
Second-Hand Smoke and Its Synergistic Effect with a Body-Mass Index of >24.9 kg/m2 Increase the Risk of Gout Arthritis in Indonesia


 ,
,
Abstract
:1. Introduction
2. Materials and Methods
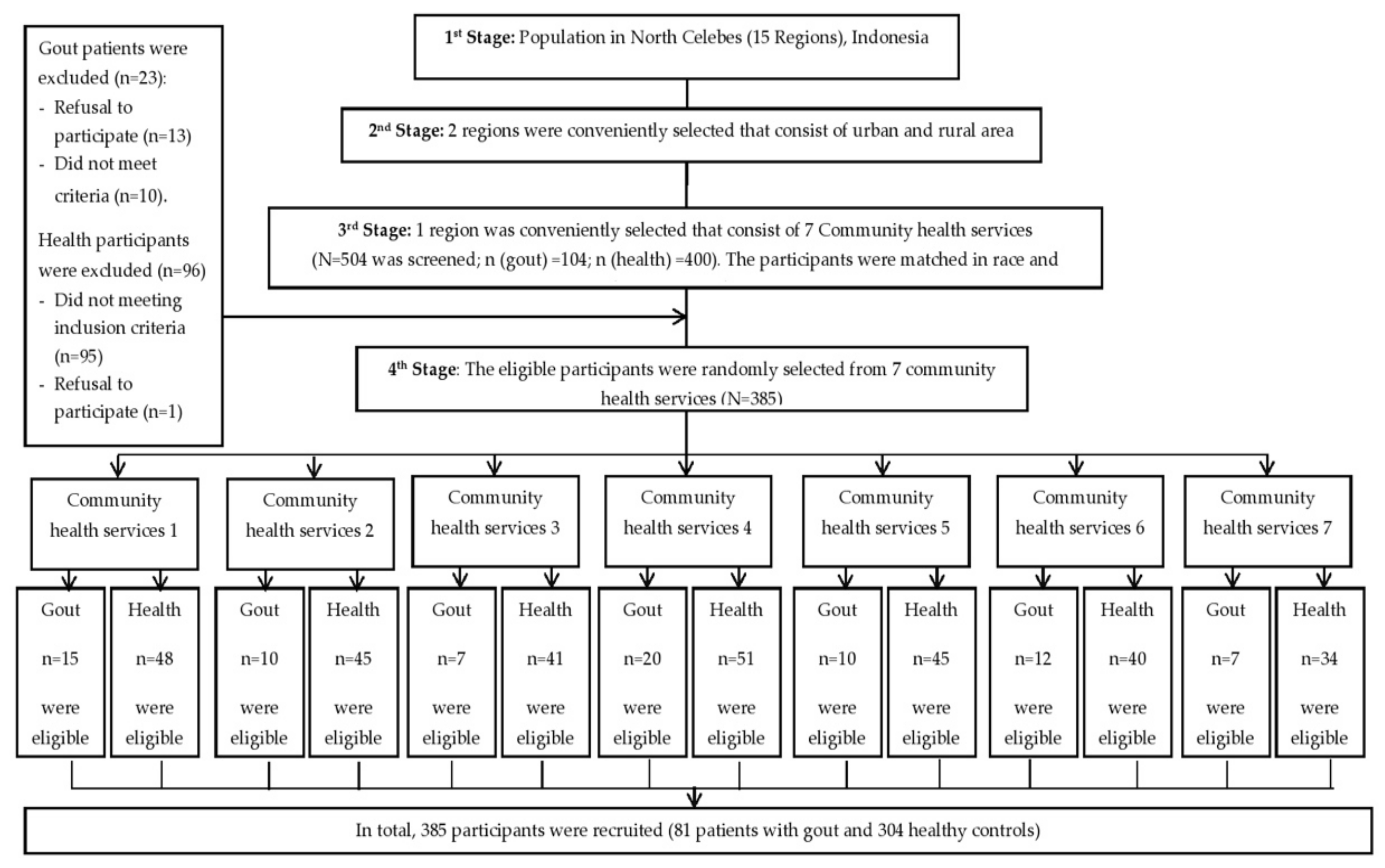
2.1. Study Design
2.2. Participants
2.3. Data Collection
2.3.1. Physical Examination and Blood Biochemistry Analysis
2.3.2. Questionnaire
2.4. Ethical Considerations
2.5. Data Analysis
3. Results
3.1. Sociodemographic Characteristics and Determination of Risk Factors for Gout
3.2. Association between Smoking Status and Gout Disease
3.3. Synergistic Effects of BMI and Smoking Status on the Risk of Gout
3.4. Association between Smoking Status and Hyperuricemia
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rock, K.; Kataoka, H.; Lai, J.-J. Uric acid as a danger signal in gout and its comorbidities. Nat. Rev. Rheumatol. 2014, 27, 1–19. [Google Scholar] [CrossRef] [Green Version]
- Xia, Y.; Wu, Q.; Wang, H.; Zhang, S.; Jiang, Y. Global, regional and national burden of gout, 1990–2017: A systematic analysis of the Global Burden of Disease Study. Rheumatology 2019. [Google Scholar] [CrossRef]
- Yu, K.-H.; Chen, D.-Y.; Chen, J.-H.; Chen, S.-Y.; Chen, S.-M.; Cheng, T.-T.; Hsieh, S.-C.; Hsieh, T.-Y.; Hsu, P.-F.; Kuo, C.-F.; et al. Management of gout and hyperuricemia: Multidisciplinary consensus in Taiwan. Int. J. Rheum. Dis. 2018, 21, 772–787. [Google Scholar] [CrossRef]
- Kuo, C.F.; Grainge, M.J.; Zhang, W.; Doherty, M. Global epidemiology of gout: Prevalence, incidence and risk factors. Nat. Rev. Rheumatol. 2015, 11, 649–662. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, T.; Hori, H.; Umeyama, M.; Shimizu, K. Characteristics of gout patients according to the laterality of nephrolithiasis: A cross-sectional study using helical computed tomography. Int. J. Rheum. Dis. 2019, 22, 567–573. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robert, T. Gout and Other Crystal Arthropathies, 1st ed.; Elsevier Saunders: Philadelphia, PA, USA, 2012. [Google Scholar]
- Singh, J.A.; Edwards, N.L. Gout management and outcomes during the COVID-19 pandemic: A cross-sectional internet survey. Ther. Adv. Musculoskelet. Dis. 2020, 12, 1759720X20966124. [Google Scholar] [CrossRef] [PubMed]
- Padang, C.; Muirden, K.; Schumacher, R.; Darmawan, J.; Nasution, A. Characteristics of chronic gout in Northern Sulawesi, Indonesia. J. Rheumatol. 2006, 33, 1813–1817. [Google Scholar] [PubMed]
- Widyanto, F.W. Arthritis Gout dan Perkembangannya. St. Med. 2017, 10, 145–152. [Google Scholar]
- Badan, P.; dan Pengembangan, K. Hasil Utama Riset Kesehatan Dasar. Kementrian Kesehat. Repub. Indones. 2018, 2013, 1–100. [Google Scholar]
- Darmawan, M.; Valkenburg, W. The epidemiology of rheumatoid arthritis in Indonesia. Br. J. Rheumatol. 1993, 32, 537–540. [Google Scholar] [CrossRef]
- Jaliana, S.; La Ode, M.; Sety. The Related Factors With The Incidence of Uric Acid Among Patients Age 20–44 Years Old In Bahteramas General Hospital of Southest Sulawesi Province in 2017. J. Ilmiah Mhs. Kesehat. Masy. 2018, 3, 1–13. [Google Scholar]
