
Examining the Neighborhood Attributes of Recently Housed Partner Violence Survivors in Rapid Rehousing

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting
2.2. Participants
2.3. Data Collection Procedures
2.3.1. Survey Data Collection
2.3.2. Participant-Facilitated Geocoding
2.3.3. Qualitative Data Collection
2.3.4. Ethical Considerations
2.4. Measures
2.4.1. Census Tract-Level Outcome Variables: Neighborhood Deprivation and Residential Segregation
2.4.2. Covariates
2.5. Data Analysis
2.5.1. Quantitative Data Analysis
2.5.2. Qualitative Data Analysis
3. Results
3.1. Descriptive Statistics: Sample Characteristics and Neighborhood Indicators
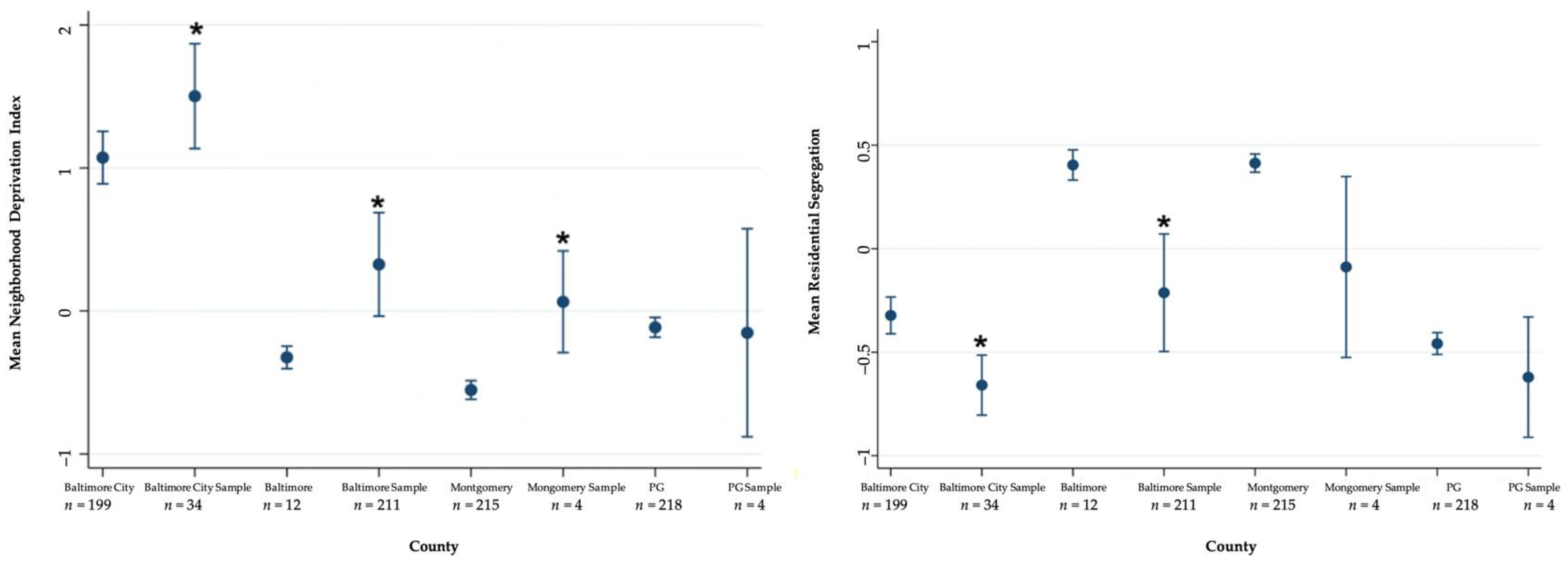
3.2. Spatial Distribution of Recently Re-Housed IPV Survivors in Study Areas and NDI and Residential Segregation Characteristics
3.3. Factors Associated with NDI among Recently Housed IPV Survivors
3.4. Factors Associated with Residential Segregation among Recently Housed IPV Survivors
3.5. Considerations of IPV Survivor’s Re-Housing Decisions
3.5.1. Overview of Housing Location Considerations
3.5.2. Considerations of Family, Friends, and Other Loved Ones
“I’m being really careful with my friends so that they don’t associate my name and my new address. Who knows how it gets leaked? But, at the same time, it’s still not too far away for them to visit me. It’s much more [important] for me and the children to live in a safe home away from friends than living in a place where I have to hide more, where I have to worry about if he is looking for me.”(1055)
“I told my friends and family in North Carolina (about the abuse), but it’s nothing they can really do because they all way down there. That’s another reason why I was so worried about getting a place to stay.”(1028)
“Since I’m alone here, and I don’t have family. Well, recently, one cousin is close, but I don’t have family here. For me, it was very important to stay in the place that I already knew to have some distant neighbors, at least, to ask for help. If I were in a totally new neighborhood, it would have been different.”(1067)
“I didn’t want to be too far away from my family, but I didn’t want to be so close that I can walk. (…) not super, super far to where it’s a 30-minute commute or anything like that.”(1045)
“Luckily, I do have family who would be willing to watch one or two of them, or my mom would take all three of them. (…) I just need somebody, some other adult supervision, to help. (laughs) She (mom) will take them off my hands and let me get some rest. It’s been pretty good.”(1025)
My family, like my mom, my sisters, and my brothers, they’re all supportive of me. (…) They didn’t turn their backs on me because I took him back. (…) I still have all my family to stand behind me, like to go and talk to if I need to. They might not give me the advice I want to hear or sugarcoat things, but sometimes honesty and straightforwardness are what you really need.(1045)
However, proximity to loved ones did not impact the housing selection of one who lacked family support. “Nobody never comes to see us. Nobody, no matter where I live.”(1032)
3.5.3. Housing Affordability Stress
“I mean, my housing in itself is OK, but I live every day not knowing if I can pay the amount that needs to be paid because I’m not working.”(1018)
“I’m just starting to pay my rent on my own. I had to get help from other sources because I got in an accident at work. The trailer hit me. I was out of work for a long time.”(1032)
“My current living situation, I live with myself and my two kids, my two sons. It’s not really stable because I lost my job when all of this stuff was going on (laughs). It’s a struggle trying to stay on a good foot. (…) Now I’m in debt because I’m struggling (after not being able to secure additional services).”(1018)
“I’m still a little behind and stuff. I’m not really sure if I’m going to be able to pay. I paid my rent for this month. I did do that, but I still have my BG&E [gas and electric] to pay. I still have my water to pay, my car insurance, and my car payment. Then it’s like, “Oh, my God. It’s so much stuff.” This is my very first house by myself. I’ve always lived with my mom, so I never really had to deal with all the bills being on top of me and having to stretch my money out, working paycheck to paycheck, and stuff like that. It’s a little scary because I really don’t know if I’m going to be able to. I’m going to try to stay positive. Don’t stress about tomorrow. Just worry about today. That’s all I really can do.”(1045)
