
COVID-19 Aftermath: Exploring the Mental Health Emergency among Students at a Northern Italian University

 , , , , , ,
, , , , , ,  ,
,  ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Enrollment and Questionnaire
2.3. Statistical Analysis
3. Results
3.1. Descriptive Statistics
3.2. Inferential Data Analysis
3.2.1. Factor Analysis
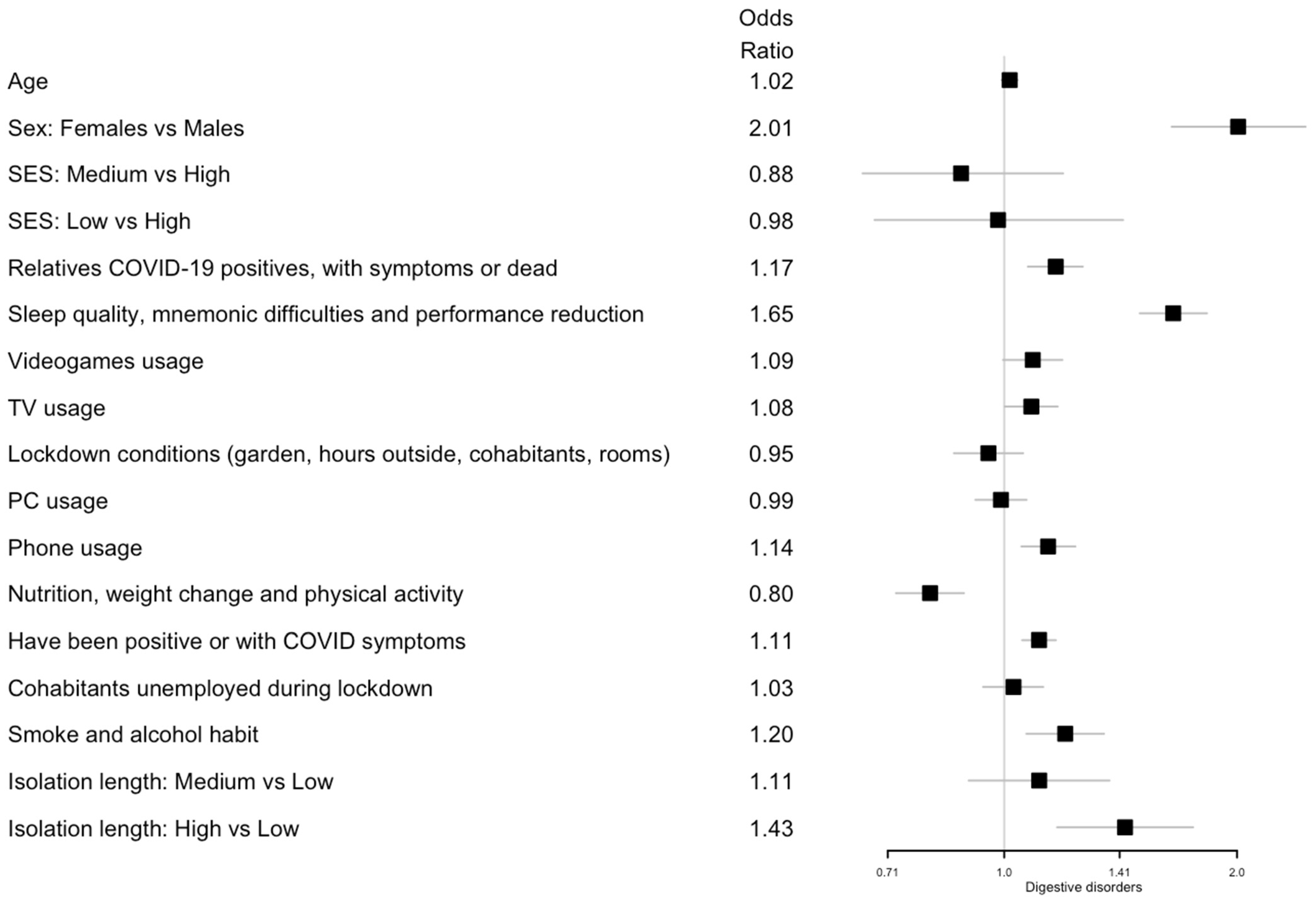
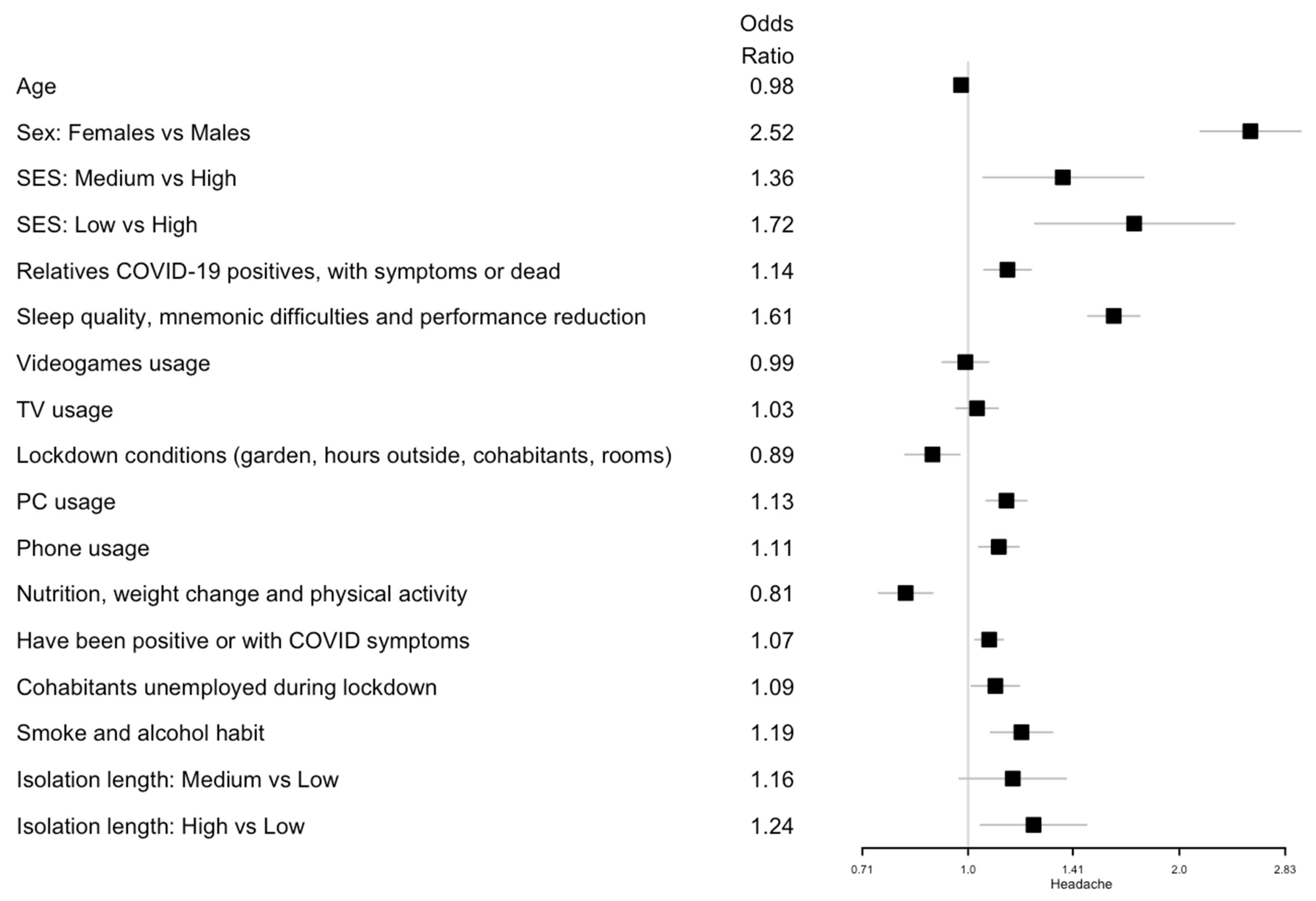
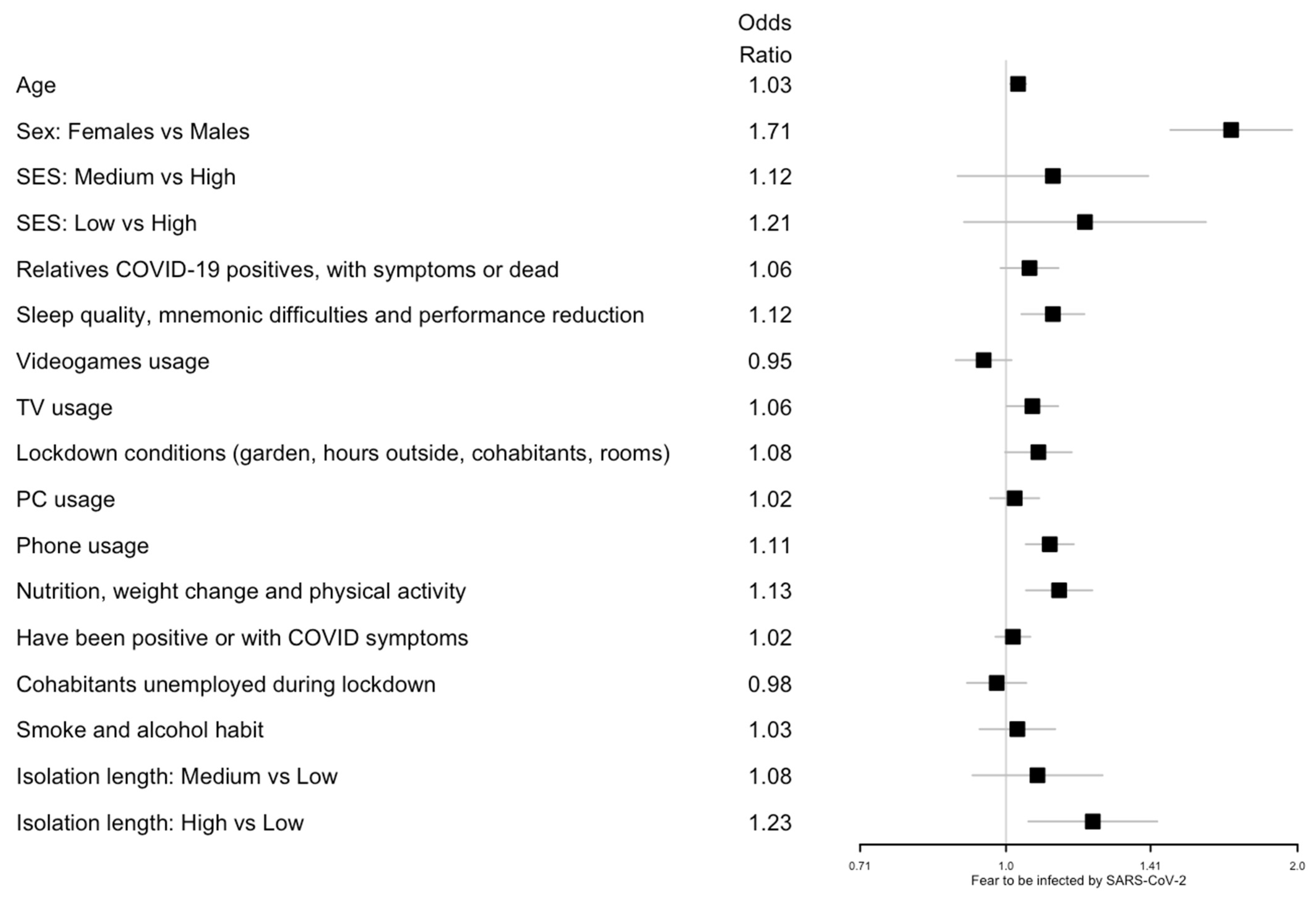
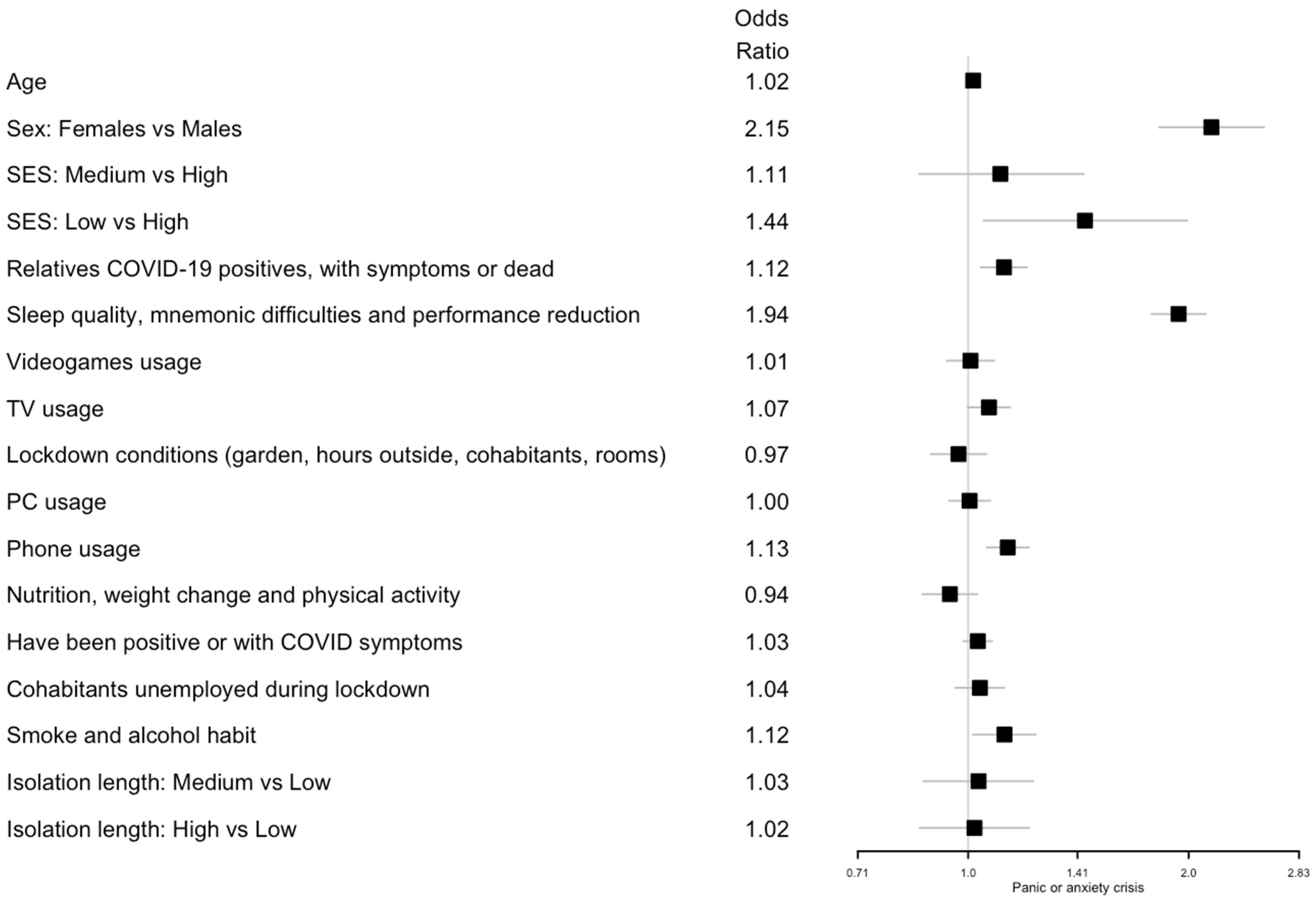
3.2.2. Association between Health Outcomes and Covariates
4. Discussion
5. Limitations and Further Research
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef] [Green Version]
- Salari, N.; Hosseinian-Far, A.; Jalali, R.; Vaisi-Raygani, A.; Rasoulpoor, S.; Mohammadi, M.; Rasoulpoor, S.; Khaledi-Paveh, B. Prevalence of stress, anxiety, depression among the