
Can Motivational Interviewing Make a Difference in Supporting Employees to Deal with Elevated Blood Pressure? A Feasibility Study at the Workplace


{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
- How many employees with so far unidentified or uncontrolled hypertension who have not yet started medical treatment can be identified in the occupational health service of a large manufacturing company as a database for further interventions?
- How many of the identified employees can be motivated to undergo validation after positive screening for elevated blood pressure? How many of them will perform further self-assessments to validate their initially elevated blood pressure value? What are promoting and hindering factors?
- How many employees with validated elevated blood pressure can be motivated to undergo hypertension prevention counseling in the occupational health service? How many are willing to be randomized? How many are willing to be subsequently supported by the health coach, and at least how many complete the intervention?
- Which factors inhibit or support the implementation of motivational interviewing in the occupational health setting?
- Are the evaluation instruments feasible? How many participants complete all questionnaires up to the end of the study?
- How do German occupational health physicians and study participants assess the motivational interviewing approach? When we designed the study in 2010, to our knowledge, motivational interviewing had not been used regularly in the occupational health sector to affect employees’ behavior in Germany, with the exception of an alcohol use intervention program.
2. Materials and Methods
2.1. Study Part A (Methods of Screening and Validating Hypertension)
2.2. Study Part B (Intervention Methods)
2.3. Evaluation Methods and Instruments
2.4. Statistical Analysis
3. Results
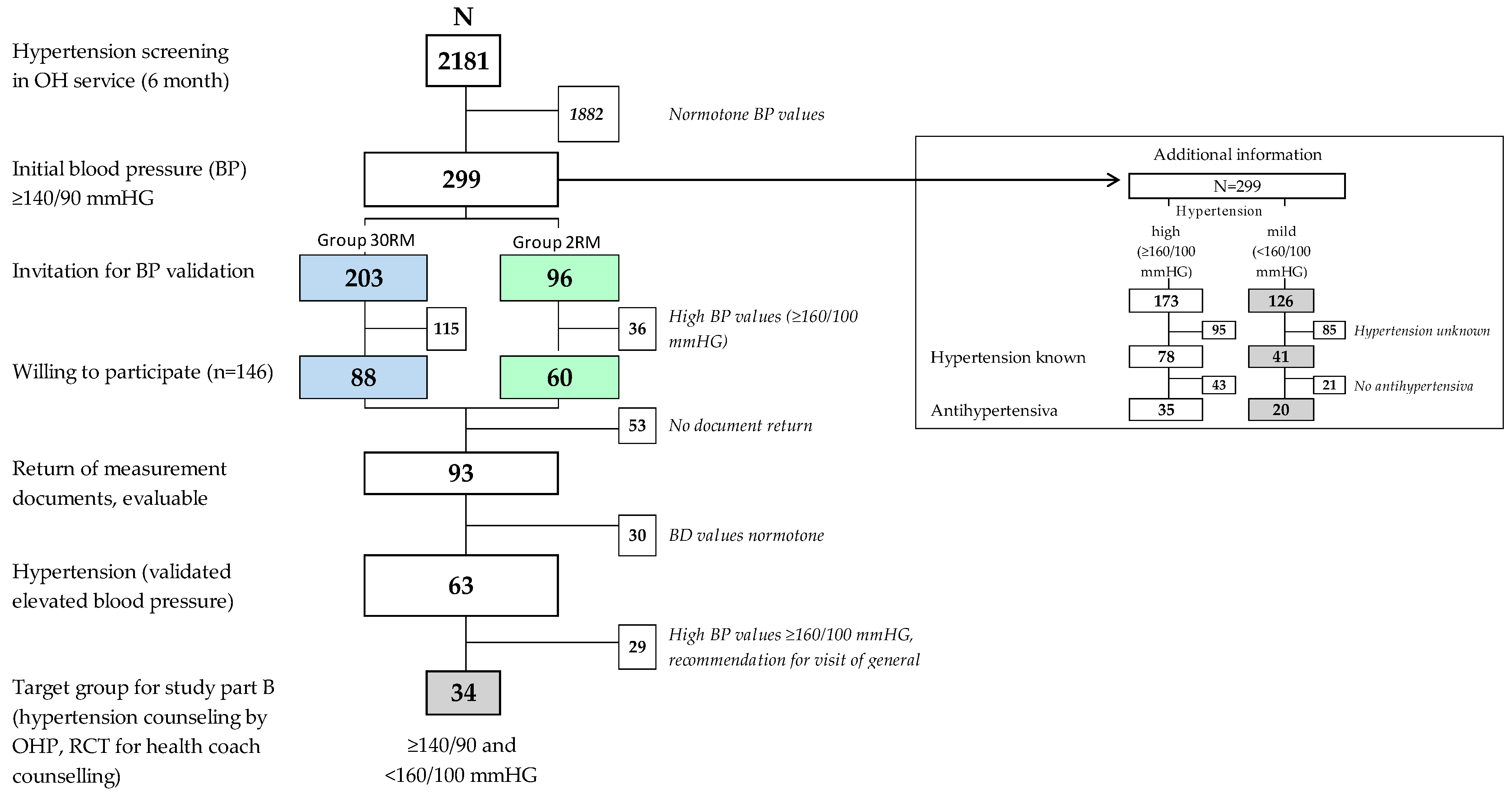
3.1. Study Part A (Screening and Validation of Hypertension)
3.1.1. Results of Outcome Evaluation: Number of Individuals with Mild Hypertension
3.1.2. Results of Process Evaluation: Feasibility of Screening with Focus on Employees
3.1.3. Results of Process Evaluation: Feasibility of Screening with Focus on OH Service
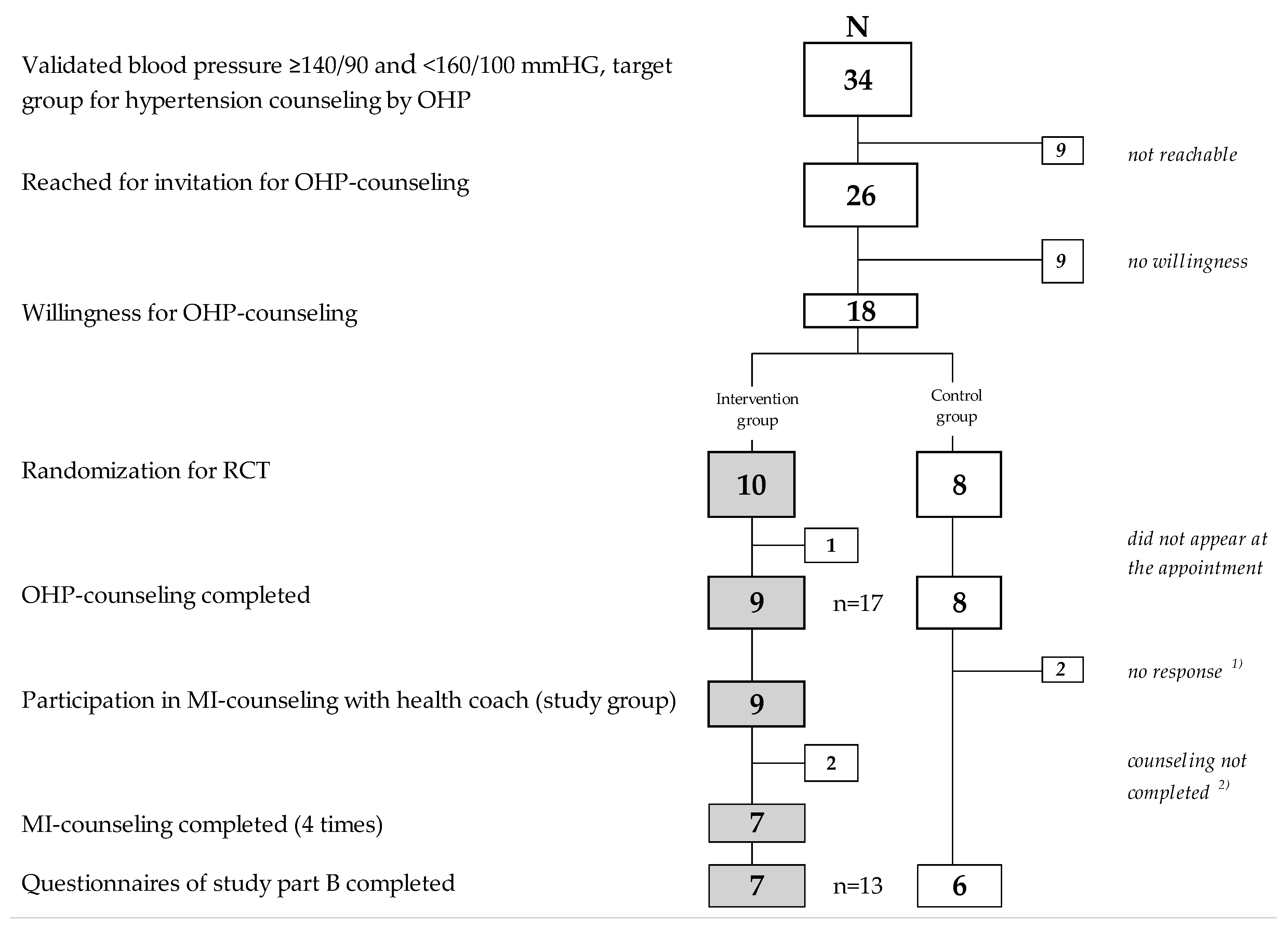
3.2. Study Part B (Intervention)
3.2.1. Feasibility of RCT Design and of Hypertension Counseling by OH Physicians (Focus on Participants)
3.2.2. Feasibility of Study Processes and OHP Counseling–Assessment of OH Physicians (Focus on Own Work)
3.2.3. Feasibility of Repeated MI-Counseling by the Health Coach (Focus on Participants; IG Only)
- In the 12-item sum score concerning assessment of and satisfaction with the concept (median 3.7, ranging from, 1 ‘fully applies to 5 ‘not applies at all’ (see Online Supplementary Table S9);
- In the oral feedback during the four health coach MI-counseling sessions. The self-assessment of importance of own goals (median 7.3–10.0 from T1 to T4 with a possible range from 1 ‘not at all’ to 10 ‘very much’), self-confidence (median 4.0–8.8), and readiness to work for these goals (median 8.0–10.0).
