
Do Physical Activity, BMI, and Wellbeing Affect Logical Thinking?


 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedure
2.3. Measurements
2.4. Statistical Analysis
3. Results
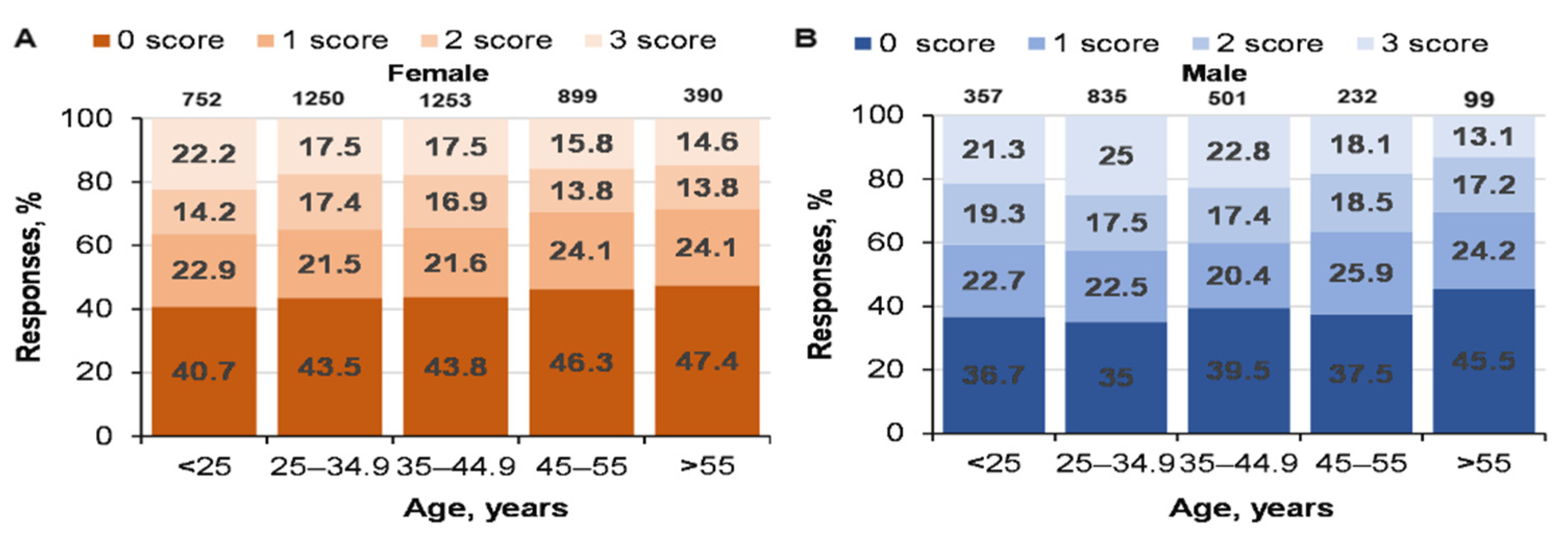
3.1. Effect of Age and Gender on CRT Scores
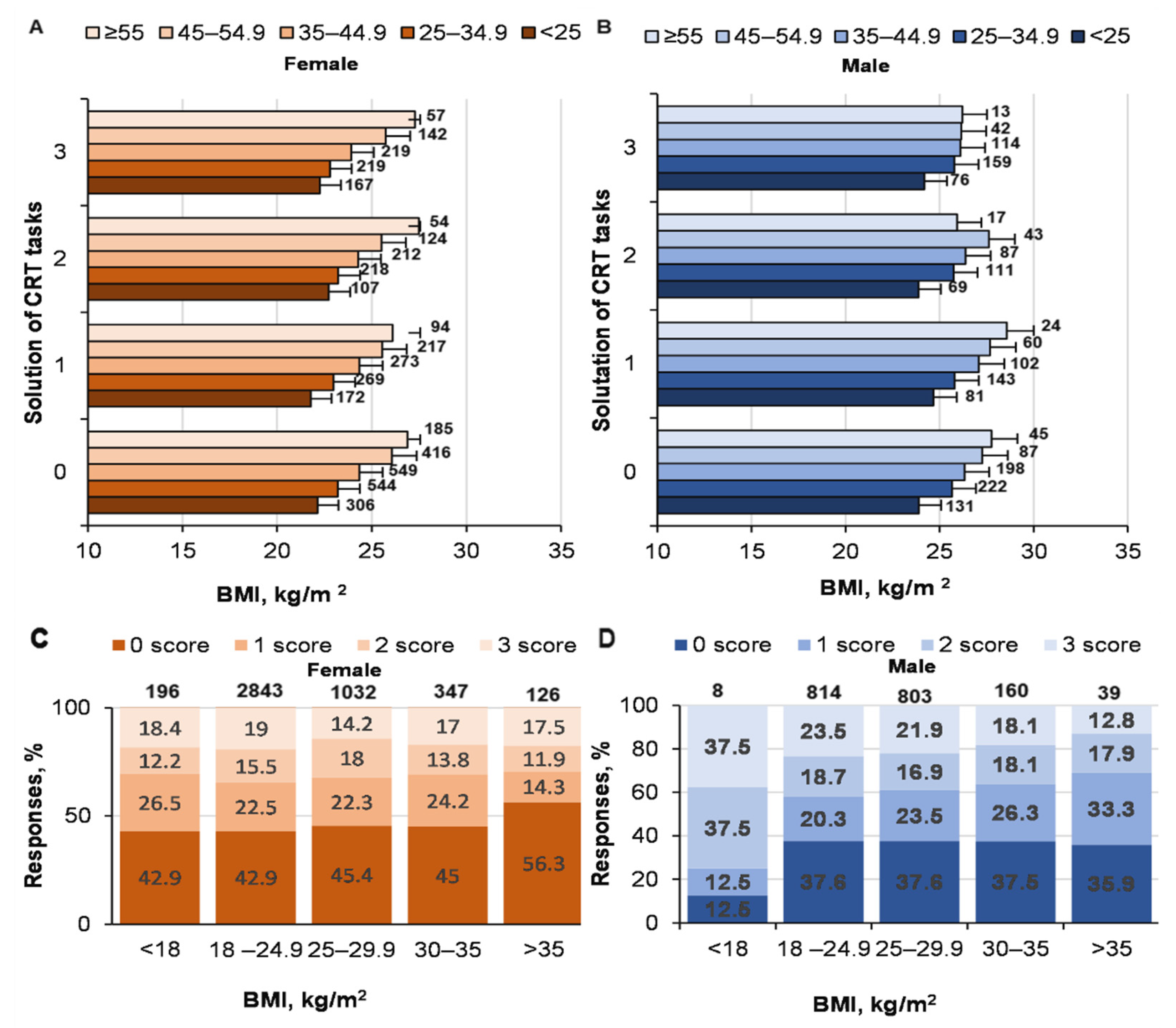
3.2. Relationship between BMI and CRT Results
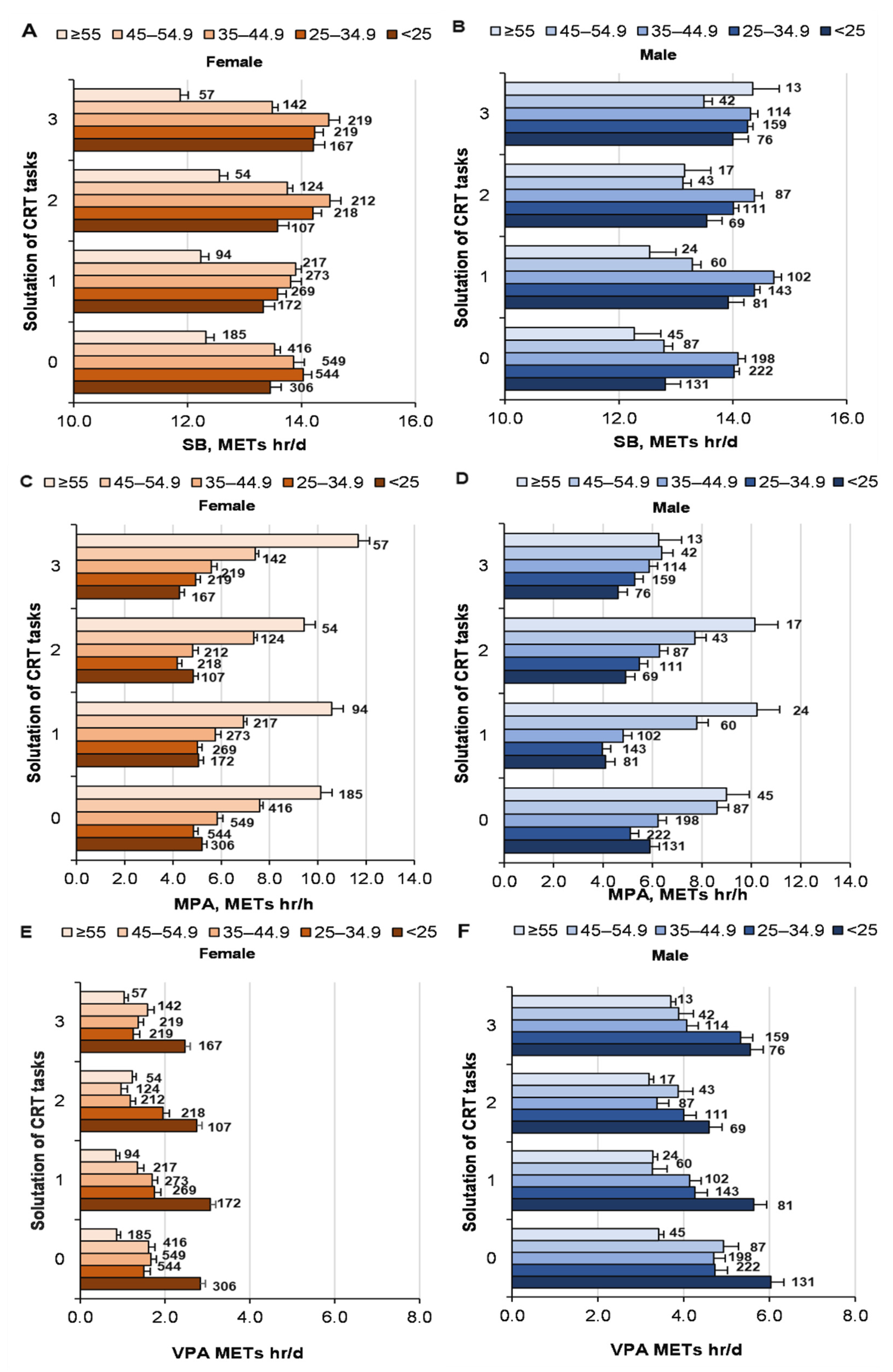
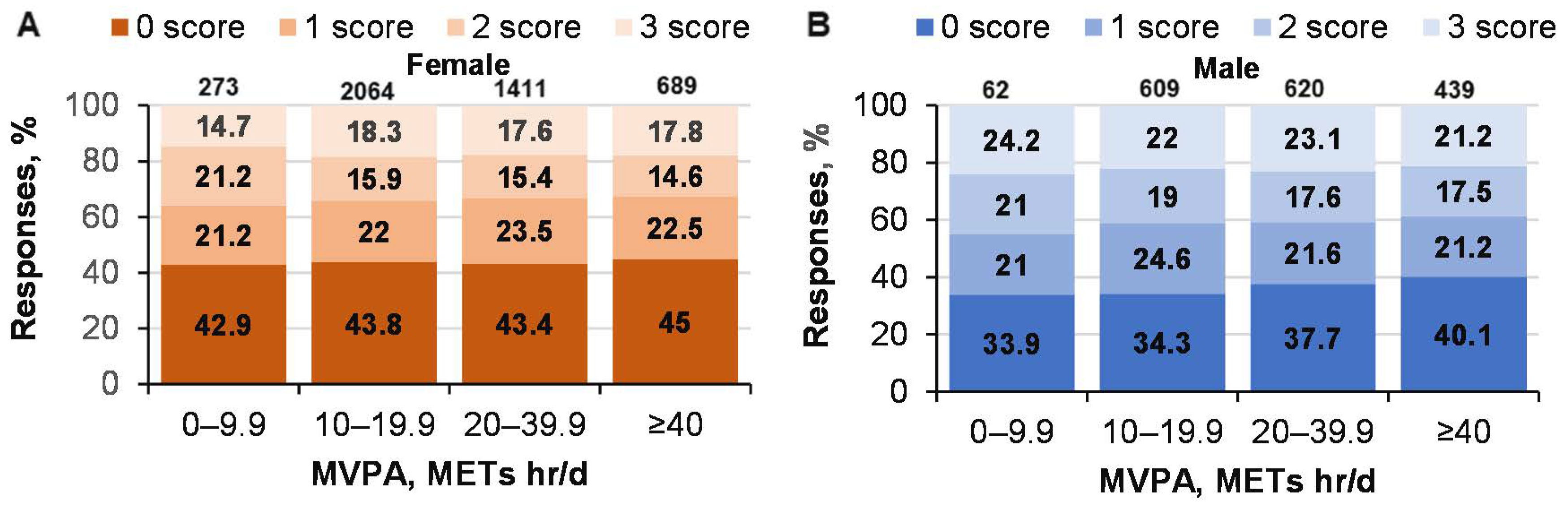
3.3. Relationship between PA and CRT Results
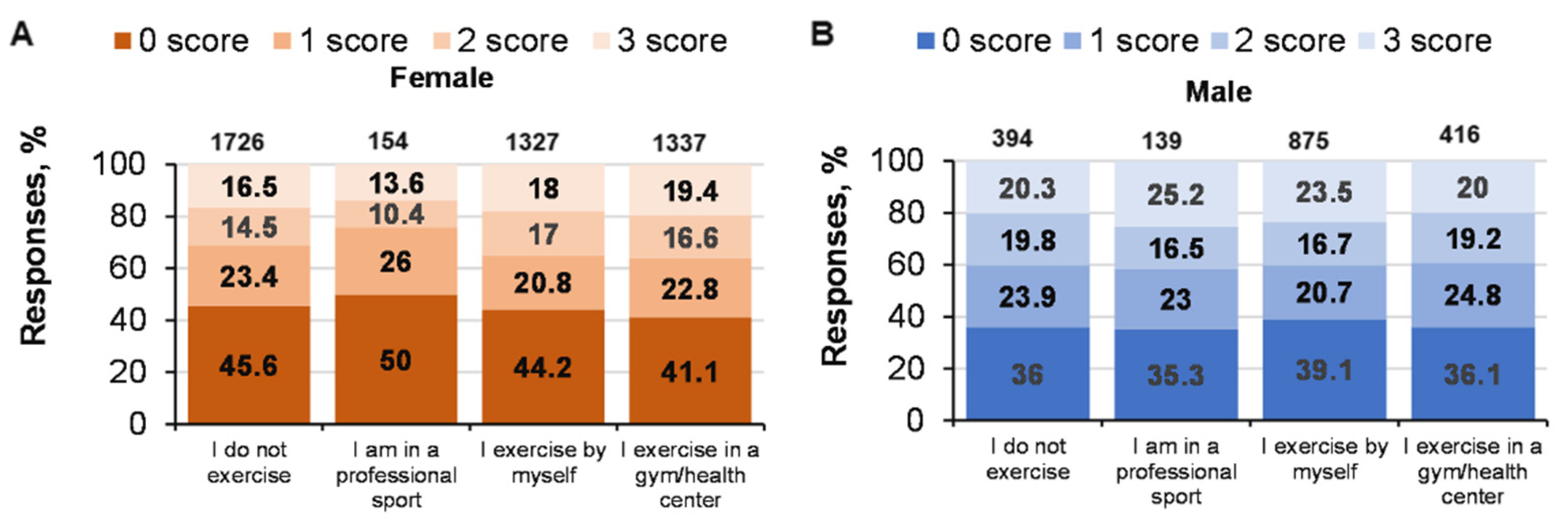
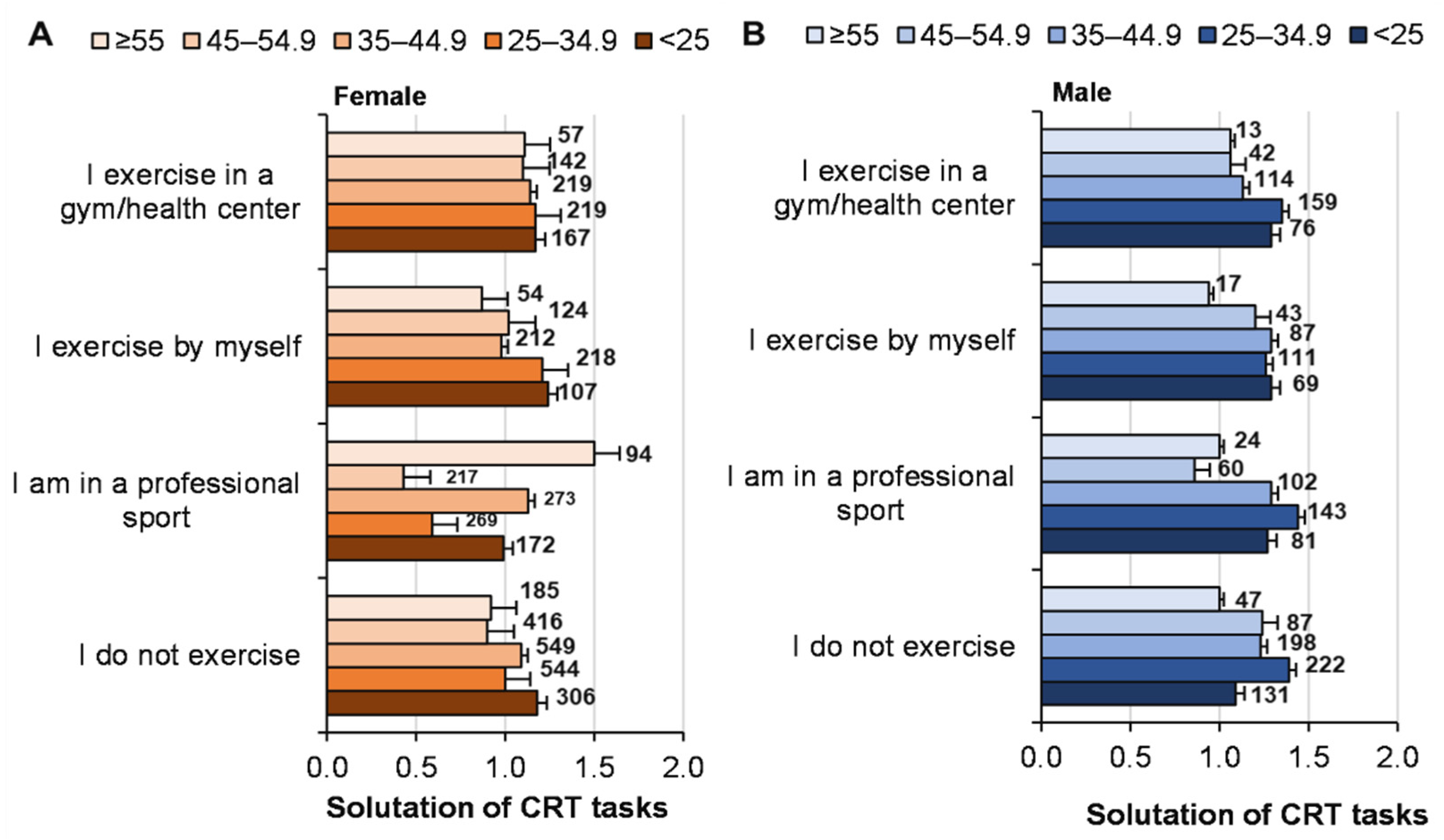
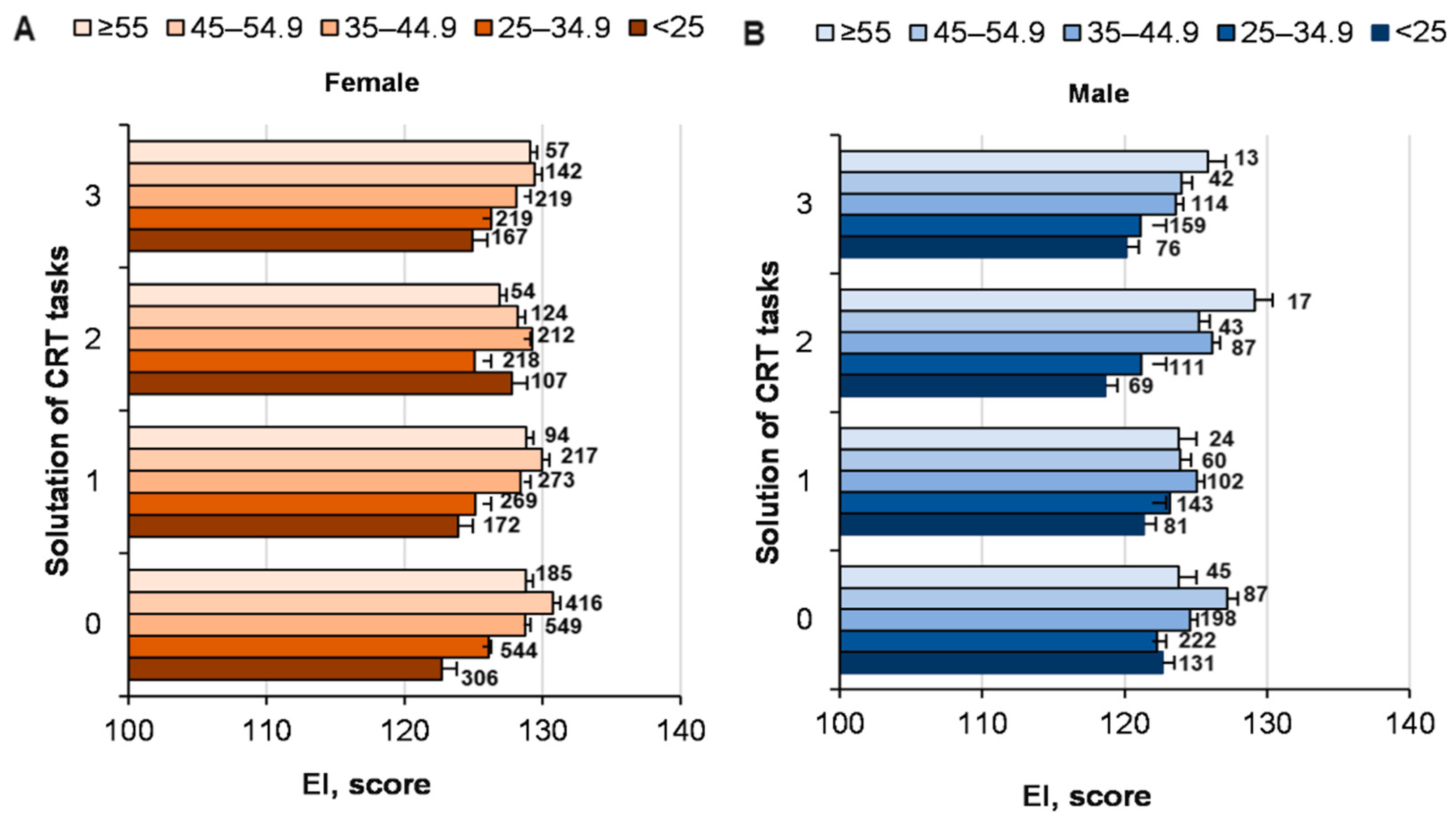
3.4. Relationship between Sports-Specific Activities and CRT Results
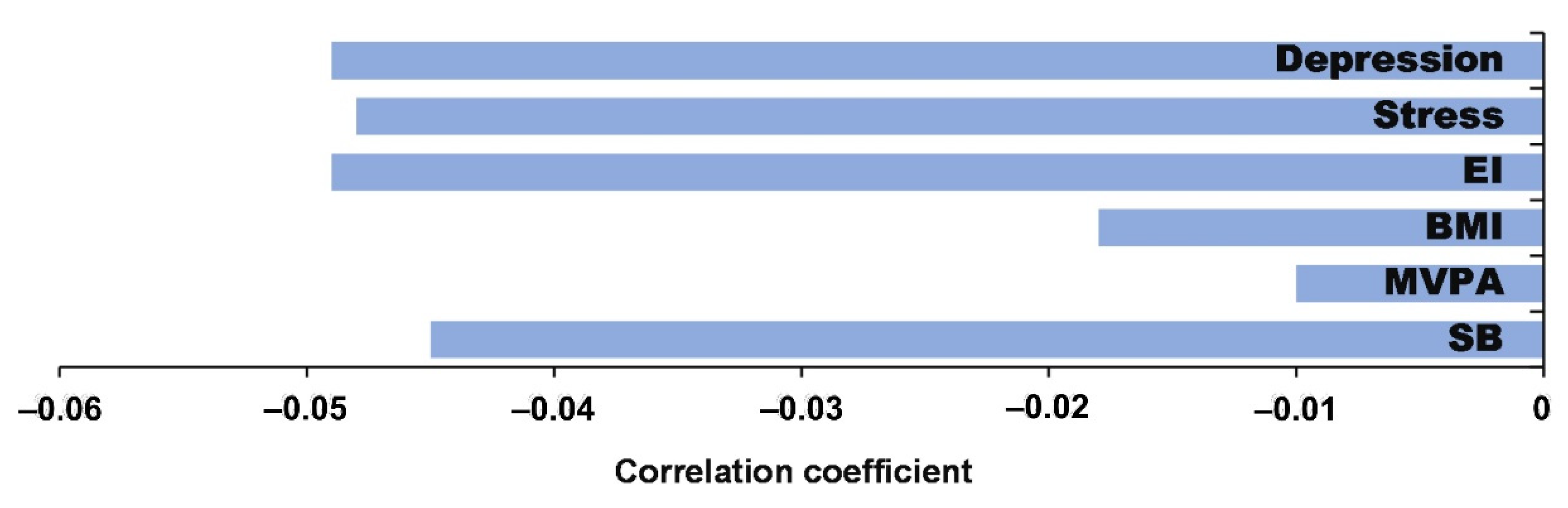
3.5. Effectiveness of Solving CRT Tasks with Sociodemographic Factors and Healthy Lifestyle Factors
4. Discussion
5. Limitations and Directions for Future Research
6. Practical Implications of the Study
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pedersen, B.K.; Saltin, B. Exercise as medicine—Evidence for prescribing exercise as therapy in 26 different chronic diseases. Scand. J. Med. Sci. Sports 2015, 25, 1–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on physical activity and sedentary behavior. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef] [PubMed]
- Tomporowski, P.D.; Davis, C.L.; Miller, P.H.; Naglieri, J.A. Exercise and children’s intelligence, cognition, and academic achievement. Educ. Psychol. Rev. 2008, 20, 111–131. [Google Scholar] [CrossRef] [PubMed]
- Laborde, S.; Dosseville, F.; Allen, M.S. Emotional intelligence in sport and exercise: A systematic review. Scand. J. Med. Sci. Sports 2016, 26, 862–874. [Google Scholar] [CrossRef] [PubMed]
- Watson, A.; Timperio, A.; Brown, H.; Best, K.; Hesketh, K.D. Effect of classroom-based physical activity interventions on academic and physical activity outcomes: A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 114. [Google Scholar] [CrossRef] [Green Version]
- Erickson, K.I.; Hillman, C.; Stillman, C.M.; Ballard, R.M.; Bloodgood, B.; Conroy, D.E.; Macko, R.; Marquez, D.X.; Petruzzello, S.J.; Powell, K.E. Physical activity, cognition, and brain outcomes: A review of the 2018 physical activity guidelines. Med. Sci. Sports Exerc. 2019, 51, 1242. [Google Scholar] [CrossRef]
- Zlibinaite, L.; Skurvydas, A.; Kilikeviciene, S.; Solianik, R. Two Months of Using Global Recommendations for Physical Activity Had No Impact on Cognitive or Motor Functions in Overweight and Obese Middle-Aged Women. J. Phys. Act. Health 2020, 18, 52–60. [Google Scholar] [CrossRef]