general population during the COVID-19 pandemic: A systematic review and meta-analysis. Glob. Health 2020, 16, 57. [Google Scholar] [CrossRef] [PubMed]
- Nitschke, J.P.; Forbes, P.; Ali, N.; Cutler, J.; Apps, M.; Lockwood, P.; Lamm, C. Resilience during uncertainty? Greater social connectedness during COVID-19 lockdown is associated with reduced distress and fatigue. Br. J. Health Psychol. 2021, 26, 553–569. [Google Scholar] [CrossRef]
- Kim, H.H.; Jung, J.H. Social Isolation and Psychological Distress during the COVID-19 Pandemic: A Cross-National Analysis. Gerontologist 2021, 61, 103–113. [Google Scholar] [CrossRef] [PubMed]
- Bu, F.; Steptoe, A.; Fancourt, D. Who is lonely in lockdown? Cross-cohort analyses of predictors of loneliness before and during the COVID-19 pandemic. Public Health 2020, 186, 31–34. [Google Scholar] [CrossRef]
- Volken, T.; Zysset, A.; Amendola, S.; Swormink, A.; Huber, M.; Wyl, A.; Dratva, J. Depressive Symptoms in Swiss University Students during the COVID-19 Pandemic and Its Correlates. Int. J. Environ. Res. Public Health 2021, 18, 1458. [Google Scholar] [CrossRef]
- Xiong, J.; Lipsitz, O.; Nasri, F.; Lui, L.; Gill, H.; Phan, L.; Chen-Li, D.; Iacobucci, M.; Ho, R.; Majeed, A.; et al. Impact of COVID-19 pandemic on mental health in the general population: A systematic review. J. Affect Disord. 2020, 277, 55–64. [Google Scholar] [CrossRef]
- Rogowska, A.M.; Kuśnierz, C.; Bokszczanin, A. Examining Anxiety, Life Satisfaction, General Health, Stress and Coping Styles during COVID-19 Pandemic in Polish Sample of University Students. Psychol. Res. Behav. Manag. 2020, 13, 797–811. [Google Scholar] [CrossRef]
- Schnell, T.; Krampe, H. Meaning in Life and Self-Control Buffer Stress in Times of COVID-19: Moderating and Mediating Effects with Regard to Mental Distress. Front. Psychiatry 2020, 11, 582352. [Google Scholar] [CrossRef]
- Qi, M.; Li, P.; Moyle, W.; Weeks, B.; Jones, C. Physical Activity, Health-Related Quality of Life, and Stress among the Chinese Adult Population during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2020, 17, 6494. [Google Scholar] [CrossRef]
- Merikangas, K.R.; Nakamura, E.F.; Kessler, R.C. Epidemiology of mental disorders in children and adolescents. Dialogues Clin. Neurosci. 2009, 11, 7–20. [Google Scholar] [CrossRef]
- Vahratian, A.; Blumberg, S.J.; Terlizzi, E.P.; Schiller, J.S. Symptoms of Anxiety or Depressive Disorder and Use of Mental Health Care among Adults during the COVID-19 Pandemic—United States. Available online: https://www.cdc.gov/mmwr/volumes/70/wr/mm7013e2.htm (accessed on 2 April 2021).
