
Association between Dietary Fibre Intake and Colorectal Adenoma: A Systematic Review and Meta-Analysis

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy and Data Sources
2.2. Inclusion/Exclusion Criteria
2.3. Data Extraction
2.4. Critical Appraisal
2.5. Statistical Analysis
2.6. Sub-Group and Sensitivity Analysis
2.7. Cumulative Analysis
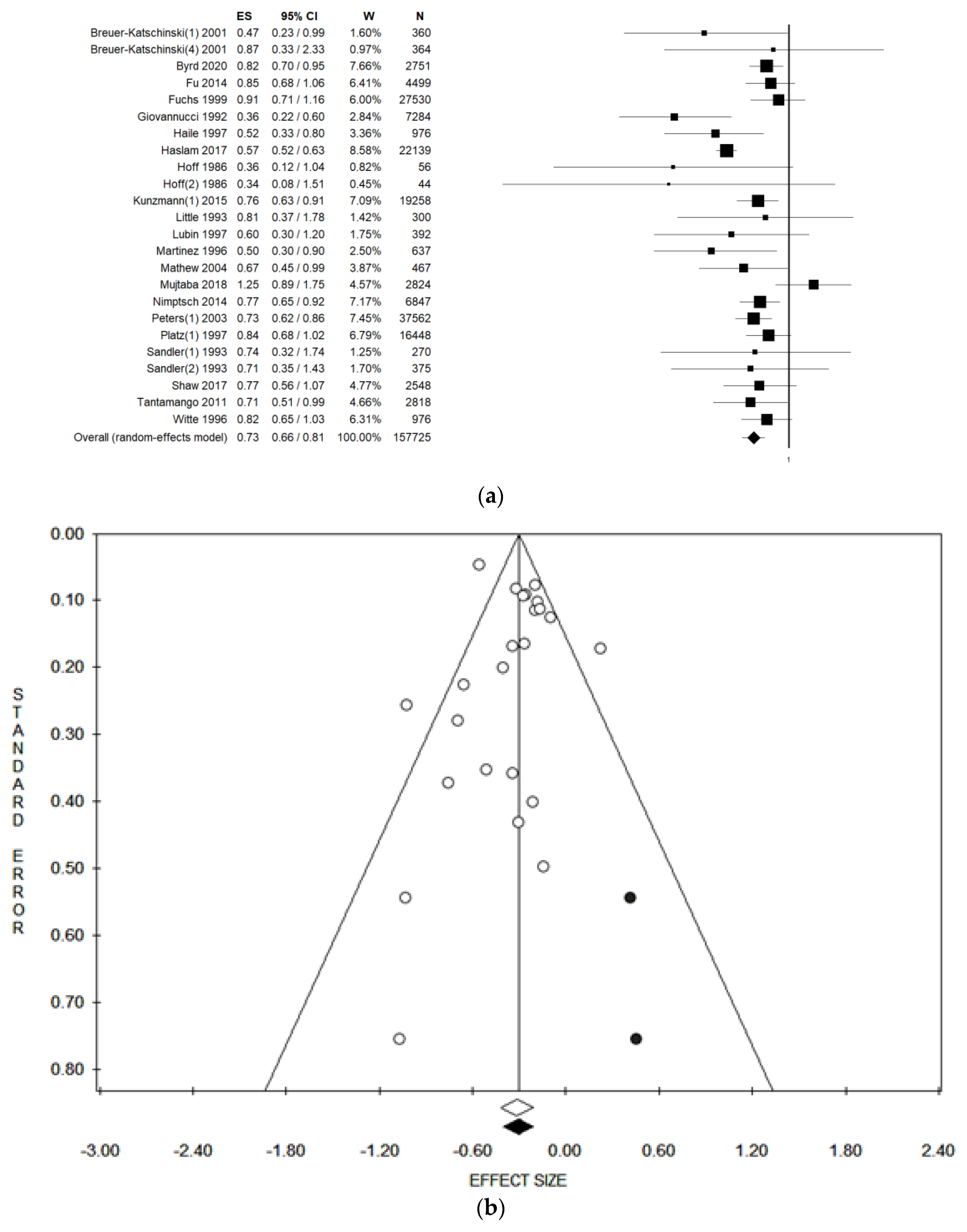
3. Results
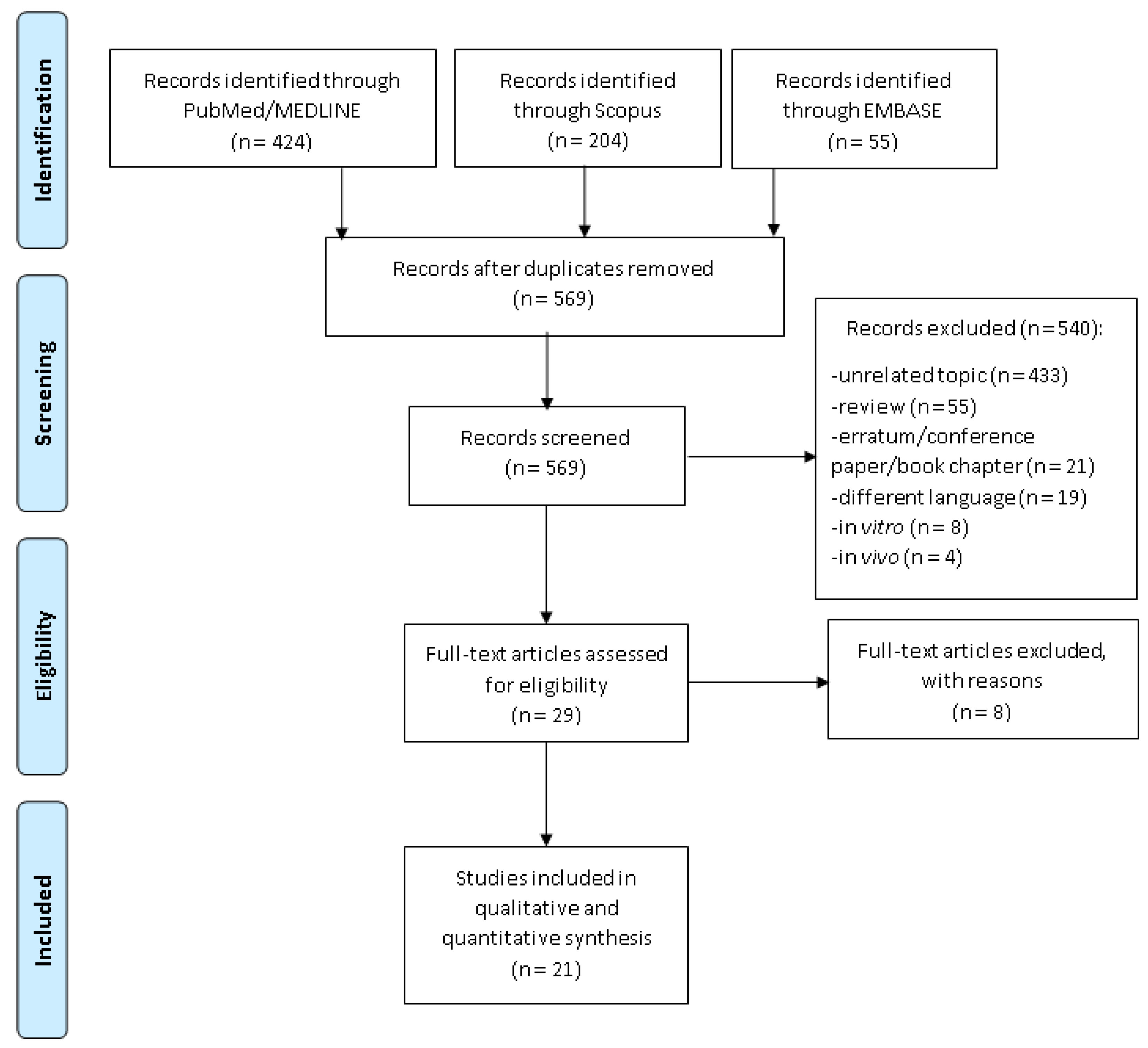
3.1. Literature Search
3.2. Characteristics of Included Studies