3.2.4. Intervention Effect on Primary Outcome ‘Lifestyle Changes’
3.2.5. Intervention Effect on Secondary Outcomes at T5
4. Discussion
Strengths and Limitations of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Diederichs, C.; Neuhauser, H. Regional variations in hypertension prevalence and management in Germany: Results from the German Health Interview and Examination Survey (DEGS1). J. Hypertens. 2014, 32, 1405–1413. [Google Scholar] [CrossRef] [PubMed]
- Grobe, T.G.; Steinmann, S.; Szecsenyi, J. Physicians’ Report 2019 (In German: Arztreport 2019); Series of Publications on Health Analysis; Barmer Health Insurance: Berlin, Germany, 2019; Volume 14, ISBN 978-3-946199-20-5. [Google Scholar]
- Schneider, M.; Scholl, J. Analysis of the current health status of middle-aged persons. Preliminary results of a cross-sectional survey of employees aged 40 to 65 years in a pharmaceutical company (In German: Analyse des Aktuellen Gesundheitsstatus bei Personen im Mittleren Lebensalter: Erste Ergebnisse einer Querschnitterhebung bei Mitarbeitern zwischen 40 und 65 Jahren in einem pharmazeutischen Unternehmen). Arbeitsmed. Sozialmed. Umweltmed. 2007, 42, 596–604. [Google Scholar]
- Löwel, H.; Meisinger, C.; Heier, M.; Hymer, H.; Alte, D.; Völzke, H. Epidemiology of hypertension. Selective results of population-representative studies in Southern and Northern Germany (In German: Epidemiologie der arteriellen Hypertonie in Deutschland). Dtsch. Med. Wochenschr. 2006, 131, 2586–2591. [Google Scholar] [CrossRef] [PubMed]
- Lacruz, M.E.; Kluttig, A.; Hartwig, S.; Löer, M.; Tiller, D.; Greiser, K.H.; Werdan, K.; Haerting, J. Prevalence and Incidence of Hypertension in the General Adult Population. Results of the CARLA-Cohort Study. Medicine 2015, 94, e952. [Google Scholar] [CrossRef]
- Chen, R.; Tunstall-Pedoe, H.; Morrison, C.; Connaghan, J.; A’Brook, R. Trends and social factors in blood pressure control in Scottish MONICA surveys 1986–1995: The rule of halves revisited. J. Hum. Hypertens. 2003, 17, 751–759. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Powietzka, J.; March, S.; Stallmann, C.; Swart, E.; Ladebeck, N. Selected diseases of older employed persons (In German: Ausgewählte Erkrankungen älterer Erwerbstätiger). Zbl. Arbeitsmed. 2016, 66, 331–336. [Google Scholar] [CrossRef]
- Van der Niepen, P.; Van De Borne, P.; Persu, A.; Andries, A.; Committee, B.H. Prevalence of hypertension and cardiovascular risk factors in Belgian civil employees: Results of the screening during World Hypertension Day 2007. J. Hypertens. 2008, 26, 1045–1046. [Google Scholar] [CrossRef]
- Steiner, S.; Helis, E.; Chen, L.; Turton, P.; Leenen, F.H.; Sonkodi, S.; Sonkodi, B.; D’Angelo, M.S.; Fodor, J.G. A cross-national comparative study of blood pressure levels and hypertension prevalence in Canada and Hungary. J. Hypertens. 2012, 30, 2105–2111. [Google Scholar] [CrossRef] [PubMed]
- Lang, T.; de Gaudemaris, R.; Chatellier, G.; Hamici, L.; Diène, E. Prevalence and therapeutic control of hypertension in 30,000 subjects in the workplace. Hypertension 2001, 38, 449–454. [Google Scholar] [CrossRef] [Green Version]
- Randerath, O.; Noetel, A.; Möckel, L.; Klinge, M.; Hohlfeld, A.; Eich, S.; Wagner, C.; Kim, J.; Morak, R.; Pychny, J.; et al. In-company blood pressure measurement—A useful preventive measure? Results of a blood pressure measurement campaign in an SME (In German: Innerbetriebliche Blutdruckmessung—eine sinnvolle präventive Maßnahme?). Arbeitsmed. Sozialmed. Umweltmed. 2019, 54, 600–603. Available online: https://www.asu-arbeitsmedizin.com/wissenschaft/ergebnisse-einer-blutdruckmessaktion-einem-mittelstaendischen-unternehmen (accessed on 16 November 2020).