3.5.4. Trouble Finding Housing
“I filled out for this apartment about three months into being at the (shelter). I had to wait until I passed inspection. At first, I didn’t know what it was. I think he [the landlord] was just giving me the runaround. I applied, my finances were in order, everything was correct on my end. He kept telling me that we’re waiting to be scheduled. What happened is he got the inspection, and the inspection did not pass. Then, he kept having me waiting. Finally, the inspection came around again. That’s when I got it.”(1031)
“I was supposed to move on April 5th, but it didn’t pass the inspection. Once they fixed whatever the inspector had told them, it took forever for the inspector to come back. So that pushed it all the way out. I think I moved in on May 30th.”(1023)
“At first, when the inspectors came out, they had failed it twice, so I was getting a little discouraged and stuff because my counselor told me that the inspectors only go out three times, and if they deny it all three times, then I would have to look for somewhere else to go because they wasn’t going to keep coming out. Thankfully, the third time that the inspectors came out, everything was passed.”(1045)
“You can get there, and some places make you feel as though you are beneath society because you need additional help from the government or from wherever you’re getting the help from. Sometimes, it makes you not want to visit certain places because you feel like they’re going to look at you like, oh, they want a handout.”(1028)
“What was hard about it is what a lot of people don’t know or understand that it’s a lot of people that scam people out there. It didn’t happen to me per se. Because of the information that I got from someone else at the (shelter), I was able to not be in the same situation. What happened was a young lady went to go see a house. She put her money down on the house regarding an application fee. The person that was renting out the house did that with other people, meaning they collected all of the application fees, even though they knew that they already selected someone for that place. Eventually, when you do a lot of application fees, that’s almost a month’s rent, you know?”(1010)
“The trouble that I had also is even though I was going to have a voucher, they want you to have three times the income. (…) I had to tell them everything. Even if I was receiving money or something from someone as a gift, I had to put all of that down in order for me to get this place (new home) because a lot of the other places wasn’t working with me.”(1010)
3.5.5. Neighborhood Safety
“I felt like I made a poor choice as far as the neighborhood. I should have took time if I had more time, and I think that was the problem. I didn’t have enough time to really research the neighborhood.”(1010)
“I don’t feel safe here no more. I’m ready to find a new house and move. It’s too much for me.”(1048)
“I feel safe here besides them stealing my packages. That just makes me feel like I don’t want to live here no more. Then it makes me feel like somebody’s watching me, my every move, stuff like that.”(1032)
“Since I moved in September, maybe about nine people have been killed in the neighborhood, and one across the street. It’s to the point that my kids really don’t go outside, and if they do, maybe the backyard. We pretty much stay inside the house, and I only leave out if I really have to.”(1010)
“I don’t speak to nobody. I go to the store, buy me some cigarettes, and go back in the house.”(1028)
“The front door has been kicked in before, and she (landlord) never fixed the frame. It still wobbles. The door’s still hard to close. The window doesn’t lock. It’s the front window. That where my daughter be right there playing her games. What if somebody comes through the window?”