- Žlibinaitė, L.; Solianik, R.; Vizbaraitė, D.; Mickevičienė, D.; Skurvydas, A. The effect of combined aerobic exercise and calorie restriction on mood, cognition, and motor behavior in overweight and obese women. J. Phys. Act. Health 2020, 17, 204–210. [Google Scholar] [CrossRef]
- Skurvydas, A.; Lisinskiene, A.; Lochbaum, M.; Majauskiene, D.; Valanciene, D.; Dadeliene, R.; Fatkulina, N.; Sarkauskiene, A. Physical activity, stress, depression, emotional intelligence, logical thinking, and overall health in a large Lithuanian from October 2019 to June 2020: Age and gender differences adult sample. Int. J. Environ. Res. Public Health 2021, 18, 12809. [Google Scholar] [CrossRef]
- Bennie, J.A.; De Cocker, K.; Teychenne, M.J.; Brown, W.J.; Biddle, S.J. The epidemiology of aerobic physical activity and muscle-strengthening activity guideline adherence among 383,928 US adults. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 34. [Google Scholar] [CrossRef] [Green Version]
- Ekelund, U.; Tarp, J.; Steene-Johannessen, J.; Hansen, B.H.; Jefferis, B.; Fagerland, M.W.; Whincup, P.; Diaz, K.M.; Hooker, S.P.; Chernofsky, A.; et al. Dose-response associations between accelerometry measured physical activity and sedentary time and all cause mortality: Systematic review and harmonised meta-analysis. BMJ 2019, 366, l4570. [Google Scholar] [CrossRef] [Green Version]
- Pedersen, B.K. The physiology of optimizing health with a focus on exercise as medicine. Annu. Rev. Physiol. 2019, 81, 607–627. [Google Scholar] [CrossRef] [PubMed]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Worldwide trends in insufficient physical activity from 2001 to 2016: A pooled analysis of 358 population-based surveys with 19 million participants. Lancet Glob. Health 2018, 6, e1077–e1086. [Google Scholar] [CrossRef] [Green Version]
- Matikainen-Ankney, B.A.; Kravitz, A.V. Persistent effects of obesity: A neuroplasticity hypothesis. Ann. N. Y. Acad. Sci. 2018, 1428, 221. [Google Scholar] [CrossRef] [PubMed]
- Saruco, E.; Pleger, B. A Systematic Review of Obesity and Binge Eating Associated Impairment of the Cognitive Inhibition System. Front. Nutr. 2021, 8, 609012. [Google Scholar] [CrossRef]
- Skurvydas, A.; Lisinskiene, A.; Lochbaum, M.; Majauskiene, D.; Valanciene, D.; Dadeliene, R.; Fatkulina, N.; Sarkauskiene, A. Did COVID-19 pandemic change people’s physical activity distribution, eating, and alcohol consumption habits as well as body mass index? Int. J. Environ. Res. Public Health 2021, 18, 12405. [Google Scholar] [CrossRef]
