
Development of a Tool for Measuring Ventilator-Associated Pneumonia Prevention Behaviors of Intensive Care Unit Nurses


Abstract
:1. Introduction
Aim
2. Materials and Methods
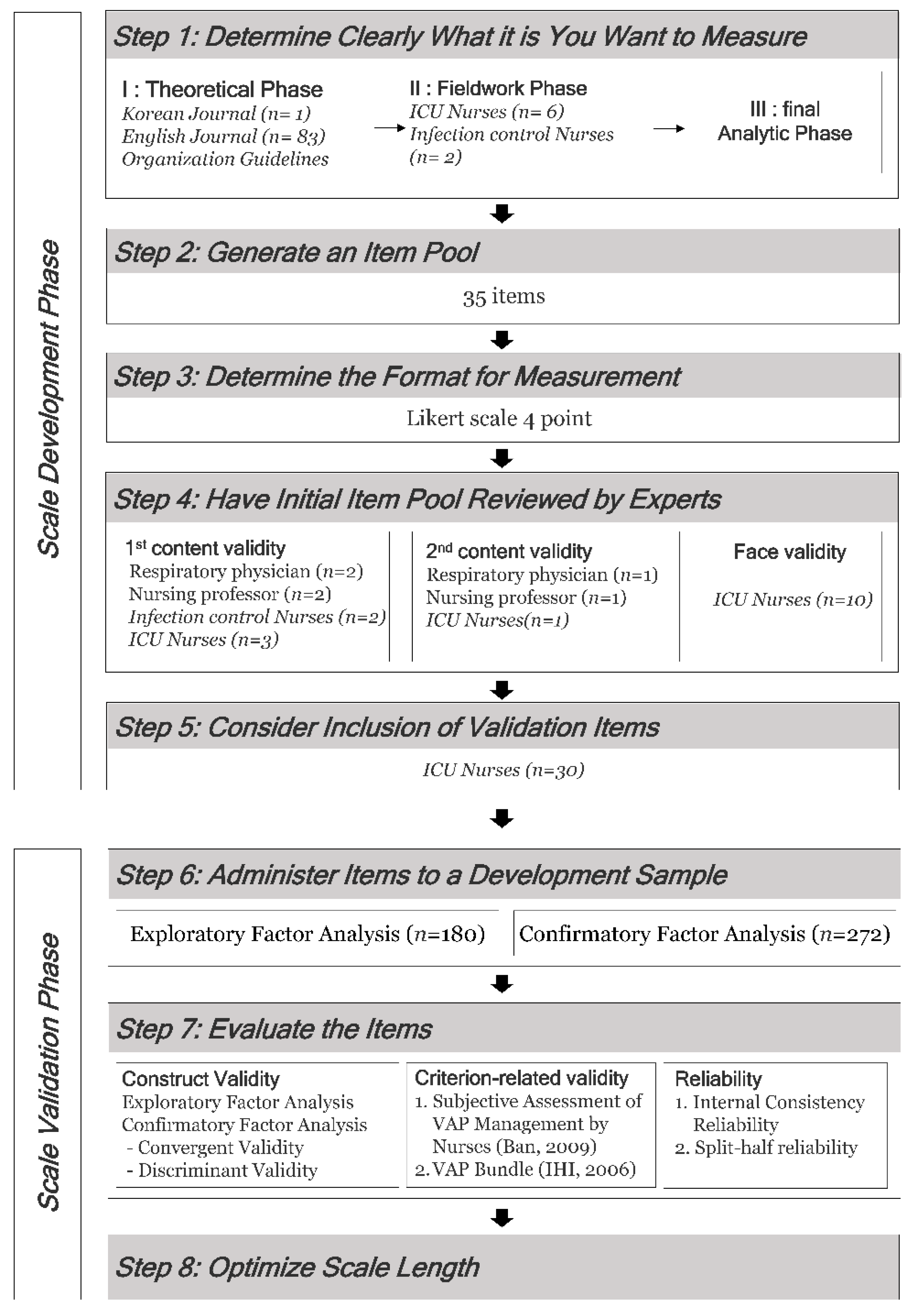
2.1. Study Design
2.2. Study Procedure
2.2.1. Phase 1: Scale Development Phase
- Step 1. Determine What You Want to Measure Clearly
- (1)
- Theoretical Phase
- (2)
- Fieldwork Phase
- (3)
- Final Analytic Phase
- Step 2. Generate an Item Pool
- Step 3. Determine the Format for Measurement
- Step 4. Have Initial Item Pool Reviewed by Experts
- (1)
- Content Validity
- (2)
- Face Validity
- Step 5. Consider the Inclusion of Validation Items
2.2.2. Phase 2: Scale Validation Phase
- Step 6. Administer Items to a Development Sample
- (1)
- Research Method
- (2)
- Subjects and Data Collection Method
- Step 7. Evaluate the Items
- (1)
- Exploratory Factor Analysis Plan
- (2)
- Criterion Analysis Plan
- (3)
- Reliability Analysis Plan
3. Results
3.1. Exploratory Factor Analysis
3.2. Confirmation Factor Analysis
3.3. Convergent Validity and Discriminant Validity
3.4. Criterion Validity Analysis
3.5. Reliability
- Step 8. Optimize Scale Length
4. Discussion
Limitation and Practical Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. VAP Preventative Behavior Measurement Tool

| No | Item | I Never Do It | I Seldom Do It | I Mostly Do It | I Always Do It |
|---|---|---|---|---|---|
| 1 | Except for contraindicated patients, elevate at an angle of 30–45 degrees the head of the bed | ① | ② | ③ | ④ |
| 2 | Cuff pressure should be maintained at 20–30 cm H2O | ① | ② | ③ | ④ |
| 3 | Regularly check and control of tracheal cuff pressure using a manual manometer | ① | ② | ③ | ④ |
| 4 | Regularly check the proper positioning of the nasogastric tube | ① | ② | ③ | ④ |
| 5 | Oral care is performed with chlorhexidine (0.12% or 2%) | ① | ② | ③ | ④ |
| 6 | Oral care is performed every 4–8 h | ① | ② | ③ | ④ |
| 7 | Perform subglottic secretion suction (subglottic secretion: oropharyngeal secretions in the subglottic region above the cuff of the endotracheal tube) | ① | ② | ③ | ④ |
| 8 | Before deflating the cuff of an endotracheal tube, before moving the tube, or patient position change ensure that secretions are cleared from above the tube cuff | ① | ② | ③ | ④ |
| 9 | Except for contraindicated patients, Daily Perform spontaneous awakening trials with sedatives turned off | ① | ② | ③ | ④ |
| 10 | Daily perform spontaneous breathing trials once a day | ① | ② | ③ | ④ |
| 11 | Change the ventilator circuit when it is visibly soiled or mechanically malfunctioning | ① | ② | ③ | ④ |
| 12 | Do not flush condensate water from the ventilator circuit into the machine or onto the patient | ① | ② | ③ | ④ |
| 13 | Use sterile water to fill ventilator humidifiers | ① | ② | ③ | ④ |
| 14 | In patients using an open suction system, use a sterile disposable suction catheter and sterile water for each suction. | ① | ② | ③ | ④ |
