
Healthy Environments: Understanding Perceptions of Underrepresented Communities in the United Kingdom

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participant Recruitment
2.1.1. Co-Creators
2.1.2. Community Hosts
2.1.3. Participants
2.2. Study Design
2.3. Data Collection
2.4. Data Analysis
2.5. Ethics Statement
3. Results
3.1. Co-Creator and Participant Characteristics
3.1.1. Co-Creator Characteristics
3.1.2. Participant Characteristics
3.2. Key Themes
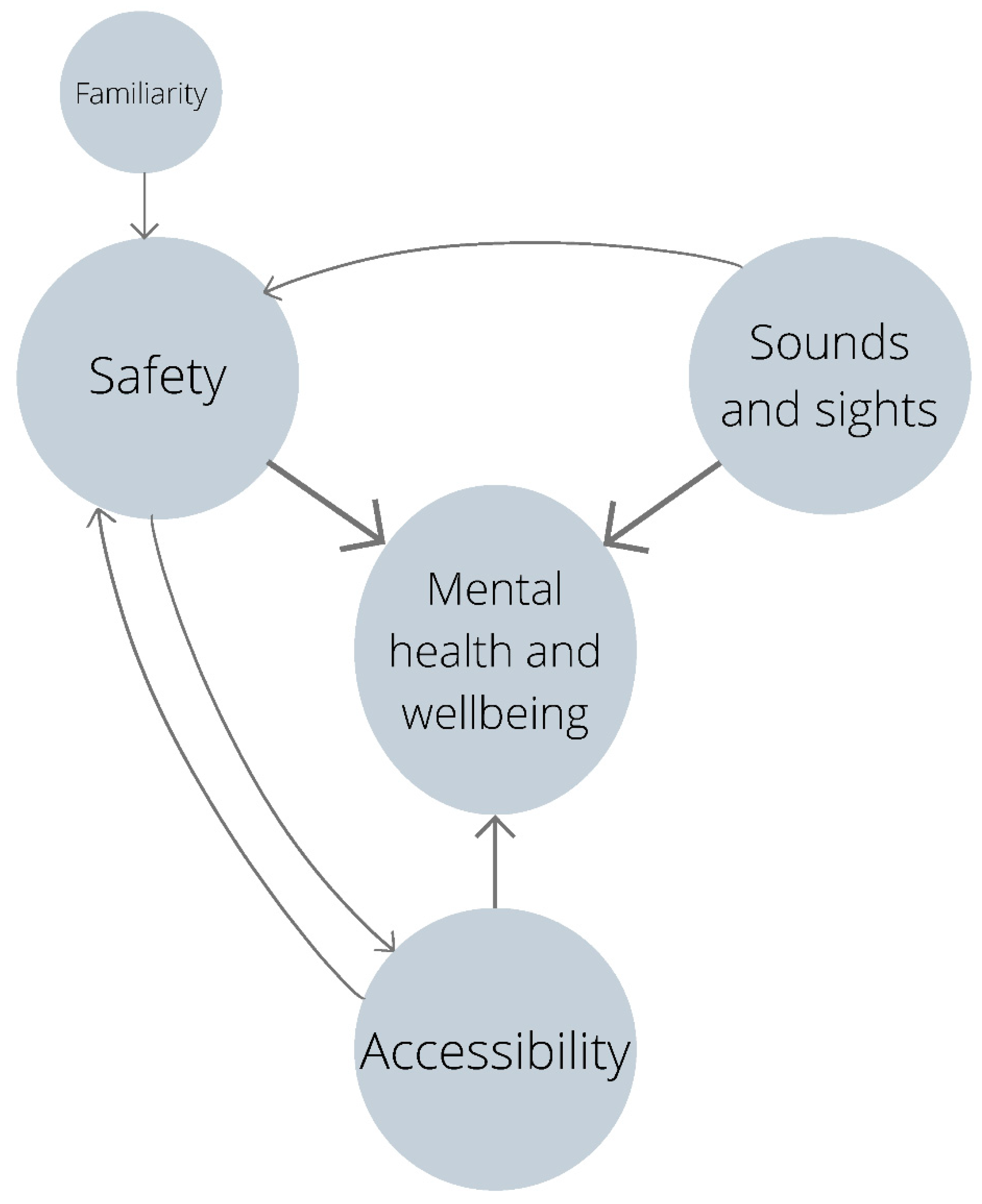
3.2.1. Sounds and Sights
“I realised the importance of the birdsong and where there was a variety of different birds singing … that kind of to me felt like it was a healthier space.”(female, urban home environment, 26–35 years old, white, self-reported disability and long-term condition)
“The idea that the sound of your environment matters, which I don’t think I paid much attention to before, but that idea that birds are important, waves are important. You know, those kind of audio inputs are important.”(female, suburban/urban fringe home environment, 26–35 years old)
“I like the sound of the birds and the lapping of the water … especially I think because I live in a crowded city.”(female, urban home environment, mixed heritage)
“It [green and blue space] kind of gives you that break away from the hectic noise from, you know, if you’re in the city.”(female, urban home environment, 18–25 years old, self-reported disability)
“The peatland bog … that felt very healthy intrinsically. I guess it’s because there was no one around. What sort of stood out to me was, they [the 360° videos] didn’t show many people. There was no traffic. So they felt a lot healthier and … wilder and more peaceful. Then in the summer … loads of people, loads of noise, a lot of traffic going through the town … which feels kind of innately unhealthy.”(female, suburban/urban fringe home environment, 18–25 years old, white)
“Cities feel very stifling … there’s cars everywhere and there’s just a lot of noise and sound. Obviously, this is probably just biased because I have asthma, so I was automatically thinking ‘Oh no’. Even if I saw the smoke blooming out, it didn’t really make me feel too comfortable.”(male, urban home environment, 18–25 years old, African)
“When I see the city [in the 360° video] … it’s not healthy at all. There’s loads of cars so pollution is definitely affecting everything … and there’s a lack of trees … there was only one type of shrub that I felt was just there for decoration.”(female, urban home environment, 18–25 years old, African)
“I’ve lived mostly in the inner city most of my life. And in terms of the videos, I felt most connected when I could hear the birds tweeting … Even though I live in an inner-city area, I really felt disconnected when I heard other noises [from the urban areas].”(female, urban home environment, Asian)
“When we see the areas that we live in, you know, with all the traffic and stuff, that is what we see day to day. But then when you go out into the countryside, it’s really powerful. And you can breathe, and you can hear stuff. You can literally hear things, you know, birds and animals. In the city, all you hear is horns and cars and trucks. So it’s a bit depressing.”(male, urban home environment, Asian)
3.2.2. Accessibility
“I was thinking of our town centre and we’ve got some trees there. And it [the small urban green space video] reminded me of that, and how lucky we are that there are trees in some of the shopping areas that we have in our city.”(female, coastal home environment, Asian)
“I had mixed reactions … it was beautiful, but that reaction was followed quickly with sadness and a sense of exclusion, because there’s likely no chance of getting to similar places in a wheelchair.”(female, urban home environment, 26–35 years old, white, self-reported disability and long-term condition)