- Barros, M.B.A.; Lima, M.G.; Malta, D.C.; Szwarcwald, C.L.; Azevedo, R.C.S.; Romero, D.; Júnior, P.R.B.; Azevedo, L.O.; Machado, I.E.; Damacena, G.N.; et al. Report on sadness/depression, nervousness/anxiety and sleep problems in the Brazilian adult population during the COVID-19 pandemic. Epidemiol. Serv. Saude 2020, 29, e2020427. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Zhao, J.; Ma, Z.; McReynolds, L.S.; Lin, D.; Chen, Z.; Wang, T.; Wang, D.; Zhang, Y.; Zhang, J.; et al. Mental Health Among College Students during the COVID-19 Pandemic in China: A 2-Wave Longitudinal Survey. J. Affect Disord. 2021, 281, 597–604. [Google Scholar] [CrossRef]
- Marinaci, T.; Carpinelli, L.; Venuleo, C.; Savarese, G.; Cavallo, P. Emotional distress, psychosomatic symptoms and their relationship with institutional responses: A survey of Italian frontline medical staff during the COVID-19 pandemic. Heliyon 2020, 6, e05766. [Google Scholar] [CrossRef] [PubMed]
- Almeida-Leite, C.M.; Stuginski-Barbosa, J.; Conti, P.C.R. How psychosocial and economic impacts of COVID-19 pandemic can interfere on bruxism and temporomandibular disorders? J. Appl. Oral Sci. 2020, 28, e20200263. [Google Scholar] [CrossRef] [PubMed]
- Cavallo, P.; Savarese, G.; Carpinelli, L. Bruxism and health related quality of life in southern Italy’s prison inmates. Community Dent. Health 2014, 31, 117–122. [Google Scholar] [PubMed]
- Wang, X.; Hegde, S.; Son, C.; Keller, B.; Smith, A.; Sasangohar, F. Investigating Mental Health of US College Students during the COVID-19 Pandemic: Cross-Sectional Survey Study. J. Med. Internet Res. 2020, 22, e22817. [Google Scholar] [CrossRef] [PubMed]
- Woolston, C. ‘The problem is greater than it’s ever been’: US universities urged to invest in mental-health resources. Nature 2021, 590, 171–172. Available online: https://www.nature.com/articles/d41586-021-00229-2 (accessed on 25 January 2021). [CrossRef]
- Wilson, R.S.; Krueger, K.R.; Arnold, S.E.; Schneider, J.A.; Kelly, J.F.; Barnes, L.L.; Tang, Y.; Bennett, D.A. Loneliness and risk of Alzheimer disease. Arch. Gen. Psychiatry 2007, 64, 234–240. [Google Scholar] [CrossRef] [Green Version]
- Achenbach, T.M.; Ivanova, M.Y.; Rescorla, L.A. Empirically based assessment and taxonomy of psychopathology for ages 1½-90+ years: Developmental, multi-informant, and multicultural findings. Compr. Psychiatry 2017, 79, 4–18. [Google Scholar] [CrossRef]
- Son, C.; Hegde, S.; Smith, A.; Wang, X.; Sasangohar, F. Effects of COVID-19 on College Students’ Mental Health in the United States: Interview Survey Study. J. Med. Internet Res. 2020, 22, e21279. [Google Scholar] [CrossRef]
- Weiner, H. The dynamics of the organism: Implications of recent biological thought for psychosomatic theory and research. Psychosom. Med. 1989, 51, 608–635. [Google Scholar] [CrossRef] [PubMed]
- Fava, G.A.; Cosci, F.; Sonino, N. Current Psychosomatic Practice. Psychother. Psychosom. 2017, 86, 13–30. [Google Scholar] [CrossRef] [PubMed]
- Gitlin, D.F.; Levenson, J.L.; Lyketsos, C.G. Psychosomatic medicine: A new psychiatric subspecialty. Acad. Psychiatry 2004, 28, 4–11. [Google Scholar] [CrossRef] [PubMed]
- Moriarty, T.; Bourbeau, K.; Fontana, F.; McNamara, S.; Silva, M.P. The Relationship between Psychological Stress and Healthy Lifestyle Behaviors during COVID-19 among Students in a US Midwest University. Int. J. Environ. Res. Public Health 2021, 18, 4752. [Google Scholar] [CrossRef]
- Xiao, H.; Shu, W.; Li, M.; Li, Z.; Tao, F.; Wu, X.; Yu, Y.; Meng, H.; Vermund, S.H.; Hu, Y. Social Distancing among Medical Students during the 2019 Coronavirus Disease Pandemic in China: Disease Awareness, Anxiety Disorder, Depression, and Behavioral Activities. Int. J. Environ. Res. Public Health 2020, 17, 5047. [Google Scholar] [CrossRef]
- Özdin, S.; Özdin, S.B. Levels and predictors of anxiety, depression and health anxiety during COVID-19 pandemic in Turkish society: The importance of gender. Int. J. Soc. Psychiatry 2020, 66, 504–511. [Google Scholar] [CrossRef]
- Bäuerle, A.; Teufel, M.; Musche, V.; Weismüller, B.; Kohler, H.; Hetkamp, M.; Dörrie, N.; Schweda, A.; Skoda, E. Increased generalized anxiety, depression and distress during the COVID-19 pandemic: A cross-sectional study in Germany. J. Public Health 2020, 42, 672–678. [Google Scholar] [CrossRef]