- Hidayat, I.I.; Hamijoyo, L.; Moeliono, M.A. A survey on the clinical diagnosis and management of gout among general practitioners in Bandung. Indones. J. Rheumatol. 2013, 4, 14–19. [Google Scholar]
- Fanning, N.; Merriman, T.R.; Dalbeth, N.; Stamp, L.K. An association of smoking with serum urate and gout: A health paradox. Semin. Arthritis Rheum. 2018, 47, 825–842. [Google Scholar] [CrossRef]
- Dalbeth, N.; Merriman, T.R.; Stamp, L.K. Gout. Lancet 2016, 6736, 1–14. [Google Scholar]
- Aune, D.; Norat, T.; Vatten, L.J. Body mass index and the risk of gout: A systematic review and dose–response meta-analysis of prospective studies. Eur. J. Nutr. 2014, 53, 1591–1601. [Google Scholar] [CrossRef] [PubMed]
- Palmer, T.M.; Nordestgaard, B.G.; Benn, M.; Tybjarg-Hansen, A.; Smith, G.D.; Lawlor, D.A.; Timpson, N.J. Association of plasma uric acid with ischaemic heart disease and blood pressure: Mendelian randomization analysis of two large cohorts. BMJ (Online) 2013, 347, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cavalcanti, N.G.; Diniz, C.; Marques, L.; Ubiratan, T.; Lins, L.; Pereira, M.C.; Jesus, M.; Melo, B.D.; Luzia, A.; Pinto, B.; et al. Cytokine Profile in Gout: Inflammation Driven by Cytokine Pro fi le in Gout: In fl ammation Driven by IL-6 and IL-18. Immunol. Investig. 2016, 139, 383–395. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.; Jiang, X.; Wu, W.; Zhang, D. A meta-analysis of alcohol consumption and the risk of gout. Clin. Rheumatol. 2013, 32, 1641–1648. [Google Scholar] [CrossRef] [PubMed]
- Booranasuksakul, U.; Singhato, A.; Rueangsri, N.; Prasertsri, P. Association between Alcohol Consumption and Body Mass Index in University Students. Asian Pac. Island Nurs. J. 2019, 4, 57–65. [Google Scholar] [CrossRef]
- Hanna, B.E.; Hamed, J.M.; Touhala, L.M. Serum Uric Acid in Smokers. Oman Med. J. 2008, 23, 269–274. [Google Scholar] [PubMed]
- Kim, S.-K.; Choe, J.-Y. Association between smoking and serum uric acid in Korean population. Medicine 2019, 98, e14507. [Google Scholar] [CrossRef]
- Burke, B.T.; Köttgen, A.; Law, A.; Grams, M.; Baer, A.N.; Coresh, J.; McAdams-demarco, M.A. Gout in Older Adults: The Atherosclerosis Risk in Communities Study. J. Gerontol. Med. Sci. 2016, 71, 536–542. [Google Scholar] [CrossRef] [Green Version]
- Kuo, C.F.; Grainge, M.J.; Mallen, C.; Zhang, W.; Doherty, M. Comorbidities in Patients with Gout Prior to and Following Diagnosis: Case-control Study. Ann. Rheum. Dis. 2016, 75, 210–217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsuchiya, M.; Asada, A.; Kasahara, E.; Sato, E.F.; Shindo, M.; Inoue, M. Smoking a single cigarette rapidly reduces combined concentrations of nitrate and nitrite and concentrations of antioxidants in plasma. Circulation 2002, 105, 1155–1157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strauss, J.; Witoelar, F.; Sikoki, B. The Fifth Wave of the Indonesia Family Life Survey: Overview and Field Report; RAND: Santa Monica, CA, USA, 2016; Volume 1. [Google Scholar]