- Schaller, N.; Blume, K.; Hanssen, H.; Schuster, T.; Schmidt-Trucksäss, A.; Bischof, J.; Halle, M. Prevalence of the metabolic syndrome and its risk factors. Results of a large work-site health assessment. Dtsch. Med. Wochenschr. 2014, 139, 2279–2284. [Google Scholar] [CrossRef]
- Kempf, K.; Martin, S.; Döhring, C.; Dugi, K.; Wolfram von Wolmar, C.; Haastert, B.; Schneider, M. The epidemiological Boehringer Ingelheim Employee study—part I: Impact of overweight and obesity on cardiometabolic risk. J. Obes. 2013, 2013, 159123. [Google Scholar] [CrossRef]
- European Communities. Facing the challenge. The Lisbon Strategy for Growth and Employment: Report from the High Level Group Chaired by Wim Kok; Publications of the European Communities: Luxembourg, 2004; ISBN 92-894-7054-2. [Google Scholar]
- Robroek, S.J.; van de Vathorst, S.; Hilhorst, M.T.; Burdorf, A. Moral issues in workplace health promotion. Int. Arch. Occup. Environ. Health 2012, 85, 327–331. [Google Scholar] [CrossRef] [Green Version]
- Burton, J. WHO Healthy Workplace Framework and Model: Background and Supporting Literature and Practices. 2010. Available online: https://www.who.int/occupational_health/HealthyWorkplaces_Backgrounddoc.pdf (accessed on 16 November 2020).
- Tautz, A. Company health management (In German: Betriebliches Gesundheitsmanagement). In Prevention and Health Promotion at the Interface between Curative Medicine and Occupational Medicine; Rieger, M.A., Hildebrand, S., Nesseler, T., Letzel, S., Nowak, D., Eds.; A Compendium for Corporate Health Management; Ecomed: Landsberg, Germany, 2016; pp. 23–34. ISBN 978-3-609-10560-4. [Google Scholar]
- Drexler, H.; Letzel, S.; Nesseler, T.; Stork, J.; Tautz, A. Occupational medicine 4.0: Theses of the occupational medicine to the conditions and the development need of the workplace health prevention and health promotion in Germany (In German: Arbeitsmedizin 4.0: Thesen der Arbeitsmedizin zum Stand und zum Entwicklungsbedarf der betrieblichen Prävention und Gesundheitsförderung in Deutschland). In (Hrsg.): Prevention and Health Promotion at the Interface between Curative Medicine and Occupational Medicine; Rieger, M.A., Hildebrand, S., Nesseler, T., Letzel, S., Nowak, D., Eds.; A Compendium for Corporate Health Management; Ecomed: Landsberg, Germany, 2016; pp. 333–343. ISBN 978-3-609-10560-4. [Google Scholar]
- Petersen, J. Screening examinations in the enterprise (In German: Screeninguntersuchungen im Unternehmen). Arbeitsmed. Sozialmed. Umweltmed. 2010, 45, 22–24. Available online: https://www.asu-arbeitsmedizin.com/sites/default/files/ulmer/de-asu/document/file_270849.pdf (accessed on 16 November 2020).
- Hartmann, B.; Seidel, D.; Hahn, T.; Bräuer, T.; Pieth, J. Results of occupational health service advice on occupational health prevention (In German: Ergebnisse betriebsärztlicher Beratung bei der arbeitsmedizinischen Vorsorge). Arbeitsmed. Sozialmed. Umweltmed. 2007, 42, 236–242. [Google Scholar]
- Busch, M. Health behaviour and results of medical examinations of trainee applicants and trainees in a major automotive company (In German: Gesundheitsverhalten und Untersuchungsbefunde von Ausbildungsplatzbewerbern und Auszubildenden in einem Großunternehmen der Automobilindustrie). Arbeitsmed. Sozialmed. Umweltmed. 2007, 42, 606–609. [Google Scholar]
- Schneider, M.; Ernsting, A.; Antoni, C.H. Program FIT FOR LIFE—FIT FOR WORK: An effective preventive intervention program for developing a health-promoting lifestyle (In German: FIT IM LEBEN—FIT IM JOB. Eine effektive Maßnahme zum Aufbau eines gesundheitsförderlichen Verhaltensstils). Arbeitsmed. Sozialmed. Umweltmed. 2009, 10, 540–547. [Google Scholar]
- Bünger, J.; Lanzerath, I.; Ruhnau, P.; Görlitz, A.; Fischer, C.; Kott, J.; Ellrott, T.; Fiege, A.; Tschentscher, H.; Reutemann, S.-K.; et al. Workplace health promotion: Evaluation of interventions to reduce cardiovascular risks (In German: Betriebliche Gesundheitsförderung: Evaluation von Interventionen zur Senkung kardiovaskulärer Risiken). Arbeitsmed. Sozialmed. Umweltmed. 2003, 38, 421–425. [Google Scholar]
