
Effect of Second-Hand Smoke Exposure on Establishing Urinary Cotinine-Based Optimal Cut-Off Values for Smoking Status Classification in Korean Adults


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Self-Report for Smoking Status
2.3. Self-Report for SHS Exposure
2.4. Self-Report for the Use of e-Cigarettes
2.5. Measurement of Urinary Cotinine Concentration
2.6. Statistical Analysis
3. Results
3.1. The Characteristics of Study Participants
3.2. The Result of the Self-Reported Smoking Status
3.3. The Result of the Self-Reported SHS Exposure
3.4. The Result of the Self-Reported Use of e-Cigarettes
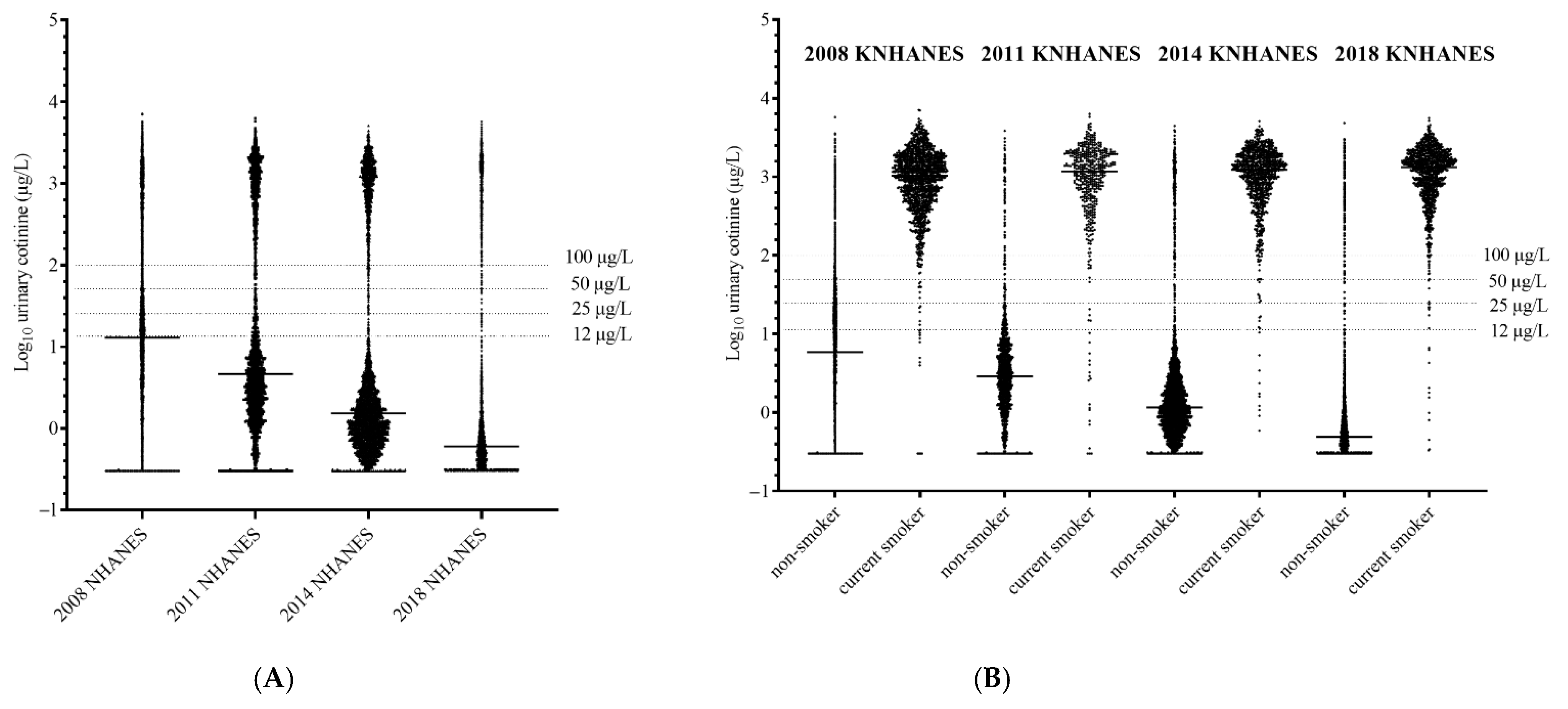
3.5. The Distributions of Urinary Cotinine Concentration from All Participants
3.6. The Distributions of Urinary Cotinine Concentration in Nonsmokers
3.7. The Established Optimal Cut-Off Values of Urinary Cotinine Concentration for Smoking Status Classification
3.8. Comparison of Diagnostic Performance According to Various Urinary Cotinine Cut-Off Values for Smoking Status Classification
3.9. Comparison between Self-Reported SHS Exposure and Urinary Cotinine Concentrations in Nonsmokers
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Samet, J. Tobacco smoking. The leading cause of preventable disease worldwide. Thorac. Surg. Clin. 2013, 23, 103–112. [Google Scholar] [CrossRef] [PubMed]
- Polosa, R.; Thomson, N.C. Smoking and asthma: Dangerous liaisons. Eur. Respir. J. 2013, 41, 716–726. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ebbert, J.O.; Croghan, I.T.; Schroeder, D.R.; Murawski, J.; Hurt, R.D. Association between respiratory tract diseases and secondhand smoke exposure among never smoking flight attendants: A cross-sectional survey. Environ. Health 2007, 6, 28. [Google Scholar] [CrossRef] [Green Version]
- Scherübl, H. Smoking tobacco and cancer risk. Dtsch. Med. Wochenschr. 2021, 146, 412–417. [Google Scholar] [CrossRef]
- Sasco, A.J.; Secretan, M.B.; Straif, K. Tobacco smoking and cancer: A brief review of recent epidemiological evidence. Lung Cancer 2004, 45 (Suppl. S2), S3–S9. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, C.W. A change in the air: Smoking bans gain momentum worldwide. Environ. Health Perspect. 2007, 115, A412–A415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Callinan, J.E.; Clarke, A.; Doherty, K.; Kelleher, C. Legislative smoking bans for reducing secondhand smoke exposure, smoking prevalence and tobacco consumption. Cochrane Database Syst. Rev. 2010, 4, CD005992. [Google Scholar] [CrossRef]
- Bell, K.; McCullough, L.; Devries, K.; Jategaonkar, N.; Greaves, L.; Richardson, L. Location restrictions on smoking: Assessing their differential impacts and consequences in the workplace. Can. J. Public Health 2009, 100, 46–50. [Google Scholar] [CrossRef]