- Elias, M.F.; Elias, P.K.; Sullivan, L.M.; Wolf, P.A.; D’agostino, R.B. Lower cognitive function in the presence of obesity and hypertension: The Framingham heart study. Int. J. Obes. 2003, 27, 260–268. [Google Scholar] [CrossRef] [Green Version]
- Kivipelto, M.; Mangialasche, F.; Ngandu, T. Lifestyle interventions to prevent cognitive impairment, dementia and Alzheimer disease. Nat. Rev. Neurol. 2018, 14, 653–666. [Google Scholar] [CrossRef] [PubMed]
- Foldi, C.J.; Morris, M.J.; Oldfield, B.J. Executive function in obesity and anorexia nervosa: Opposite ends of a spectrum of disordered feeding behaviour? Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2021, 111, 110395. [Google Scholar] [CrossRef]
- Erickson, K.I.; Voss, M.W.; Prakash, R.S.; Basak, C.; Szabo, A.; Chaddock, L.; Kim, J.S.; Heo, S.; Alves, H.; White, S.M.; et al. Exercise training increases size of hippocampus and improves memory. Proc. Natl. Acad. Sci. USA 2011, 108, 3017–3022. [Google Scholar] [CrossRef] [Green Version]
- Najar, J.; Östling, S.; Gudmundsson, P.; Sundh, V.; Johansson, L.; Kern, S.; Guo, X.; Hällström, T.; Skoog, I. Cognitive and physical activity and dementia: A 44-year longitudinal population study of women. Neurology 2019, 92, e1322–e1330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Čekanauskaitė, A.; Skurvydas, A.; Žlibinaitė, L.; Mickevičienė, D.; Kilikevičienė, S.; Solianik, R. A 10-week yoga practice has no effect on cognition, but improves balance and motor learning by attenuating brain-derived neurotrophic factor levels in older adults. Exp. Gerontol. 2020, 138, 110998. [Google Scholar] [CrossRef] [PubMed]
- Brown, B.M.; Frost, N.; Rainey-Smith, S.R.; Doecke, J.; Markovic, S.; Gordon, N.; Weinborn, M.; Sohrabi, H.R.; Laws, S.M.; Martins, R.N.; et al. High-intensity exercise and cognitive function in cognitively normal older adults: A pilot randomised clinical trial. Alzheimer’s Res. Ther. 2021, 13, 33. [Google Scholar] [CrossRef] [PubMed]
- Smith, E.; Hay, P.; Campbell, L.; Trollor, J.N. A review of the association between obesity and cognitive function across the lifespan: Implications for novel approaches to prevention and treatment. Obes. Rev. 2011, 12, 740–755. [Google Scholar] [CrossRef]
- Anstey, K.J.; Cherbuin, N.; Budge, M.; Young, J. Body mass index in midlife and late-life as a risk factor for dementia: A meta-analysis of prospective studies. Obes. Rev. 2011, 12, e426–e437. [Google Scholar] [CrossRef]
- Kelly, S.J.; Daniel, M.; Dal Grande, E.; Taylor, A. Mental ill-health across the continuum of body mass index. BMC Public Health 2011, 11, 765. [Google Scholar] [CrossRef] [Green Version]