| 15 | In patients using an closed suction system, a closed suction catheter should be used for each new patient | ① | ② | ③ | ④ |
| 16 | Observe aseptic technique when managing the tracheostomy site and replacing the tracheostomy tube | ① | ② | ③ | ④ |
| 17 | Do not use the oxygen tube, mask, and ambu bag used for one patient on another patient. | ① | ② | ③ | ④ |
References
- Chastre, J.; Fagon, J.Y. Ventilator-associated pneumonia. Am. J. Respir. Crit. Care Med. 2002, 165, 867–903. [Google Scholar] [CrossRef] [PubMed]
- Tablan, O.C.; Anderson, L.J.; Besser, R.; Bridges, C.; Hajjeh, R. Guidelines for Preventing Healthcare Associated Pneumonia; US National Centers for Infectious Disease, MMWR 53/RR-3: Atlanta, GA, USA, 2003. [Google Scholar]
- McEnery, T.; Martin-Loeches, I. Predicting ventilator-associated pneumonia. Ann. Transl. Med. 2020, 8, 670. [Google Scholar] [CrossRef] [PubMed]
- Álvarez-Lerma, F.; Sánchez García, M. “The multimodal approach for ventilator-associated pneumonia prevention”—Requirements for nationwide implementation. Ann. Transl. Med. 2018, 6, 420. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.J.; Kwak, Y.G.; Kwak, S.H.; Ko, S.H.; Kim, J.H.; Kim, E.S.; Kim, T.H.; Ryu, S.Y.; Moon, H.; Park, S.H.; et al. Korean National Healthcare-associated Infections Surveillance System, Intensive Care Unit Module Report: Summary of Data from July 2018 to June 2019. Korean J. Healthc. Assoc. Infect. Control Prev. 2020, 25, 115–127. [Google Scholar] [CrossRef]
- Institute for Healthcare Improvement. Getting started kit: Prevent ventilator-associated pneumonia: How-to guide. Crit. Care Nurs. Q. 2006, 29, 157–173. [Google Scholar] [CrossRef] [PubMed]
- Rello, J.; Lode, H.; Cornaglia, G.; Masterton, R.; Masterton, R.; Rello, J.; Struelens, M.; Chastre, J.; Ortqvist, A.; Lode, H.; et al. A European care bundle for prevention of ventilator-associated pneumonia. Intensive Care Med. 2010, 36, 773–780. [Google Scholar] [CrossRef] [PubMed]
- Korea Center for Disease Control and Prevention. Standard Prevention Guidelines for Medical Related Infections. 2017. Available online: https://www.ksid.or.kr/board/list.html?num=2758&start=0&sort=top%20desc,thread%20desc,pos&code=pds&key=&keyword= (accessed on 22 June 2019).
- Song, J.H.; Kim, K.H. A Meta-Analysis of the Ventilator Circuit Change Period on Ventilator-Associated Pneumonia. J. Korean Clin. Nurs. Res. 2010, 16, 111–121. [Google Scholar]
- Hong, H.K.; Kim, J.S.; Cho, E.S.; Kang, Y.S.; Park, M.R.; Chang, B.K.; Hwang, K.J.; Lee, H.; Lee, K.S.; Lim, H.S. Effects of oral care using chlorhexidine gluconate on ventilator-associated pneumonia in the intensive care unit. Korean J. Nosocom. Infect. Control. 2006, 11, 129–137. [Google Scholar]
- Cha, K.S.; Park, H.R. [Endotracheal colonization and ventilator-associated pneumonia in mechanically ventilated patients according to type of endotracheal suction system]. J. Korean Acad. Nurs. 2011, 41, 175–181. [Google Scholar] [CrossRef] [Green Version]