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dichter, M.E.; Wagner, C.; Borrero, S.; Broyles, L.; Montgomery, A.E. Intimate partner violence, unhealthy alcohol use, and housing instability among women veterans in the Veterans Health Administration. Psychol. Serv. 2017, 14, 246–249. [Google Scholar] [CrossRef]
- Kull, M.A.; Coley, R.L.; Lynch, A.D. The Roles of Instability and Housing in Low-Income Families’ Residential Mobility. J. Fam. Econ. Issues 2016, 37, 422–434. [Google Scholar] [CrossRef]
- Montgomery, A.E.; Sorrentino, A.E.; Cusack, M.C.; Bellamy, S.L.; Medvedeva, E.; Roberts, C.B.; Dichter, M.E. Recent Intimate Partner Violence and Housing Instability Among Women Veterans. Am. J. Prev. Med. 2018, 54, 584–590. [Google Scholar] [CrossRef]
- Pavao, J.; Alvarez, J.; Baumrind, N.; Induni, M.; Kimerling, R. Intimate partner violence and housing instability. Am. J. Prev. Med. 2007, 32, 143–146. [Google Scholar] [CrossRef]
- Baker, C.K.; Cook, S.L.; Norris, F.H. Domestic Violence and Housing Problems: A Contextual Analysis of Women’s Help-seeking, Received Informal Support, and Formal System Response. Violence Against Women 2003, 9, 754–783. [Google Scholar] [CrossRef]
- Clough, A.; Draughon, J.E.; Njie-Carr, V.; Rollins, C.; Glass, N. ‘Having housing made everything else possible’: Affordable, safe and stable housing for women survivors of violence. Qual. Soc. Work 2013, 13, 671–688. [Google Scholar] [CrossRef] [Green Version]
- Arnold, G.W. From Victim to Offender: How Nuisance Property Laws Affect Battered Women. J. Interpers. Violence 2016, 34, 1103–1126. [Google Scholar] [CrossRef]
- Mayock, P.; Sheridan, S.; Parker, S. ‘It’s just like we’re going around in circles and going back to the same thing …’: The Dynamics of Women’s Unresolved Homelessness. Hous. Stud. 2015, 30, 877–900. [Google Scholar] [CrossRef]
- Osuji, J.; Hirst, S. History of abuse and the experience of homelessness: A framework for assisting women overcome housing instability. Hous. Care Support 2015, 18, 89–100. [Google Scholar] [CrossRef]
- Wesely, J.K.; Wright, J.D. The Pertinence of Partners: Examining Intersections Between Women’s Homelessness and Their Adult Relationships. Am. Behav. Sci. 2005, 48, 1082–1101. [Google Scholar] [CrossRef]
- Olsen, L.; Rollins, C.; Billhardt, K. The Intersection of Domestic Violence and Homelessness; Washington State Coalition Against Domestic Violence: Washington, DC, USA, 2013. [Google Scholar]
- Campbell, J.C.; Webster, D.; Koziol-McLain, J.; Block, C.; Campbell, D.; Curry, M.A.; Gary, F.; Glass, N.; McFarlane, J.; Sachs, C.; et al. Risk factors for femicide in abusive relationships: Results from a multisite case control study. Am. J. Public Health 2003, 93, 1089–1097. [Google Scholar] [CrossRef] [PubMed]
- Swope, C.B.; Hernandez, D. Housing as a determinant of health equity: A conceptual model. Soc. Sci. Med. 2019, 243, 112571. [Google Scholar] [CrossRef] [PubMed]
- Wilson, W.J. The Truly Disadvantaged: The Inner City, the Underclass, and Public Policy, 2nd ed.; University of Chicago Press: Chicago, IL, USA, 2012; 317p. [Google Scholar]
- Massey, D. The Prodigal Paradigm Returns: Ecology Comes Back to Sociology. In Does It Take A Village?: Community Effects on Children, Adolescents, and Families; Booth, A., Crouter, A.C., Eds.; Lawrence Erlbaum Associates, Inc.: Mahwah, NJ, USA, 1999; pp. 44–48. [Google Scholar]
- Rothstein, R. The Color. of Law: A Forgotten History of How Our Government Segregated America; Liveright: New York, NY, USA, 2017. [Google Scholar]
- Mehra, R.; Boyd, L.M.; Ickovics, J.R. Racial residential segregation and adverse birth outcomes: A systematic review and meta-analysis. Soc. Sci. Med. 2017, 191, 237–250. [Google Scholar] [CrossRef] [PubMed]
- Mendez, D.D.; Thorpe, R.J.; Amutah, N.; Davis, E.M.; Walker, R.E.; Chapple-McGruder, T.; Bodnar, L. Neighborhood racial composition and poverty in association with pre-pregnancy weight and gestational weight gain. SSM Popul. Health 2016, 2, 692–699. [Google Scholar] [CrossRef] [Green Version]
- Mendez, D.D.; Doebler, D.A.; Kim, K.H.; Amutah, N.N.; Fabio, A.; Bodnar, L.M. Neighborhood socioeconomic disadvantage and gestational weight gain and loss. Matern Child. Health J. 2014, 18, 1095–1103. [Google Scholar] [CrossRef] [PubMed]
- Mayne, S.L.; Yellayi, D.; Pool, L.R.; Grobman, W.A.; Kershaw, K.N. Racial Residential Segregation and Hypertensive Disorder of Pregnancy Among Women in Chicago: Analysis of Electronic Health Record Data. Am. J. Hypertens. 2018, 31, 1221–1227. [Google Scholar] [CrossRef] [Green Version]
- Nardone, A.L.; Casey, J.A.; Rudolph, K.E.; Karasek, D.; Mujahid, M.; Morello-Frosch, R. Associations between historical redlining and birth outcomes from 2006 through 2015 in California. PLoS ONE 2020, 15, e0237241. [Google Scholar] [CrossRef] [PubMed]
- Salow, A.D.; Pool, L.R.; Grobman, W.A.; Kershaw, K.N. Associations of neighborhood-level racial residential segregation with adverse pregnancy outcomes. Am. J. Obs. Gynecol. 2018, 218, 351.e1–351.e7. [Google Scholar] [CrossRef]
- Beyer, K.; Wallis, A.B.; Hamberger, L.K. Neighborhood Environment and Intimate Partner Violence: A Systematic Review. Trauma Violence Abus. 2013, 16, 16–47. [Google Scholar] [CrossRef] [Green Version]
- Obasaju, M.A.; Palin, F.L.; Jacobs, C.; Anderson, P.; Kaslow, N.J. Won’t you be my neighbor? Using an ecological approach to examine the impact of community on revictimization. J. Interpers Violence 2009, 24, 38–53. [Google Scholar] [CrossRef] [PubMed]
- Gezinski, L.B.; Gonzalez-Pons, K.M. Unlocking the Door to Safety and Stability: Housing Barriers for Survivors of Intimate Partner Violence. J. Interpers Violence 2019, 0886260519851792. [Google Scholar] [CrossRef] [PubMed]
- Barata, P.C.; Stewart, D.E. Searching for Housing as a Battered Woman: Does Discrimination Affect Reported Availability of a Rental Unit? Psychol. Women Q. 2010, 34, 43–55. [Google Scholar] [CrossRef]
- Pager, D.; Shepherd, H. The Sociology of Discrimination: Racial Discrimination in Employment, Housing, Credit, and Consumer Markets. Annu. Rev. Sociol. 2008, 34, 181–209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holliday, C.N.; Morse, S.M.; Irvin, N.A.; Green-Manning, A.; Nitsch, L.M.; Burke, J.G.; Campbell, J.C.; Decker, M.R. Concept Mapping: Engaging Urban Men to Understand Community Influences on Partner Violence Perpetration. J. Urban Health Bull. N. Y. Acad. Med. 2018, 96, 97–111. [Google Scholar] [CrossRef] [PubMed]