- Kim, B. Workplace smoking ban policy and smoking behavior. J. Prev. Med. Public Health 2009, 42, 293–297. [Google Scholar] [CrossRef]
- Sim, B.; Park, M.B. Exposure to Secondhand Smoke: Inconsistency between Self-Response and Urine Cotinine Biomarker Based on Korean National Data during 2009-2018. Int. J. Environ. Res. Public Health 2021, 18, 9284. [Google Scholar] [CrossRef]
- Kim, J.; Lee, K. Changes in urinary cotinine concentrations in non-smoking adults from the Korean National Environmental Health Survey (KoNEHS) II (2012-2014) after implementation of partial smoke-free regulations. Int. J. Hyg. Environ. Health 2020, 224, 113419. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.Y.; Lim, M.K.; Cho, H.-J. Trends in the Socioeconomic Inequalities Related to Second-Hand Smoke Exposure as Verified by Urine Cotinine Levels Among Nonsmoking Adults: Korea National Health and Nutrition Examination Survey 2008–2018. Nicotine Tob. Res. 2021, 23, 1518–1526. [Google Scholar] [CrossRef] [PubMed]
- Jarvis, M.J.; Tunstall-Pedoe, H.; Feyerabend, C.; Vesey, C.; Saloojee, Y. Comparison of tests used to distinguish smokers from nonsmokers. Am. J. Public Health 1987, 77, 1435–1438. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roussel, G.; Le Quang, N.T.; Miguères, M.L.; Roche, D.; Mongin-Charpin, D.; Chrétien, J.; Ekindjian, O.G. Interpretation of the values of urinary cotinine in smokers and non-smokers. Rev. Mal. Respir. 1991, 8, 225–232. [Google Scholar] [PubMed]
- Jung, S.; Lee, I.S.; Kim, S.B.; Moon, C.S.; Jung, J.Y.; Kang, Y.A.; Park, M.S.; Kim, Y.S.; Kim, S.K.; Chang, J.; et al. Urine Cotinine for Assessing Tobacco Smoke Exposure in Korean: Analysis of the Korea National Health and Nutrition Examination Survey (KNHANES). Tuberc. Respir. Dis. 2012, 73, 210–218. [Google Scholar] [CrossRef]
- Stragierowicz, J.; Mikołajewska, K.; Zawadzka-Stolarz, M.; Polańska, K.; Ligocka, D. Estimation of Cutoff Values of Cotinine in Urine and Saliva for Pregnant Women in Poland. Biomed. Res. Int. 2013, 2013, 386784. [Google Scholar] [CrossRef]
- Campo, L.; Polledri, E.; Bechtold, P.; Gatti, G.; Ranzi, A.; Lauriola, P.; Goldoni, C.A.; Bertazzi, P.A.; Fustinoni, S. Determinants of active and environmental exposure to tobacco smoke and upper reference value of urinary cotinine in not exposed individuals. Environ. Res. 2016, 148, 154–163. [Google Scholar] [CrossRef]
- Ware, L.J.; Charlton, K.; Kruger, R.; Breet, Y.; van Rooyen, J.; Huisman, H.; Botha, S.; Uys, A.S.; Rennie, K.L.; Naidoo, N.; et al. Assessing tobacco use in an African population: Serum and urine cotinine cut-offs from South Africa. Drug Alcohol Depend. 2019, 195, 82–89. [Google Scholar] [CrossRef]
- Domino, E.F. Nontobacco sources of cotinine in the urine of nonsmokers. Clin. Pharmacol. Ther. 1995, 57, 479. [Google Scholar] [CrossRef]