- Gong, M.; Wang, C. Converging Relationships of Obesity and Hyperuricemia with Special Reference to Metabolic Disorders and Plausible Therapeutic Implications. Diabetes Metab. Syndr. Obes. Targets Ther. 2020, 943–962. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liew, H.-P.; Hsu, T.-L. Smoking and Health In Indonesia. Asian Popul. Stud. 2009, 5, 189–209. [Google Scholar] [CrossRef]
- Oberg, M.; Jaakkola, M.S.; Pruss-Ustun, A.; Schweizer, C.; Woodward, A. Second-Hand Smoke: Assessing the Burden of Diseases at National and Local Levels; WHO: Geneva, Switzerland, 2020; Available online: https://www.who.int/quantifying_ehimpacts/publicat (accessed on 25 December 2020).
- Birru, R.L.; Di, Y.P. Pathogenic mechanism of second hand smoke induced inflammation and COPD. Front. Physiol. 2012, 3, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mvalkaonen, M.; Kuusi, T. Vitamin C Prevents the Acute Atherogenic Effect of Passive Smoking. Free Radic. Biol. Med. 2000, 28, 428–436. [Google Scholar] [CrossRef]
- Mvalkaonen, M.; Kuusi, T. Passive Smoking Induces Atherogenic Changes in Low-Density Lipoprotein. Circulation 2016, 2012–2016. [Google Scholar] [CrossRef] [Green Version]
- Jones, M.R.; Magid, H.S.; Al-Rifai, M.; McEvoy, J.W.; Kaufman, J.D.; Hinckley Stukovsky, K.D.; Szklo, M.; Polak, J.; Burke, G.L.; Post, W.S.; et al. Secondhand smoke exposure and subclinical cardiovascular disease: The multi-ethnic study of atherosclerosis. J. Am. Heart Assoc. 2016, 5. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.; Jiang, S.; Watson, R.R. Antioxidant supplementation prevents oxidation and inflammatory responses induced by sidestream cigarette smoke in old mice. Environ. Health Perspect. 2001, 109, 1007–1009. [Google Scholar] [CrossRef] [PubMed]
- Paul, T.W. Effects of diet, physical activity and performance, and body weight on incident gout in ostensibly healthy, vigorously active men. Am. J. Clin. Nutr. 2014, 87, 1480–1487. [Google Scholar]
- Mittal, M.; Siddiqui, M.R.; Tran, K.; Reddy, S.P.; Malik, A.B. Reactive oxygen species in inflammation and tissue injury. Antioxid. Redox Signal. 2014, 20, 1126–1167. [Google Scholar] [CrossRef] [Green Version]
- Startev, V.; Jordanova, M.; Petev, J. Oxidative stress, obesity and chronic inflammation in smokers according to smoking duration and heaviness. Eur. Respir. J. 2011, 38, 55. [Google Scholar]
- Pingmuangkaew, P.; Tangvarasittichai, O. Association of Elevated Serum Uric Acid with the Components of Metabolic Syndrome and Oxidative Stress in Abdominal Obesity Subjects. Indian J. Clin. Biochem. 2015, 30, 286–292. [Google Scholar] [CrossRef] [Green Version]
- Ortega, A.M.; Davies, M.M.; Jarjour, S.; Burnett, R.T.; Mann, J.K.; Hughes, E.; Balmes, J.R.; Turner, M.C.; Jerrett, M. Developing small-area predictions for smoking and obesity prevalence in the United States for use in Environmental Public Health Tracking. Environ. Res. 2014, 134, 435–452. [Google Scholar] [CrossRef]
- Rachmi, C.N.; Li, M.; Baur, L.A. Overweight and obesity in Indonesia: Prevalence and risk factors d a literature review. Public Health 2017, 7, 20–29. [Google Scholar] [CrossRef] [PubMed]
- Kementerian Kesehatan Republik Indonesia. Epidemi Obesitas. 2019; pp. 1–8. Available online: http://p2ptm.kemkes.go.id/uploads/N2VaaXIxZGZwWFpEL1VlRFdQQ3ZRZz09/2018/02/FactSheet_Obesitas_Kit_Informasi_Obesitas.pdf (accessed on 1 January 2020).