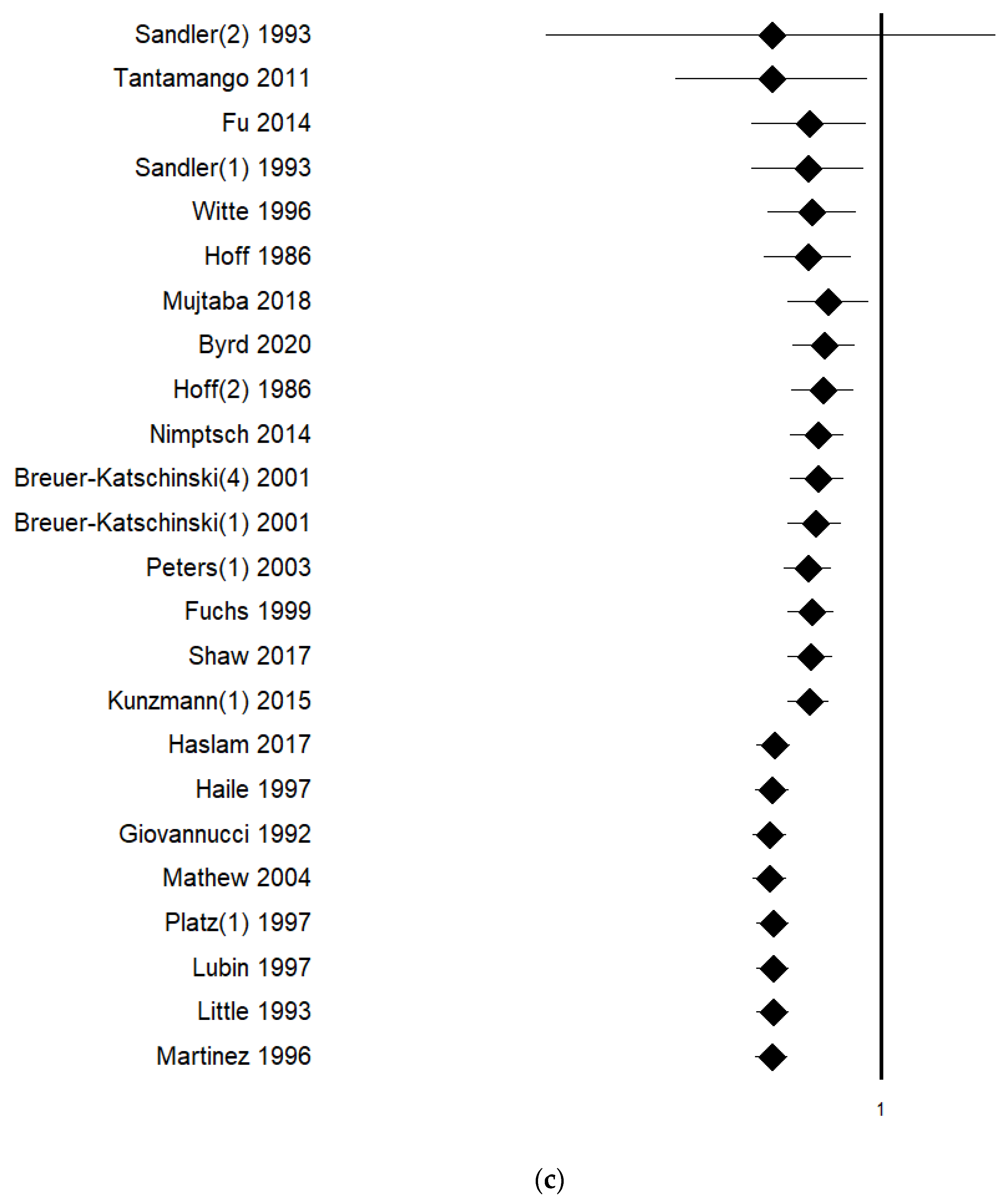
3.3. Sub-Group and Sensitivity Analysis
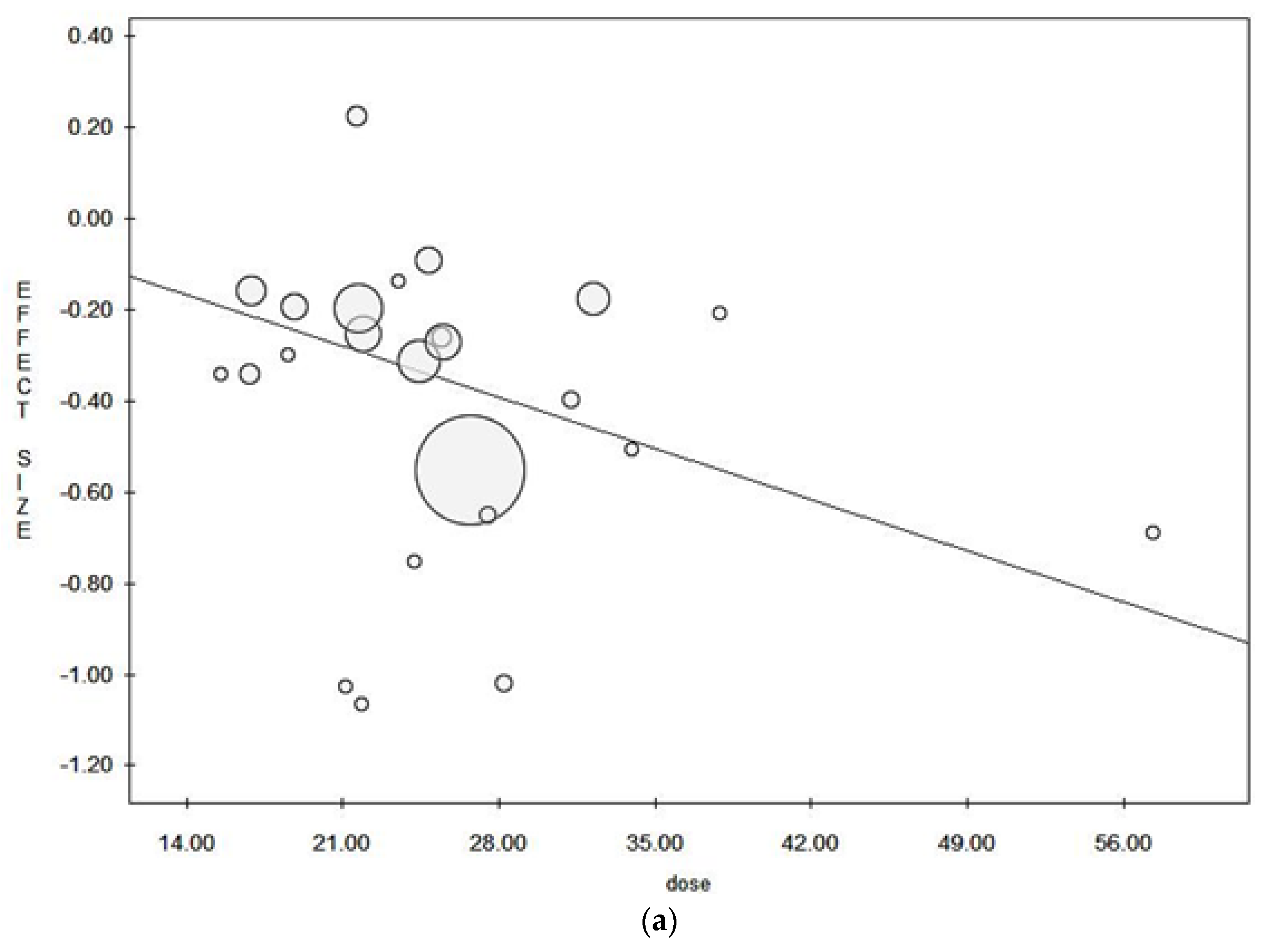
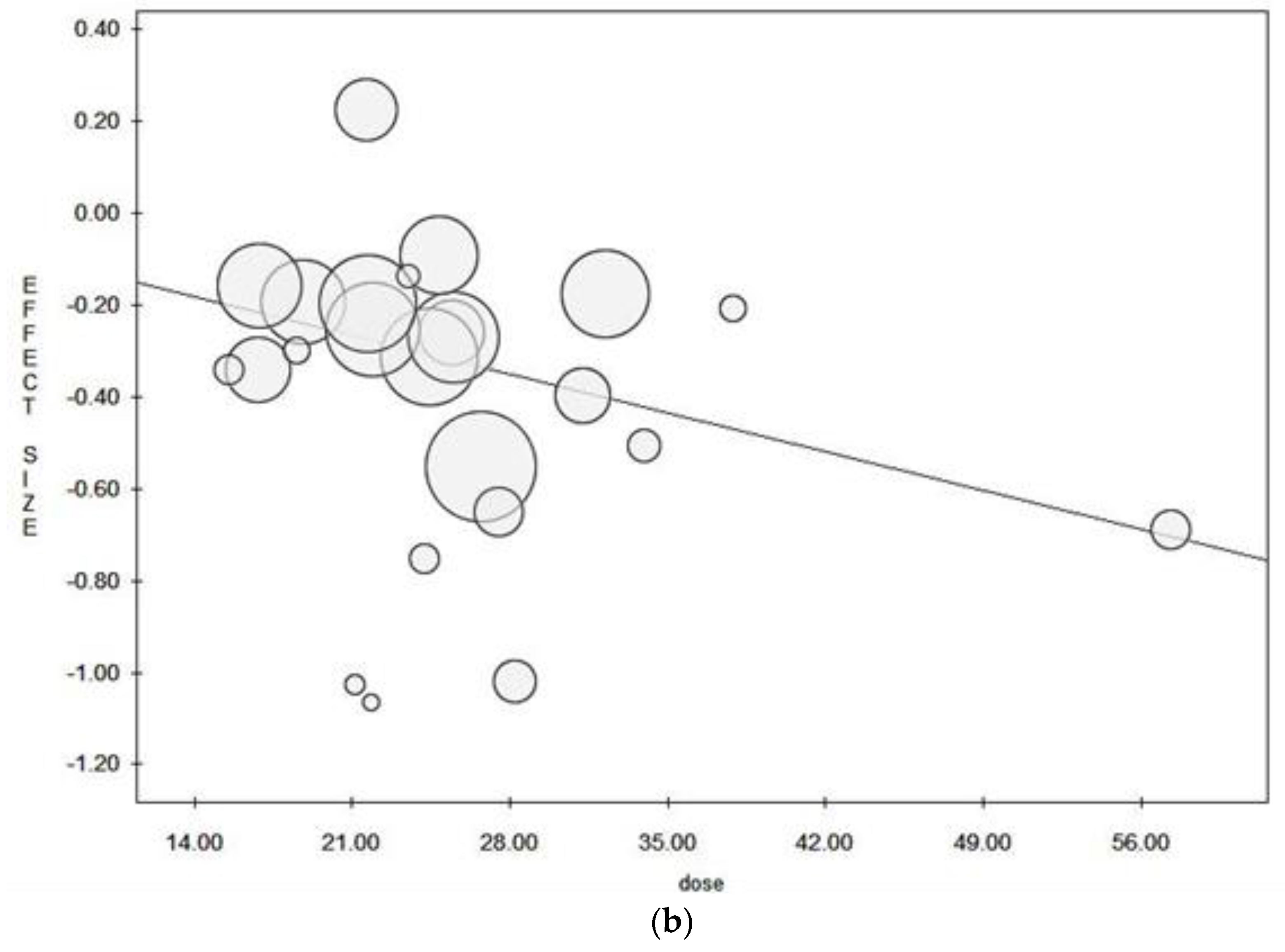
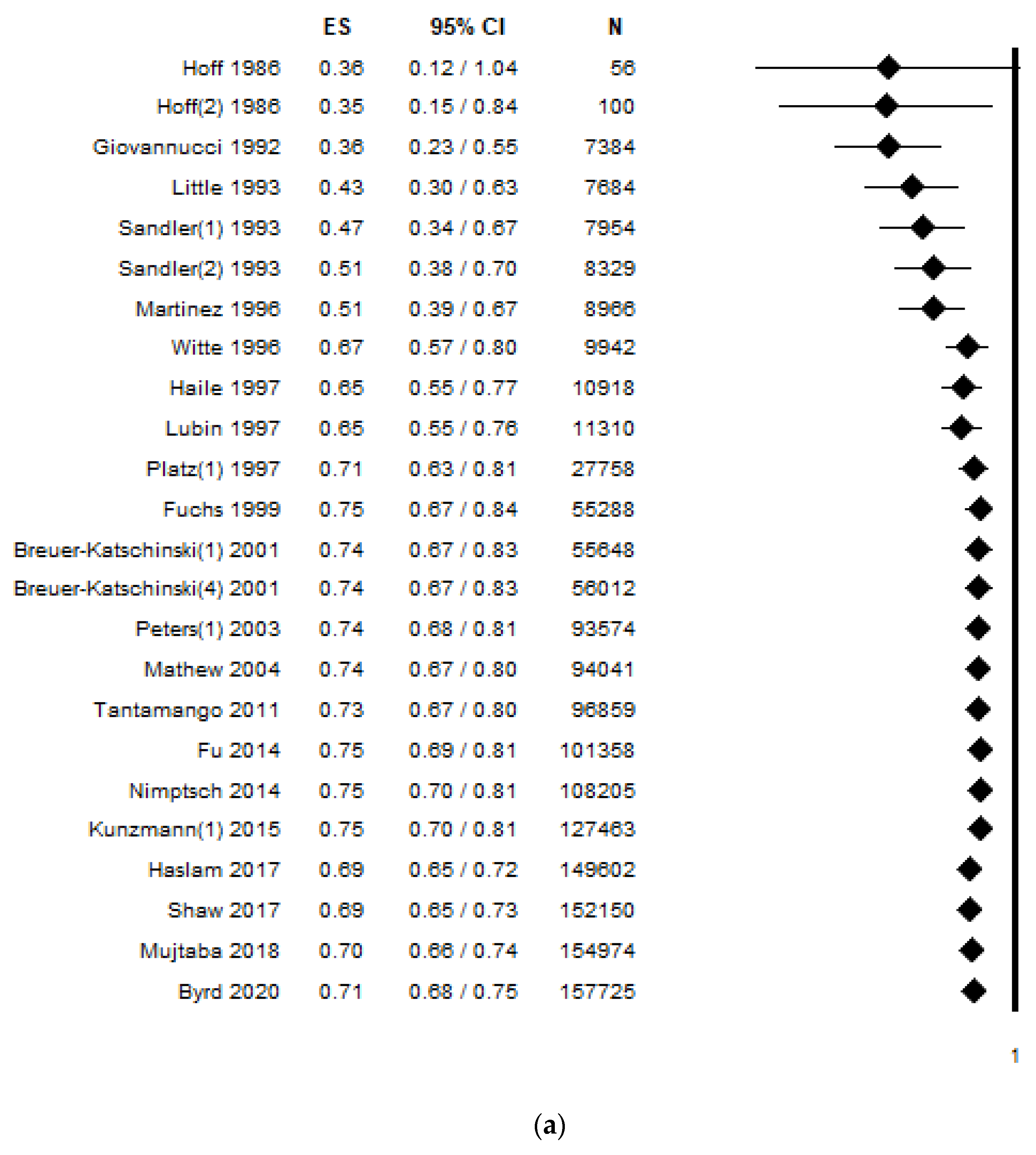
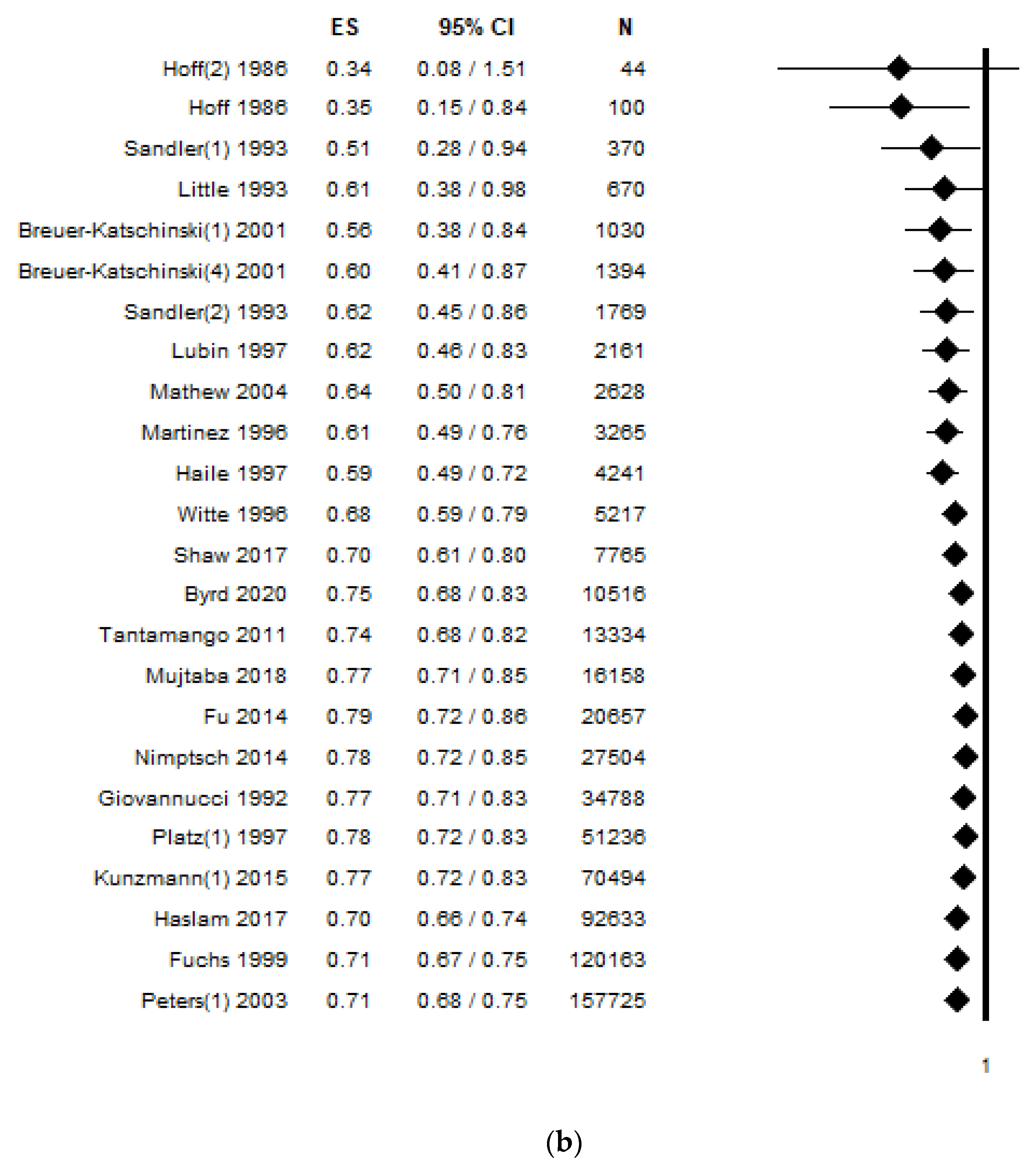
3.4. Cumulative Analysis
4. Discussion
4.1. Potential Biological Mechanisms
4.2. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- International Agency for Research on Cancer. World Cancer Report: Cancer Research for Cancer Prevention; Wild, C.P., Weiderpass, E., Stewart, B.W., Eds.; International Agency for Research on Cancer (IARC): Lyon, France, 2020. [Google Scholar]
- Schreuders, E.H.; Ruco, A.; Rabeneck, L.; Schoen, R.E.; Sung, J.J.; Young, G.P.; Kuipers, E.J. Colorectal cancer screening: A global overview of existing programmes. Gut 2015, 64, 1637–1649. [Google Scholar] [CrossRef]
- Centres for Diseases Control and Prevention. Colorectal Cancer Screening Tests. Available online: https://www.cdc.gov/cancer/colorectal/basic_info/screening/tests.htm (accessed on 20 February 2021).