- Hoffmann, D.; Haley, N.J.; Adams, J.D.; Brunnemann, K.D. Tobacco sidestream smoke: Uptake by nonsmokers. Prev. Med. 1984, 13, 608–617. [Google Scholar] [CrossRef]
- Goniewicz, M.L.; Eisner, M.D.; Lazcano-Ponce, E.; Zielinska-Danch, W.; Koszowski, B.; Sobczak, A.; Havel, C.; Jacob, P.; Benowitz, N.L. Comparison of urine cotinine and the tobacco-specific nitrosamine metabolite 4-(methylnitrosamino)-1-(3-pyridyl)-1-butanol (NNAL) and their ratio to discriminate active from passive smoking. Nicotine Tob. Res. 2011, 13, 202–208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pickett, K.E.; Rathouz, P.J.; Kasza, K.; Wakschlag, L.S.; Wright, R. Self-reported smoking, cotinine levels, and patterns of smoking in pregnancy. Paediatr. Perinat. Epidemiol. 2005, 19, 368–376. [Google Scholar] [CrossRef] [PubMed]
- Riboli, E.; Preston-Martin, S.; Saracci, R.; Haley, N.J.; Trichopoulos, D.; Becher, H.; Burch, J.D.; Fontham, E.T.; Gao, Y.T.; Jindal, S.K.; et al. Exposure of nonsmoking women to environmental tobacco smoke: A 10-country collaborative study. Cancer Causes Control 1990, 1, 243–252. [Google Scholar] [CrossRef] [PubMed]
- Zielińska-Danch, W.; Wardas, W.; Sobczak, A.; Szołtysek-Bołdys, I. Estimation of urinary cotinine cut-off points distinguishing non-smokers, passive and active smokers. Biomarkers 2007, 12, 484–496. [Google Scholar] [CrossRef]
- Kim, S. Overview of Cotinine Cutoff Values for Smoking Status Classification. Int. J. Environ. Res. Public Health 2016, 13, 1236. [Google Scholar] [CrossRef]
- Pirkle, J.L.; Bernert, J.T.; Caudill, S.P.; Sosnoff, C.S.; Pechacek, T.F. Trends in the exposure of nonsmokers in the U.S. population to secondhand smoke: 1988-2002. Environ. Health Perspect. 2006, 114, 853–858. [Google Scholar] [CrossRef] [Green Version]
- Göney, G.; Çok, İ.; Tamer, U.; Burgaz, S.; Şengezer, T. Urinary cotinine levels of electronic cigarette (e-cigarette) users. Toxicol. Mech. Methods 2016, 26, 414–418. [Google Scholar] [CrossRef]
- Ichihara, K.; Itoh, Y.; Lam, C.W.; Poon, P.M.; Kim, J.H.; Kyono, H.; Chandrawening, N.; Muliaty, D. Sources of variation of commonly measured serum analytes in 6 Asian cities and consideration of common reference intervals. Clin. Chem. 2008, 54, 356–365. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Data Characteristics | KNHANES (2008–2018) | |||
|---|---|---|---|---|
| 2008 | 2011 | 2014 | 2018 | |
| Total enrolled participants (n) | 5658 | 1857 | 4939 | 5775 |
| Age, year (mean ± SD) | 49.1 ± 16.3 | 45.6 ± 14.7 | 51.6 ± 16.4 | 51.5 ± 16.8 |
| Sex, female (n, %) | 3135 (55.4%) | 892 (48.0%) | 2804 (56.8%) | 3179 (55.0%) |
| Urinary cotinine (µg/L) | 314.6 ± 691.8 | 363.5 ± 761.3 | 286.4 ± 655.6 | 277.7 ± 662.8 |
| Response for self-report (n, %) | 5627 (99.4%) | 1832 (98.7%) | 4639 (93.9%) | 5739 (99.4%) |