- Johnson, R.M.; Parker, E.M.; Rinehart, J.; Nail, J.; Rothman, E.F. Neighborhood Factors and Dating Violence Among Youth: A Systematic Review. Am. J. Prev. Med. 2015, 49, 458–466. [Google Scholar] [CrossRef] [Green Version]
- O’Campo, P.; Burke, J.; Peak, G.L.; McDonnell, K.A.; Gielen, A.C. Uncovering neighbourhood influences on intimate partner violence using concept mapping. J. Epidemiol. Community Health 2005, 59, 603–608. [Google Scholar] [CrossRef] [Green Version]
- Mears, D.P.; Carlson, M.J.; Holden, G.W.; Harris, S.D. Reducing Domestic Violence Revictimization: The Effects of Individual and Contextual Factors and Type of Legal Intervention. J. Interpers. Violence 2001, 16, 1260–1283. [Google Scholar] [CrossRef]
- McKinney, C.M.; Caetano, R.; Harris, T.R.; Ebama, M.S. Alcohol availability and intimate partner violence among US couples. Alcohol. Clin. Exp. Res. 2009, 33, 169–176. [Google Scholar] [CrossRef] [PubMed]
- Benson, M.L.; Fox, G.L.; DeMaris, A.; Van Wyk, J. Neighborhood Disadvantage, Individual Economic Distress and Violence Against Women in Intimate Relationships. J. Quant. Criminol. 2003, 19, 207–235. [Google Scholar] [CrossRef]
- Li, Q.; Kirby, R.S.; Sigler, R.T.; Hwang, S.-S.; LaGory, M.E.; Goldenberg, R.L. A Multilevel Analysis of Individual, Household, and Neighborhood Correlates of Intimate Partner Violence Among Low-Income Pregnant Women in Jefferson County, Alabama. Am. J. Public Health 2010, 100, 531–539. [Google Scholar] [CrossRef]
- Waller, M.W.; Iritani, B.J.; Christ, S.L.; Clark, H.K.; Moracco, K.E.; Halpern, C.T.; Flewelling, R.L. Relationships among alcohol outlet density, alcohol use, and intimate partner violence victimization among young women in the United States. J. Interpers Violence 2012, 27, 2062–2086. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cunradi, C.B. Drinking level, neighborhood social disorder, and mutual intimate partner violence. Alcohol. Clin. Exp. Res. 2007, 31, 1012–1019. [Google Scholar] [CrossRef] [PubMed]
- Cunradi, C.B. Intimate partner violence among hispanic men and women: The role of drinking, neighborhood disorder, and acculturation-related factors. Violence Vict. 2009, 24, 83–97. [Google Scholar] [CrossRef] [PubMed]
- Browning, C.R. The Span of Collective Efficacy: Extending Social Disorganization Theory to Partner Violence. J. Marriage Fam. 2002, 64, 833–850. [Google Scholar] [CrossRef]
- DeMaris, A.; Benson, M.L.; Fox, G.L.; Hill, T.; Van Wyk, J. Distal and Proximal Factors in Domestic Violence: A Test of an Integrated Model. J. Marriage Fam. 2003, 65, 652–667. [Google Scholar] [CrossRef]
- Lauritsen, J.L.; Schaum, R.J. The Social Ecology of Violence Against Women. Criminology 2004, 42, 323–357. [Google Scholar] [CrossRef]
- Van Wyk, J.A.; Benson, M.L.; Fox, G.L.; DeMaris, A. Detangling Individual-, Partner-, and Community-level Correlates of Partner Violence. Crime Delinq. 2003, 49, 412–438. [Google Scholar] [CrossRef]
- Dekeseredy, W.S.; Alvi, S.; Tomaszewski, E.A. Perceived collective efficacy and women’s victimization in public housing. Crim. Justice 2003, 3, 5–27. [Google Scholar] [CrossRef] [Green Version]
- Raghavan, C.; Mennerich, A.; Sexton, E.; James, S.E. Community violence and its direct, indirect, and mediating effects on intimate partner violence. Violence Against Women 2006, 12, 1132–1149. [Google Scholar] [CrossRef] [PubMed]
- Reed, E.; Silverman, J.G.; Welles, S.L.; Santana, M.C.; Missmer, S.A.; Raj, A. Associations between perceptions and involvement in neighborhood violence and intimate partner violence perpetration among urban, African American men. J. Community Health 2009, 34, 328–335. [Google Scholar] [CrossRef]
- Stueve, A.; O’Donnell, L. Urban young women’s experiences of discrimination and community violence and intimate partner violence. J. Urban Health Bull. N. Y. Acad. Med. 2008, 85, 386–401. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, L.T. The Black Butterfly: The Harmful Politics of Race and Space in America; Johns Hopkins University Press: Baltimore, ML, USA, 2021. [Google Scholar]
- DeLuca, S.; Garboden, P.M.E.; Rosenblatt, P. Segregating Shelter: How Housing Policies Shape the Residential Locations of Low-Income Minority Families. Ann. Am. Acad. Political Soc. Sci. 2013, 647, 268–299. [Google Scholar] [CrossRef]
- Jaramillo, A.; Rohe, W.M.; Webb, M.D. Neighborhood Opportunity and Satisfaction Among Housing Choice Voucher Recipients: A Subjective Well-Being Perspective. Hous. Policy Debate 2020, 30, 703–717. [Google Scholar] [CrossRef]
- Rice, R.L. Residential Segregation by Law, 1910–1917. J. South. Hist. 1968, 34, 179–199. [Google Scholar] [CrossRef]
- Massey, D. The Legacy of the 1968 Fair Housing Act. Sociol. Forum 2015, 30, 571–588. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conley, D. Being Black, Living in the Red: Race, Wealth, and Social Policy in America; University of California Press: Berkeley, CA, USA, 1999; 209p. [Google Scholar]
- Pfeffer, F.T.; Killewald, A. Intergenerational Wealth Mobility and Racial Inequality. Socius 2019, 5, 2378023119831799. [Google Scholar] [CrossRef]
- Wilson, W.J. The Truly Disadvantaged: The Inner City, the Underclass, and Public Policy; University of Chicago Press: Chicago, IL, USA, 1987; 254p. [Google Scholar]
- Richardson, J.; Mitchell, B.; West, N. Home Mortgage and Small Business Lending in Baltimore and Surrounding Areas; National Community Reinvestment Coalition: Washington, DC, USA, 2015. [Google Scholar]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Cond, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing transla-tional research informatics support. J. Biomed. Inf. 2009, 42, 377–381. [Google Scholar] [CrossRef] [Green Version]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap consortium: Building an international community of software platform partners. J. Biomed. Inf. 2019, 95, 103208. [Google Scholar] [CrossRef] [PubMed]
- United States Census Bureau. Geocoder. 2021. Available online: https://geocoding.geo.census.gov/geocoder/geographies/address?form (accessed on 15 February 2021).