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: New York, NY, USA, 1988. [Google Scholar]
- Indonesian Rheumatologist Association. Pedoman Diagnosis dan Pengelolaan Gout Rekomendasi Pedoman Diagnosis dan Pengelolaan Gout Perhimpunan Reumatologi Indonesia; Indonesian Rheumatologist Association: Jakarta, India, 2018; pp. 3–6. [Google Scholar]
- Neogi, T.; Jansen, T.L.T.A.; Dalbeth, N.; Fransen, J.; Schumacher, H.R.; Berendsen, D.; Brown, M.; Choi, H.; Edwards, N.L.; Janssens, H.J.E.M.; et al. 2015 Gout Classification Criteria An American College of Rheumatology/European League Against Rheumatism Collaborative Initiative. Arthritis Rheumatol. 2015, 67, 2557–2568. [Google Scholar] [CrossRef]
- Rias, Y.A.; Gordon, C.J.; Niu, S.F.; Wiratama, B.S.; Chang, C.W.; Tsai, H.T. Secondhand Smoke Correlates with Elevated Neutrophil-Lymphocyte Ratio and Has a Synergistic Effect with Physical Inactivity on Increasing Susceptibility to Type 2 Diabetes Mellitus: A Community-Based Case Control Study. Int. J. Environ. Res. Public Health 2020, 17, 5696. [Google Scholar] [CrossRef]
- Fabre, S.; Clerson, P.; Launay, J.-M.; Gautier, J.-F.; Vidal-Trecan, T.; Riveline, J.-P.; Platt, A.; Abrahamsson, A.; Miner, J.N.; Hughes, G.; et al. Accuracy of the HumaSens(plus) point-of-care uric acid meter using capillary blood obtained by fingertip puncture. Arthritis Res. Ther. 2018, 20, 78. [Google Scholar] [CrossRef] [Green Version]
- Tsai, H.-T.; Tsai, Y.-M.; Yang, S.-F.; Wu, K.-Y.; Chuang, H.-Y. Lifetime cigarette smoke and second-hand smoke and cervical intraepithelial neoplasm—A community-based case–control study. Gynecol. Oncol. 2007, 105, 181–188. [Google Scholar] [CrossRef]
- Zeng, J.; Yang, S.; Wu, L.; Wang, J.; Wang, Y.; Liu, M.; Zhang, D.; Jiang, B.; He, Y. Prevalence of passive smoking in the community population aged 15 years and older in China: A systematic review and meta-analysis. BMJ Open 2016, 6, e009847. [Google Scholar] [CrossRef] [PubMed]
- Naeem, Z. Second-hand smoke-ignored implications. Int. J. Health Sci. 2015, 9, V–VI. [Google Scholar] [CrossRef] [PubMed]
- Couraud, S.; Debieuvre, D.; Moreau, L.; Dumont, P.; Margery, J.; Quoix, E.; Duvert, B.; Cellerin, L.; Baize, N.; Taviot, B.; et al. No impact of passive smoke on the somatic profile of lung cancers in never-smokers. Eur. Respir. J. 2015, 45, 1415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klepeis, N.E.; Ott, W.R.; Switzer, P. Real–Time Measurement of Outdoor Tobacco Smoke Particles. J. Air Waste Manag. Assoc. 2007, 57, 522–534. [Google Scholar] [CrossRef]
- Lee, C.H.; Yang, S.F.; Peng, C.Y.; Li, R.N.; Chen, Y.C.; Chan, T.F.; Tsai, E.M.; Kuo, F.C.; Huang, J.J.; Tsai, H.T.; et al. The precancerous effect of emitted cooking oil fumes on precursor lesions of cervical cancer. Int. J. Cancer 2010, 127, 932–941. [Google Scholar] [CrossRef]
- National Cancer Institute. National Cancer Institute Dictionaries. Available online: https://www.cancer.gov/publications/dictionaries/cancer-terms/def/pack-year (accessed on 26 December 2020).