- Nguyen, H.T.; Do, B.N.; Pham, K.M.; Kim, G.B.; Dam, H.T.B.; Nguyen, T.T.; Nguyen, T.T.P.; Nguyen, Y.H.; Sørensen, K.; Pleasant, A.; et al. Fear of COVID-19 Scale-Associations of Its Scores with Health Literacy and Health-Related Behaviors among Medical Students. Int. J. Environ. Res. Public Health 2020, 17, 4164. [Google Scholar] [CrossRef]
- Parker, G.; Brotchie, H. Gender differences in depression. Int. Rev. Psychiatry 2010, 22, 429–436. [Google Scholar] [CrossRef]
- Lancet, T. The gendered dimensions of COVID-19. Lancet 2020, 395, 1168. [Google Scholar] [CrossRef]
- Huckins, J.F.; DaSilva, A.W.; Wang, R.; Wang, W.; Hedlund, E.L.; Murphy, E.I.; Lopez, R.B.; Rogers, C.; Holtzheimer, P.E.; Kelley, W.M.; et al. Fusing Mobile Phone Sensing and Brain Imaging to Assess Depression in College Students. Front. Neurosci. 2019, 13, 248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhai, L.; Zhang, Y.; Zhang, D. Sedentary behaviour and the risk of depression: A meta-analysis. Br. J. Sports Med. 2015, 49, 705–709. [Google Scholar] [CrossRef]
- Arend, A.K.; Blechert, J.; Pannicke, B.; Reichenberger, J. Increased Screen Use on Days with Increased Perceived COVID-19-Related Confinements—A Day Level Ecological Momentary Assessment Study. Front. Public Health 2020, 8, 623205. [Google Scholar] [CrossRef]
- Dixit, A.; Marthoenis, M.; Arafat, S.M.Y.; Sharma, P.; Kar, S.K. Binge watching behavior during COVID-19 pandemic: A cross-sectional, cross-national online survey. Psychiatry Res. 2020, 289, 113089. [Google Scholar] [CrossRef] [PubMed]
- Akulwar-Tajane, I.; Parmar, K.K.; Naik, P.H.; Shah, A. Rethinking screen time during COVID-19: Impact on psychological well-being in physiotherapy students. Int. J. Clin. Exp. Med. Res. 2020, 4, 201–216. [Google Scholar] [CrossRef]
- Hartley, S.; Colas des Francs, C.; Aussert, F.; Martinot, C.; Dagneaux, S.; Londe, V.; Waldron, L.; Royant-Parola, S. The effects of quarantine for SARS-CoV-2 on sleep: An online survey. Encephale 2020, 46, S53–S59. [Google Scholar] [CrossRef]
- Shoval, D.; Tal, N.; Tzischinsky, O. Relationship of smartphone use at night with sleep quality and psychological well-being among healthy students: A pilot study. Sleep Health 2020, 6, 495–497. [Google Scholar] [CrossRef]
- Acharya, L.; Jin, L.; Collins, W. College life is stressful today—Emerging stressors and depressive symptoms in college students. J. Am. Coll. Health 2018, 66, 655–664. [Google Scholar] [CrossRef]
- Odegård, S.S.; Sand, T.; Engstrøm, M.; Stovner, L.J.; Zwart, J.A.; Hagen, K. The long-term effect of insomnia on primary headaches: A prospective population-based cohort study (HUNT-2 and HUNT-3). Headache 2011, 51, 570–580. [Google Scholar] [CrossRef]
- Ballou, S.; Alhassan, E.; Hon, E.; Lembo, C.; Rangan, V.; Singh, P.; Hirsch, W.; Sommers, T.; Iturrino, J.; Nee, J.; et al. Sleep Disturbances Are Commonly Reported Among Patients Presenting to a Gastroenterology Clinic. Dig. Dis. Sci. 2018, 63, 2983–2991. [Google Scholar] [CrossRef] [PubMed]
- Dauvilliers, Y.; Arnulf, I.; Lecendreux, M.; Charley, C.M.; Franco, P.; Drouot, X.; d’Ortho, M.P.; Launois, S.; Lignot, S.; Bourgin, P.; et al. Increased risk of narcolepsy in children and adults after pandemic H1N1 vaccination in France. Brain 2013, 136, 2486–2496. [Google Scholar] [CrossRef] [Green Version]
- Okano, K.; Kaczmarzyk, J.R.; Dave, N.; Gabrieli, J.D.E.; Grossman, J.C. Sleep quality, duration, and consistency are associated with better academic performance in college students. NPJ Sci. Learn 2019, 4, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [Green Version]
- Baglioni, C.; Battagliese, G.; Feige, B.; Spiegelhalder, K.; Nissen, C.; Voderholzer, U.; Lombardo, C.; Riemann, D. Insomnia as a predictor of depression: A meta-analytic evaluation of longitudinal epidemiological studies. J. Affect Disord. 2011, 135, 10–19. [Google Scholar] [CrossRef]
- Chen, T.; Lucock, M. The mental health of university students during the COVID-19 pandemic: An online survey in the UK. PLoS ONE 2022, 17, e0262562. [Google Scholar] [CrossRef]
- Sidor, A.; Rzymski, P. Dietary Choices and Habits during COVID-19 Lockdown: Experience from Poland. Nutrients 2020, 12, 1657. [Google Scholar] [CrossRef]
- Epel, E.; Lapidus, R.; McEwen, B.; Brownell, K. Stress may add bite to appetite in women: A laboratory study of stress-induced cortisol and eating behavior. Psychoneuroendocrinology 2001, 26, 37–49. [Google Scholar] [CrossRef]
- Ulrich-Lai, Y.M.; Fulton, S.; Wilson, M.; Petrovich, G.; Rinaman, L. Stress exposure, food intake and emotional state. Stress 2015, 18, 381–399. [Google Scholar]