- Mumford, E.A.; Liu, W.; Hair, E.C.; Yu, T.C. Concurrent trajectories of BMI and mental health patterns in emerging adulthood. Soc. Sci. Med. 2013, 98, 1–7. [Google Scholar] [CrossRef]
- Tanaka, H.; Gourley, D.D.; Dekhtyar, M.; Haley, A.P. Cognition, brain structure, and brain function in individuals with obesity and related disorders. Curr. Obes. Rep. 2020, 9, 544–549. [Google Scholar] [CrossRef]
- Morys, F.; Dadar, M.; Dagher, A. Association between mid-life obesity, its metabolic consequences, cerebrovascular disease and cognitive decline. J. Clin. Endocrinol. Metab. 2021, 106, e4260–e4274. [Google Scholar] [CrossRef]
- Balasubramanian, P.; Kiss, T.; Tarantini, S.; Nyúl-Tóth, Á.; Ahire, C.; Yabluchanskiy, A.; Csipo, T.; Lipecz, A.; Tabak, A.; Institoris, A.; et al. Obesity-induced cognitive impairment in older adults: A microvascular perspective. Am. J. Physiol. Heart Circ. Physiol. 2021, 320, H740–H761. [Google Scholar] [CrossRef]
- Sui, S.X.; Williams, L.J.; Holloway-Kew, K.L.; Hyde, N.K.; Pasco, J.A. Skeletal muscle health and cognitive function: A narrative review. Int. J. Mol. Sci. 2020, 22, 255. [Google Scholar] [CrossRef] [PubMed]
- Gunstad, J.; Lhotsky, A.; Wendell, C.R.; Ferrucci, L.; Zonderman, A.B. Longitudinal examination of obesity and cognitive function: Results from the Baltimore longitudinal study of aging. Neuroepidemiology 2010, 34, 222–229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prickett, C.; Brennan, L.; Stolwyk, R. Examining the relationship between obesity and cognitive function: A systematic literature review. Obes. Res. Clin. Pract. 2015, 9, 93–113. [Google Scholar] [CrossRef] [PubMed]
- Horowitz, A.M.; Fan, X.; Bieri, G.; Smith, L.K.; Sanchez-Diaz, C.I.; Schroer, A.B.; Gontier, G.; Casaletto, K.B.; Kramer, J.H.; Williams, K.E.; et al. Blood factors transfer beneficial effects of exercise on neurogenesis and cognition to the aged brain. Science 2020, 369, 167–173. [Google Scholar] [CrossRef]
- Blondell, S.J.; Hammersley-Mather, R.; Veerman, J.L. Does physical activity prevent cognitive decline and dementia? A systematic review and meta-analysis of longitudinal studies. BMC Public Health 2014, 14, 510. [Google Scholar] [CrossRef] [Green Version]
- Pesta, B.J.; Bertsch, S.; McDaniel, M.A.; Mahoney, C.B.; Poznanski, P.J. Differential epidemiology: IQ, neuroticism, and chronic disease by the 50 US states. Intelligence 2012, 40, 107–114. [Google Scholar] [CrossRef] [Green Version]