- Rodrigues, C.F.D.S.; Lima, F.J.C.D.; Barbosa, F.T. Importance of using basic statistics adequately in clinical research. Braz. J. Anesthesiol. (English Edition) 2017, 67, 619–625. [Google Scholar] [CrossRef]
- Knol, M.J.; Tweel, I.V.D.; Grobbee, D.E.; Numans, M.E. Estimating interaction on an additive scale between continuous determinants in a logistic regression model. Int. J. Epidemiol. 2007, 36, 1111–1118. [Google Scholar] [CrossRef]
- Rias, Y.A.; Kurniasari, M.D.; Traynor, V.; Niu, S.F.; Wiratama, B.S.; Chang, C.W.; Tsai, H.T. Synergistic Effect of Low Neutrophil–Lymphocyte Ratio With Physical Activity on Quality of Life in Type 2 Diabetes Mellitus: A Community-Based Study. Biol. Res. Nurs. 2020, 22, 378. [Google Scholar] [CrossRef]
- Sund, M.; Lo, H.; Imhof, A.; Hoffmeister, A.; Koenig, W. Independent association of various smoking characteristics with markers of systemic inflammation in men Results from a representative sample of the general population (MONICA Augsburg Survey 1994/95) Margit Fro. Eur. Heart J. 2003, 24, 1365–1372. [Google Scholar]
- Liu, L.; Lou, S.; Xu, K.; Meng, Z. Relationship between lifestyle choices and hyperuricemia in Chinese men and women. Clin. Rheumatol. 2013, 32, 233–239. [Google Scholar] [CrossRef] [PubMed]
- Poudel, D.R.; Karmacharya, P.; Donato, A. Risk of acute gout among active smokers: Data from nationwide inpatient sample. Clin. Rheumatol. 2016, 35, 3015–3018. [Google Scholar] [CrossRef]
- Richette, P.; Doherty, M.; Pascual, E.; Barskova, V.; Becce, F.; Coy, M.; Guillo, S.; Jansen, T.L.; Janssens, H.; Lioté, F.; et al. 2016 updated EULAR evidence-based recommendations for the management of gout. BMJ 2017, 29–42. [Google Scholar] [CrossRef]
- Teng, G.G.; Pan, A.; Yuan, J.-M.; Koh, W.-P. Cigarette smoking and risk of incident gout in the Singapore Chinese health study. Arthritis Care Res. 2016, 68, 1135. [Google Scholar] [CrossRef] [Green Version]
- Wang, W.; Krishnan, E. Cigarette smoking is associated with a reduction in the risk of incident gout: Results from the Framingham Heart Study original cohort. Rheumatology 2014, 54, 91–95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robinson, P.C.; Taylor, W.J.; Dalbeth, N. An Observational Study of Gout Prevalence and Quality of Care in a National Australian General Practice Population. J. Rheumatol. 2015, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez, G.; Soriano, L.C.; Choi, H.K. Impact of diabetes against the future risk of developing gout. Ann. Rheum. Dis. 2010, 2, 2090–2094. [Google Scholar] [CrossRef] [PubMed]
- Bhat, T.A.; Kalathil, S.G.; Bogner, P.N.; Lehmann, P.V.; Thatcher, T.H.; Richard, P.; Sime, P.J.; Thanavala, Y. Secondhand Smoke Induces Inflammation and Impairs Immunity to Respiratory Infections. J. Immunol. 2019, 200, 2927–2940. [Google Scholar] [CrossRef] [PubMed]
- Sears, B.; Walker, J.C.; Al, S.E.T. Environmental Tobacco Smoke: Current Assessment and Future Directions. Toxicol. Pathol. 1992, 20, 289–305. [Google Scholar]