- Fleming, M.; Ravula, S.; Tatishchev, S.F.; Wang, H.L. Colorectal carcinoma: Pathologic aspects. J. Gastrointest Oncol. 2012, 3, 153–173. [Google Scholar] [CrossRef]
- World Cancer Research Fund. Diet, Nutrition, Physical Activity and Colorectal Cancer. Available online: https://www.wcrf.org/sites/default/files/Colorectal-cancer-report.pdf (accessed on 13 March 2021).
- Gianfredi, V.; Salvatori, T.; Villarini, M.; Moretti, M.; Nucci, D.; Realdon, S. Is dietary fibre truly protective against colon cancer? A systematic review and meta-analysis. Int. J. Food Sci. Nutr. 2018, 69, 904–915. [Google Scholar] [CrossRef]
- Gianfredi, V.; Nucci, D.; Salvatori, T.; Dallagiacoma, G.; Fatigoni, C.; Moretti, M.; Realdon, S. Rectal Cancer: 20% Risk Reduction Thanks to Dietary Fibre Intake. Systematic Review and Meta-Analysis. Nutrients 2019, 11, 1579. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B. Meta-analysis of observational studies in epidemiology: A proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA 2000, 283, 2008–2012. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. Ann. Intern. Med. 2009, 151, W65–W94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.T.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions. Version 5.1.0.; The Cochrane Collaboration: London, UK, 2013. [Google Scholar]
- Brown, P.; Brunnhuber, K.; Chalkidou, K.; Chalmers, I.; Clarke, M.; Fenton, M.; Forbes, C.; Glanville, J.; Hicks, N.J.; Moody, J.; et al. How to formulate research recommendations. BMJ Clin. Res. Ed. 2006, 333, 804–806. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gianfredi, V.; Salvatori, T.; Nucci, D.; Villarini, M.; Moretti, M. Can chocolate consumption reduce cardio-cerebrovascular risk? A systematic review and meta-analysis. Nutrition 2018, 46, 103–114. [Google Scholar] [CrossRef] [PubMed]
- Gianfredi, V.; Bragazzi, N.L.; Nucci, D.; Villarini, M.; Moretti, M. Cardiovascular diseases and hard drinking waters: Implications from a systematic review with meta-analysis of case-control studies. J. Water Health 2017, 15, 31–40. [Google Scholar] [CrossRef]
- Wells, G.A.; Shea, B.; O’Connell, D.; Paterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 15 November 2020).
- Herzog, R.; Alvarez-Pasquin, M.J.; Diaz, C.; Del Barrio, J.L.; Estrada, J.M.; Gil, A. Are healthcare workers’ intentions to vaccinate related to their knowledge, beliefs and attitudes? A systematic review. BMC Public Health 2013, 13, 154. [Google Scholar] [CrossRef] [Green Version]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ Clin. Res. Ed. 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duval, S.; Tweedie, R. A nonparametric ”Trim and Fill” method of accounting for Publication Bias in Meta-Analysis. J. Am. Stat. Assoc. 2000, 95, 89–98. [Google Scholar] [CrossRef]
- Leimu, R.; Koricheva, J. Cumulative meta-analysis: A new tool for detection of temporal trends and publication bias in ecology. Proc. Biol. Sci. 2004, 271, 1961–1966. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Austin, G.L.; Adair, L.S.; Galanko, J.A.; Martin, C.F.; Satia, J.A.; Sandler, R.S. A diet high in fruits and low in meats reduces the risk of colorectal adenomas. J. Nutr. 2007, 137, 999–1004. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benito, E.; Cabeza, E.; Moreno, V.; Obrador, A.; Bosch, F.X. Diet and colorectal adenomas: A case-control study in Majorca. Int. J. Cancer 1993, 55, 213–219. [Google Scholar] [CrossRef] [PubMed]
- Haslam, A.; Wagner Robb, S.; Hébert, J.R.; Huang, H.; Ebell, M.H. Association between dietary pattern scores and the prevalence of colorectal adenoma considering population subgroups. Nutr. Diet. J. Dietit. Assoc. Aust. 2018, 75, 167–175. [Google Scholar] [CrossRef]
- Kopp, T.I.; Vogel, U.; Tjonneland, A.; Andersen, V. Meat and fiber intake and interaction with pattern recognition receptors (TLR1, TLR2, TLR4, and TLR10) in relation to colorectal cancer in a Danish prospective, case-cohort study. Am. J. Clin. Nutr. 2018, 107, 465–479. [Google Scholar] [CrossRef] [Green Version]
- Kune, G.A.; Kune, S.; Read, A.; MacGowan, K.; Penfold, C.; Watson, L.F. Colorectal polyps, diet, alcohol, and family history of colorectal cancer: A case-control study. Nutr. Cancer 1991, 16, 25–30. [Google Scholar] [CrossRef]
- Macquart-Moulin, G.; Riboli, E.; Cornee, J.; Kaaks, R.; Berthezene, P. Colorectal polyps and diet: A case-control study in Marseilles. Int. J. Cancer 1987, 40, 179–188. [Google Scholar] [CrossRef]
- Neugut, A.I.; Garbowski, G.C.; Lee, W.C.; Murray, T.; Nieves, J.W.; Forde, K.A.; Treat, M.R.; Waye, J.D.; Fenoglio-Preiser, C. Dietary risk factors for the incidence and recurrence of colorectal adenomatous polyps. A case-control study. Ann. Intern. Med. 1993, 118, 91–95. [Google Scholar] [CrossRef] [PubMed]
- Zheng, X.; Nguyen, L.H.; Liu, P.H.; Wu, K.; Smith-Warner, S.; Willett, W.; Chan, A.T.; Giovannucci, E.; Cao, Y. Comprehensive assessment of diet quality and risk of early-onset colorectal adenoma. Gastroenterology 2019, 156, S208. [Google Scholar] [CrossRef]
- Breuer-Katschinski, B.; Nemes, K.; Marr, A.; Rump, B.; Leiendecker, B.; Breuer, N.; Goebell, H.; Colorectal Adenoma Study, G. Colorectal adenomas and diet: A case-control study. Colorectal Adenoma Study Group. Dig. Dis. Sci. 2001, 46, 86–95. [Google Scholar] [CrossRef] [PubMed]
- Byrd, D.A.; Judd, S.; Flanders, W.D.; Hartman, T.J.; Fedirko, V.; Bostick, R.M. Associations of Novel Dietary and Lifestyle Inflammation Scores with Incident, Sporadic Colorectal Adenoma. Cancer Epidemiol. Biomarkers Prev. 2020, 29, 2300–2308. [Google Scholar] [CrossRef] [PubMed]
- Fu, Z.; Shrubsole, M.J.; Smalley, W.E.; Ness, R.M.; Zheng, W. Associations between dietary fiber and colorectal polyp risk differ by polyp type and smoking status. J. Nutr. 2014, 144, 592–598. [Google Scholar] [CrossRef] [Green Version]
- Fuchs, C.S.; Giovannucci, E.L.; Colditz, G.A.; Hunter, D.J.; Stampfer, M.J.; Rosner, B.; Speizer, F.E.; Willett, W.C. Dietary fiber and the risk of colorectal cancer and adenoma in women. N. Engl. J. Med. 1999, 340, 169–176. [Google Scholar] [CrossRef] [Green Version]
- Giovannucci, E.; Stampfer, M.J.; Colditz, G.; Rimm, E.B.; Willett, W.C. Relationship of diet to risk of colorectal adenoma in men. J. Natl. Cancer Inst. 1992, 84, 91–98. [Google Scholar] [CrossRef]