- Wraw, C.; Der, G.; Gale, C.R.; Deary, I.J. Intelligence in youth and health behaviours in middle age. Intelligence 2018, 69, 71–86. [Google Scholar] [CrossRef]
- Meincke, R.H.; Hansen, Å.M.; Mortensen, L.H.; Osler, M.; Mortensen, E.L. Intelligence in early adulthood and midlife physical performance in men: The mediating roles of education and physical activity. Intelligence 2016, 58, 62–68. [Google Scholar] [CrossRef]
- Kahneman, D.; Frederick, S. Representativeness revisited: Attribute substitution in intuitive judgment. In Heuristics and Biases: The Psychology of Intuitive Judgment; Gilovich, T., Griffin, D., Kahneman, D., Eds.; Cambridge University Press: Cambridge, UK, 2002; pp. 49–81. [Google Scholar]
- Evans, J.S.B. Dual-processing accounts of reasoning, judgment, and social cognition. Annu. Rev. Psychol. 2008, 59, 255–278. [Google Scholar] [CrossRef] [Green Version]
- Sheeran, P.; Gollwitzer, P.M.; Bargh, J.A. Nonconscious processes and health. Health Psychol. 2013, 32, 460–473. [Google Scholar] [CrossRef]
- Maxwell, A.L.; Gardiner, E.; Loxton, N.J. Investigating the relationship between reward sensitivity, impulsivity, and food addiction: A systematic review. Eur. Eat. Disord. Rev. 2020, 28, 368–384. [Google Scholar] [CrossRef] [PubMed]
- Daugherty, A.M.; Zwilling, C.; Paul, E.J.; Sherepa, N.; Allen, C.; Kramer, A.F.; Hillmanc, C.H.; Cohen, N.J.; Barbey, A.K. Multi-modal fitness and cognitive training to enhance fluid intelligence. Intelligence 2018, 66, 32–43. [Google Scholar] [CrossRef]
- Frederick, S. Cognitive reflection and decision making. J. Econ. Perspect. 2005, 19, 25–42. [Google Scholar] [CrossRef] [Green Version]
- Toplak, M.E.; West, R.F.; Stanovich, K.E. The Cognitive Reflection Test as a predictor of performance on heuristics-and-biases tasks. Mem. Cogn. 2011, 39, 1275–1289. [Google Scholar] [CrossRef] [PubMed]
- Kahan, D.M. Ideology, motivated reasoning, and cognitive reflection: An experimental study. Judgm. Decis. Mak. 2012, 8, 407–424. [Google Scholar] [CrossRef]
- Pennycook, G.; Cheyne, J.A.; Koehler, D.J.; Fugelsang, J.A. Is the cognitive reflection test a measure of both reflection and intuition? Behav. Res. Methods 2016, 48, 341–348. [Google Scholar] [CrossRef]
- Baugh, C.M.; Gedlaman, M.A.; Daneshvar, D.H.; Kroshus, E. Factors Influencing College Football Players’ Beliefs about Incurring Football-Related Dementia. Orthop. J. Sports Med. 2021, 9, 23259671211001129. [Google Scholar] [CrossRef]