- Seo, H.K.; Choi, E.H.; Kim, J.H. The effect of oral hygiene for ventilator-associated pneumonia (VAP) incidence. J. Korean Crit. Care Nurs. 2011, 4, 39–46. [Google Scholar]
- Marjanovic, N.; Frasca, D.; Asehnoune, K.; Paugam, C.; Lasocki, S.; Ichai, C.; Lefrant, J.Y.; Leone, M.; Dahyot-Fizelier, C.; Pottecher, J.; et al. Multicentre randomised controlled trial to investigate the usefulness of continuous pneumatic regulation of tracheal cuff pressure for reducing ventilator-associated pneumonia in mechanically ventilated severe trauma patients: The AGATE study protocol. BMJ Open 2017, 7, e017003. [Google Scholar] [CrossRef] [Green Version]
- Dat, V.Q.; Yen, L.M.; Loan, H.T.; Phu, V.D.; Binh, N.T.; Geskus, R.B.; Trinh, D.H.K.; Mai, N.T.H.; Phu, N.H.; Phu Huong Lan, N.; et al. Effectiveness of continuous endotracheal cuff pressure control for the prevention of ventilator associated respiratory infections: An open-label randomised, controlled trial. Clin. Infect. Dis. 2022, 74, 1795–1803. [Google Scholar] [CrossRef] [PubMed]
- Swain, S.K.; Jena, P.P. Role of early tracheostomy for preventing ventilator associated pneumonia in intensive care unit: A review. Int. J. Otorhinolaryngol. Head Neck Surg. 2021, 7, 1083–1088. [Google Scholar] [CrossRef]
- Wu, D.; Wu, C.; Zhang, S.; Zhong, Y. Risk Factors of Ventilator-Associated Pneumonia in Critically III Patients. Front. Pharmacol. 2019, 10, 482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jahansefat, L.; Vardanjani, M.M.; Bigdelian, H.; Massoumi, G.; Khalili, A.; Mardani, D. Exploration of knowledge of, adherence to, attitude and barriers toward evidence-based guidelines (EBGs) for prevention of ventilator-associated pneumonia (VAP) in healthcare workers of pediatric cardiac intensive care units (PCICUs): A Quali-Quantitative survey. Int. J. Med. Res. Health Sci. 2016, 5, 67–73. [Google Scholar]
- Hawe, C.S.; Ellis, K.S.; Cairns, C.J.; Longmate, A. Reduction of ventilator-associated pneumonia: Active versus passive guideline implementation. Intensive Care Med. 2009, 35, 1180–1186. [Google Scholar] [CrossRef]
- Agodi, A.; Auxilia, F.; Barchitta, M.; D’Errico, M.M.; Montagna, M.T.; Pasquarella, C.; Tardivo, S.; Mura, I. Control of intubator associated pneumonia in intensive care unit: Results of the GISIO-SItI SPIN-UTI Project. Epidemiol. Prev. 2014, 38, 51–56. [Google Scholar]
- Grol, R. Successes and failures in the implementation of evidence-based guidelines for clinical practice. Med. Care 2001, 39, II46–II54. [Google Scholar] [CrossRef]
- Grimshaw, J.M.; Shirran, L.; Thomas, R.; Mowatt, G.; Fraser, C.; Bero, L.; Grilli, R.; Harvey, E.; Oxman, A.; O’Brien, M.A. Changing provider behavior: An overview of systematic reviews of interventions. Med. Care 2001, 39, II2–II45. [Google Scholar] [CrossRef]