- Finell, M.; Weiler, D.; Keskin, M.-C.; Stork, J. General secondary prevention in the operational setting: Example check-up at AUDI. In (Hrsg.): Prevention and Health Promotion at the Interface between Curative Medicine and Occupational Medicine; Rieger, M.A., Hildebrand, S., Nesseler, T., Letzel, S., Nowak, D., Eds.; A Compendium for Corporate Health Management; Ecomed: Landsberg, Germany, 2016; pp. 207–209. ISBN 978-3-609-10560-4. [Google Scholar]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; De Simone, G.; Dominiczak, A.; et al. ESC/ESH Guidelines for the management of arterial hypertension. The Task Force for the management of arterial hypertension of the European Society of Cardiology (ESC) and the European Society of Hypertension (ESH). EHJ 2018, 39, 3021–3104. [Google Scholar] [CrossRef]
- Glynn, L.G.; Murphy, A.W.; Smith, S.M.; Schroeder, K.; Fahey, T. Interventions used to improve control of blood pressure in patients with hypertension. Cochrane Database Syst. Rev. 2010, CD005182. [Google Scholar] [CrossRef]
- Visram, S.; Clarke, C.; White, M. Making and maintaining lifestyle changes with the support of a lay health advisor: Longitudinal qualitative study of health trainer services in northern England. PLoS ONE 2014, 9, e94749. [Google Scholar] [CrossRef] [Green Version]
- Artinian, N.T.; Fletcher, G.F.; Mozaffarian, D.; Kris-Etherton, P.; Van Horn, L.; Lichtenstein, A.H.; Kumanyika, S.; Kraus, W.E.; Fleg, J.L.; Redeker, N.S.; et al. Interventions to promote physical activity and dietary lifestyle changes for cardiovascular risk factor reduction in adults. A scientific statement from the American Heart Association. Circulation 2010, 122, 406–441. [Google Scholar] [CrossRef] [PubMed]
- Miller, W.R.; Rollnick, S. Motivational Interviewing. In Helping People Change (Applications of Motivational Interviewing), 1st ed.; The Gilford Press: New York, NY, USA, 1991. [Google Scholar]
- Miller, W.R.; Rollnick, S. Motivational Interwiewing (In German: Motivierende Gesprächsführung): 3rd Edition of the Standard Work in German; Lambertus: Freiburg, Germany, 2015; ISBN 978-3-7841-2545-9. [Google Scholar]
- Miller, W.R. Motivational interviewing with problem drinkers. Behav. Psychother. 1983, 11, 147–172. [Google Scholar] [CrossRef] [Green Version]
- Lundahl, B.; Moleni, T.; Burke, B.L.; Butters, R.; Tollefson, D.; Butler, C.; Rollnick, S. Motivational interviewing in medical care settings: A systematic review and meta-analysis of randomized controlled trials. Patient Educ. Couns. 2013, 93, 157–168. [Google Scholar] [CrossRef] [PubMed]
- Miller, W.R.; Rose, G.S. Toward a theory of motivational interviewing. Am. Psychol. 2009, 64, 527–537. [Google Scholar] [CrossRef] [PubMed]
- Miller, W.R. Motivational interviewing: Research, practice, and puzzles. Addic. Behav. 1996, 21, 835–842. [Google Scholar] [CrossRef]
- Magill, M.; Gaume, J.; Apodaca, T.R.; Walthers, J.; Mastroleo, N.R.; Borsari, B.; Longabaugh, R. The technical hypothesis of motivational interviewing: A meta-analysis of MI’s key causal model. J. Consult. Clin. Psychol. 2014, 82, 973–983. [Google Scholar] [CrossRef] [PubMed]
- Eyler, R.; Shvets, K.; Blakely, M.L. Motivational Interviewing to increase postdischarge antibiotic adherence in older adults with pneumonia. Consult. Pharm. 2016, 31, 38–43. [Google Scholar] [CrossRef]
- O’Brien, F.; McKee, G.; Mooney, M.; O’Donnell, S.; Moser, D. Improving knowledge, attitudes and beliefs about acute coronary syndrome through an individualized educational intervention: A randomized controlled trial. Patient Educ. Couns. 2014, 96, 179–187. [Google Scholar] [CrossRef] [Green Version]
- Tuccero, D.; Railey, K.; Briggs, M.; Hull, S.K. Behavioral health in prevention and chronic illness management: Motivational interviewing. Prim. Car. 2016, 43, 191–202. [Google Scholar] [CrossRef]
- Elliot, D.L.; Goldberg, L.; Kuehl, K.S.; Moe, E.L.; Breger, R.K.; Pickering, M.A. The PHLAME (Promoting Healthy Lifestyles: Alternative Models’ Effects) firefighter study: Outcomes of two models of behavior change. J. Occup. Environ. Med. 2007, 49, 204–213. [Google Scholar] [CrossRef] [PubMed]