“I noticed on the bog one … it had a nice accessible-looking boardwalk which is a really big deal in those kinds of areas, you know, otherwise they’re impossible.”(female, urban home environment, 26–35 years old, white, self-reported disability and long-term condition)
“So accessible green and blue spaces … I use a wheelchair. And I think that if places are more accessible to people with disabilities, then they are more accessible to the average non-disabled person as well. And if you can get people into these spaces, they’re more likely to care.”(female, urban home environment, 26–35 years old, white, self-reported disability and long-term condition)
“It would be lovely to live away from the hustle and bustle of the busy areas that we are in, but we need a transport system.”(female, coastal home environment, Asian)
“I realised that actually a healthy space and an urban environment … they aren’t mutually exclusive. You can kind of have both … when the 360° angle was kind of centred on the green space, I had a more in-depth look and realised that, despite the environment being in a city environment, in some cases, they were actually still healthy, which initially I kind of dismissed.”(male, suburban/urban fringe home environment, 18–25 years old, Asian)
3.2.3. Familiarity
“I’m quite a coastal person myself because my homeland is near the coast … so I love the water.”(female, urban home environment, Asian)
“I really liked the lakes … that is one of my picks…I felt like it connected back to my homeland … you know like some of these hilly areas”(female, rural home environment, Asian)
“I’m from a countryside background. So it’s more familiar … when you’re familiar, you tend to be more safe”(male, 18–25 years old, suburban/urban fringe home environment)
“I know the urban coastal area will have problems with pollution, I just know it. You can’t see it in the video, but I know that to be the case because the boats discharge and the fishing industry discharges as well, so they’re bound to.”(Female, suburban/urban fringe home environment, white, self-reported long-term condition)
“When it came to the seafront or coastal views, it was unfamiliar and very quiet. And if I were in that space, I wouldn’t really know how to navigate it. And feel really unsafe in that space as well.”(Female, urban home environment, 18–25 years old, African)
3.2.4. Safety
“I like urban green spaces because I like people around, and I feel safer with people around.”(female, suburban/urban fringe home environment, white, self-reported disability and long-term condition)
“I love the countryside, but also know that I’m probably not going to see another black or brown person and feel people are looking at me. Whereas in the city I very much enjoy the feeling of just walking around and feeling, you know, blending in …”(female, mixed heritage)
“It probably is not a physically healthy space pollution-wise, but I always feel safest in the city.”(female, urban home environment, 36–45 years old, white, self-reported disability and long-term condition)
“I like to go there [the city] for work, and then come back, but I like to leave that behind. I think when you have kids … you like to come back to somewhere that you feel like they are safe in terms of, you know, the green space, and then the pollution as well.”(female, urban home environment, 36–45 years old, African)
“You know that the industry one … with the lorries and the traffic. It kind of made me feel unsafe … it just didn’t feel comfortable”(female, urban home environment, 36–45 years old, white, self-reported disability and long-term condition)
“The industrial side … the quality of the air could be a lot worse … there’ll be more pollution, and it might not be as healthy for you as, say, you lived and worked in a rural environment.”(female, 18–25 years old, White and Asian)
3.2.5. Mental Wellbeing
“I think they’ve [open green and blue spaces] had such an impact on my mental health so positively.”(male, suburban/urban fringe home environment, 18–25 years old, Asian)