- Cocanour, C.S.; Peninger, M.; Domonoske, B.D.; Li, T.; Wright, B.; Valdivia, A.; Luther, K.M. Decreasing ventilator-associated pneumonia in a trauma ICU. J. Trauma 2006, 61, 122–129, discussion 129–130. [Google Scholar] [CrossRef]
- Wall, R.J.; Ely, E.W.; Elasy, T.A.; Dittus, R.S.; Foss, J.; Wilkerson, K.S.; Speroff, T. Using real time process measurements to reduce catheter related bloodstream infections in the intensive care unit. Qual. Saf. Health Care 2005, 14, 295–302. [Google Scholar] [CrossRef] [PubMed]
- Jansson, M.; Ala-Kokko, T.; Ylipalosaari, P.; Syrjälä, H.; Kyngäs, H. Critical care nurses’ knowledge of, adherence to and barriers towards evidence-based guidelines for the prevention of ventilator-associated pneumonia—A survey study. Intensive Crit. Care Nurs. 2013, 29, 216–227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- America Hospital Association. Checklists to Improve Patient Safety. 2013. Available online: https://www.aha.org/ahahret-guides/2013-07-10-checklists-improve-patient-safety (accessed on 2 November 2018).
- Kiyoshi-Teo, H.; Cabana, M.D.; Froelicher, E.S.; Blegen, M.A. Adherence to institution-specific ventilator-associated pneumonia prevention guidelines. Am. J. Crit. Care 2014, 23, 201–214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ban, K.O. The Development and Effectiveness of a Program to Prevent Ventilator Associated Pneumonia in the ICU. Korean Soc. Adult Nurs. 2009, 21, 155–166. [Google Scholar]
- Kim, K.S.; Kim, J.A.; Ahn, J.W. Development and implementation of a self-directed critical care nursing e-learning program. Perspect. Nurs. Sci. 2012, 9, 51–60. [Google Scholar]
- Lee, H.H.; Han, M.H.; Park, J.; Choi, S.W. Associated Factors with Performance of Infection Control for the Prevention of Ventilator-associated Pneumonia among Some Intensive Care Unit Nurses. J. Health. Info. Stat. 2016, 43, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.S.; Park, Y.W.; Kim, J.Y.; Lee, E.S.; Park, A.S.; Han, A.R.; Kim, E.A.; Lee, H.S.; Koh, S.O. The Effect of Backrest Elevation Education on ICU Nurse’s Knowledge, Perception and Performance. J. Korean Clin. Nurs. Res. 2008, 14, 117–128. [Google Scholar]
- Schwartz-Barcott, D. An expansion and elaboration of the hybrid model of concept development. In Concept Development in Nursing: Foundations, Techniques, and Applications; Saunders: Philadelphia, PA, USA, 2000; pp. 129–159. [Google Scholar]
- De Vellis, R.F. Scale Development: Theory and Applications, 4th ed.; SAGE Publications, Inc.: Los Angeles, CA, USA, 2017; pp. 6–262. ISBN 978-15-0634-156-9. [Google Scholar]
- American Psychological Association. Guidelines for Preventing Health-Care-Associated Pneumonia, 2003: Recommendations of CDC and the Healthcare Infection Control Practices Advisory Committee: (548652006-001). 2004. Available online: http://doi.apa.org/get-pe-doi.cfm?doi=10.1037/e548652006-001 (accessed on 22 December 2021).