- Haile, R.W.; Witte, J.S.; Longnecker, M.P.; Probst-Hensch, N.; Chen, M.J.; Harper, J.; Frankl, H.D.; Lee, E.R. A sigmoidoscopy-based case-control study of polyps: Macronutrients, fiber and meat consumption. Int. J. Cancer 1997, 73, 497–502. [Google Scholar] [CrossRef]
- Haslam, A.; Wagner Robb, S.; Hebert, J.R.; Huang, H.; Wirth, M.D.; Shivappa, N.; Ebell, M.H. The association between Dietary Inflammatory Index scores and the prevalence of colorectal adenoma. Public Health Nutr. 2017, 20, 1609–1616. [Google Scholar] [CrossRef] [Green Version]
- Hoff, G.; Moen, I.E.; Trygg, K.; Frolich, W.; Sauar, J.; Vatn, M.; Gjone, E.; Larsen, S. Epidemiology of polyps in the rectum and sigmoid colon. Evaluation of nutritional factors. Scand. J. Gastroenterol. 1986, 21, 199–204. [Google Scholar] [CrossRef]
- Kunzmann, A.T.; Coleman, H.G.; Huang, W.Y.; Kitahara, C.M.; Cantwell, M.M.; Berndt, S.I. Dietary fiber intake and risk of colorectal cancer and incident and recurrent adenoma in the Prostate, Lung, Colorectal, and Ovarian Cancer Screening Trial. Am. J. Clin. Nutr. 2015, 102, 881–890. [Google Scholar] [CrossRef]
- Little, J.; Logan, R.F.; Hawtin, P.G.; Hardcastle, J.D.; Turner, I.D. Colorectal adenomas and diet: A case-control study of subjects participating in the Nottingham faecal occult blood screening programme. Br. J. Cancer 1993, 67, 177–184. [Google Scholar] [CrossRef] [Green Version]
- Lubin, F.; Rozen, P.; Arieli, B.; Farbstein, M.; Knaani, Y.; Bat, L.; Farbstein, H. Nutritional and lifestyle habits and water-fiber interaction in colorectal adenoma etiology. Am. Assoc. Cancer Res. 1997, 6, 79–85. [Google Scholar]
- Martinez, M.E.; McPherson, R.S.; Annegers, J.F.; Levin, B. Association of diet and colorectal adenomatous polyps: Dietary fiber, calcium, and total fat. Epidemiology 1996, 7, 264–268. [Google Scholar] [CrossRef] [Green Version]
- Mathew, A.; Peters, U.; Chatterjee, N.; Kulldorff, M.; Sinha, R. Fat, fiber, fruits, vegetables, and risk of colorectal adenomas. Int. J. Cancer 2004, 108, 287–292. [Google Scholar] [CrossRef] [PubMed]
- Mujtaba, S.; Bostick, R.M. Differences in risk factor-colorectal adenoma associations according to non-steroidal anti-inflammatory drug use. Eur. J. Gastroenterol. Hepatol. 2018, 30, 1318–1326. [Google Scholar] [CrossRef]
- Nimptsch, K.; Malik, V.S.; Fung, T.T.; Pischon, T.; Hu, F.B.; Willett, W.C.; Fuchs, C.S.; Ogino, S.; Chan, A.T.; Giovannucci, E.; et al. Dietary patterns during high school and risk of colorectal adenoma in a cohort of middle-aged women. Int. J. Cancer 2014, 134, 2458–2467. [Google Scholar] [CrossRef] [Green Version]
- Peters, U.; Sinha, R.; Chatterjee, N.; Subar, A.F.; Ziegler, R.G.; Kulldorff, M.; Bresalier, R.; Weissfeld, J.L.; Flood, A.; Schatzkin, A.; et al. Dietary fibre and colorectal adenoma in a colorectal cancer early detection programme. Lancet 2003, 361, 1491–1495. [Google Scholar] [CrossRef]
- Platz, E.A.; Giovannucci, E.; Rimm, E.B.; Rockett, H.R.; Stampfer, M.J.; Colditz, G.A.; Willett, W.C. Dietary fiber and distal colorectal adenoma in men. Cancer Epidemiol. Biomarkers Prev. 1997, 6, 661–670. [Google Scholar]
- Sandler, R.S.; Lyles, C.M.; Peipins, L.A.; McAuliffe, C.A.; Woosley, J.T.; Kupper, L.L. Diet and risk of colorectal adenomas: Macronutrients, cholesterol, and fiber. J. Natl. Cancer Inst. 1993, 85, 884–891. [Google Scholar] [CrossRef]
- Shaw, E.; Warkentin, M.T.; McGregor, S.E.; Town, S.; Hilsden, R.J.; Brenner, D.R. Intake of dietary fibre and lifetime non-steroidal anti-inflammatory drug (NSAID) use and the incidence of colorectal polyps in a population screened for colorectal cancer. J. Epidemiol. Community Health 2017, 71, 961–969. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tantamango, Y.M.; Knutsen, S.F.; Beeson, L.; Fraser, G.; Sabate, J. Association between dietary fiber and incident cases of colon polyps: The adventist health study. Gastrointest. Cancer Res. 2011, 4, 161–167. [Google Scholar]
- Witte, J.S.; Longnecker, M.P.; Bird, C.L.; Lee, E.R.; Frankl, H.D.; Haile, R.W. Relation of vegetable, fruit, and grain consumption to colorectal adenomatous polyps. Am. J. Epidemiol. 1996, 144, 1015–1025. [Google Scholar] [CrossRef] [Green Version]
- U.S. Department of Agriculture; U.S. Department of Health and Human Services. Dietary Guidelines for Americans, 2020–2025, 9th ed.; United States Department of Agriculture (USDA): Washington, DC, USA, 2020.
- Angelino, D.; Godos, J.; Ghelfi, F.; Tieri, M.; Titta, L.; Lafranconi, A.; Marventano, S.; Alonzo, E.; Gambera, A.; Sciacca, S.; et al. Fruit and vegetable consumption and health outcomes: An umbrella review of observational studies. Int. J. Food Sci. Nutr. 2019, 70, 652–667. [Google Scholar] [CrossRef]
- Gianfredi, V.; Vannini, S.; Moretti, M.; Villarini, M.; Bragazzi, N.L.; Izzotti, A.; Nucci, D. Sulforaphane and Epigallocatechin Gallate Restore Estrogen Receptor Expression by Modulating Epigenetic Events in the Breast Cancer Cell Line MDA-MB-231: A Systematic Review and Meta-Analysis. J. Nutr. 2017, 10, 126–135. [Google Scholar] [CrossRef]
- Gianfredi, V.; Nucci, D.; Vannini, S.; Villarini, M.; Moretti, M. In vitro Biological Effects of Sulforaphane (SFN), Epigallocatechin-3-gallate (EGCG), and Curcumin on Breast Cancer Cells: A Systematic Review of the Literature. Nutr. Cancer 2017, 69, 969–978. [Google Scholar] [CrossRef]
- EFSA Panel on Dietetic Products Nutrition and Allergies (NDA). Scientific Opinion on Dietary Reference Values for carbohydrates and dietary fibre. EFSA J. 2010, 8, 77. [Google Scholar] [CrossRef] [Green Version]
- Macfarlane, G.T.; Macfarlane, S. Bacteria, colonic fermentation, and gastrointestinal health. J. AOAC Int. 2012, 95, 50–60. [Google Scholar] [CrossRef]
- Canani, R.B.; Costanzo, M.D.; Leone, L.; Pedata, M.; Meli, R.; Calignano, A. Potential beneficial effects of butyrate in intestinal and extraintestinal diseases. World J. Gastroenterol. 2011, 17, 1519–1528. [Google Scholar] [CrossRef] [PubMed]
- Iebba, V.; Totino, V.; Gagliardi, A.; Santangelo, F.; Cacciotti, F.; Trancassini, M.; Mancini, C.; Cicerone, C.; Corazziari, E.; Pantanella, F.; et al. Eubiosis and dysbiosis: The two sides of the microbiota. New Microbiol. 2016, 39, 1–12. [Google Scholar]