“I realised my mental health is much better when I’m in Bangor, even though it is boring and there’s not much to do. But I can go out and see the golf course; I can go to Bangor Mountain; I can go to the pier and seeing all that greenery, the water, the birds. It does something to me mentally.”(female, urban home environment, self-reported disability)
“Being out in a green space really helped my mental health. Where I live, it’s quite green, quite quiet. It’s not urban at all. And when I go to university in London it’s really overwhelming for me.”(female, 18–25 years old)
“You could see for a good few hundred metres … even if it was an urban environment, as long as you weren’t kind of closed in by buildings and stuff like that … as long as you feel you have some kind of space in front of you, then it can lead to a person feeling more relaxed and, in turn, maybe being slightly more healthy.”(male, urban home environment, 36–45 years old, self-reported long-term condition)
“I was feeling a bit stressed at work. So after, you know, I’m going to log off, and get my bicycle. And I’ll just go around for 30 min. And I felt great … just looking at the green spaces, taking it all in … I felt refreshed. So it’s something like that. Just having that peace around and feeling safe.”(female, urban home environment, 36–45 years old, Asian)
“That’s why they’re [mosques and churches] important because that’s how you form community and shared values. Different studies talk about how some sense of spirituality keeps people happy in life, just being able to connect, whether it’s to your surroundings or to what you believe to be a higher power.”(male, urban home environment, African)
“Like community gardens, I think that’s also not just good for the environment, but it has an impact on mental health because you can go, and you can have your chill out time. You can speak to people, you can socialise.”(female, rural home environment, 26–35 years old, white)
“Inclusive community … in terms of healthy space … without everybody being included and being recognised, I think that spaces become negative because … there’s the psychological impact of being stressed, of being unable to communicate, to change. People are less likely to be aggressive or … domestic violence and things like that are reduced … and also depression—if there’s things for them to do and communities to go to …”(female, urban home environment, white, self-reported disability and long-term condition)
“My feelings changed about what a healthy environment was … I started off with what makes me feel nicest, what I prefer … like accessibility, public transport … but then I remember my impression of the peatland bog [in the 360° video] is very healthy because there’s lots of insects, lots of life and rotten things … but that doesn’t mean that it was my favourite place … so maybe a healthy environment isn’t just about how I feel about being there.”(female, mixed heritage)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Activity | Detail |
|---|---|
| Community host introduces self, the focus of the session, and gives participants the opportunity to introduce themselves. | Talking points:
|
| Community host facilitates icebreaker | Please say your name, location, and 3 words to describe the environment you live in |
| Community host leads a conversation on the group’s reflections after watching the 360 videos (before the workshop). | What did you like about the spaces you saw in the 360 Virtual Reality videos? What didn’t you like? Why? How did these spaces make you feel? If you could live in any of the 360 spaces presented, which would be your first choice? And your last choice? Why? Has your view of a healthy space changed after exploring the 360 spaces? Why? |
References
- World Health Organization Europe. Environment and Health Risks: A Review of the Influence and Effects of Social Inequalities. 2010. Available online: https://www.euro.who.int/__data/assets/pdf_file/0003/78069/E93670.pdf (accessed on 20 April 2022).