- Perez, S.; Johnson, D.M.; Wright, C.V. The attenuating effect of empowerment on IPV-related PTSD symptoms in battered women living in domestic violence shelters. Violence Against Women 2012, 18, 102–117. [Google Scholar] [CrossRef] [PubMed]
- WHO. Ethical and safety recommendations for intervention research on violence against women. In Putting Women First: Ethical and Safety Recommendations for Research on Domestic Violence against Women; World Health Organization: Geneva, Switzerland, 2016; Available online: https://www.who.int/reproductivehealth/publications/violence/intervention-research-vaw/en/ (accessed on 8 April 2021).
- 2013–2017 ACS 5-Year Estimates [Internet]. 2018. Available online: https://www.census.gov/programs-surveys/acs/technical-documentation/table-and-geography-changes/2017/5-year.html (accessed on 15 February 2021).
- Messer, L.C.; Laraia, B.A.; Kaufman, J.S.; Eyster, J.; Holzman, C.; Culhane, J.; Elo, I.; Burke, J.G.; O’campo, P. The development of a standardized neighborhood deprivation index. J. Urban Health Bull. N. Y. Acad. Med. 2006, 83, 1041–1062. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DeVellis, R.F. Scale Development: Theory and Applications, 3rd ed.; Sage Publications: Thousand Oaks, CA, USA, 2003. [Google Scholar]
- Robbins, H.A.; Hurley, E.A.; Liu, L.; Chao, S.M. Multilevel correlates of broadly- and narrowly-defined intimate partner violence among pregnant women in Los Angeles. Matern. Child. Health J. 2015, 19, 1643–1651. [Google Scholar] [CrossRef] [Green Version]
- Krieger, N.; Waterman, P.D.; Batra, N.; Murphy, J.S.; Dooley, D.P.; Shah, S.N. Measures of Local Segregation for Monitoring Health Inequities by Local Health Departments. Am. J. Public Health 2017, 107, 903–906. [Google Scholar] [CrossRef] [PubMed]
- Closson, K.; Smith, R.V.; Olarewaju, G.; Crosby, R. Associations between economic dependence, sexual behaviours, and sexually transmitted infections among young, Black, gay, bisexual and other men who have sex with men living with and without HIV in Jackson, Mississippi, USA. Sex. Health 2018, 15, 473–476. [Google Scholar] [CrossRef] [PubMed]
- House of Ruth Maryland. Measuring Success. 2021. Available online: https://hruth.org/training-institute/measuring-success/ (accessed on 8 April 2021).
- Breiding, M.J.; Basile, K.C.; Klevens, J.; Smith, S.G. Economic Insecurity and Intimate Partner and Sexual Violence Victimization. Am. J. Prev. Med. 2017, 53, 457–464. [Google Scholar] [CrossRef] [PubMed]
- Rollins, C.; Glass, N.E.; Perrin, N.A.; Billhardt, K.A.; Clough, A.; Barnes, J.; Hanson, G.C.; Bloom, T.L. Housing Instability Is as Strong a Predictor of Poor Health Outcomes as Level of Danger in an Abusive Relationship: Findings From the SHARE Study. J. Interpers. Violence 2012, 27, 623–643. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harding, H.G.; Helweg-Larsen, M. Perceived Risk for Future Intimate Partner Violence among Women in a Domestic Violence Shelter. J. Fam. Violence 2008, 24, 75–85. [Google Scholar] [CrossRef]
- Mujahid, M.S.; Diez Roux, A.V.; Morenoff, J.D.; Raghunathan, T. Assessing the measurement properties of neighborhood scales: From psychometrics to ecometrics. Am. J. Epidemiol. 2007, 165, 858–867. [Google Scholar] [CrossRef]
- Straus, M.A.; Douglas, E.M. A Short Form of the Revised Conflict Tactics Scales, and Typologies for Severity and Mutuality. Violence Vict. 2005, 19, 507–520. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The Patient Health Questionnaire-2: Validity of a Two-Item Depression Screener. Med. Care 2003, 41, 1284–1292. [Google Scholar] [CrossRef]
- Lang, A.J.; Stein, M.B. An abbreviated PTSD checklist for use as a screening instrument in primary care. Behav. Res. 2005, 43, 585–594. [Google Scholar] [CrossRef]
- QGIS. Version 3.18.0. 2021. Available online: https://qgis.org/en/site/ (accessed on 26 February 2021).