- Lobionda, S.; Sittipo, P.; Kwon, H.Y.; Lee, Y.K. The Role of Gut Microbiota in Intestinal Inflammation with Respect to Diet and Extrinsic Stressors. Microorganisms 2019, 7, 271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahn, J.; Sinha, R.; Pei, Z.; Dominianni, C.; Wu, J.; Shi, J.; Goedert, J.J.; Hayes, R.B.; Yang, L. Human gut microbiome and risk for colorectal cancer. J. Natl. Cancer Inst. 2013, 105, 1907–1911. [Google Scholar] [CrossRef] [Green Version]
- FAO (Food and Agriculture Organization); WHO (World Health Organization). Carbohydrates in Human Nutrition; Report of a Joint FAO/WHO Expert Consultation (FAO Food and Nutrition Paper 66); Food and Agricolture Organization: Rome, Italy, 1998. [Google Scholar]
- Williams, B.A.; Mikkelsen, D.; Flanagan, B.M.; Gidley, M.J. “Dietary fibre”: Moving beyond the “soluble/insoluble” classification for monogastric nutrition, with an emphasis on humans and pigs. J. Anim. Sci. Biotechnol. 2019, 10, 45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Cancer Research Fund; American Institute for Cancer Research. Diet., Nutrition, Physical Activity and Cancer: A Global Perspective; Continuous Update Project Expert Report 2018; World Cancer Research Fund: London, UK, 2018. [Google Scholar]
- Bach-Faig, A.; Berry, E.M.; Lairon, D.; Reguant, J.; Trichopoulou, A.; Dernini, S.; Medina, F.X.; Battino, M.; Belahsen, R.; Miranda, G.; et al. Mediterranean diet pyramid today. Science and cultural updates. Public Health Nutr. 2011, 14, 2274–2284. [Google Scholar] [CrossRef] [Green Version]
- Fiolet, T.; Srour, B.; Sellem, L.; Kesse-Guyot, E.; Alles, B.; Mejean, C.; Deschasaux, M.; Fassier, P.; Latino-Martel, P.; Beslay, M.; et al. Consumption of ultra-processed foods and cancer risk: Results from NutriNet-Sante prospective cohort. BMJ Clin. Res. Ed. 2018, 360, k322. [Google Scholar] [CrossRef] [Green Version]
- Monteiro, C.A.; Cannon, G.; Moubarac, J.C.; Levy, R.B.; Louzada, M.L.C.; Jaime, P.C. The UN Decade of Nutrition, the NOVA food classification and the trouble with ultra-processing. Public Health Nutr. 2018, 21, 5–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agus, A.; Denizot, J.; Thevenot, J.; Martinez-Medina, M.; Massier, S.; Sauvanet, P.; Bernalier-Donadille, A.; Denis, S.; Hofman, P.; Bonnet, R.; et al. Western diet induces a shift in microbiota composition enhancing susceptibility to Adherent-Invasive E. coli infection and intestinal inflammation. Sci. Rep. 2016, 6, 19032. [Google Scholar] [CrossRef] [Green Version]
- Garcia-Montero, C.; Fraile-Martinez, O.; Gomez-Lahoz, A.M.; Pekarek, L.; Castellanos, A.J.; Noguerales-Fraguas, F.; Coca, S.; Guijarro, L.G.; Garcia-Honduvilla, N.; Asunsolo, A.; et al. Nutritional Components in Western Diet Versus Mediterranean Diet at the Gut Microbiota-Immune System Interplay. Implications for Health and Disease. Nutrients 2021, 13, 1579. [Google Scholar] [CrossRef]
- Yu, G.; Bei, J.; Zhao, J.; Li, Q.; Cheng, C. Modification of carrot (Daucus carota Linn. var. Sativa Hoffm.) pomace insoluble dietary fiber with complex enzyme method, ultrafine comminution, and high hydrostatic pressure. Food Chem. 2018, 257, 333–340. [Google Scholar] [CrossRef]
- Wang, Y.; Sun, P.; Li, H.; Adhikari, B.P.; Li, D. Rheological Behavior of Tomato Fiber Suspensions Produced by High Shear and High Pressure Homogenization and Their Application in Tomato Products. Int. J. Anal. Chem. 2018, 2018, 5081938. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Year [Ref] | Country | Study Period | Study Design | Population Characteristics | Tool | Diagnostic Assessment | Funds | Conflicts of Interest |
|---|---|---|---|---|---|---|---|---|
| Breuer-Katschinski, 2001 [29] | Germany | 2 years | Case-controls | Patients from five major hospitals in Essen; controls were selected from among hospital patients and stratified by sex | Personal interview not validated | Endoscopy and histology | yes | n.a. |
| Breuer-Katschinski, 2001 (a) [29] | Germany | 2 years | Case-controls | Patients from five major hospitals in Essen; controls were selected from among the general population and stratified by sex | Personal interview not validated | Endoscopy and histology | yes | n.a. |
| Byrd, 2020 [30] | USA | 1991–19941994–19972002 | Case-controls | MAP I and MAP Il | Validated self-administered 61-FFQs and 98-FFQ | Colonoscopy and histology | yes | yes |
| Fu, 2014 [31] | USA | 7 years | Case-controls | TCPS | Validated self-administered 108-FFQ | Colonoscopy and histology | yes | no |
| Fuchs, 1999 [32] | USA | 16 years | Cohort | Without history of cancer, IBD, or familial polyposis | Validated self-administered 136-FFQ | Medical records | n.a. | n.a. |
| Giovannucci, 1992 [33] | USA | 2 years | Cohort | HPF | Validated self-administered 131-FFQ | Endoscopy and histology | n.a. | n.a. |
| Haile, 1997 [34] | USA | 2 years | Case-controls | Screening sigmoidoscopy subjects from 2 Southern California Kaiser Permanente Medical Centers | Validated 126-item semi-quantitative FFQ | Sigmoidoscopy and histology | yes | n.a. |
| Haslam, 2017 [35] | USA | 7 years | Cohort | PLCO | Validated questionnaire 137-FFQ | Sigmoidoscopy and histology | no | yes |
| Hoff, 1986 [36] | Norway | Case-controls | Endoscopic population screening study | Food diary for 5 consecutive days | Rectosigmoidoscopy | n.a. | n.a. | |
| Kunzmann, 2015 [37] | USA | 13 years | Cohort | PLCO outcome stratified by adenoma site (incident) | Validated self-administered 137-FFQ | Sigmoidoscopy and histology | n.a. | no |
| Kunzmann, 2015 (a) [37] | USA | 13 years | Cohort | PLCO outcome stratified by adenoma site (recurrent) | Validated self-administered 137-FFQ | Sigmoidoscopy and histology | n.a. | no |
| Little, 1993 [38] | UK | 7 years | Case-controls | Subjects recruited in a colorectal cancer screening trial in Nottingham | Interview conducted at the subject’s home by specially trained interviewers | Colonoscopy and histology | yes | n.a. |
| Lubin, 1997 [39] | Israel | 3 years | Paired Case-controls | Subjects identified in the SPGD at the Tel Aviv Medical Center | 180-item questionnaire (interview) | Endoscopy and histology | n.a. | n.a. |
| Martìnez, 1996 [40] | USA | 2 years | Case-controls | Population without history of colorectal polyps and familial polyposis | 138-FFQ (interview) validation n.a. | Sigmoidoscopy or colonoscopy and histology | n.a. | n.a. |