| Nonsmoker, self-report (n, %) | 4340 (77.1%) | 1375 (75.1%) | 3754 (80.9%) | 4692 (81.8%) |
| Current smoker, self-report (n, %) | 1287 (22.9%) | 457 (24.9%) | 885 (19.1%) | 1047 (18.2%) |
| Use of e-cigarettes | ||||
| Current e-cigarette user (n, %) | 65 (1.3%) | 163 (2.8%) | ||
| Non-e-cigarette user (n, %) | 4874 (98.7%) | 5612 (97.2%) | ||
| Year | Daily Smoking Status | ≤100 µg/L of Urinary Cotinine | >100 µg/L of Urinary Cotinine | Total | |||
|---|---|---|---|---|---|---|---|
| n (%) | Concentration (µg/L, [Median, IQR]) | n (%) | Concentration (µg/L) | n (%) | Concentration (µg/L) | ||
| 2008 | Daily smoker | 43 (100.0%) | 39.5 (9.7–76.3) | 1243 (100.0%) | 1067.1 (573.6–1712.9) | 1286 (100.0%) | 1032.1 (529.7–1687.6) |
| Non-daily smoker | 1 | 313.0 | 1 | 313.0 | |||
| total | 43 (100.0%) | 39.5 (9.7–76.3) | 1244 (100.0%) | 1067.1 (573.6–1712.9) | 1287 (100.0%) | 1032.1 (529.7–1687.6) | |
| 2011 | Daily smoker | 19 (61.3%) | 2.9 (1.1–14.9) | 411 (96.5%) | 1304.3 (728.2–1975.1) | 430 (94.1%) | 1251.0 (678.9–1945.0) |
| Non-daily smoker | 12 (38.7%) | 33.3 (7.5–75.6) | 15 (3.5%) | 423.2 (205.2–1371.7) | 27 (5.9%) | 107.9 (45.9–425.1) | |
| total | 31 (100.0%) | 5.7 (1.2–49.0) | 426 (100.0%) | 1275.3 (710.1–1962.6) | 457 (100.0%) | 1170.4 (559.1–1935.1) | |
| 2014 | Daily smoker | 6 (17.6%) | 55.1 (0.9–84.0) | 788 (92.6%) | 1310.7 (808.5–1886.2) | 794 (89.7%) | 1295.7 (797.4–1876.6) |
| Non-daily smoker | 28 (83.4%) | 30.0 (7.9–49.5) | 63 (7.4%) | 548.3 (254.5–1015.6) | 91 (10.3%) | 310.5 (64.5–758.6) | |
| total | 34 (100.0%) | 27.5 (4.9–67.3) | 851 (100.0%) | 1257.1 (730.6–1844.1) | 885 (100.0%) | 1231.0 (670.6–1823.6) | |
| 2018 | Daily smoker | 8 (22.8%) | 42.2 (8.8–84.3) | 898 (88.7%) | 1438.0 (844.0–1980.0) | 906 (93.6%) | 1434.0 (828.3–1973.0) |
| Non-daily smoker | 27 (77.2%) | 21.8 (2.1–69.1) | 114 (11.3%) | 577.5 (335.0–1228.0) | 141 (6.4%) | 472.0 (174.5–1069.0) | |
| total | 35 (100.0%) | 24.0 (2.1–74.0) | 1012 (100.0%) | 1374.0 (765.5–1908.0) | 1047 (100.0%) | 1324.0 (697.5–1890.0) | |
| Year | ≤0.30 µg/L of Urinary Cotinine (%) | Self-Report for SHS Exposure | ≤0.30 µg/L of Urinary Cotinine | >0.30 µg/L of Urinary Cotinine | Total | |||
|---|---|---|---|---|---|---|---|---|
| n (%) | Concentration (µg/L) | n (%) | Concentration (µg/L, [Median, IQR]) | n (%) | Concentration (µg/L) | |||
| 2008 | 25.8% | SHS exposure | 320 (28.5%) | 0.30 | 1290 (40.1%) | 15.03 (4.97–35.02) | 1610 (37.1%) | 9.54 (1.34–26.97) |
| Unclear response | 21 (1.9%) | 0.30 | 52 (1.6%) | 8.40 (1.65–19.05) | 73 (1.7%) | 2.26 (0.30–11.46) | ||
| No SHS exposure | 780 (69.6%) | 0.30 | 1877(58.3%) | 10.40 (3.47–22.98) | 2657 (61.2%) | 4.26 (1.00–16.47) | ||
| Total | 1121 (100.0%) | 0.30 | 3219 (100.0%) | 11.95 (3.98–26.91) | 4340 (100.0%) | 5.86 (0.30–20.03) | ||