- Butterworth, S.; Linden, A.; McClay, W.; Leo, M.C. Effect of motivational interviewing-based health coaching on employees’ physical and mental health status. J. Occup. Health Psychol. 2006, 11, 358–365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Croissant, B.; Hupfer, K.; Löber, S.; Mann, K.; Zober, A. Long-term follow-up on alcohol use in a big company after brief intervention by a company physician (In German: Längsschnittuntersuchung alkoholauffälliger Mitarbeiter in einem Großbetrieb nach werksärztlicher Kurzintervention). Nervenarzt 2008, 79, 80–85. [Google Scholar] [CrossRef] [PubMed]
- McPherson, T.L.; Goplerud, E.; Derr, D.; Mickenberg, J.; Courtemanche, S. Telephonic screening and brief intervention for alcohol misuse among workers contacting the employee assistance program: A feasibility study. Drug Alcohol Rev. 2010, 29, 641–646. [Google Scholar] [CrossRef]
- Prochaska, J.O.; Butterworth, S.; Redding, C.A.; Burden, V.; Perrin, N.; Leo, M.; Flaherty-Robb, M.; Prochaska, J.M. Initial efficacy of MI, TTM tailoring and HRI’s with multiple behaviors for employee health promotion. Prev. Med. 2008, 46, 226–231. [Google Scholar] [CrossRef] [Green Version]
- Schneider, R.J.; Casey, J.; Kohn, R. Motivational versus confrontational interviewing: A comparison of substance abuse assessment practices at employee assistance programs. J. Behav. Health Serv. Res. 2000, 27, 60–74. [Google Scholar] [CrossRef]
- Adams, A. Prevention of cardio-vascular diseases and diabetes mellitus (In German: Prävention von Herz-Kreislauf-Erkrankungen und Diabetes mellitus). Arbeitsmed. Sozialmed. Umweltmed. 2011, 46, 7–13. [Google Scholar]
- Groeneveld, I.F.; Proper, K.I.; van der Beek, A.J.; Hildebrandt, V.H.; van Mechelen, W. Short and long term effects of a lifestyle intervention for construction workers at risk for cardiovascular disease: A randomized controlled trial. BMC Public Health 2011, 31, 836. [Google Scholar] [CrossRef] [Green Version]
- Kouwenhoven-Pasmooij, T.A.; Robroek, S.J.W.; Kraaijenhagen, R.A.; Helmhout, P.H.; Nieboer, D.; Burdorf, A.; Hunink, M.G.M. Effectiveness of the blended-care lifestyle intervention ‘PerfectFit’: A cluster randomised trial in employees at risk for cardiovascular diseases. BMC Public Health 2018, 18, 766. [Google Scholar] [CrossRef]
- Formanoy, M.A.; Dusseldorp, E.; Coffeng, J.K.; Van Mechelen, I.; Boot, C.R.; Hendriksen, I.J.; Tak, E.C. Physical activity and relaxation in the work setting to reduce the need for recovery: What works for whom? BMC Public Health 2016, 16, 866. [Google Scholar] [CrossRef] [Green Version]
- Park, J.; Esmail, S.; Rayani, F.; Norris, C.M.; Gross, D.P. Motivational interviewing for workers with disabling musculoskeletal disorders: Results of a cluster randomized control trial. J. Occup. Rehabil. 2018, 28, 252–264. [Google Scholar] [CrossRef] [Green Version]
- Boerger, N.L.; Barleen, N.A.; Marzec, M.L.; Moloney, D.P.; Dobro, J. The impact of specialized telephonic guides on employee engagement in corporate well-being programs. Popul. Health Manag. 2018, 21, 32–39. [Google Scholar] [CrossRef] [Green Version]
- Verweij, L.M.; Proper, K.I.; Weel, A.N.; Hulshof, C.T.; van Mechelen, W. The application of an occupational health guideline reduces sedentary behaviour and increases fruit intake at work: Results from an RCT. Occup. Environ. Med. 2012, 69, 500–507. [Google Scholar] [CrossRef]
- Auer, R.; Gencer, B.; Tango, R.; Nanchen, D.; Matter, C.M.; Lüscher, T.F.; Windecker, S.; Mach, F.; Cornuz, J.; Humair, J.-P.; et al. Uptake and efficacy of a systematic intensive smoking cessation intervention using motivational interviewing for smokers hospitalised for an acute coronary syndrome: A multicentre before-after study with parallel group comparisons. BMJ Open. 2016, 6, e011520. [Google Scholar] [CrossRef] [Green Version]