- Pisl, V.; Volavka, J.; Chvojkova, E.; Cechova, K.; Kavalirova, G.; Vevera, J. Dissociation, Cognitive Reflection and Health Literacy Have a Modest Effect on Belief in Conspiracy Theories about COVID-19. Int. J. Environ. Res. Public Health 2021, 18, 5065. [Google Scholar] [CrossRef]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [Green Version]
- Behera, S.K.; Das, S.; Xavier, A.S.; Selvarajan, S.; Anandabaskar, N. Indian Council of Medical Research’s National Ethical Guidelines for biomedical and health research involving human participants: The way forward from 2006 to 2017. Perspect. Clin. Res. 2019, 10, 108. [Google Scholar] [CrossRef]
- Matthiessen, J.; Biltoft-Jensen, A.; Rasmussen, L.B.; Hels, O.; Fagt, S.; Groth, M.V. Comparison of the Danish physical activity questionnaire with a validated position and motion instrument. Eur. J. Epidemiol. 2008, 23, 311–322. [Google Scholar] [CrossRef] [PubMed]
- Aadahl, M.; Jørgensen, T. Validation of a new self-report instrument for measuring physical activity. Med. Sci. Sports Exerc. 2003, 35, 1196–1202. [Google Scholar] [CrossRef] [PubMed]
- Schutte, N.S.; Malouff, J.M.; Hall, L.E.; Haggerty, D.J.; Cooper, J.T.; Golden, C.J.; Dornheim, L. Development and validation of a measure of emotional intelligence. Personal. Individ. Differ. 1998, 25, 167–177. [Google Scholar] [CrossRef]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef]
- Patton, J.H.; Stanford, M.S.; Barratt, E.S. Factor structure of the Barratt impulsiveness scale. J. Clin. Psychol. 1995, 51, 768–774. [Google Scholar] [CrossRef]
- Salthouse, T.A. Trajectories of normal cognitive aging. Psychol. Aging 2019, 34, 17. [Google Scholar] [CrossRef]
- Sewell, K.R.; Erickson, K.I.; Rainey-Smith, S.R.; Peiffer, J.J.; Sohrabi, H.R.; Brown, B.M. Relationships between physical activity, sleep and cognitive function: A narrative review. Neurosci. Biobehav. Rev. 2021, 130, 369–378. [Google Scholar] [CrossRef]
- Hou, Q.; Guan, Y.; Yu, W.; Liu, X.; Wu, L.; Xiao, M.; Lü, Y. Associations between obesity and cognitive impairment in the Chinese elderly: An observational study. Clin. Interv. Aging 2019, 14, 367–373. [Google Scholar] [CrossRef] [Green Version]
- Cook, R.L.; O’Dwyer, N.J.; Donges, C.E.; Parker, H.M.; Cheng, H.L.; Steinbeck, K.S.; Cox, E.P.; Franklin, J.L.; Garg, M.L.; Rooney, K.B.; et al. Relationship between obesity and cognitive function in young women: The food, mood and mind study. J. Obes. 2017, 2017, 5923862. [Google Scholar] [CrossRef] [Green Version]
- Fitzpatrick, S.; Gilbert, S.; Serpell, L. Systematic review: Are overweight and obese individuals impaired on behavioural tasks of executive functioning? Neuropsychol. Rev. 2013, 23, 138–156. [Google Scholar] [CrossRef]