| 2011 | 8.1% | SHS exposure | 22 (19.8%) | 0.30 | 458 (36.2%) | 3.53 (1.91–7.39) | 480 (34.9%) | 3.33 (1.61–7.15) |
| Unclear response | 10 (9.0%) | 0.30 | 52 (4.1%) | 2.81 (1.19–4.36) | 62 (4.5%) | 1.78 (0.64–4.12) | ||
| No SHS exposure | 79 (71.2%) | 0.30 | 754 (59.7%) | 2.94 (1.51–6.29) | 833 (60.6%) | 2.54 (1.16–5.45) | ||
| Total | 111 (100.0%) | 0.30 | 1264 (100.0%) | 3.20 (1.59–6.64) | 1375 (100.0%) | 2.83 (1.25–6.17) | ||
| 2014 | 4.9% | SHS exposure | 26 (14.1%) | 0.30 | 1004 (28.1%) | 1.67 (0.93–3.29) | 1030 (27.4%) | 1.61 (0.88–3.21) |
| Unclear response | 2 (0.1%) | 1.85 (0.66–3.03) | 2 (0.1%) | 1.85 (0.66–3.03) | ||||
| No SHS exposure | 159 (85.9%) | 0.30 | 2563 (71.8%) | 1.09 (0.68–1.91) | 2722 (72.5%) | 1.03 (0.62–1.84) | ||
| Total | 185 (100.0%) | 0.30 | 3569 (100.0%) | 1.20 (0.73–2.28) | 3754 (100.0%) | 1.14 (0.67–2.19) | ||
| 2018 | 25.4% | SHS exposure | 36 (3.3%) | 0.30 | 284 (8.1%) | 0.82 (0.54–1.95) | 320 (6.8%) | 0.73 (0.44–1.43) |
| Unclear response | 7 (0.3%) | 0.30 | 129 (3.7%) | 1.23 (0.67–2.68) | 136 (2.9%) | 1.21 (0.62–2.54) | ||
| No SHS exposure | 1148 (96.4%) | 0.30 | 3088 (88.2%) | 0.59 (0.42–0.99) | 4236 (90.3%) | 0.46 (0.30–0.78) | ||
| Total | 1191 (100.0%) | 0.30 | 3501 (100.0%) | 0.62 (0.43–1.07) | 4692 (100.0%) | 0.48 (0.30–0.84) | ||
| Year | Self-Report for SHS Exposure | Current e-Cigarette Users | Non-e-Cigarette Users | Total | |||
|---|---|---|---|---|---|---|---|
| n (%) | Concentration (µg/L, [Median, IQR]) | n (%) | Concentration (µg/L) | n (%) | Concentration (µg/L) | ||
| 2014 | Daily smoker | 47 (72.3%) | 1473.9 (973.3–2015.6) | 747 (15.3%) | 1291.4 (779.7–1870.8) | 794 (16.1%) | 1295.7 (797.4–1876.6) |
| Non-daily smoker | 4 (6.2%) | 844.7 (45.6–1394.5) | 87 (1.8%) | 310.5 (64.5–735.6) | 91 (2.9%) | 310.5 (64.5–758.6) | |
| Nonsmoker with SHS exposure | 6 (9.2%) | 2.8 (2.4–676.5) | 1024 (21.0%) | 1.61 (0.88–3.21) | 1030 (20.9%) | 1.61 (0.88–3.21) | |
| Nonsmoker with unclear response | 2 (0.1%) | 1.85 (0.66–3.03) | 2 (0.0%) | 1.85 (0.66–3.03) | |||
| Nonsmoker without SHS exposure | 8 (12.3%) | 760.4 (57.7–1175.0) | 2714 (55.7%) | 1.03 (0.62–1.82) | 2722 (55.1%) | 1.03 (0.62–1.84) | |
| total | 65 (100.0%) | 1124.2 (711.6–1832.0) | 4874 (100.0%) | 1.48 (0.75–6.14) | 4939 (100.0%) | 1.52 (0.76–7.22) | |
| 2018 | Daily smoker | 124 (76.1%) | 1540.0 (870.0–2176.0) | 782 (14.0%) | 1422.0 (820.0–1948.0) | 906 (16.1%) | 1434.0 (828.3–1973.0) |
| Non-daily smoker | 20 (12.3%) | 693.5 (424.5–1084.5) | 121 (2.2%) | 352.0 (96.9–906.5) | 141 (2.5%) | 472.0 (174.5–1069.0) | |
| Nonsmoker with SHS exposure | 5 (3.1%) | 1530.0 (1068.0–1884.0) | 318 (5.7%) | 0.73 (0.30–1.54) | 320 (5.7%) | 0.73 (0.44–1.43) | |
| Nonsmoker with unclear response | 1 (0.6%) | 2168 | 135 (2.4%) | 1.21 (0.62–2.53) | 136 (2.4%) | 1.21 (0.62–2.54) | |