- UNICEF. Healthy Environments for Healthy Children: Global Programme Framework. 2021. Available online: https://www.unicef.org/documents/healthy-environments-healthy-children-global-programme-framework (accessed on 20 April 2022).
- United Nations. The 17 Sustainable Development Goals. 2015. Available online: https://sdgs.un.org/goals (accessed on 20 April 2022).
- Office of Disease Prevention and Health Promotion. Environmental Quality. 2020. Available online: https://www.healthypeople.gov/2020/leading-health-indicators/2020-lhi-topics/Environmental-Quality (accessed on 20 April 2022).
- Prüss-Ustün, A.; Wolf, J.; Corvalán, C.; Bos, R.; Neira, M. Preventing Disease through Healthy Environments: A Global Assessment of the Burden of Disease from Environmental Risks; World Health Organization: Geneva, Switzerland, 2016; Available online: https://www.who.int/publications/i/item/9789241565196 (accessed on 20 April 2022).
- Sharifi, F.; Nygaard, A.; Stone, W. Heterogeneity in the subjective well-being impact of access to urban green space. Sustain. Cities Soc. 2021, 74, 103244. [Google Scholar] [CrossRef]
- NHS. Health and the Environment. Available online: https://www.longtermplan.nhs.uk/online-version/appendix/health-and-the-environment/ (accessed on 20 April 2022).
- Orban, E.; McDonald, K.; Sutcliffe, R.; Hoffmann, B.; Fuks, K.B.; Dragano, N.; Viehmann, A.; Erbel, R.; Jöckel, K.-H.; Pundt, N.; et al. Residential Road Traffic Noise and High Depressive Symptoms after Five Years of Follow-up: Results from the Heinz Nixdorf Recall Study. Environ. Health Perspect. 2016, 124, 578–585. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coldwell, D.F.; Evans, K.L. Visits to urban green-space and the countryside associate with different components of mental well-being and are better predictors than perceived or actual local urbanisation intensity. Landsc. Urban Plan. 2018, 175, 114–122. [Google Scholar] [CrossRef]
- Public Health England. Mental Health and Wellbeing: JSNA Toolkit. Mental Health: Environmental Factors. 2019. Available online: https://www.gov.uk/government/publications/better-mental-health-jsna-toolkit/2-understanding-place (accessed on 20 April 2022).
- Lovell, B.; Depledge, M.; Maxwell, S. Health and the Natural Environment: A Review of Evidence, Policy, Practice and Opportunities for the Future. 2018. Available online: https://beyondgreenspace.files.wordpress.com/2018/09/health-and-the-natural-environment_full-report.pdf (accessed on 26 July 2022).
- Pulido-Salgado, M.; Mena, F.A.C. Bringing Policymakers to Science through Communication: A Perspective from Latin America. Front. Res. Metr. Anal. 2021, 6, 654191. [Google Scholar] [CrossRef]
- Intergovernmental Panel on Climate Change (IPCC). Climate Change: Widespread, Rapid, and Intensifying. 2021. Available online: https://www.ipcc.ch/2021/08/09/ar6-wg1-20210809-pr/ (accessed on 20 April 2022).