- Klompas, M.; Branson, R.; Eichenwald, E.C.; Greene, L.R.; Howell, M.D.; Lee, G.; Magill, S.S.; Maragakis, L.L.; Priebe, G.P.; Speck, K.; et al. Strategies to prevent ventilator-associated pneumonia in acute care hospitals: 2014 update. Infect. Control Hosp. Epidemiol. 2014, 35 (Suppl. 2), S133–S154. [Google Scholar] [CrossRef] [Green Version]
- Rotstein, C.; Evans, G.; Born, A.; Grossman, R.; Light, R.B.; Magder, S.; McTaggart, B.; Weiss, K.; Zhanel, G.G. Clinical practice guidelines for hospital-acquired pneumonia and ventilator-associated pneumonia in adults. Can. J. Infect. Dis. Med. Microbiol. 2008, 19, 19–53. [Google Scholar] [CrossRef]
- Institute for Clinical Systems Improvement. Health Care Protocol: Prevention of Ventilator-Associated Pneumonia, 5th ed.; Institute for Clinical Systems Improvement: Bloomington, MN, USA, 2011; pp. 1–30. [Google Scholar]
- Kline, R.B. Principles and Practice of Structural Equation Modeling, 4th ed.; The Guilford Press: New York, NY, USA, 2015; pp. 188–217. ISBN 978-14-6252-334-4. [Google Scholar]
- Sung, T.J. Theory and Practice of Item Making and Analysis, 2nd ed.; Hakjisa: Seoul, Korea, 2016; pp. 272–524. ISBN 978-89-9972-038-3. [Google Scholar]
- Woo, J.P. Structural Equation Model Concept and Understanding; Hannalae Academy: Seoul, Korea, 2016; pp. 334–568. ISBN 978-89-5566-124-8. [Google Scholar]
- Browne, M.W.; Cudeck, R. Alternative ways of assessing model fit. In Testing Structural Equation Models; Bollen, K.A., Long, J.S., Eds.; Sage Publications, Inc.: Beverly Hills, CA, USA, 1993; pp. 111–135. ISBN 978-08-0394-507-4. [Google Scholar]
- Bae, B.R. Amos 24 Structural Equation Modeling; Cheonglam: Seoul, Korea, 2017; pp. 1–506. ISBN 978-89-5972-552-6. [Google Scholar]
- No, K.S. Statistical Analysis of Papers That You Know and Write Properly; Hanbit Academy: Seoul, Korea, 2019; pp. 11–460. ISBN 979-11-5664-440-8. [Google Scholar]
- McGinn, K.; Miller, R.; Ding, L.; Brevard, S.B.; Simmons, J.D.; Kahn, S. 200 Spontaneous Breathing and Awakening Trials Plus a Multimodal Sedation/Agitation Protocol Decrease Vent Days and Benzodiazepine Use in the Burn ICU. J. Burn Care Res. 2018, 39 (Suppl. 1), S66. [Google Scholar] [CrossRef]
- Bardwell, J.; Brimmer, S.; Davis, W. Implementing the ABCDE Bundle, Critical-Care Pain Observation Tool, and Richmond Agitation-Sedation Scale to Reduce Ventilation Time. AACN Adv. Crit. Care 2020, 31, 16–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, K.S.; Lee, S.M. Effects of ventilator-associated pneumonia (VAP) control education on ICU nurses’ infection control performance and incidence of pneumonia. J. Korean Crit. Care Nurs. 2010, 3, 13–22. [Google Scholar]