| Mathew, 2004 [41] | USA | 2 years | Case-controls | Subjects with new or recurrent adenomas in a study conducted at the NNMC | Validated self-administered 100-item | Sigmoidoscopy or colonoscopy and histology | n.a. | n.a. |
| Mujtaba,2018 [42] | USA | 1991–19941994–19972002 | Case-controls | CPRU MAP I MAP Il | Validated self-administered 61-FFQs | Colonoscopy and histology | n.a. | no |
| Nimptsch, 2014 [43] | USA | 9 years | Cohort | NHS II | Validated self-administered 131-FFQ | Medical record | yes | n.a. |
| Peters, 2003 [44] | USA | 7 years | Case-controls | PLCO | Self-administered 137-FFQ (adaptation from previous validated FFQ) | Endoscopy and histology | n.a. | n.a. |
| Platz, 1997 [45] | USA | 8years | Cohort | HPF | Validated self-administered 131-FFQ) | Sigmoidoscopy or colonoscopy and histology | yes | n.a. |
| Sandler, 1993 [46] | USA | 2 years | Case-controls | Subjects who underwent colonoscopy at the University of North Carolina Hospitals | Validated quantitative food frequency questionnaire (interview) | Sigmoidoscopy or colonoscopy and histology | n.a. | n.a. |
| Shaw, 2017 [47] | USA | 7 years | Cross-sectional | FMCCSC | DHQ I or II | Colonoscopy and histology | yes | no |
| Tantamango, 2011 [48] | USA | 26 years | Cohort | AHS-1 and AHS-2 | Self-administered 55-FFQ validation n.a. | Self-reported | yes | no |
| Witte, 1996 [49] | USA | 2 years | Paired Case-controls | Subjects free of invasive cancer, IBD and familial polyposis | Validated self-administered 126-FFQ | Sigmoidoscopy and histology | n.a. | n.a. |
| Author, Year [Ref] (Number of Stratified Analysis) | Total Sample ^ | Sex | Age (In Years) Mean ± SD | Dietary Fibre Intake Mean ± SD | Outcome | n. Subjects at the Highest Fibre Intake | Highest Dietary Fibre Intake | Effect Size (95% CI) p | Adjustment |
|---|---|---|---|---|---|---|---|---|---|
| Breuer-Katschinski, 2001 [29] (1) | Ca: 182 Co I: 178 | Ca: M = 94 Co I: M = 88 | Ca: 63.8 ± 9.9 Co I: 63.4 ± 9.8 | Ca: 23.01 ± 7.68 g/d Co: 24.27 ± 8.09 g/d | colorectal adenoma | n.a. | n.a. | RR 0.47 (0.23–0.99) p < 0.05 | TEn, BMI, and social class |
| Breuer-Katschinski, 2001 [29] (2) | Ca: 94 Co I: 88 | Ca: M = 94 Co I: M = 88 | Ca: 63.8 ± 9.9 Co I: 63.4 ± 9.8 | n.a. | RR 0.16 (0.05–0.57) p < 0.05 | ||||
| Breuer-Katschinski, 2001 [29] (3) | Ca: 88 Co I: 90 | Ca: F = 88 Co I: F = 90 | Ca: 63.8 ± 9.9 Co I: 63.4 ± 9.8 | n.a. | RR 0.66 (0.23–1.86) p = n.s. | ||||
| Breuer-Katschinski, 2001 (a) [29] (4) | Ca: 182 Co II: 182 | Ca: M = 94 Co II: M = 92 | Ca: 63.8 ± 9.9 Co II: 64.2 ± 9.9 | Ca: 23.01 ± 7.68 g/d Co: 23.60 ± 6.75 g/d | colorectal adenoma | n.a. | n.a. | RR 0.87 (0.33–2.33) p = n.s. | TEn, BMI, and social class |
| Breuer-Katschinski, 2001 (a) [29] (5) | Ca:94 Co II: 92 | Ca: M = 94 Co II: M = 92 | Ca: 63.8 ± 9.9 Co II: 64.2 ± 9.9 | n.a. | RR 0.38 (0.14–1.05) p = n.s. | ||||
| Breuer-Katschinski, 2001 (a) [29] (6) | Ca: 88 Co II: 90 | Ca: F = 88 Co II: F = 90 | Ca: 63.8 ± 9.9 Co II: 64.2 ± 9.9 | n.a. | RR 0.86 (0.29–2.29) p = n.s. | ||||
| Byrd, 2020 [30] | Ca: 765 Co: 1986 | Ca: M = 462 Co: M = 846 | Ca: 58.2 ± 9.2 Co: 54.5 ± 10.9 | Ca: 10.9 ± 3.7 g/1000 kcal/d Co: 11.3 ± 3.9 g/1000 kcal/d | colorectal adenoma | n.a. | n.a. | OR 0.82 (0.70–0.95) p = 0.01 | none |
| Fu, 2014 [31] | Ca: 1315 Co: 3184 | Ca: M = 913 Co: M = 1732 | Ca: 59.2 Co: 57.5 | Ca: 17.0 ± 1.0 g/d Co: 17.3 ± 1.0 g/d | colorectal adenoma | Ca: 278 | 24.8 g/d | OR 0.85 (0.68–1.06) p = 0.06 | Age, sex, sites, education, smoking, PA, food supplement, dietary calcium and folate intake, and TEn |
| Fuchs, 1999 [32] | 27,530 Ca: 787 | only F | 49 | n.a. | colorectal adenoma | Ca: 212 | 24.9 ± 5.5 g/d | RR: 0.91 (0.71–1.16) p = 0.36 | Age, smoking, BMI, PA, aspirin use, family history of CRC, history of colorectal adenoma, red meat intake, alcohol, TEn, folate, methionine, calcium, vitamin D intake |
| Giovannucci, 1992 [33] | 7284 Ca: 170 | only M | 40–75 (range) | n.a. | colorectal adenoma | n.a. | ≥28.3 g/d | RR: 0.36 (0.22–0.60) p < 0.0001 | Age, TEn, and family history of CRC |
| Haile, 1997 [34] | Ca: 488 Co: 488 | Ca: M = 325 Co: M = 325 | Ca: 61.9 ± 6.7 Co: 61.8 ± 6.8 | Ca: 19.1 g/d Co: 20.1 g/d | colorectal adenoma | n.a. | 27.6 g/d | OR: 0.52 (0.33–0.80) p < 0.01 | BMI, TEn, PA, smoking and ethnicity |
| Haslam, 2017 [35] | 24,251 Ca: 4063 | Ca: M = 1418 | 55–74 (range) | n.a. | colorectal adenoma | Ca: 796 | 26.8 ± 10.8 g/d | OR 0.57 (0.52–0.63) p < 0.0001 | none |
| Hoff, 1986 [36] (1) | Ca: 23 Co: 77 | Ca: M: 16 Co: M = 40 | 50–59 (range) | Ca: 18.3 ± 1.2 M Co: 21.2 ± 0.9 M | rectal adenoma | n.a. | n.a. | OR: 0.36 (0.12–1.04) p = 0.06 | none |
| Hoff, 1986 [36] (2) | Ca: F: 7 Co: F = 37 | Ca: 18.9 ± 2.0 F Co: 21.9 ± 0.9 F | OR: 0.34 (0.08–1.51) p = 0.16 | ||||||
| Kunzmann, 2015 [37] (1) | 19,258 Ca: 1004 | Ca: M = 665 Co: M = 8,756 | Ca: 66.6 ± 5.0 Co: 66.7 ± 4.9 | Ca: 11.2 ± 3.5 g/1000 kcal Co: 12.0 ± 3.6 g/1000 kcal | colorectal adenoma | Ca: 270 | ≥12.8 g/1000 kcal | OR: 0.76 (0.63–0.91) p < 0.003 | Age, sex, study center, ethnicity, TEn, smoking status, alcohol intake, total folate intake from diet |
| Kunzmann, 2015 [37] (2) | Ca: 770 | colon adenoma | Ca: 206 | OR: 0.75 (0.61–0.92) p < 0.006 | |||||
| Kunzmann, 2015 [37] (3) | Ca: 262 | rectal adenoma | Ca: 69 | OR 0.68 (0.48–0.96) p = 0.03 | |||||
| Kunzmann, 2015 (a) [37] (4) | Ca: 738 Co: 929 | Ca: M = 535 Co: M = 570 | Ca: 66.9 ± 5.3 Co: 68.2 ± 5.4 | Ca: 11.1 ± 3.4 g/1000 kcal Co: 11.2 ± 3.5 g/1000 kcal | recurrent colorectal adenoma | Ca: 203 | ≥12.8 g/1000 kcal | OR: 1.08 (0.75–1.55) p = 0.67 | Age, sex, study center, ethnicity, TEn, smoking status, alcohol intake, total folate intake from diet |
| Kunzmann, 2015 (a) [37] (5) | Ca: 257 | recurrent colon adenoma | Ca: 70 | OR: 0.99 (0.59–1.66) p = 0.96 | |||||
| Kunzmann, 2015 (a) [37] (6) | Ca: 78 | recurrent rectal adenoma | Ca: 26 | OR: 0.88 (0.39–1.99) p = 0.86 | |||||
| Little, 1993 [38] | Ca: 147 Co: 153 | Ca: M = 65 Co: M = 65 | Ca: 66.0 ± 7.0 Co: 66.0 ± 7.0 | Ca: 25.5 g/d Co: 25 g/d | colorectal adenoma | Ca: 26 | 38 g/d | RR: 0.81 (0.37–1.78) p = n.a. | Age, sex, social class and total energy intake |
| Lubin, 1997 [39] | Ca: 196 Co: 196 | Ca: M = 111 Co: M = 111 | 21–75 (range) | n.a. | colorectal adenoma | n.a. | >34 g/d | OR 0.6 (0.3–1.2) p = 0.14 | TEn, PA, weight smoking |
