
Are Organizational Interventions Effective in Protecting Healthcare Worker Mental Health during Epidemics/Pandemics? A Systematic Literature Review

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search
2.2. Study Eligibility and Exclusion
2.3. Methodologic Quality Assessment of Individual Studies
2.4. Data Extraction and Analysis
2.5. Evidence Synthesis
3. Results
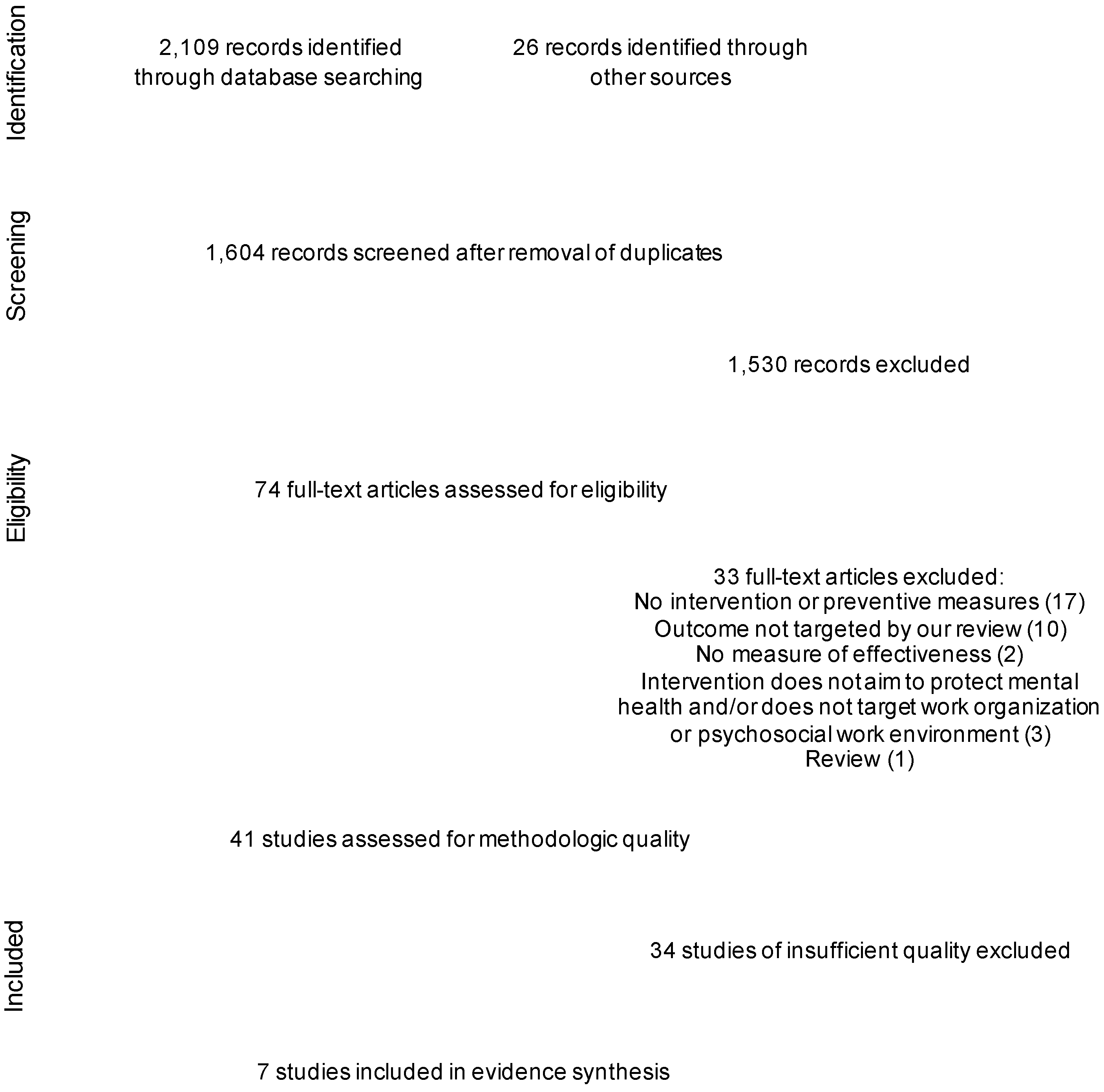
3.1. Identification and Selection of Studies
3.2. Methodologic Quality of Individual Studies
3.3. Description of Analyzed Studies and Interventions

{kind=link}
| Studies | Items 1 | Study Score | Study Quality 2 | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | /30 | % | ||
| Zaghini et al. 2021 [45] | 2 | 0 | 2 | 2 | 1.5 | 2 | 1.5 | 2 | 2 | 2 | 2 | 1.5 | 1 | 0 | 1 | 22.5 | 75.0 | M |
| Giordano et al. 2021 [44] | 2 | 0 | 1.5 | 1.5 | 1.5 | 2 | 1 | 2 | 0 | 2 | 2 | 2 | 0.5 | 0 | 1 | 19.0 | 63.3 | M |
| Chen et al. 2006 [19] | 2 | 0 | 1.5 | 1 | 0 | 2 | 1.5 | 2 | 0 | 2 | 2 | 1 | 1.5 | 0 | 1 | 17.5 | 58.3 | M |
| Maunder et al. 2006 [47] | 2 | 1 | 2 | 1 | 1 | 1 | 2 | 2 | 1.5 | 0 | 0 | 0.5 | 1.5 | 0 | 2 | 17.5 | 58.3 | M |
| Zhu et al. 2020 [46] | 2 | 1 | 1.5 | 1 | 0.5 | 1 | 1.5 | 1 | 2 | 0 | 0 | 1.5 | 2 | 0.5 | 1.5 | 17.0 | 56.7 | M |