{kind=link}
{kind=link}

| Characteristics | Categories | Data Set EFA (n = 180) n (%) or M ± SD | Data Set CFA (n = 272) n (%) or M ± SD |
|---|---|---|---|
| Gender | Man | 22 (12.2) | 40 (14.7) |
| Woman | 158 (87.8) | 232 (85.3) | |
| Age (years) | 29.3 ± 4.90 | 28.9 ± 4.80 | |
| Level of education | College | 19 (10.6) | 27 (9.9) |
| University | 129 (71.7) | 191 (70.2) | |
| ≥Graduate | 32 (17.8) | 54 (19.8) | |
| Current work unit | MICU | 58 (32.2) | 85 (31.3) |
| SICU | 68 (37.8) | 78 (28.7) | |
| NCU | 16 (8.9) | 33 (12.1) | |
| CICU | 3 (1.7) | 8 (2.9) | |
| ECU | 32 (17.8) | 66 (24.3) | |
| Others | 3 (1.7) | 2 (0.7) | |
| Clinical career (years) | ≤1 | 16 (8.9) | 25 (9.2) |
| 1~<5 | 87 (48.3) | 139 (51.1) | |
| 5~<10 | 45 (25.0) | 78 (28.7) | |
| 10~<15 | 26 (14.4) | 22 (8.1) | |
| ≥15 | 6 (3.3) | 8 (2.9) | |
| 5.64 ± 4.33 | 5.12 ± 4.04 | ||
| Region of hospital | Seoul | 85 (37.2) | 152 (55.9) |
| Daejeon | 48 (22.8) | 86 (31.6) | |
| Gyeongsang-do | 9 (5.1) | 19 (7.2) | |
| Gyeonggi-do | 7 (3.9) | 6 (2.2) | |
| Chungcheong-do | 29 (16.1) | 6 (2.2) | |
| Jeolla-do | 2 (1.2) | 3 (1.1) | |
| Scale of Hospital (beds) | 800~899 | 124 (68.9) | 181 (66.5) |
| 900~999 | 15 (8.3) | 16 (5.9) | |
| ≥1000 | 41 (22.8) | 75 (27.6) |
| Factors | Item | Item Analysis | Factor Loading | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| M ± SD | ITC | Alpha If Item Deleted | Communality | 1 | 2 | 3 | 4 | 5 | 6 | 7 | ||
| 1. Prevention of aspiration | Q2 | 3.61 ± 0.55 | 0.42 | 0.84 | 0.71 | 0.76 | 0.10 | 0.03 | 0.22 | 0.21 | −0.11 | −0.02 |
| Q1 | 3.74 ± 0.47 | 0.41 | 0.84 | 0.72 | 0.76 | 0.14 | 0.17 | −0.20 | 0.03 | 0.15 | 0.17 | |
| Q3 | 3.43 ± 0.81 | 0.53 | 0.83 | 0.73 | 0.65 | 0.09 | −0.14 | 0.37 | 0.20 | 0.06 | 0.28 | |
| Q6 | 3.69 ± 0.61 | 0.41 | 0.84 | 0.76 | 0.60 | 0.12 | 0.42 | −0.02 | −0.11 | 0.41 | −0.13 | |
| 2. Ventilator circuit management | Q18 | 3.60 ± 0.52 | 0.42 | 0.84 | 0.74 | 0.10 | 0.81 | 0.01 | 0.20 | 0.03 | 0.15 | 0.01 |
| Q14 | 3.53 ± 0.73 | 0.50 | 0.83 | 0.74 | 0.16 | 0.81 | 0.19 | 0.06 | 0.06 | 0.03 | 0.05 | |
| Q15 | 3.63 ± 0.60 | 0.34 | 0.84 | 0.62 | 0.06 | 0.57 | −0.19 | 0.45 | 0.09 | −0.13 | 0.13 | |
| 3. Spontaneous awakening trials and spontaneous breathing trials | Q10 | 2.42 ± 1.05 | 0.51 | 0.83 | 0.79 | 0.08 | 0.11 | 0.82 | 0.16 | 0.14 | −0.06 | 0.19 |
| Q11 | 2.59 ± 0.98 | 0.44 | 0.83 | 0.74 | 0.09 | −0.03 | 0.78 | 0.24 | 0.06 | 0.04 | 0.20 | |
| 4. Subglottic suction | Q13 | 3.18 ± 0.82 | 0.47 | 0.83 | 0.70 | 0.06 | 0.15 | 0.25 | 0.76 | −0.01 | 0.17 | −0.01 |