- Maryland Census Data—Census Tracts [Internet]. 2020. Available online: https://data.imap.maryland.gov/datasets/bbe7d09a81fc40c8a7c9f4c80155842e_0 (accessed on 18 February 2021).
- Maryland Physical Boundaries- County Boundaries (Generalized) [Internet]. 2019. Available online: https://data.imap.maryland.gov/datasets/4c172f80b626490ea2cff7b699febedb_1 (accessed on 18 February 2021).
- StataCorp. Stata Statistical Software: Release 15; StataCorp LLC: College Station, TX, USA, 2017; Available online: https://www.stata.com (accessed on 8 April 2021).
- Glaser, B. The Constant Comparative Method of Qualitative Analysis. Soc. Probl. 1965, 12, 436–445. [Google Scholar] [CrossRef]
- Maxwell, J.A. Qualitative Research Design; Leonard Bickman, D.J.R., Ed.; SAGE Publications: Thousand Oaks, CA, USA, 2005. [Google Scholar]
- LeCompte, M.; Schensul, J. Analyizing and Interpreting Ethnographic Data; SAGE Press: Walnut Creek, PA, USA, 1999. [Google Scholar]
- Glaser, B.; Strauss, A. The Discovery of Grounded Theory: Strategies for Qualitative Research; Aldine de Gruyter: Chicago, IL, USA, 1967. [Google Scholar]
- Postmus, J.L.; Plummer, S.B.; McMahon, S.; Murshid, N.S.; Kim, M.S. Understanding economic abuse in the lives of survivors. J. Interpers Violence 2012, 27, 411–430. [Google Scholar] [CrossRef] [PubMed]
- England, P.; Levine, A.; Mishel, E. Progress toward gender equality in the United States has slowed or stalled. Proc. Natl. Acad. Sci. USA 2020, 117, 6990–6997. [Google Scholar] [CrossRef] [PubMed]
- Glass, N.; Eden, K.B.; Bloom, T.; Perrin, N. Computerized aid improves safety decision process for survivors of intimate partner violence. J. Interpers Violence 2010, 25, 1947–1964. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glass, N.E.; Clough, A.; Messing, J.T.; Bloom, T.; Brown, M.L.; Eden, K.B.; Campbell, J.C.; Gielen, A.; Laughon, K.; Grace, K.T.; et al. Longitudinal Impact of the myPlan App on Health and Safety Among College Women Experiencing Partner Violence. J. Interpers Violence 2021, 886260521991880. [Google Scholar] [CrossRef]
- Parenteau, M.P.; Sawada, M.C. The modifiable areal unit problem (MAUP) in the relationship between exposure to NO2 and respiratory health. Int. J. Health Geogr. 2011, 10, 58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- US Department of Justice. Investigation of the Baltimore City Police Department; U.S. Department of Justice, Civil Rights Division: Washington, DC, USA, 2016. Available online: https://www.justice.gov/opa/file/883366/download (accessed on 8 April 2021).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| % (n) | |
|---|---|
| DEMOGRAPHIC CHARACTERISTICS | |
| Age | |
| Less than 35 years | 63 (34) |
| 35 years or older | 37 (20) |
| Race | |
| White | 2 (1) |
| Black | 76 (41) |
| Hispanic | 7 (4) |
| Asian/Other | 6 (3) |
| Multiracial | 9 (5) |
| ECONOMIC CHARACTERISTICS | |
| Education | |
| Some HS | 7 (4) |
| HS Graduate | 35 (19) |
| At least some college | 57 (31) |
| Income | |
| $0–$16,000 | 33 (17) |
| $16,001–$24,000 | 29 (15) |
| $24,001–$32,000 | 13 (7) |
| $32,001 or more | 25 (13) |
| Past month employment (Yes) | 65 (35) |
| Financial ability | |
| Meets needs independently | 6 (3) |
| Meets needs with assistance | 47 (25) |
| Partially meets needs with assistance | 38 (20) |
| Cannot meet needs | 9 (5) |
| Food stress | |
| Always or usually | 40 (21) |
| Sometimes | 28 (15) |
| Rarely/never | 32 (17) |
| Economically dependent on partner | 57 (31) |
| HOUSING CHARACTERISTICS | |
| Trouble getting housing, past 3 m | 59 (29) |
| Recent difficulty with landlord | 23 (12) |
| Housing affordability stress | |
| Always | 59 (31) |
| Sometimes | 28 (15) |
| Rarely/Never | 13 (7) |
| HEALTH CHARACTERISTICS | |
| PTSD Symptoms | 78 (42) |
| Unable to access necessary healthcare, past 12 m | 17 (9) |
| Depression symptoms | 39 (21) |
| SOCIAL/COMMUNITY CONTEXT | |
| Intimate partner violence, past 3 m | 54 (28) |
| Feels safe at home | 87 (47) |
| Co-parenting with abusive partner | 70 (38) |
| Comfortable with proximity to family/friends | 58 (31) |
| Comfortable with proximity to abuser | 72 (38) |