- Zhang, M.; Yang, X.J. Effects of a high fat diet on intestinal microbiota and gastrointestinal diseases. World J. Gastroenterol. 2016, 22, 8905–8909. [Google Scholar] [CrossRef]
- Lassale, C.; Batty, G.D.; Baghdadli, A.; Jacka, F.; Sánchez-Villegas, A.; Kivimäki, M.; Akbaraly, T. Healthy dietary indices and risk of depressive outcomes: A systematic review and meta-analysis of observational studies. Mol. Psychiatry 2019, 24, 965–986. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Finocchi, C.; Sivori, G. Food as trigger and aggravating factor of migraine. Neurol. Sci. 2012, 33, S77–S80. [Google Scholar] [CrossRef]
- Grant, J.E.; Potenza, M.N.; Weinstein, A.; Gorelick, D.A. Introduction to behavioral addictions. Am. J. Drug Alcohol Abuse 2010, 36, 233–241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singu, S.; Acharya, A.; Challagundla, K.; Byrareddy, S.N. Impact of Social Determinants of Health on the Emerging COVID-19 Pandemic in the United States. Front. Public Health 2020, 8, 406. [Google Scholar] [CrossRef] [PubMed]
- Schimmenti, A.; Billieux, J.; Starcevic, V. The Four Horsemen of Fear: An Integrated Model of Understanding Fear Experiences during the COVID-19 Pandemic. Clin. Neuropsychiatry 2020, 17, 41–45. [Google Scholar]
- Bonabi, H.; Müller, M.; Ajdacic-Gross, V.; Eisele, J.; Rodgers, S.; Seifritz, E.; Rössler, W.; Rüsch, N. Mental Health Literacy, Attitudes to Help Seeking, and Perceived Need as Predictors of Mental Health Service Use: A Longitudinal Study. J. Nerv. Ment. Dis. 2016, 204, 321–324. [Google Scholar] [CrossRef] [Green Version]
- Czeisler, M.; Drane, A.; Winnay, S.S.; Capodilupo, E.R.; Czeisler, C.A.; Rajaratnam, S.M.; Howard, M.E. Mental health, substance use, and suicidal ideation among unpaid caregivers of adults in the United States during the COVID-19 pandemic: Relationships to age, race/ethnicity, employment, and caregiver intensity. J. Affect Disord. 2021, 295, 1259–1268. [Google Scholar] [CrossRef]
- Hong, Z.; Li, N.; Li, D.; Li, J.; Li, B.; Xiong, W.; Lu, L.; Li, W.; Zhou, D. Telemedicine during the COVID-19 Pandemic: Experiences from Western China. J. Med. Internet Res. 2020, 22, e19577. [Google Scholar] [CrossRef]
- Mortagy, Y.; Boghikian-Whitby, S.; Helou, I. An Analytical Investigation of the Characteristics of the Dropout Students in Higher Education. Available online: https://www.informingscience.org/Publications/3999 (accessed on 30 December 2018).






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographic Information | N (3533) |
| Age | |
| Median (Q1, Q3) | 22.0 (20.0, 24.0) |
| Sex | |
| F | 2086 (59.0%) |
| M | 1447 (41.0%) |
| Socio-economic status (SES) | |
| Low | 474 (13.4%) |
| Medium | 2749 (77.8%) |
| High | 310 (8.8%) |
| Condition of Social Isolation | |
| Isolation length | |
| Median (Q1, Q3) | 63.0 (56.0, 76.0) |
| Access to private garden | |
| No | 1059 (30.0%) |
| Yes | 2474 (70.0%) |
| Number of cohabitants | |
| 0–1 | 467 (13.2%) |
| 2–3 | 2176 (61.6%) |
| >3 | 890 (25.2%) |
| Number of rooms in the house | |
| <3 | 251 (7.1%) |
| 3–6 | 1556 (44.0%) |
| >6 | 1726 (48.9%) |
| Average hours spent outside on a daily basis | |
| Never | 851 (24.1%) |
| <1 h | 1575 (44.6%) |
| 1–3 h | 850 (24.1%) |
| >3 h | 257 (7.3%) |
| Average hours spent using a phone | |
| ≤3 h | 1284 (36.3%) |
| 4–6 h | 1400 (39.6%) |
| >6 h | 849 (24.0%) |
| Change in time using a phone | |
| Same/decreased | 872 (24.7%) |
| Increased | 2661 (75.3%) |
| Average hours spent using a PC | |
| ≤3 h | 1071 (30.3%) |
| 4–6 h | 1180 (33.4%) |
| >6 h | 1282 (36.3%) |
| Change in time using a PC | |
| Same/decreased | 837 (23.7%) |
| Increased | 2696 (76.3%) |
| Average hours spent playing video games | |
| Never | 2097 (59.4%) |
| <1 h | 619 (17.5%) |
| ≥1 h | 817 (23.1%) |
| Change in time playing video games | |
| Same/decreased | 2741 (77.6%) |
| Increased | 792 (22.4%) |
| Average hours spent watching TV | |
| <1 h | 1606 (45.5%) |
| 1–3 h | 1543 (43.7%) |
| >3 h | 384 (10.9%) |
| Change in time watching TV | |
| Same/decreased | 2411 (68.2%) |
| Increased | 1122 (31.8%) |
| Lifestyles | |
| Smoking status during lockdown | |
| Non-smoker | 2594 (73.4%) |
| Former smoker | 175 (5.0%) |
| Decreased | 346 (9.8%) |
| Same | 216 (6.1%) |
| Increased | 202 (5.7%) |
| Alcohol consumption during lockdown | |
| Never | 655 (18.5%) |
| Decreased | 1700 (48.1%) |
| Same | 962 (27.2%) |
| Increased | 216 (6.1%) |
| Physical activity | |
| No | 984 (27.9%) |
| Decreased | 896 (25.4%) |
| Same | 441 (12.5%) |