- Leckie, R.L.; Oberlin, L.E.; Voss, M.W.; Prakash, R.S.; Szabo-Reed, A.; Chaddock-Heyman, L.; Phillips, S.M.; Gothe, N.; Mailey, E.; Vieira-Potter, V.; et al. BDNF mediates improvements in executive function following a 1-year exercise intervention. Front. Hum. Neurosci. 2014, 8, 985. [Google Scholar] [CrossRef] [PubMed]
- Whiteman, A.S.; Young, D.E.; He, X.; Chen, T.C.; Wagenaar, R.C.; Stern, C.E.; Schon, K. Interaction between serum BDNF and aerobic fitness predicts recognition memory in healthy young adults. Behav. Brain Res. 2014, 259, 302–312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cox, E.P.; Cook, R.; O’Dwyer, N.; Donges, C.; Parker, H.; Cheng, H.L.; Steinbeck, K.; Franklin, J.; O’Connor, H. The Relationship Between Habitual Physical Activity, Sitting Time, and Cognitive Function in Young Adult Women. J. Phys. Act. Health 2021, 18, 1082–1087. [Google Scholar] [CrossRef]
- Schutte, N.S.; Malouff, J.M.; Thorsteinsson, E.B.; Bhullar, N.; Rooke, S.E. A meta-analytic investigation of the relationship between emotional intelligence and health. Personal. Individ. Differ. 2007, 42, 921–933. [Google Scholar] [CrossRef]
- Sarrionandia, A.; Mikolajczak, M. A meta-analysis of the possible behavioural and biological variables linking trait emotional intelligence to health. Health Psychol. Rev. 2020, 14, 220–244. [Google Scholar] [CrossRef] [PubMed]
- Mayer, J.D.; Roberts, R.D.; Barsade, S.G. Human abilities: Emotional intelligence. Annu. Rev. Psychol. 2008, 59, 507–536. [Google Scholar] [CrossRef] [Green Version]
- Cole, S.; Kvavilashvili, L. Spontaneous and deliberate future thinking: A dual process account. Psychol. Res. 2021, 85, 464–479. [Google Scholar] [CrossRef] [Green Version]
- Aleksovska, K.; Puggina, A.; Giraldi, L.; Buck, C.; Burns, C.; Cardon, G.; Carlin, A.; Chantal, S.; Ciarapica, D.; Colotto, M.; et al. Biological determinants of physical activity across the life course: A “Determinants of Diet and Physical Activity” (DEDIPAC) umbrella systematic literature review. Sports Med. Open 2019, 5, 2. [Google Scholar] [CrossRef]
- Koeneman, M.A.; Verheijden, M.W.; Chinapaw, M.J.; Hopman-Rock, M. Determinants of physical activity and exercise in healthy older adults: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 142. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. WHO Guidelines on Physical Activity and Sedentary Behaviour: Web Annex: Evidence Profiles. 2020. Available online: https://apps.who.int/iris/handle/10665/336657. (accessed on 1 November 2020).