- Vargas-Santo, A.B.; Neogi, T. Management of Gout and Hyperuricemia in CKD. Am. J. Kidney Dis. 2018, 70, 422–439. [Google Scholar] [CrossRef] [PubMed]
- Guthikonda, S.; Sinkey, C.; Barenz, T.; Haynes, W.G. Xanthine oxidase inhibition reverses endothelial dysfunction in heavy smokers. Circulation 2003, 107, 416–421. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Becker, M.A. Inflammation: A possible mechanism for a causative role of hyperuricemia/gout in cardiovascular disease Brief review Inflammation: A possible mechanism for a causative role of hyperuricemia/gout in cardiovascular disease. Curr. Med. Res. Opin. 2015, 7995, 9.14–19.14. [Google Scholar]
- Robinson, P.C.; Kempe, S.; Tebbutt, I.; Roberts, L. Epidemiology of inpatient gout in Australia and New Zealand: Temporal trends, comorbidities and gout flare site. Int. J. Rheum. Dis. 2017, 20, 779–784. [Google Scholar] [CrossRef] [PubMed]
- Mostafa, R.M. Dilemma of women’s passive smoking. Ann. Thorac. Med. 2011, 6, 55–57. [Google Scholar] [CrossRef] [PubMed]
- Saag, K.G.; Choi, H. Epidemiology, risk factors, and lifestyle modifications for gout. Arthritis Res. Ther. 2006, 8, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Jacob, L.; Freyn, M.; Kalder, M.; Dinas, K.; Kostev, K. Impact of tobacco smoking on the risk of developing 25 different cancers in the UK: A retrospective study of 422,010 patients followed for up to 30 years. Oncotarget 2018, 9, 17420–17429. [Google Scholar] [CrossRef] [Green Version]
- Lakier, J.B. Smoking and cardiovascular disease. Am. J. Med. 1992, 93, 8s–12s. [Google Scholar] [CrossRef]
- Gallucci, G.; Tartarone, A.; Lerose, R.; Lalinga, A.V.; Capobianco, A.M. Cardiovascular risk of smoking and benefits of smoking cessation. J. Thorac. Dis. 2020, 12, 3866–3876. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | Healthy Control Group n (%) | Gout Group n (%) | p Value |
|---|---|---|---|
| Gender | <0.05 | ||
| Female | 212 (69.70%) | 47 (58%) | |
| Male | 92 (30.30%) | 34 (42%) | |
| Marital status | |||
| Unmarried | 70 (23%) | 15 (18.50%) | 0.38 |
| Married | 234 (77%) | 66 (81.50%) | |
| Educational level | |||
| College | 61 (20%) | 13 (16%) | <0.05 |
| Senior high school | 144 (47.40%) | 27 (33.30%) | |
| Junior high school or below | 99 (32.60%) | 41 (50.70%) | |
| Monthly income | |||
| >US$214 | 40 (13.10%) | 12 (14.80%) | 0.68 |
| US$128~214 | 68 (22.40%) | 21 (25.90%) | |
| <US$128 | 196 (64.50%) | 48 (59.30%) | |
| Occupational status | 0.35 | ||
| Employed | 151 (49.70%) | 45 (55.60%) | |
| Unemployed | 153 (50.30%) | 36 (44.40%) | |
| Age (years) | <0.05 | ||
| ≤47 | 164 (53.90%) | 34 (42%) | |
| >47 | 140 (46.10%) | 47 (58%) | |
| Uric acid level (mg/dL) | <0.01 | ||
| ≤5.7 | 195 (64.10%) | 2 (2.50%) | |
| >5.7 | 109 (35.90%) | 79 (97.50%) | |
| Systolic blood pressure (mmHg) | |||
| ≤131 | 162 (53.30%) | 31 (38.30%) | <0.05 |
| >131 | 142 (46.70%) | 50 (61.70%) | |
| Diastolic blood pressure (mmHg) | |||
| ≤80 | 152 (50%) | 44 (54.30%) | 0.48 |
| >80 | 152 (50%) | 37 (45.70%) | |
| BMI (kg/m2) | <0.05 | ||
| ≤24.9 | 151 (49.70%) | 22 (27.20%) | |
| >24.9 | 153 (50.30%) | 59 (72.80%) | |