| Nonsmoker without SHS exposure | 13 (8.0%) | 712.0 (0.43–1528.0) | 4223 (75.7%) | 0.46 (1.08–0.78) | 4236 (75.5%) | 0.46 (0.30–0.78) | |
| total | 163 (100.0%) | 1408.0 (740.0–2122.0) | 5576 (100.0%) | 0.58 (0.33–17.75) | 5612 (100.0%) | 1.48 (0.75–6.14) | |
| Year | Classification | Optimal Cut-Off Value of Urinary Cotinine (µg/L) | Sensitivity (%) | Specificity (%) | Youden’s Index | AUC | p Value |
|---|---|---|---|---|---|---|---|
| 2008 | Current smoker | 86.48 | 97.20 | 94.06 | 0.913 | 0.978 | <0.0001 |
| (95% CI, 71.30–104.60) | (96.15–98.03) | (93.31–94.74) | (0.899–0.922) | (0.974–0.982) | |||
| Daily smoker | |||||||
| 2011 | Current smoker | 43.85 | 95.19 | 94.84 | 0.901 | 0.962 | <0.0001 |
| (38.51–67.70) | (92.80–96.96) | (93.53–95.95) | (0.873–0.921) | (0.952–0.970) | |||
| Daily smoker | 107.91 | 93.00 | 96.15 | 0.906 | 0.962 | <0.0001 | |
| (49.56–130.64) | (90.26–95.16) | (94.99–97.10) | (0.881–0.925) | (0.953–0.971) | |||
| 2014 | Current smoker | 15.93 | 98.53 | 95.05 | 0.936 | 0.983 | <0.0001 |
| (10.45–42.41) | (97.50–99.22) | (94.30–95.72) | (0.923–0.944) | (0.978–0.986) | |||
| Daily smoker | 110.51 | 95.99 | 96.16 | 0.933 | 0.980 | <0.0001 | |
| (79.71–135.29) | (94.51–97.16) | (95.50–96.76) | (0.923–0.941) | (0.975–0.983) | |||
| 2018 | Current smoker | 11.50 | 98.85 | 95.80 | 0.947 | 0.986 | <0.0001 |
| (5.89–19.90) | (98.01–99.41) | (95.19–96.36) | (0.936–0.954) | (0.982–0.989) | |||
| Daily smoker | 77.90 | 97.33 | 96.29 | 0.933 | 0.981 | <0.0001 | |
| (11.53–112.00) | (96.16–98.22) | (95.71–96.81) | (0.922–0.940) | (0.978–0.985) |
| Year | Current Smoking Prevalence (%) | Cut-Off Value of Urinary Cotinine (µg/L) | Sensitivity (%) | Specificity (%) | PPV (%) | NPV (%) | AUC | p Value |
|---|---|---|---|---|---|---|---|---|
| 2008 | 22.87% | 12 | 98.91 | 62.95 | 44.19 | 99.49 | 0.809 | <0.0001 |
| (98.18 to 99.40) | (61.49 to 64.39) | (43.22 to 45.16) | (99.14 to 99.70) | (0.799 to 0.819) | ||||
| 25 | 98.52 | 79.98 | 59.34 | 99.46 | 0.893 | <0.0001 | ||
| (97.70 to 99.11) | (78.76 to 81.16) | (57.88 to 60.77) | (99.15 to 99.65) | (0.884 to 0.900) | ||||
| 50 | 97.98 | 90.39 | 75.15 | 99.34 | 0.942 | <0.0001 | ||
| (97.05 to 98.68) | (89.48 to 91.25) | (73.40 to 76.82) | (99.04 to 99.55) | (0.935 to 0.948) | ||||
| 100 | 96.66 | 94.49 | 83.88 | 98.96 | 0.956 | <0.0001 | ||
| (95.53 to 97.57) | (93.77 to 95.15) | (82.14 to 85.49) | (98.61 to 99.23) | (0.950 to 0.961) | ||||
| 2011 | 24.95% | 12 | 96.06 | 88.36 | 73.29 | 98.54 | 0.922 | <0.0001 |
| (93.85 to 97.65) | (86.55 to 90.01) | (70.32 to 76.06) | (97.72 to 99.07) | (0.909 to 0.934) | ||||
| 25 | 95.19 | 93.24 | 82.39 | 98.31 | 0.942 | <0.0001 | ||
| (92.80 to 96.96) | (91.78 to 94.51) | (79.34 to 85.07) | (97.48 to 98.87) | (0.930 to 0.952) | ||||
| 50 | 94.97 | 94.98 | 86.28 | 98.27 | 0.950 | <0.0001 | ||