| Martìnez, 1996 [40] | Ca: 157 Co: 480 | Ca: M = 98 Co: M = 229 | Ca: 57.7 Co: 54.7 | n.a. | colorectal adenoma | Ca: 29 Co: 120 | 28.0–86.8 g/d | OR 0.5 (0.3–0.9) p = 0.01 | Age, sex, race, BMI, smoking status, family history of CRC, NSAID and aspirin, calcium and fat intake |
| Mathew, 2004 [41] | Ca: 239 Co: 228 | Ca: M = Co: M = | 18–74 (range) | n.a. | colorectal adenoma | n.a. | Median (10th–90th percentiles) 6 (4, 11) of energy from various fibres | OR 0.67 (0.45–0.99) p = n.a. | Age, sex and TEn |
| Mujtaba, 2018 [42] | Ca: 789 Co: 2035 | Ca: M = 482 Co: M = 871 | Ca:58.1 ± 9.2 Co:54.5 ± 10.9 | Ca: 21.7 ± 9.4 g/d Co: 22.0 ± 10.1 g/d | colorectal adenoma | Ca: 187 | n.a. | OR 1.25 (0.89–1.75) p = 0.28 | Age, sex, family history of CRC, smoking, alcohol, BMI, height, PA, hormone therapy, aspirin use, NSAID calcium, folate, TEn, total fat, SFA, red and processed meat intake |
| Nimptsch, 2014 [43] | 17,221 Ca: 1299 | only F | 34–51 (range) | E: 22.0 ± 5.5 g/d nE: 16.7 ± 4.8 g/d | colorectal adenoma | Ca E: 231 Ca nE: 293 | n.a. | OR 0.77 (0.65–0.92) p = n.a. | TEn |
| Peters, 2003 [44] (1) | Ca: 3591 Co: 33,971 | Ca: M = n.a. Co: M = 17,435 | 55–74 (range) | 21.9 g/d | colorectal adenoma | Ca: 637 | 30.6 g/d | OR 0.73 (0.62–0.86) p < 0.002 | Age, sex, study center, TEn |
| Peters, 2003 [44] (2) | Ca: 2378 Co: 33,971 | colon adenoma | Ca: 412 | OR 0.70 (0.58–0.85) p < 0.0006 | |||||
| Peters, 2003 [44] (3) | Ca: 659 Co: 33,971 | rectal adenoma | Ca: 123 | OR 0.93 (0.65–1.33) p = 0.97 | |||||
| Platz, 1997 [45] (1) | 16,448 Ca: 690 | only M | 59.5 ± 9.4 | n.a. | colorectal adenoma | Ca: 120 Co: 3171 | 32.3 g/d | RR = 0.88 (0.72–1.08) p = 0.218 | Age, endoscopy prior 1986, family history of CRC, BMI, smoking, multivitamin use, PA, aspirin use, alcohol, red meat, folate and methionine |
| Platz, 1997 [45] (2) | Ca: 531 | colon adenoma | Ca: 91 | RR: 0.88 (0.59–1.31) p = 0.10 | |||||
| Platz, 1997 [45] (3) | Ca: 159 | rectal adenoma | Ca: 29 | RR: 1.12 (0.54–2.35) p = 0.78 | |||||
| Sandler, 1993 [46] (1) | Ca: 105 Co: 165 | only M | Ca:63.5 ± 12.2 Co:58.7 ± 12.1 | n.a. | colorectal adenoma | Ca: n.a. | ≥18.6 g/d | OR 0.74 (0.32–1.74) p = 0.873 | Age, alcohol intake, BMI, and TEn |
| Sandler, 1993 [46] (2) | Ca: 131 Co: 244 | only F | Ca:62.2 ± 11.6 Co:58.7 ± 12.5 | Ca: n.a. | ≥15.6 g/d | OR 0.71 (0.35–1.43) p = 0.120 | |||
| Shaw, 2017 [47] | Ca: 1098 no Ca: 1450 | Ca: M = 710 no Ca: 675 | 50–75 (range) | Ca: 10.5–33.59 g/d no Ca: 11.01–33.88 g/d | colorectal adenoma | Ca:205 no Ca: 347 | >25.52 g/d | OR 0.77 (0.56–1.07) p = 0.14 | Age, sex, BMI, smoking, reason for colonoscopy, family history of polyps, TEn |
| Tantamango, 2011 [48] | 2818 Ca: 441 | Ca: M = 211 Ca: M = 922 | Ca: 73.4 ± 9.2 Co: 71.2 ± 9.7 | Ca: 11.2 ± 4.3 g/d Co: 11.7 ± 4.8 g/d | colon adenoma | Ca: 93 | 16.9 g/d | OR 0.71 (0.51–0.99) p = 0.04 | Age, sex, BMI, education, PA, alcohol and meat intake |
| Witte, 1996 [49] | Ca: 488 Co: 488 | Ca: M = 334 Co: M = 334 | Ca: 61.9 ± 6.7 Co: 61.8 ± 6.8 | Ca: 18.9 ± 9.6 g/d Co: 20.0 ± 9.7 g/d | colorectal adenoma | n.a. | n.a. | OR 0.82 (0.65–1.03) p = 0.09 | None |
| Analysis | Model | n. Studies Included | ES | 95% CI | p | Sample Size | I2 | p | Intercept | Tau (t) | p |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Trim and Fill colorectal | Fixed * | 24 | 0.71 | 0.68–0.75 | 0.000 | 157,725 | 62.71 | 0.000 | 0.12 | 0.21 | 0.838 |
| Random ^ | 0.74 | 0.67–0.82 | 0.000 | ||||||||
| Excluding potential overlapping cohort | Fixed | 19 | 0.79 | 0.74–0.85 | 0.000 | 87,629 | 13.00 | 0.295 | −0.89 | −1.93 | 0.070 |
| Random | 0.79 | 0.73–0.86 | 0.000 | ||||||||
| Excluding studies with estimated OR | Fixed | 18 | 0.76 | 0.71–0.82 | 0.000 | 115,311 | 39.33 | 0.045 | −0.84 | −1.41 | 0.179 |
| Random | 0.74 | 0.67–0.83 | 0.000 | ||||||||
| 9y FU | Fixed | 4 | 0.79 | 0.71–0.88 | 0.000 | 56,453 | 0.00 | 0.595 | 0.15 | 0.07 | 0.950 |
| Random | 0.79 | 0.71–0.88 | 0.000 | ||||||||
| Validated FFQ | Fixed | 15 | 0.71 | 0.68–0.75 | 0.000 | 115,192 | 74.88 | 0.000 | 1.16 | 1.14 | 0.276 |
| Random | 0.75 | 0.66–0.86 | 0.000 | ||||||||
| Diagnosis | Fixed | 21 | 0.70 | 0.66–0.73 | 0.000 | 120,530 | 64.52 | 0.000 | 0.09 | 0.14 | 0.891 |
| Random | 0.71 | 0.63–0.80 | 0.000 | ||||||||
| Quality score ≥ 7 | Fixed | 20 | 0.78 | 0.73–0.83 | 0.000 | 125,561 | 38.10 | 0.044 | −0.99 | −1.96 | 0.065 |
| Random | 0.77 | 0.70–0.84 | 0.000 | ||||||||
| Colon adenoma | Fixed | 4 | 0.73 | 0.65–0.83 | 0.000 | 74,714 | 0.00 | 0.774 | 1.20 | 1.20 | 0.352 |
| Random | 0.73 | 0.65–0.83 | 0.000 | ||||||||
| Rectal adenoma | Fixed | 5 | 0.77 | 0.62–0.96 | 0.019 | 69,905 | 30.54 | 0.218 | −0.98 | −0.86 | 0.455 |
| Random | 0.76 | 0.56–1.03 | 0.074 | ||||||||
| Cohort studies (incidence) | Fixed | 10 | 0.67 | 0.63–0.71 | 0.000 | 135,506 | 75.38 | 0.000 | 1.32 | 1.12 | 0.297 |
| Random | 0.72 | 0.61–0.84 | 0.000 | ||||||||
| Case-Control/Cross-sectional (prevalence) | Fixed | 17 | 0.78 | 0.72–0.84 | 0.000 | 55,401 | 25.13 | 0.165 | −0.86 | −189 | 0.079 |
| Random | 0.76 | 0.69–0.85 | 0.000 | ||||||||
| Women | Fixed | 6 | 0.81 | 0.70–0.92 | 0.002 | 35,152 | 0.00 | 0.745 | −0.50 | −1.06 | 0.349 |
| Random | 0.81 | 0.70–0.92 | 0.002 | ||||||||
| Men | Fixed | 6 | 0.69 | 0.58–0.82 | 0.000 | 24,426 | 72.73 | 0.003 | −2.24 | −2.72 | 0.053 |
| Random | 0.46 | 0.27–0.78 | 0.004 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nucci, D.; Fatigoni, C.; Salvatori, T.; Nardi, M.; Realdon, S.; Gianfredi, V. Association between Dietary Fibre Intake and Colorectal Adenoma: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 4168. https://doi.org/10.3390/ijerph18084168
Nucci D, Fatigoni C, Salvatori T, Nardi M, Realdon S, Gianfredi V. Association between Dietary Fibre Intake and Colorectal Adenoma: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2021; 18(8):4168. https://doi.org/10.3390/ijerph18084168
Chicago/Turabian StyleNucci, Daniele, Cristina Fatigoni, Tania Salvatori, Mariateresa Nardi, Stefano Realdon, and Vincenza Gianfredi. 2021. "Association between Dietary Fibre Intake and Colorectal Adenoma: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 18, no. 8: 4168. https://doi.org/10.3390/ijerph18084168
APA StyleNucci, D., Fatigoni, C., Salvatori, T., Nardi, M., Realdon, S., & Gianfredi, V. (2021). Association between Dietary Fibre Intake and Colorectal Adenoma: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health, 18(8), 4168. https://doi.org/10.3390/ijerph18084168