| Alcohol Consumption | 0.001 | ||
| Non-drinker | 253 (65.70%) | 52 (13.50%) | |
| Drinker | 51 (13.20%) | 29 (7.50%) |
| Characteristics | Healthy Control Group n (%) | Gout Group n (%) | p Value |
|---|---|---|---|
| Smoking status | 304 (100%) | 81 (100%) | |
| Non-smoker | 212 (69.70%) | 22 (27.20%) | <0.01 |
| Exposed to SHS | 47 (15.50%) | 35 (43.20%) | |
| Active smoker | 45 (14.80%) | 24 (29.60%) | |
| No. of cigarettes consumed per day by an active smoker (pcs) | 257 (100%) | 46 (100%) | |
| 0 | 212 (82.50%) | 22 (47.80%) | <0.01 |
| >0~≤16 | 25 (9.70%) | 13 (28.30%) | |
| >16 | 20 (7.80%) | 11 (23.90%) | |
| Duration active smoker (years) | 257 (100%) | 46 (100%) | |
| 0 | 212 (82.50%) | 22 (47.80%) | |
| >0~≤23 | 24 (9.30%) | 11 (23.90%) | <0.01 |
| >23 | 21 (8.20%) | 13 (28.30%) | |
| Pack-year of active smoker | 257 (100%) | 46 (100%) | |
| 0 | 212 (82.50%) | 22 (47.80%) | |
| >0~<20 | 28 (10.90%) | 10 (21.70%) | <0.01 |
| >20 | 17 (6.60%) | 14 (30.50%) | |
| No. of cigarettes per day generating SHS exposure (pcs) | 259 (100%) | 57 (100%) | |
| 0 | 212 (81.8%) | 22 (38.6%) | <0.01 |
| >0~≤20 | 38 (14.7%) | 24 (42.1%) | |
| >20 | 9 (3.5%) | 11 (19.3%) | |
| Duration of exposure to SHS (years) | 259 (100%) | 57 (100%) | |
| 0 | 212 (81.8%) | 22 (38.6%) | |
| >0~≤31.50 | 30 (11.6%) | 11 (19.3%) | <0.01 |
| >31.50 | 17 (6.6%) | 24 (42.1%) | |
| Pack-year of SHS exposure | 259 (100%) | 57 (100%) | |
| 0 | 212 (81.90%) | 22 (38.60%) | |
| >0~≤26.5 | 31 (12.00%) | 10 (17.5%) | <0.01 |
| >26.5 | 16 (6.10%) | 25 (43.9%) |
| Characteristic | Healthy Control Group n (%) | Gout Group n (%) | OR (95% CI) | AOR (95% CI) |
|---|---|---|---|---|
| Smoking status | 304 (100%) | 81 (100%) | ||
| Non-smoker | 212 (69.70%) | 22 (27.20%) | 1.00 | 1.00 |
| Exposed to SHS | 47 (15.50%) | 35 (43.20%) | 7.17 (3.86~13.33) ** | 4.67 (2.18~10.00) ** |
| Active smoker | 45 (14.80%) | 24 (29.60%) | 5.13 (2.65~9.96) ** | 3.26 (1.07~9.90) * |
| Duration as active smoker (years) | 257 (100%) | 46 (100%) | ||
| 0 | 212 (82.50%) | 22 (47.80%) | 1.00 | 1.00 |
| >0~≤23 | 24 (9.30%) | 11 (23.90%) | 2.93 (1.13~7.60) * | 2.34 (0.46~11.98) |
| >23 | 21 (8.20%) | 13 (28.30%) | 7.45 (3.45~16.08) ** | 5.95 (1.41~25.03) * |
| No. of cigarettes consumed per day by an active smoker | 257 (100%) | 46 (100%) | ||
| 0 | 212 (82.50%) | 22 (47.80%) | 1.00 | 1.00 |
| >0~≤16 | 25 (9.70%) | 13 (28.30%) | 2.83 (0.95~8.42) | 2.50 (0.45~13.96) |
| >16 | 20 (7.80%) | 11 (23.90%) | 6.54 (3.15~13.56) ** | 5.15 (1.28~20.63) * |
| Pack~year of active smoker | 257 (100%) | 46 (100%) | ||
| 0 | 212 (82.50%) | 22 (47.80%) | 1.00 | 1.00 |
| >0~<20 | 28 (10.90%) | 10 (21.70%) | 3.44 (1.47~8.01) ** | 2.94 (0.68~12.76) |
| >20 | 17 (6.60%) | 14 (30.50%) | 7.93 (3.45~18.24) ** | 7.18 (1.53~33.67) * |
| Duration of exposure to SHS (years) | 259 (100%) | 57 (100%) | ||
| 0 | 212 (81.80%) | 22 (38.60%) | 1.00 | 1.00 |
| >0~≤31.5 | 30 (11.60%) | 11 (19.30%) | 3.53 (1.55~8.01) ** | 2.11 (0.79~5.66) |
| >31.5 | 17 (6.60%) | 24 (42.10%) | 13.60 (6.35~29.11) ** | 10.12 (3.51~29.14) ** |