| Neighborhood Deprivation Index Coeff., 95% CI | ||||
|---|---|---|---|---|
| % (n) | M (SD) | Unadjusted | Adjusted | |
| Range across four regions (847 census tracts) | - | - | −1.25, 4.30 | - |
| Range across sample (43 census tracts) | - | - | −0.88, 3.53 | - |
| Demographic Characteristics | ||||
| Age (ref: <35 years) | 63 (34) | 1.00 (1.09) | - | - |
| 35 years or older | 37 (20) | 1.04 (1.24) | 0.04 (−0.62, 0.71) | - |
| Race | - | - | 0.20 (−0.55, 0.15) | - |
| Black | 76 (41) | 1.15 (1.13) | - | - |
| White | 2 (1) | 1.24 (.) | - | - |
| Hispanic | 7 (4) | 0.36 (0.88) | - | - |
| Asian/other | 6 (3) | 0.04 (1.04) | - | - |
| Multiracial | 9 (5) | 0.92 (1.42) | - | - |
| Economic Demographic Characteristics | ||||
| Education (Ref: At least some college) | 57 (31) | 0.91 (1.17) | - | - |
| Some HS | 7 (4) | 0.59 (1.24) | −0.32 (−1.51, 0.87) | - |
| HS Graduate | 35 (19) | 1.26 (1.08) | 0.35 (−0.30, 1.00) | - |
| Income (Ref: $0–$16,000) | 33 (17) | 2.00 (1.17) | - | - |
| $16,001–$24,000 | 29 (15) | 1.07 (1.14) | −0.13 (−0.96, 0.70) | −0.12 (−1.06, 0.81) |
| $24,001–$32,000 | 13 (7) | 1.50 (1.26) | 0.30 (−0.79, 1.39) | 0.30 (−0.77, 1.37) |
| $32,001 or more | 25 (13) | 0.24 (0.51) | −0.96 (−1.61, −0.32) ** | −0.46 (−1.30, 0.38) |
| Past month employment (Yes) | 65 (35) | 1.03 (1.21) | 0.06 (−0.56, 0.68) | - |
| Financial Ability (Ref: Cannot meet needs) | 9 (5) | 0.04 (0.96) | - | - |
| Meets needs independently | 6 (3) | 1.16 (0.46) | 1.12 (0.20, 2.03) ** | 0.88 (−0.87, 2.63) |
| Meets needs with assistance | 47 (25) | 0.99 (1.11) | 0.94 (0.02, 1.86) ** | 0.82 (−0.70, 2.34) |
| Partially meets needs with assistance | 38 (20) | 1.15 (1.14) | 1.10 (0.15, 2.06) ** | 0.81(−0.82, 2.44) |
| Economically dependent on partner | 57 (31) | 1.23 (1.29) | 0.52 (−0.06, 1.10) * | 0.31 (−0.25, 0.88) |
| Food stress (Ref: Always) | 40 (21) | 1.11 (1.35) | - | - |
| Sometimes | 28 (15) | 0.78 (0.90) | −0.33 (−1.08, 0.43) | - |
| Rarely/never | 32 (17) | 0.96 (0.95) | −0.15 (−0.91, 0.60) | - |
| Housing Characteristics | ||||
| Trouble getting housing, past 3 m | 59 (29) | 1.30 (1.28) | 0.65 (0.04, 1.27) ** | 0.74 (0.13, 1.34) ** |
| Recent difficulty with landlord | 23 (12) | 1.14 (1.57) | 0.17 (−0.77, 1.11) | - |
| Housing affordability stress (Ref: Always) | 59 (31) | 1.00 (1.17) | - | - |
| Sometimes | 28 (15) | 0.78 (1.10) | −0.22(−0.93, 0.49) | - |
| Rarely/never | 13 (7) | 1.23 (0.79) | 0.23 (−0.48, 0.95) | - |
| Social/Community Context | ||||
| Feels safe at home | 87 (47) | 1.07 (1.10) | 0.45 (−0.61, 1.52) | - |
| Child(ren) with abusive partner | 70 (38) | 0.91 (1.11) | −0.33 (−1.03, 0.36) | - |
| Comfortable with proximity to family/friends | 58 (31) | 1.24 (1.00) | 0.58 (−0.06, 1.22) * | 0.75 (0.02, 1.48) ** |
| Comfortable with proximity to abuser | 72 (38) | 1.12 (1.11) | 0.44 (−0.26, 1.16) | - |
| Social cohesion (Ref: Neutral) | 50 (27) | 0.84 (0.99) | - | - |
| Yes | 39 (21) | 1.21 (1.32) | 0.38 (−0.33, 1.078) | - |
| No | 11 (6) | 1.01 (1.09) | 0.24 (−0.68, 1.16) | - |
| Intimate Partner Violence, past 3 m | 54 (28) | 1.12 (1.11) | 0.23 (−0.42, 0.87) | - |
| Perceived risk of IPV, next 3 m (Ref: Unlikely) | 69 (37) | 1.20 (1.17) | - | - |
| Unsure | 24 (13) | 0.61 (0.91) | −0.59 (−1.22, 0.05) * | −0.76 (−1.39, −0.14) ** |
| Likely | 7 (4) | 0.55 (1.30) | −0.65 (−1.84, 0.54) | −0.40 (−1.46, 0.66) |
| Constant | - | - | - | −0.59 (−2.30, 1.12) |
| Residential Segregation Coeff., 95% CI | ||||
|---|---|---|---|---|
| % (n) | M (SD) | Unadjusted | Adjusted | |
| Range across four regions (847 census tracts) | - | - | 0.99, −1 | - |
| Range across sample (43 census tracts) | - | - | 0.66, −1 | - |
| Demographic Characteristics | ||||
| Age (ref: <35 years) | 63 (34) | −0.53 (0.48) | - | - |
| 35 years or older | 37 (20) | −0.49 (0.51) | 0.05 (−0.22, 0.33) | - |
| Race | - | - | - | - |
| Black | 76 (41) | −0.59 (0.46) | - | - |
| White | 2 (1) | −0.43 (.) | - | - |
| Hispanic | 7 (4) | −0.09 (0.68) | - | - |
| Asian/other | 6 (3) | −0.27 (0.25) | - | - |
| Multiracial | 9 (5) | −0.42 (0.57) | - | - |