- Healy, N.; Barry, J. Politicizing energy justice and energy system transitions: Fossil fuel divestment and a “just transition”. Energy Policy 2017, 108, 451–459. [Google Scholar] [CrossRef] [Green Version]
- International Labour Organization. Guidelines for a Just Transition towards Environmentally Sustainable Economics and Societies for All. 2015. Available online: https://www.ilo.org/wcmsp5/groups/public/---ed_emp/---emp_ent/documents/publication/wcms_432859.pdf (accessed on 20 April 2022).
- World Health Organization. Healthy villages: A Guide for Communities and Community Health. Available online: https://www.who.int/publications/i/item/9241545534 (accessed on 20 April 2022).
- Williams, T.; Logan, T.M.; Zuo, C.T.; Liberman, K.D.; Guikema, S.D. Parks and safety: A comparative study of green space access and inequity in five US cities. Landsc. Urban Plan. 2020, 201, 103841. [Google Scholar] [CrossRef]
- Rigolon, A.; Browning, M.H.E.M.; Lee, K.; Shin, S. Access to Urban Green Space in Cities of the Global South: A Systematic Literature Review. Urban Sci. 2018, 2, 67. [Google Scholar] [CrossRef] [Green Version]
- Natural England. Monitor of Engagement with the Natural Environment: The national Survey on People and the Natural Environment. 2019. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/828552/Monitor_Engagement_Natural_Environment_2018_2019_v2.pdf (accessed on 20 April 2022).
- Horton, J. Disabilities, urban natures and children’s outdoor play. Soc. Cult. Geogr. 2016, 18, 1152–1174. [Google Scholar] [CrossRef] [Green Version]
- Anderson, L.; Heyne, L. A Statewide Needs Assessment Using Focus Groups: Perceived Challenges and Goals in Providing Inclusive Recreation Services in Rural Communities. J. Park Recreat. Admin. 2000, 18, 17–37. [Google Scholar]
- Eftekhari, M.B.; Falahat, K.; Dejman, M.; Forouzan, A.S.; Afzali, H.M.; Heidari, N.; Mirabzadeh, A. The Main Advantages of Community Based Participatory Health Programs: An Experience from the Islamic Republic of Iran. Glob. J. Health Sci. 2013, 5, 28–33. [Google Scholar] [CrossRef] [Green Version]
- Israel, B.A.; Coombe, C.M.; Cheezum, R.R.; Schulz, A.J.; McGranaghan, R.J.; Lichtenstein, R.; Reyes, A.G.; Clement, J.; Burris, A. Community-Based Participatory Research: A Capacity-Building Approach for Policy Advocacy Aimed at Eliminating Health Disparities. Am. J. Public Health 2010, 100, 2094–2102. [Google Scholar] [CrossRef] [PubMed]
- Song, H.; Lewis, N.A.; Ballew, M.T.; Bravo, M.; Davydova, J.; Gao, H.O.; Garcia, R.J.; Hiltner, S.; Naiman, S.M.; Pearson, A.R.; et al. What counts as an “environmental” issue? Differences in issue conceptualization by race, ethnicity, and socioeconomic status. J. Environ. Psychol. 2020, 68, 101404. [Google Scholar] [CrossRef]
- Bowleg, L. Evolving Intersectionality Within Public Health: From Analysis to Action. Am. J. Public Health 2021, 111, 88–90. [Google Scholar] [CrossRef] [PubMed]
- Alvidrez, J.; Greenwood, G.L.; Johnson, T.L.; Parker, K.L. Intersectionality in Public Health Research: A View from the National Institutes of Health. Am. J. Public Health 2021, 111, 95–97. [Google Scholar] [CrossRef] [PubMed]
- Broomfield, K.; Craig, C.; Smith, S.; Jones, G.; Judge, S.; Sage, K. Creativity in public involvement: Supporting authentic collaboration and inclusive research with seldom heard voices. Res. Involv. Engagm. 2021, 7, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Yonas, M.A.; Burke, J.G.; Rak, K.; Bennett, A.; Kelly, V.; Gielen, A.C. A Picture’s Worth a Thousand Words: Engaging Youth in CBPR Using the Creative Arts. Prog. Community Health Partnersh. Res. Educ. Action 2009, 3, 349–358. [Google Scholar] [CrossRef]
- Gray, N.; de Boehm, C.O.; Farnsworth, A.; Wolf, D. Integration of Creative Expression Into Community-Based Participatory Research and Health Promotion with Native Americans. Fam. Community Health 2010, 33, 186–192. [Google Scholar] [CrossRef] [Green Version]
- Shea, J.M.; Poudrier, J.; Thomas, R.; Jeffery, B.; Kiskotagan, L. Reflections from a Creative Community-Based Participatory Research Project Exploring Health and Body Image with First Nations Girls. Int. J. Qual. Methods 2013, 12, 272–293. [Google Scholar] [CrossRef] [Green Version]
- Diversity UK. Diversity in the UK. 2017. Available online: https://diversityuk.org/diversity-in-the-uk/ (accessed on 26 July 2022).