| Q12 | 3.43 ± 0.77 | 0.43 | 0.83 | 0.61 | 0.07 | 0.25 | 0.26 | 0.67 | 0.01 | 0.10 | −0.01 | |
| 5. Suction system management | Q22 | 3.87 ± 0.36 | 0.30 | 0.84 | 0.77 | 0.09 | −0.04 | 0.08 | 0.12 | 0.82 | 0.18 | −0.15 |
| Q23 | 3.83 ± 0.48 | 0.41 | 0.84 | 0.74 | 0.15 | 0.19 | 0.09 | −0.09 | 0.79 | 0.10 | 0.13 | |
| 6. Standard precaution | Q28 | 3.90 ± 0.30 | 0.36 | 0.84 | 0.78 | 0.07 | −0.06 | 0.05 | 0.18 | 0.15 | 00.84 | 0.08 |
| Q30 | 3.79 ± 0.42 | 0.39 | 0.84 | 0.68 | 0.06 | 0.25 | −0.08 | 0.04 | 0.22 | 0.67 | 0.30 | |
| 7. Oral care | Q8 | 2.93 ± 0.92 | 0.39 | 0.84 | 0.70 | 0.20 | 0.06 | 0.09 | 0.14 | −0.07 | 0.15 | 0.77 |
| Q7 | 3.18 ± 0.82 | 0.31 | 0.84 | 0.63 | −0.02 | 0.04 | 0.27 | −0.10 | 0.04 | 0.09 | 0.73 | |
| Eigen value | 2.12 | 1.94 | 1.84 | 1.70 | 1.54 | 1.54 | 1.50 | |||||
| Explained variance (%) | 12.5 | 11.4 | 10.8 | 10.0 | 9.1 | 9.0 | 8.8 | |||||
| Cumulative variance (%) | 12.5 | 23.9 | 34.7 | 44.8 | 53.9 | 63.0 | 71.8 | |||||
| KMO (Kaiser–Meyer–Olkin) | 0.75 | |||||||||||
| Bartlett’s Sphere Formation Test | X2 = 840.75, df = 136, p < 0.000 | |||||||||||
| Fitness Index | df | GFI | AGFI | NFI | IFI | TLA | CFI | RMSEA | RMR | SRMR | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Criteria | ≥0.90 | ≥0.90 | ≥0.90 | ≥0.80 | ≥0.80 | ≥0.95 | ≤0.05 | ≤0.05 | ≤0.05 | ||
| VAP prevention | 137.8 | 98 | 0.94 | 0.91 | 0.92 | 0.97 | 0.96 | 0.97 | 0.03 | 0.01 | 0.03 |
| Factors | Item (17) | Standardized estimate (β) | Standard error (SE) | Critical ratio (C.R.) | ρ | Error variances | AVE | CR | |||
| 1. Prevention of aspiration | 1 | 0.74 | 0.10 | 0.51 | 0.81 | ||||||
| 2 | 0.70 | 0.09 | 10.33 | <0.001 | 0.13 | ||||||
| 3 | 0.68 | 0.10 | 10.11 | <0.001 | 0.15 | ||||||
| 6 | 0.75 | 0.09 | 10.99 | <0.001 | 0.11 | ||||||
| 2. Oral care | 7 | 0.85 | 0.17 | 0.61 | 0.75 | ||||||
| 8 | 0.70 | 0.13 | 6.28 | <0.001 | 0.35 | ||||||
| 3. Spontaneous awakening trials and spontaneous | 10 | 0.70 | 0.52 | 0.60 | 0.75 | ||||||
| Breathing trials | 11 | 0.84 | 0.13 | 8.47 | <0.001 | 0.26 | |||||
| 4. Subglottic suction | 12 | 0.71 | 0.25 | 0.55 | 0.75 | ||||||
| 13 | 0.77 | 0.15 | 8.01 | <0.001 | 0.26 | ||||||
| 5. Ventilator circuit management | 14 | 0.94 | 0.01 | 0.65 | 0.84 | ||||||
| 15 | 0.50 | 0.06 | 8.66 | <0.001 | 0.26 | ||||||
| 18 | 0.85 | 0.05 | 15.89 | <0.001 | 0.07 | ||||||
| 6. Suction system management | 22 | 0.95 | 0.01 | 0.79 | 0.88 | ||||||
| 23 | 0.82 | 0.08 | 12.17 | <0.001 | 0.07 | ||||||
| 7. Standard precaution | 28 | 0.84 | 0.04 | 0.60 | 0.75 | ||||||
| 30 | 0.71 | 0.09 | 9.37 | <0.001 | 0.08 | ||||||
| Factors | |||||||
|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | |
| 1. Prevention of aspiration | 0.72 † | ||||||