| Increased | 1210 (34.3%) |
| Usual sleep quality | |
| Poor | 145 (4.1%) |
| Fairly good | 717 (20.3%) |
| Good | 2196 (62.2%) |
| Excellent | 475 (13.4%) |
| Sleep quality | |
| Worsened | 1468 (41.6%) |
| Same | 1719 (48.7%) |
| Improved | 346 (9.8%) |
| Change in weight | |
| Lost weight | 878 (24.9%) |
| No | 1411 (39.9%) |
| Gained weight | 1244 (35.2%) |
| Change in nutrition | |
| Worsened | 663 (18.8%) |
| No | 1851 (52.4%) |
| Improved | 1019 (28.8%) |
| COVID-19 Information | |
| Positive for COVID-19 | |
| No/do not know | 3450 (97.7%) |
| Yes | 83 (2.3%) |
| COVID-19 symptoms | |
| No | 3075 (87.0%) |
| Yes | 458 (13.0%) |
| Relatives infected with COVID-19 | |
| No | 3316 (93.9%) |
| Yes | 217 (6.1%) |
| Relatives with COVID-19 symptoms | |
| No | 3281 (92.9%) |
| Yes | 252 (7.1%) |
| Relatives died from COVID-19 | |
| No | 3464 (98.0%) |
| Yes | 69 (2.0%) |
| Economic and Financial Situation | |
| Cohabitant unemployed because of the pandemic | |
| No | 3055 (86.5%) |
| Yes | 478 (13.5%) |
| Productivity | |
| Mnemonic difficulties | |
| No | 1863 (52.7%) |
| Yes | 1670 (47.3%) |
| Performance reduction | |
| No | 1996 (56.5%) |
| Yes | 1537 (43.5%) |
| Outcomes | N (3533) |
| Digestive disorders | |
| No | 2754 (78.0%) |
| Yes | 779 (22.0%) |
| Headache | |
| No | 1991 (56.4%) |
| Yes | 1542 (43.6%) |
| Fear of being infected by SARS-CoV-2 | |
| Low | 1081 (30.6%) |
| Medium | 1687 (47.7%) |
| High | 765 (21.7%) |
| Panic or anxiety crisis | |
| Low | 2250 (63.7%) |
| Medium | 820 (23.2%) |
| High | 463 (13.1%) |
| Sadness/depression | |
| Low | 930 (26.3%) |
| Medium | 1461 (41.4%) |
| High | 1142 (32.3%) |
| Initial Variables | Latent Variables |
|---|---|
| Average hours spent using a TV; change in time using a TV | TV usage |
| Average hours spent using a phone; change in time using a phone | Phone usage |
| Average hours spent using a PC; change in time using a PC | PC usage |
| Average hours spent playing video games; change in time playing video games | Video games usage |
| Number of rooms in the house; private garden availability; cohabitants; average hours spent outside | Lockdown conditions |
| Smoking status during lockdown; alcohol consumption during lockdown | Smoking and alcohol habits |
| Cohabitants unemployed during lockdown | Unemployed cohabitants during lockdown |
| Relatives positive for COVID-19; relatives with COVID-19 symptoms; relatives died from COVID-19 | Having had relatives positive for COVID-19, with symptoms, or deceased |
| Having been positive for COVID-19; COVID-19 symptoms | Having been positive for or with COVID-19 symptoms |
| Physical activity; change in weight; change in nutrition | Nutrition, weight change, and physical activity |
| Usual sleep quality; lockdown sleep quality; mnemonic difficulties; performance reduction | Sleep quality, mnemonic difficulties, and performance reduction |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Patrono, A.; Renzetti, S.; Manco, A.; Brunelli, P.; Moncada, S.M.; Macgowan, M.J.; Placidi, D.; Calza, S.; Cagna, G.; Rota, M.; et al. COVID-19 Aftermath: Exploring the Mental Health Emergency among Students at a Northern Italian University. Int. J. Environ. Res. Public Health 2022, 19, 8587. https://doi.org/10.3390/ijerph19148587
Patrono A, Renzetti S, Manco A, Brunelli P, Moncada SM, Macgowan MJ, Placidi D, Calza S, Cagna G, Rota M, et al. COVID-19 Aftermath: Exploring the Mental Health Emergency among Students at a Northern Italian University. International Journal of Environmental Research and Public Health. 2022; 19(14):8587. https://doi.org/10.3390/ijerph19148587
Chicago/Turabian StylePatrono, Alessandra, Stefano Renzetti, Angela Manco, Paola Brunelli, Stefanny M. Moncada, Mark J. Macgowan, Donatella Placidi, Stefano Calza, Giuseppa Cagna, Matteo Rota, and et al. 2022. "COVID-19 Aftermath: Exploring the Mental Health Emergency among Students at a Northern Italian University" International Journal of Environmental Research and Public Health 19, no. 14: 8587. https://doi.org/10.3390/ijerph19148587
APA StylePatrono, A., Renzetti, S., Manco, A., Brunelli, P., Moncada, S. M., Macgowan, M. J., Placidi, D., Calza, S., Cagna, G., Rota, M., Memo, M., Tira, M., & Lucchini, R. G. (2022). COVID-19 Aftermath: Exploring the Mental Health Emergency among Students at a Northern Italian University. International Journal of Environmental Research and Public Health, 19(14), 8587. https://doi.org/10.3390/ijerph19148587