- Rey Lopez, J.P.; Sabag, A.; Martinez, J.M.; Rezende, L.F.; Pastor-Valero, M. Do vigorous-intensity and moderate-intensity physical activities reduce mortality to the same extent? A systematic review and meta-analysis. BMJ Open Sport Exerc. Med. 2020, 6, e000775. [Google Scholar] [CrossRef]
- Martins, A.; Ramalho, N.; Morin, E. A comprehensive meta-analysis of the relationship between emotional intelligence and health. Personal. Individ. Differ. 2018, 49, 554–564. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Figure | Chi-Square | p Value | ||
|---|---|---|---|---|
| Female | Male | Female | Male | |
| Education | 11.7 | 17.6 | 0.69 | 0.28 |
| Residential place (city vs. country) | 48.1 | 11.3 | <0.001 | 0.25 |
| Married vs. single | 4.4 | 12.9 | 0.88 | 0.16 |
| Type of work | 14.2 | 7.7 | 0.077 | 0.56 |
| Residential place (house) | 38.1 | 27.8 | <0.001 | <0.001 |
| Breakfast | 2.1 | 5.8 | 0.9 | 0.43 |
| Overeating | 11.4 | 7.3 | 0.075 | 0.28 |
| Smoking | 15 | 11.2 | 0.089 | 0.026 |
| Alcohol | 13.2 | 17.7 | 0.77 | 0.47 |
| Health | 5.2 | 3.9 | 0.83 | 0.91 |
| Stress | 17.2 | 13.9 | 0.009 | 0.03 |
| Impulsivity | 8.7 | 9.4 | 0.45 | 0.41 |
| Depression | 19.3 | 12.6 | 0.023 | 0.175 |
| Sleep | 15.8 | 8.8 | 0.19 | 0.71 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Skurvydas, A.; Lisinskiene, A.; Majauskiene, D.; Valanciene, D.; Dadeliene, R.; Fatkulina, N.; Sarkauskiene, A. Do Physical Activity, BMI, and Wellbeing Affect Logical Thinking? Int. J. Environ. Res. Public Health 2022, 19, 6631. https://doi.org/10.3390/ijerph19116631
Skurvydas A, Lisinskiene A, Majauskiene D, Valanciene D, Dadeliene R, Fatkulina N, Sarkauskiene A. Do Physical Activity, BMI, and Wellbeing Affect Logical Thinking? International Journal of Environmental Research and Public Health. 2022; 19(11):6631. https://doi.org/10.3390/ijerph19116631
Chicago/Turabian StyleSkurvydas, Albertas, Ausra Lisinskiene, Daiva Majauskiene, Dovile Valanciene, Ruta Dadeliene, Natalja Fatkulina, and Asta Sarkauskiene. 2022. "Do Physical Activity, BMI, and Wellbeing Affect Logical Thinking?" International Journal of Environmental Research and Public Health 19, no. 11: 6631. https://doi.org/10.3390/ijerph19116631
APA StyleSkurvydas, A., Lisinskiene, A., Majauskiene, D., Valanciene, D., Dadeliene, R., Fatkulina, N., & Sarkauskiene, A. (2022). Do Physical Activity, BMI, and Wellbeing Affect Logical Thinking? International Journal of Environmental Research and Public Health, 19(11), 6631. https://doi.org/10.3390/ijerph19116631