| 2. Oral care | 0.25 | 0.78 † | |||||
| 3. Spontaneous awakening trials and spontaneous breathing trials | 0.34 | 0.43 | 0.77 † | ||||
| 4. Subglottic suction | 0.29 | 0.22 | 0.52 | 0.75 † | |||
| 5. Ventilator management | 0.28 | 0.13 | 0.07 | 0.394 | 0.80 † | ||
| 6. Suction system management | 0.42 | 0.05 | 0.02 | 0.17 | 0.17 | 0.89 † | |
| 7. Standard precaution | 0.44 | 0.24 | 0.04 | 0.35 | 0.33 | 0.57 | 0.77 † |
| Factor A ↔ Factor B | Φ | SE | Φ − 2 × SE | Φ + 2 × SE | |||
| PA ↔ OC | 0.25 | 0.02 | 0.21 | 0.29 | |||
| PA ↔ SAT & SBT | 0.34 | 0.02 | 0.29 | 0.39 | |||
| PA ↔ SS | 0.29 | 0.02 | 0.25 | 0.33 | |||
| PA ↔ VM | 0.28 | 0.01 | 0.26 | 0.30 | |||
| PA ↔ SM | 0.42 | 0.01 | 0.40 | 0.45 | |||
| PA ↔ SP | 0.44 | 0.01 | 0.42 | 0.46 | |||
| OC ↔ SAT & SBT | 0.43 | 0.04 | 0.33 | 0.52 | |||
| OC ↔ SS | 0.22 | 0.03 | 0.15 | 0.30 | |||
| OC ↔ VM | 0.13 | 0.01 | 0.10 | 0.16 | |||
| OC ↔ SM | 0.05 | 0.01 | 0.01 | 0.08 | |||
| OC ↔ SP | 0.24 | 0.01 | 0.21 | 0.28 | |||
| SAT & SBT ↔ SS | 0.52 | 0.04 | 0.42 | 0.62 | |||
| SAT & SBT ↔ VM | 0.07 | 0.01 | 0.03 | 0.10 | |||
| SAT & SBT ↔ SM | 0.02 | 0.02 | 0.00 | 0.07 | |||
| SAT & SBT ↔ SP | 0.04 | 0.01 | 0.00 | 0.08 | |||
| SS ↔ VM | 0.39 | 0.01 | 0.36 | 0.42 | |||
| SS ↔ SM | 0.17 | 0.01 | 0.13 | 0.20 | |||
| SS ↔ SP | 0.35 | 0.01 | 0.31 | 0.38 | |||
| VM ↔ SM | 0.17 | 0.01 | 0.15 | 0.19 | |||
| VM ↔ SP | 0.33 | 0.01 | 0.32 | 0.35 | |||
| SM ↔ SP | 0.57 | 0.01 | 0.55 | 0.60 | |||
| Criteria | whether (Φ ± 2 × SE) includes 1.0 | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kwak, S.; Han, S. Development of a Tool for Measuring Ventilator-Associated Pneumonia Prevention Behaviors of Intensive Care Unit Nurses. Int. J. Environ. Res. Public Health 2022, 19, 8822. https://doi.org/10.3390/ijerph19148822
Kwak S, Han S. Development of a Tool for Measuring Ventilator-Associated Pneumonia Prevention Behaviors of Intensive Care Unit Nurses. International Journal of Environmental Research and Public Health. 2022; 19(14):8822. https://doi.org/10.3390/ijerph19148822
Chicago/Turabian StyleKwak, Sungjung, and Sujeong Han. 2022. "Development of a Tool for Measuring Ventilator-Associated Pneumonia Prevention Behaviors of Intensive Care Unit Nurses" International Journal of Environmental Research and Public Health 19, no. 14: 8822. https://doi.org/10.3390/ijerph19148822
APA StyleKwak, S., & Han, S. (2022). Development of a Tool for Measuring Ventilator-Associated Pneumonia Prevention Behaviors of Intensive Care Unit Nurses. International Journal of Environmental Research and Public Health, 19(14), 8822. https://doi.org/10.3390/ijerph19148822