| (92.54 to 96.78) | (93.69 to 96.08) | (83.31 to 88.79) | (97.44 to 98.83) | (0.939 to 0.959) | ||||
| 100 | 93.22 | 96.07 | 88.75 | 97.71 | 0.946 | <0.0001 | ||
| (90.51 to 95.35) | (94.91 to 97.04) | (85.85 to 91.12) | (96.81 to 98.36) | (0.935 to 0.956) | ||||
| 2014 | 19.08% | 12 | 98.76 | 94.73 | 81.53 | 99.69 | 0.967 | <0.0001 |
| (97.79 to 99.38) | (93.96 to 95.42) | (79.40 to 83.49) | (99.45 to 99.83) | (0.962 to 0.972) | ||||
| 25 | 98.31 | 95.21 | 82.86 | 99.58 | 0.968 | <0.0001 | ||
| (97.22 to 99.05) | (94.47 to 95.87) | (80.73 to 84.79) | (99.31 to 99.75) | 0.962 to 0.972 | ||||
| 50 | 97.18 | 95.55 | 83.74 | 99.31 | 0.964 | <0.0001 | ||
| (95.86 to 98.16) | (94.84 to 96.19) | (81.61 to 85.66) | (98.99 to 99.53) | (0.958 to 0.969) | ||||
| 100 | 96.16 | 96.08 | 85.27 | 99.07 | 0.961 | <0.0001 | ||
| (94.67 to 97.33) | (95.41 to 96.68) | (83.16 to 87.16) | (98.71 to 99.33) | (0.955 to 0.967) | ||||
| 2018 | 18.24% | 12 | 98.76 | 95.82 | 84.07 | 99.71 | 0.973 | <0.0001 |
| (97.89 to 99.34) | (95.21 to 96.38) | (82.14 to 85.82) | (99.51 to 99.83) | (0.968 to 0.977) | ||||
| 25 | 98.28 | 96.01 | 84.62 | 99.60 | 0.971 | <0.0001 | ||
| (97.30 to 98.98) | (95.42 to 96.56) | (82.70 to 86.37) | (99.37 to 99.75) | (0.967 to 0.976) | ||||
| 50 | 97.89 | 96.10 | 84.85 | 99.51 | 0.970 | <0.0001 | ||
| (96.84 to 98.68) | (95.51 to 96.64) | (82.93 to 86.59) | (99.27 to 99.68) | (0.965 to 0.974) | ||||
| 100 | 96.85 | 96.40 | 85.71 | 99.28 | 0.966 | <0.0001 | ||
| (95.60 to 97.82) | (95.83 to 96.91) | (83.80 to 87.44) | (98.99 to 99.48) | (0.961 to 0.971) |
| Year | Current Smoking Prevalence (%) | Range of Cotinine (µg/L) | Nonsmoker | Current Smoker | Total | |||
|---|---|---|---|---|---|---|---|---|
| n (%) | Concentration (µg/L) | n (%) | Concentration (µg/L) | n (%) | Concentration (µg/L) | |||
| 2008 | 22.87% | <12 | 2732 (62.9%) | 2.91 ± 3.39 | 14 (1.1%) | 2.27 ± 4.46 | 2746 (48.8%) | 2.92 ± 3.40 |
| 12–25 | 739 (17.0%) | 17.69 ± 3.67 | 5 (0.4%) | 18.14 ± 4.15 | 744 (13.2%) | 17.71 ± 3.67 | ||
| 25–50 | 452 (10.4%) | 35.03 ± 7.24 | 7 (0.5%) | 38.89 ± 5.82 | 459 (8.2%) | 35.08 ± 7.22 | ||
| 50–100 | 178 (4.1%) | 66.95 ± 13.54 | 17 (1.3%) | 80.37 ± 11.84 | 195 (3.5%) | 68.12 ± 13.90 | ||
| >100 | 239 (5.5%) | 612.94 ± 615.77 | 1244 (96.7%) | 1260.75 ± 920.26 | 1483 (26.4%) | 1159.58 ± 919.22 | ||
| total | 4340 (100.0%) | 44.99 ± 199.65 | 1287 (100.0%) | 1220.02 ± 930.92 | 5627 (100.0%) | 314.75 ± 691.80 | ||
| 2011 | 24.95% | <12 | 1215 (88.4%) | 3.19 ± 2.67 | 18 (3.9%) | 2.78 ± 2.82 | 1233 (67.3%) | 3.20 ± 2.70 |
| 12–25 | 67 (4.9%) | 16.74 ± 3.72 | 4 (0.9%) | 16.95 ± 2.77 | 71 (3.9%) | 16.75 ± 3.66 | ||
| 25–50 | 24 (1.7%) | 34.68 ± 6.50 | 1 (0.2%) | 45.9 | 25 (1.4%) | 35.13 ± 6.74 | ||
| 50–100 | 15 (1.1%) | 75.19 ± 12.95 | 8 (1.8%) | 76.43 ± 13.99 | 23 (1.3%) | 75.62 ± 13.02 | ||