- Department for Work & Pensions. Family Resources Survey: Financial year 2020 to 2021. 2022. Available online: https://www.gov.uk/government/statistics/family-resources-survey-financial-year-2020-to-2021/family-resources-survey-financial-year-2020-to-2021#disability-1 (accessed on 26 July 2022).
- Ministry of Housing, Communities and Local Government. People living in Deprived Neighbourhoods. 2020. Available online: https://www.ethnicity-facts-figures.service.gov.uk/uk-population-by-ethnicity/demographics/people-living-in-deprived-neighbourhoods/latest#download-the-data (accessed on 26 July 2022).
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [Green Version]
- Braun, V.; Clarke, V. Thematic analysis. In APA Handbook of Research Methods in Psychology, Vol. 2. Research Designs: Quantitative, Neuropsychological, and Biological; Cooper, H., Camic, P.M., Long, D.L., Panter, A.T., Rindskopf, D., Sher, K.J., Eds.; American Psychological Association: Washington, DC, USA, 2012; pp. 57–71. [Google Scholar] [CrossRef]
- Hsieh, H.-F.; Shannon, S.E. Three Approaches to Qualitative Content Analysis. Qual. Health Res. 2005, 15, 1277–1288. [Google Scholar] [CrossRef]
- National Institute for Health Research. Policy on Payment of Fees and Expenses for Members of the Public Actively Involved with INVOLVE. 2016. Available online: https://www.invo.org.uk/wp-content/uploads/2016/05/INVOLVE-internal-payment-policy-2016-final-1.pdf (accessed on 20 April 2022).
- Thompson, S.; Fisher, H.; Dewa, L.; Hussain, T.; Kabba, Z.; Toledano, M. Adolescents’ thoughts and feelings about the local and global environment: A qualitative interview study. Child Adolesc. Ment. Health 2021, 27, 4–13. [Google Scholar] [CrossRef] [PubMed]
- Buxton, R.T.; Pearson, A.L.; Allou, C.; Fristrup, K.; Wittemyer, G. A synthesis of health benefits of natural sounds and their distribution in national parks. Proc. Natl. Acad. Sci. USA 2021, 118, e2013097118. [Google Scholar] [CrossRef] [PubMed]
- Bell, S.; Phoenix, C.; Lovell, R.; Wheeler, B. Seeking everyday wellbeing: The coast as a therapeutic landscape. Soc. Sci. Med. 2015, 142, 56–67. [Google Scholar] [CrossRef] [PubMed]
- Dzhambov, A.; Dimitrova, D. Urban green spaces’ effectiveness as a psychological buffer for the negative health impact of noise pollution: A systematic review. Noise Health 2014, 16, 157–165. [Google Scholar] [CrossRef]
- Van Kempen, E.; Babisch, W. The quantitative relationship between road traffic noise and hypertension: A meta-analysis. J. Hypertens. 2012, 30, 1075–1086. [Google Scholar] [CrossRef] [Green Version]
- The Economist Intelligence Unit. Safe Cities Index 2021. 2021. Available online: https://safecities.economist.com/wp-content/uploads/2021/09/Safe-Cities-Index-2021_eng.pdf (accessed on 20 April 2022).