| No. of cigarettes per day generating SHS exposure | 259 (100%) | 57 (100%) | ||
| 0 | 212 (81.08%) | 22 (38.60%) | 1.00 | 1.00 |
| >0~≤20 | 38 (14.70%) | 24 (42.10%) | 6.08 (3.10~11.95) ** | 4.53 (1.89~10.84) ** |
| >20 | 9 (3.50%) | 11 (19.30%) | 11.77 (4.40~31.51) ** | 4.37 (1.33~14.28) ** |
| Pack-year of SHS exposure | 259 (100%) | 57 (100%) | ||
| 0 | 212 (81.90%) | 22 (38.60%) | 1.00 | 1.00 |
| >0~≤26.5 | 31 (12.00%) | 10 (17.5%) | 3.10 (1.34~7.18) ** | 1.66 (0.58~4.72) |
| >26.5 | 16 (6.10%) | 25 (43.9%) | 15.06 (7.00~32.38) | 9.95 (3.64~27.22) ** |
| Characteristics | Healthy Control Group (n = 304) (%) | Gout Group (n = 81) (%) | OR (95% CI) | AOR (95% CI) |
|---|---|---|---|---|
| BMI ≤24.9 kg/m2 and non-smoker | 106 (34.90%) | 6 (7.40%) | 1.00 | 1.00 |
| BMI ≤24.9 kg/m2 and smoker (active smoker and exposed to SHS) | 45 (14.80%) | 16 (19.80%) | 6.28 (2.31~17.09) ** | 3.18 (1.01~9.97) * |
| BMI >24.9 kg/m2 and non-smoker | 106 (34.90%) | 16 (19.80%) | 2.67 (1.01~7.08) * | 1.94 (0.66~5.64) |
| BMI >24.9 kg/m2 and smoker (active smoker and exposed to SHS) | 47 (15.40%) | 43 (53.10%) | 16.16 (6.43~40.58) ** | 9.65 (3.25~28.65) ** |
| Characteristic | Norm Uricemia (<6 mg/dL) n (%) | Hyperuricemia (>6 mg/dL) n (%) | OR (95% CI) | AOR (95% CI) |
|---|---|---|---|---|
| Smoking status | 227 (100%) | 154 (100%) | ||
| Non-smoker | 163 (71.8%) | 69 (44.8%) | 1.00 | 1.00 |
| Exposed to SHS | 32 (14.1%) | 49 (31.8%) | 3.58 (2.12~6.05) ** | 3.37 (1.93~5.89) ** |
| Active smoker | 32 (14.1%) | 36 (23.4%) | 2.65 (1.53~4.59) ** | 1.39 (0.63~3.07) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kurniasari, M.D.; Karwur, F.F.; Rayanti, R.E.; Dharmana, E.; Rias, Y.A.; Chou, K.R.; Tsai, H.-T. Second-Hand Smoke and Its Synergistic Effect with a Body-Mass Index of >24.9 kg/m2 Increase the Risk of Gout Arthritis in Indonesia. Int. J. Environ. Res. Public Health 2021, 18, 4324. https://doi.org/10.3390/ijerph18084324
Kurniasari MD, Karwur FF, Rayanti RE, Dharmana E, Rias YA, Chou KR, Tsai H-T. Second-Hand Smoke and Its Synergistic Effect with a Body-Mass Index of >24.9 kg/m2 Increase the Risk of Gout Arthritis in Indonesia. International Journal of Environmental Research and Public Health. 2021; 18(8):4324. https://doi.org/10.3390/ijerph18084324
Chicago/Turabian StyleKurniasari, Maria Dyah, Ferry Fredy Karwur, Rosiana Eva Rayanti, Edi Dharmana, Yohanes Andy Rias, Kuei Ru Chou, and Hsiu-Ting Tsai. 2021. "Second-Hand Smoke and Its Synergistic Effect with a Body-Mass Index of >24.9 kg/m2 Increase the Risk of Gout Arthritis in Indonesia" International Journal of Environmental Research and Public Health 18, no. 8: 4324. https://doi.org/10.3390/ijerph18084324
APA StyleKurniasari, M. D., Karwur, F. F., Rayanti, R. E., Dharmana, E., Rias, Y. A., Chou, K. R., & Tsai, H. -T. (2021). Second-Hand Smoke and Its Synergistic Effect with a Body-Mass Index of >24.9 kg/m2 Increase the Risk of Gout Arthritis in Indonesia. International Journal of Environmental Research and Public Health, 18(8), 4324. https://doi.org/10.3390/ijerph18084324