, D.; Kostara, C.; Papandreou, P.; Mountzios, G.; Skouroliakou, M. Mediterranean Diet Implementation to Protect against Advanced Lung Cancer Index (ALI) Rise: Study Design and Preliminary Results of a Randomised Controlled Trial. Int. J. Environ. Res. Public Health 2021, 18, 3700. https://doi.org/10.3390/ijerph18073700
Gioxari A, Tzanos D, Kostara C, Papandreou P, Mountzios G, Skouroliakou M. Mediterranean Diet Implementation to Protect against Advanced Lung Cancer Index (ALI) Rise: Study Design and Preliminary Results of a Randomised Controlled Trial. International Journal of Environmental Research and Public Health. 2021; 18(7):3700. https://doi.org/10.3390/ijerph18073700
Chicago/Turabian StyleGioxari, Aristea, Dimitrios Tzanos, Christina Kostara, Panos Papandreou, Giannis Mountzios, and Maria Skouroliakou. 2021. "Mediterranean Diet Implementation to Protect against Advanced Lung Cancer Index (ALI) Rise: Study Design and Preliminary Results of a Randomised Controlled Trial" International Journal of Environmental Research and Public Health 18, no. 7: 3700. https://doi.org/10.3390/ijerph18073700
APA StyleGioxari, A., Tzanos, D., Kostara, C., Papandreou, P., Mountzios, G., & Skouroliakou, M. (2021). Mediterranean Diet Implementation to Protect against Advanced Lung Cancer Index (ALI) Rise: Study Design and Preliminary Results of a Randomised Controlled Trial. International Journal of Environmental Research and Public Health, 18(7), 3700. https://doi.org/10.3390/ijerph18073700