- Härter, M.; Dirmaier, J.; Dwinger, S.; Kriston, L.; Herbarth, L.; Siegmund-Schultze, E.; Bermejo, I.; Matschinger, H.; Heider, D.; König, H.-H. Effectiveness of telephone-based health coaching for patients with chronic conditions: A randomised controlled trial. PLoS ONE 2016, 11, e0161269. [Google Scholar] [CrossRef] [Green Version]
- Lin, C.-H.; Chiang, S.-L.; Heitkemper, M.M.; Hung, Y.-J.; Lee, M.-S.; Tzeng, W.-C.; Chiang, L.-C. Effects of telephone-based motivational interviewing in lifestyle modification program on reducing metabolic risks in middle-aged and older women with metabolic syndrome: A randomized controlled trial. Int. J. Nur. Stud. 2016, 60, 12–23. [Google Scholar] [CrossRef]
- Steptoe, A.; Kerry, S.; Rink, E.; Hilton, S. The impact of behavioral counseling on stage of change in fat intake, physical activity, and cigarette smoking in adults at increased risk of coronary heart disease. Am. J. Public Health 2001, 91, 265–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Nes, M.; Sawatzky, J.A. Improving cardiovascular health with motivational interviewing: A nurse practitioner perspective. J. Am. Acad. Nurse Pract. 2010, 22, 654–660. [Google Scholar] [CrossRef] [PubMed]
- Woollard, J.; Beilin, L.; Lord, T.; Puddey, I.; MacAdam, D.; Rouse, I. A controlled trial of nurse counseling on lifestyle change for hypertensives created in general practice: Preliminary results. Clin. Exp. Pharmacol. Physiol. 1995, 22, 466–468. [Google Scholar] [CrossRef] [PubMed]
- Asayama, K.; Thijs, L.; Li, Y.; Gu, Y.-M.; Hara, A.; Liu, Y.-P.; Zhang, Z.; Wie, F.-F.; Lujambio, I.; Mena, L.J. Setting thresholds to varying blood pressure monitoring intervals differentially affects risk estimates associated with white-coat and masked hypertension in the population. Hypertension 2014, 64, 935–942. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Middeke, M. Hypertension: The Crux of the RR Variability (In German: Hypertonie: Die Krux der RR-Variabilität). Dtsch. Arztebl. 2014, 111, 4. Available online: https://www.aerzteblatt.de/archiv/162154/Hypertonie-Die-Krux-der-RR-Variabilitaet (accessed on 16 November 2020).
- Slany, K.; Hitzenberger, G.; Zweiker, R.; Mayer, G.; Rosenkranz, A.R.; Watschinger, B.; Wenzel, R. Practical recommendations of the Austrian Society for Hypertensiology (ÖGH) for physician, self and ambulant 24-hour blood pressure measurement (In German: Empfehlungen der österreichischen Gesellschaft für Hypertensiologie (GH) zur Arzt-, Selbst- und ambulanten 24-Stunden- Blutdruckmessung). J. Hyperton. 2008, 12, 13–19. [Google Scholar]
- Siu, A.L. Screening for high blood pressure in adults: U.S. Preventive Services Task Force recommendation statement. Ann. Int. Med. 2015, 163, 778–786. [Google Scholar] [CrossRef] [Green Version]
- Arain, M.; Campbell, M.J.; Cooper, C.L.; Lancaster, G.A. What is a pilot or feasibility study? A review of current practice and editorial policy. BMC Med. Res. Meth. 2010, 10, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Craig, P.; Dieppe, P.; Macintyre, S.; Nazareth, I.; Petticrew, M. Developing and Evaluating Complex Interventions. Medical Research Council. 2019. Available online: https://mrc.ukri.org/documents/pdf/complex-interventions-guidance/ (accessed on 16 November 2020).
- Eldridge, S.M.; Lancaster, G.A.; Campbell, M.J.; Thabane, L.; Hopewell, S.; Coleman, C.L.; Bond, C.M. Defining Feasibility and pilot studies in preparation for randomized controlled trials: Development of a conceptual framework. PLoS ONE 2016, 11, e0150205. [Google Scholar] [CrossRef] [Green Version]
- CONSORT. Extension for Randomized Pilot and Feasibility Trials. Available online: http://www.consort-statement.org/extensions/overview/pilotandfeasibility (accessed on 16 November 2020).
- German Hypertension League—German Hypertension Society (Deutsche Hochdruckliga—Deutsche Hypertonie Gesellschaft). Leitlinien zur Behandlung der Arteriellen Hypertonie; AWMF register no. 046/001; German Hypertension League—German Hypertension Society: Heidelberg, Germany, 2008; Available online: http://www.zgk.ch/files/download/206 (accessed on 16 November 2020).