- Banks, M. Using Visual Data in Qualitative Research; Sage: London, UK, 2018. [Google Scholar]
- Public Health England. A Guide to Community-Centered Approaches for Health and Wellbeing. 2015. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/768979/A_guide_to_community-centred_approaches_for_health_and_wellbeing__full_report_.pdf (accessed on 20 April 2022).
- Verschuere, B.; Brandsen, T.; Pestoff, V. Co-production: The State of the Art in Research and the Future Agenda. Volunt. Int. J. Volunt. Nonprofit Organ. 2012, 23, 1083–1101. [Google Scholar] [CrossRef] [Green Version]
- HM Treasury. Net Zero Review: Analysis Exploring the Key Issues. 2021. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1026725/NZR_-_Final_Report_-_Published_version.pdf (accessed on 20 April 2022).
- Climate Assembly UK. The Path to Net Zero. House of Commons. 2020. Available online: https://www.climateassembly.uk/report/read/final-report.pdf (accessed on 20 April 2022).
- Mackenzie, J.S.; Jeggo, M. The One Health Approach—Why Is It So Important? Trop. Med. Infect. Dis. 2019, 4, 88. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. One Health. 2017. Available online: https://www.who.int/news-room/questions-and-answers/item/one-health (accessed on 20 April 2022).
- World Health Organization. Healthy Environments: Why Do They Matter and What Can We Do? 2019. Available online: https://www.who.int/publications/i/item/healthy-environments-why-do-they-matter-and-what-can-we-do (accessed on 20 April 2022).

| Co-Creator Characteristic | Count/6 | |
|---|---|---|
| Age | 16–25 | 3 |
| 26–45 | 1 | |
| 46–65 | 2 | |
| Gender | Female | 4 |
| Male | 2 | |
| Ethnicity | White | 3 |
| White Irish | 1 | |
| White Other | 1 | |
| Pakistani | 1 | |
| Country of residence | England | 4 |
| Northern Ireland | 1 | |
| Scotland | 1 | |
| Home environment | Urban | 2 |
| Rural | 2 | |
| Urban fringe | 1 | |
| Coastal | 1 | |
| Disability | Yes | 1 |
| No | 5 |
| Participant Characteristic | Count/95 (%) | |
|---|---|---|
| Age | 16–25 | 26 (27%) |
| 26–45 | 50 (53%) | |
| 46–65 | 14 (15%) | |
| 66–75 | 5 (5%) | |
| Gender | Female | 58 (61%) |
| Male | 36 (38%) | |
| Non-binary | 1 (1%) | |
| Ethnicity | White | 34 (36%) |
| African | 20 (21%) | |
| Bangladeshi | 15 (16%) | |
| Mixed | 6 (6%) | |
| Pakistani | 6 (6%) | |
| Indian | 5 (5%) | |
| White Irish | 3 (3%) | |
| Kashmiri | 2 (2%) | |
| Asian (Other) | 1 (1%) | |
| Arabic | 1 (1%) | |
| Malay | 1 (1%) | |
| Country of residence | England | 75 (79%) |
| Scotland | 10 (10.5%) | |
| Wales | 10 (10.5%) | |
| Home environment | Urban | 60 (63%) |
| Urban fringe | 22 (23%) | |
| Rural | 8 (8%) | |
| Coastal | 5 (5%) | |
| Index of Multiple Deprivation (IMD)—1 is most deprived decile; 10 is least deprived decile | 1 | 13 (15%) |
| 2 | 10 (12%) | |
| 3 | 9 (11%) | |
| 4 | 13 (15%) | |
| 5 | 5 (6%) | |
| 6 | 11 (13%) | |
| 7 | 8 (9%) | |
| 8 | 9 (11%) | |
| 9 | 3 (4%) | |
| 10 | 4 (5%) | |
| Disability | Yes | 28 (29%) |
| No | 63 (66%) | |
| Prefer not to say | 4 (4%) | |
| Caring responsibilities | Yes | 24 (25%) |
| No | 69 (73%) | |
| Prefer not to say | 2 (2%) |
| Theme | Description | Example Quotes |
|---|---|---|
| Sounds and sights | Green space and birdsong were sensory aspects that made an environment seem healthier; environments without greenery and with sounds of road traffic were perceived as less healthy. | “I realised the importance of the birdsong and where there was a variety of different birds singing … that kind of to me felt like it was a healthier space.” “When I see the city [in the 360° video] … it’s not healthy at all. There’s loads of cars so pollution is definitely affecting everything … and there’s a lack of trees … there was only one type of shrub that I felt was just there for decoration.” |