| >100 | 54 (3.9%) | 931.95 ± 725.49 | 426 (93.2%) | 1407.22 ± 930.46 | 480 (26.2%) | 1353.32 ± 921.67 | ||
| total | 1375 (100.0%) | 41.66 ± 229.81 | 457 (100.0%) | 1313.46 ± 963.35 | 1832 (100.0%) | 363.48 ± 761.32 | ||
| 2014 | 19.08% | <12 | 3556 (94.7%) | 1.61 ± 1.57 | 11 (1.2%) | 3.68 ± 3.92 | 3567 (76.9%) | 1.62 ± 1.60 |
| 12–25 | 18 (0.5%) | 14.86 ± 2.22 | 4 (0.5%) | 14.94 ± 2.04 | 22 (0.5%) | 15.44 ± 2.66 | ||
| 25–50 | 13 (0.3%) | 34.64 ± 5.87 | 10 (1.1%) | 38.55 ± 10.77 | 23 (0.5%) | 36.59 ± 8.29 | ||
| 50–100 | 20 (0.5%) | 79.37 ± 14.95 | 9 (1.0%) | 86.34 ± 11.25 | 29 (0.6%) | 82.03 ± 14.11 | ||
| >100 | 147 (3.9%) | 889.69 ± 673.21 | 851 (96.2%) | 1352.72 ± 805.83 | 998 (21.5%) | 1288.67 ± 811.61 | ||
| total | 3754 (100.0%) | 36.98 ± 217.51 | 885 (100.0%) | 1302.18 ± 829.72 | 4639 (100.0%) | 286.39 ± 655.64 | ||
| 2018 | 18.24% | <12 | 4496 (95.8%) | 0.73 ± 0.83 | 13 (1.2%) | 2.95 ± 3.43 | 4509 (78.6%) | 0.74 ± 0.86 |
| 12–25 | 9 (0.2%) | 20.19 ± 4.18 | 5 (0.5%) | 21.08 ± 2.45 | 14 (0.2%) | 20.51 ± 3.57 | ||
| 25–50 | 4 (0.1%) | 38.32 ± 8.5 | 4 (0.4%) | 40.25 ± 11.15 | 8 (0.1%) | 39.29 ± 9.24 | ||
| 50–100 | 14 (0.3%) | 74.42 ± 15.86 | 11 (1.1%) | 78.07 ±14.75 | 25 (0.4%) | 75.54 ± 15.08 | ||
| >100 | 169 (3.6%) | 881.79 ± 717.80 | 1014 (96.8%) | 1409.46 ± 834.49 | 1183 (20.6%) | 1338.07 ± 841.05 | ||
| total | 4692 (100.0%) | 32.76 ± 213.10 | 1047 (100.0%) | 1366.15 ± 855.65 | 5739 (100.0%) | 277.68 ± 662.80 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, H.-S.; Cho, J.-H.; Lee, Y.-J.; Park, D.-S. Effect of Second-Hand Smoke Exposure on Establishing Urinary Cotinine-Based Optimal Cut-Off Values for Smoking Status Classification in Korean Adults. Int. J. Environ. Res. Public Health 2022, 19, 7971. https://doi.org/10.3390/ijerph19137971
Lee H-S, Cho J-H, Lee Y-J, Park D-S. Effect of Second-Hand Smoke Exposure on Establishing Urinary Cotinine-Based Optimal Cut-Off Values for Smoking Status Classification in Korean Adults. International Journal of Environmental Research and Public Health. 2022; 19(13):7971. https://doi.org/10.3390/ijerph19137971
Chicago/Turabian StyleLee, Hyun-Seung, Ji-Hyun Cho, Young-Jin Lee, and Do-Sim Park. 2022. "Effect of Second-Hand Smoke Exposure on Establishing Urinary Cotinine-Based Optimal Cut-Off Values for Smoking Status Classification in Korean Adults" International Journal of Environmental Research and Public Health 19, no. 13: 7971. https://doi.org/10.3390/ijerph19137971
APA StyleLee, H. -S., Cho, J. -H., Lee, Y. -J., & Park, D. -S. (2022). Effect of Second-Hand Smoke Exposure on Establishing Urinary Cotinine-Based Optimal Cut-Off Values for Smoking Status Classification in Korean Adults. International Journal of Environmental Research and Public Health, 19(13), 7971. https://doi.org/10.3390/ijerph19137971