- Hudak, S. Can Employees with Arterial Hypertension be Motivated to Visit Their Family Doctor by a Motivating Occupational Health Counseling? Study Design and Results of a Feasibility Study (In German: Lassen sich Beschäftigte mit arterieller Hypertonie durch eine motivierende betriebsärztliche Beratung zum Besuch des Hausarztes motivieren? Studiendesign und Ergebnisse einer Machbarkeitsstudie). Ph.D. Thesis, Medical Faculty of the Eberhard Karls University of Tübingen, Tübingen, Germany, 2014. [Google Scholar]
- Frick, K.M.; Brueck, R. Short Interventions with Motivational Interviewing (In German: Kurzintervention mit Motivierender Gesprächsführung); Deutscher Ärzte-Verlag: Köln, Germany, 2009; ISBN 9783769105858. [Google Scholar]
- Frick, K. Motivational interviewing—Health-promoting counseling (In German: Motivierende Gesprächsführung–gesundheitsförderlich beraten). In Prevention and Health Promotion at the Interface between Curative Medicine and Occupational Medicine; Rieger, M.A., Hildebrand, S., Nesseler, T., Letzel, S., Nowak, D., Eds.; A Compendium for Corporate Health Management; Ecomed: Landsberg, Germany, 2016; pp. 122–137. ISBN 978-3-609-10560-4. [Google Scholar]
- Farian, C.; Michaelis, M.; Schüle, B.; Riedel, M.K.; Rieger, M.A. Repeated blood pressure measurement—Practicability of two methods for the validation of high readings for employees in a company medical setting. Results of a feasibility study (In German: Wiederholende Blutdruck-Messung—Praktikabilität zweier Methoden zur Validierung hoher Messwerte bei Beschäftigten im werksärztlichen Setting. Ergebnisse einer Machbarkeitsstudie). In Proceedings of the 58th Congress of the Society for Work Science (GfA), Kassel, Germany, 22–24 February 2012; GfA-Press: Dortmund, Germany, 2012; pp. 923–926. [Google Scholar]
- Keil, U.; Fitzgerald, A.P.; Gohlke, H.; Wellmann, J.; Hense, H.-W. Risk assessment of fatal cardiovascular diseases. The new SCORE Germany Tables for primary prevention (In German: Risikoabschätzung tödlicher Herz-Kreislauf-Erkrankungen: Die neuen SCORE-Deutschland-Tabellen für die Primärprävention). Dtsch. Arztebl. 2005, 102, 1808–1812. Available online: https://www.aerzteblatt.de/archiv/47409/Risikoabschaetzung-toedlicher-Herz-Kreislauf-Erkrankungen-Die-neuen-SCORE-Deutschland-Tabellen-fuer-die-Primaerpraevention (accessed on 16 November 2020).
- Donabedian, A. The definition of quality and approaches to its assessment. In Explorations in Quality Assessment and Monitoring; Health Administration Press: Chicago, IL, USA, 1980; Volume I. [Google Scholar]
- Bühner, M.; Ziegler, M. Statistics for Psychologists and Social Scientists; Pearson (in German Statistik für Psychologen und Sozialwissenschaftler): Munic, Germany, 2009. [Google Scholar]
- Seibt, R.; Naumann, H.-J.; Hinz, A. Evaluation criteria of blood pressure self-measurement and 24-hour blood pressure measurement (In German: Bewertungskriterien der Blutdruckselbstmessung und der 24-Stunden-Blutdruckmessung). Nieren-Hochdruckkrankh 1996, 25, 337–340. [Google Scholar]
- Seibt, R.; Hunger, B.; Stieler, L.; Stoll, R.; Kreuzfeld, S. Early Detection of Undiagnosed Hypertension Based on Occupational Screening in the Hotel and Restaurant Industry. Biomed Res. Int. 2018, 6820160. [Google Scholar] [CrossRef] [PubMed]
- Brueck, R.; Frick, K.; Loessl, B.; Kriston, L.; Schondelmaier, S.; Go, C.; Härter, M.; Berner, M. Psychometric properties of the German Version of the Motivational Interviewing Treatment Integrity Code (MITI-d). J. Subst. Abuse Treat. 2009, 36, 44–48. [Google Scholar] [CrossRef] [PubMed]
- Jarbøl, D.E.; Larsen, P.V.; Gyrd-Hansen, D.; Søndergaard, J.; Brandt, C.; Leppin, A.; Barfoed, B.L.; Nielsen, J.B. Determinants of preferences for lifestyle changes versus medication and beliefs in ability to maintain lifestyle changes. A population-based survey. Prev. Med. Rep. 2017, 6, 66–73. [Google Scholar] [CrossRef] [PubMed]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Michaelis, M.; Witte, C.; Schüle, B.; Frick, K.; Rieger, M.A. Can Motivational Interviewing Make a Difference in Supporting Employees to Deal with Elevated Blood Pressure? A Feasibility Study at the Workplace. Int. J. Environ. Res. Public Health 2021, 18, 4179. https://doi.org/10.3390/ijerph18084179
Michaelis M, Witte C, Schüle B, Frick K, Rieger MA. Can Motivational Interviewing Make a Difference in Supporting Employees to Deal with Elevated Blood Pressure? A Feasibility Study at the Workplace. International Journal of Environmental Research and Public Health. 2021; 18(8):4179. https://doi.org/10.3390/ijerph18084179
Chicago/Turabian StyleMichaelis, Martina, Carmen Witte (née Farian), Barbara Schüle, Katrin Frick, and Monika A. Rieger. 2021. "Can Motivational Interviewing Make a Difference in Supporting Employees to Deal with Elevated Blood Pressure? A Feasibility Study at the Workplace" International Journal of Environmental Research and Public Health 18, no. 8: 4179. https://doi.org/10.3390/ijerph18084179
APA StyleMichaelis, M., Witte, C., Schüle, B., Frick, K., & Rieger, M. A. (2021). Can Motivational Interviewing Make a Difference in Supporting Employees to Deal with Elevated Blood Pressure? A Feasibility Study at the Workplace. International Journal of Environmental Research and Public Health, 18(8), 4179. https://doi.org/10.3390/ijerph18084179