| Economic Demographic Characteristics | ||||
| Education (Ref: At least some college) | 57 (31) | −0.43 (0.48) | - | - |
| Some HS | 7 (4) | −0.73 (0.30) | −0.30 (−0.62, 0.02) * | −0.49 (−0.88, −0.09) ** |
| HS Graduate | 35 (19) | −0.61 (0.51) | −0.19 (−0.48, 0.10) | −0.26 (−0.57, 0.04) * |
| Income (Ref: $0–$16,000) | 33 (17) | −0.44 (0.62) | - | - |
| $16,001–$24,000 | 29 (15) | −0.47 (0.48) | −0.04 (−0.42, 0.36) | 0.01 (−0.36, 0.37) |
| $24,001–$32,000 | 13 (7) | −0.80 (0.14) | −0.37 (−0.69, 0.04) ** | −0.32 (−0.67, 0.02) * |
| $32,001 or more | 25 (13) | −0.48 (0.41) | −0.05 (−0.43, 0.33) | −0.09 (−0.49, 0.31) |
| Past month employment (Yes) | 65 (35) | −0.52 (0.45) | −0.01 (−0.30, 0.29) | |
| Financial Ability (Ref: Cannot meet needs) | 9 (5) | −0.39 (0.47) | - | |
| Meets needs independently | 6 (3) | −0.82 (0.11) | −0.43 (−0.83, −0.02) ** | −0.46 (−1.16, 0.25) |
| Meets needs with assistance | 47 (25) | −0.46 (0.53) | −0.07 (−0.52, 0.38’) | −0.22 (−0.72, 0.27) |
| Partially meets needs with assistance | 38 (20) | −0.55 (0.46) | −0.15 (−0.60, 0.29) | −0.31 (−0.80, 0.19) |
| Economically dependent on partner | 57 (31) | −0.61 (0.43) | −0.23 (−0.50, 0.03) * | −0.31 (−0.56, −0.06) ** |
| Food stress (Ref: Always) | 40 (21) | −0.60 (0.41) | - | |
| Sometimes | 28 (15) | −0.36 (0.58) | 0.24 (−0.11, 0.59) | - |
| Rarely/never | 32 (17) | −0.52 (0.47) | 0.08 (−0.21, 0.37) | - |
| Housing Characteristics | ||||
| Trouble getting housing, past 3 m | 59 (29) | −0.53 (0.52) | −0.05 (−0.33, 0.23) | - |
| Recent difficulty with landlord | 23 (12) | −0.59 (0.32) | −0.11 (−0.36, 0.13) | - |
| Housing affordability stress (Ref: Always) | 59 (31) | −0.57 (0.44) | - | - |
| Sometimes | 28 (15) | −0.28 (0.57) | 0.29 (−0.05, 0.63) * | 0.39 (0.04, 0.75) ** |
| Rarely/never | 13 (7) | −0.69 (0.32) | −0.12 (−0.40, 0.17) | −0.07 (−0.47, 0.31) |
| Social/Community Context | ||||
| Feels safe at home | 87 (47) | −0.54 (0.46) | −0.21 (−0.67, 0.24) | - |
| Child(ren) with abusive partner | 70 (38) | −0.51 (0.49) | 0.02 (−0.27, 0.31) | - |
| Comfortable with proximity to family/friends | 58 (31) | −0.60 (0.45) | −0.23 (−0.49, 0.05) | - |
| Comfortable with proximity to abuser | 72 (38) | −0.55 (0.42) | −0.15 (−0.50, 0.20) | - |
| Social cohesion (Ref: Neutral) | 50 (27) | 0.52 (0.52) | - | - |
| Yes | 39 (21) | −0.48 (0.44) | 0.05 (−0.23, 0.33) | - |
| No | 11 (6) | −0.61 (0.52) | −0.08 (−0.53, 0.37) | - |
| Intimate Partner Violence, past 3 m | 54 (28) | −0.55 (0.45) | −0.11 (−0.38, 0.17) | - |
| Perceived risk of IPV, next 3 m (Ref: Unlikely) | 69 (37) | −0.57 (0.43) | - | - |
| Unsure | 24 (13) | 0.37 (0.63) | 0.20 (−0.18, 0.57) | - |
| Likely | 7 (4) | −0.46 (0.39) | 0.11 (−0.27, 0.49) | - |
| Constant | - | - | - | 0.01 (−0.60, 0.62) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Holliday, C.N.; Bevilacqua, K.; Grace, K.T.; Denhard, L.; Kaur, A.; Miller, J.; Decker, M.R. Examining the Neighborhood Attributes of Recently Housed Partner Violence Survivors in Rapid Rehousing. Int. J. Environ. Res. Public Health 2021, 18, 4177. https://doi.org/10.3390/ijerph18084177
Holliday CN, Bevilacqua K, Grace KT, Denhard L, Kaur A, Miller J, Decker MR. Examining the Neighborhood Attributes of Recently Housed Partner Violence Survivors in Rapid Rehousing. International Journal of Environmental Research and Public Health. 2021; 18(8):4177. https://doi.org/10.3390/ijerph18084177
Chicago/Turabian StyleHolliday, Charvonne N., Kristin Bevilacqua, Karen Trister Grace, Langan Denhard, Arshdeep Kaur, Janice Miller, and Michele R. Decker. 2021. "Examining the Neighborhood Attributes of Recently Housed Partner Violence Survivors in Rapid Rehousing" International Journal of Environmental Research and Public Health 18, no. 8: 4177. https://doi.org/10.3390/ijerph18084177
APA StyleHolliday, C. N., Bevilacqua, K., Grace, K. T., Denhard, L., Kaur, A., Miller, J., & Decker, M. R. (2021). Examining the Neighborhood Attributes of Recently Housed Partner Violence Survivors in Rapid Rehousing. International Journal of Environmental Research and Public Health, 18(8), 4177. https://doi.org/10.3390/ijerph18084177