| Accessibility | Geographical and logistical accessibility were important aspects of a healthy environment. The former relates to the proximity, such as of nature, to communities; the latter is about physical aspects of an environment that can make it more or less accessible to certain communities. Logistical accessibility was of particular concern to participants with physical disabilities whose access to certain environments can be limited by physical barriers. | “It would be lovely to live away from the hustle and bustle of the busy areas that we are in, but we need a transport system.” “I had mixed reactions … it was beautiful, but that reaction was followed quickly with sadness and a sense of exclusion, because there’s likely no chance of getting to similar places in a wheelchair.” |
| Familiarity | Familiarity moderated the strength of the link between safety and healthy environments. Environments that were most familiar to participants were often where they felt safest. Hence these environments improved mental health and wellbeing and were considered healthier than unfamiliar environments. | “I’m from a countryside background. So it’s more familiar … when you’re familiar, you tend to be more safe” “When it came to the seafront or coastal views, it was unfamiliar and very quiet. And if I were in that space, I wouldn’t really know how to navigate it. And feel really unsafe in that space as well.” |
| Safety | The link between safety and healthy environments was perceived in three respects: healthy air, reduced risk of physical harm from accidents (e.g., road traffic accidents), and freedom from physical violence. These aspects were seen to compete with each other by some participants who, for instance, felt safer from physical violence in cities where the air is less healthy. | “I like urban green spaces because I like people around, and I feel safer with people around” “The industrial side … the quality of the air could be a lot worse … there’ll be more pollution, and it might not be as healthy for you as, say, you lived and worked in a rural environment.” |
| Mental health and wellbeing | Mental health and wellbeing was often cited as a primary outcome that a healthy environment can have for people. Often, when referring to a ‘healthy environment’, participants reflected on the benefits to their mental health and wellbeing. | “Being out in a green space really helped my mental health. Where I live, it’s quite green, quite quiet. It’s not urban at all. And when I go to university in London it’s really overwhelming for me.” “You could see for a good few hundred metres … even if it was an urban environment, as long as you weren’t kind of closed in by buildings and stuff like that … as long as you feel you have some kind of space in front of you, then it can lead to a person feeling more relaxed and, in turn, maybe being slightly more healthy.” |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Roberts, L.F.; Lounsbury, O.; Awuzudike, V.; Jennings, N.; Lawrance, E.L. Healthy Environments: Understanding Perceptions of Underrepresented Communities in the United Kingdom. Int. J. Environ. Res. Public Health 2022, 19, 9643. https://doi.org/10.3390/ijerph19159643
Roberts LF, Lounsbury O, Awuzudike V, Jennings N, Lawrance EL. Healthy Environments: Understanding Perceptions of Underrepresented Communities in the United Kingdom. International Journal of Environmental Research and Public Health. 2022; 19(15):9643. https://doi.org/10.3390/ijerph19159643
Chicago/Turabian StyleRoberts, Lily F., Olivia Lounsbury, Veronica Awuzudike, Neil Jennings, and Emma L. Lawrance. 2022. "Healthy Environments: Understanding Perceptions of Underrepresented Communities in the United Kingdom" International Journal of Environmental Research and Public Health 19, no. 15: 9643. https://doi.org/10.3390/ijerph19159643
APA StyleRoberts, L. F., Lounsbury, O., Awuzudike, V., Jennings, N., & Lawrance, E. L. (2022). Healthy Environments: Understanding Perceptions of Underrepresented Communities in the United Kingdom. International Journal of Environmental Research and Public Health, 19(15), 9643. https://doi.org/10.3390/ijerph19159643