| Beneria et al. 2020 [42] | 2 | 1 | 1 | 1 | 1 | 1 | 1 | 2 | 1 | 0.5 | 0 | 2 | 1 | 0.5 | 0.5 | 15.5 | 51.7 | M |
| Blake et al. 2020 [43] | 2 | 1 | 1 | 1 | 0.5 | 1 | 1.5 | 2 | 0.5 | 0 | 0 | 2 | 1 | 1 | 1 | 15.5 | 51.7 | M |
| Chen et al. 2021 | 2 | 0 | 1.5 | 1 | 1.5 | 1 | 1.5 | 0.5 | 0.5 | 0 | 0 | 0.5 | 2 | 1 | 2 | 15.0 | 50.0 | L |
| Cyr et al. 2021 | 2 | 1 | 2 | 1 | 1 | 1 | 1.5 | 1 | 0 | 0 | 0 | 0.5 | 2 | 0.5 | 1.5 | 15.0 | 50.0 | L |
| Smith et al. 2020 | 2 | 1 | 1.5 | 1 | 1 | 1 | 1.5 | 0.5 | 0.5 | 0 | 0 | 0.5 | 1.5 | 1 | 2 | 15.0 | 50.0 | L |
| Arnetz et al. 2020 | 2 | 1 | 1 | 1 | 1 | 1 | 2 | 1 | 0.5 | 0 | 0 | 0.5 | 1.5 | 0 | 2 | 14.5 | 48.3 | L |
| Lancee et al. 2008 | 2 | 0 | 1 | 1 | 1 | 1 | 2 | 2 | 1.5 | 0 | 0 | 0.5 | 1 | 0 | 1.5 | 14.5 | 48.3 | L |
| Xu et al. 2021 | 2 | 0 | 1 | 0.5 | 0.5 | 2 | 1.5 | 1 | 1 | 1 | 0 | 2 | 0 | 0 | 1.5 | 14.0 | 46.7 | L |
| Tam et al. 2004 | 2 | 1 | 1.5 | 1 | 0.5 | 1 | 1.5 | 2 | 0 | 0 | 0 | 0.5 | 1 | 0 | 2 | 14.0 | 46.7 | L |
| Lasalvia et al. 2021 | 2 | 1 | 2 | 1 | 1 | 1 | 1.5 | 1.5 | 0 | 0 | 0 | 0.5 | 1 | 0 | 1 | 13.5 | 45.0 | L |
| Castro-Sanchez et al. 2020 | 2 | 1 | 1 | 1 | 0.5 | 1 | 0 | 2 | 0 | 0 | 0 | 2 | 1 | 0.5 | 1.5 | 13.5 | 45.0 | L |
| Zhan et al. 2020 | 2 | 1 | 1.5 | 1 | 1 | 1 | 1.5 | 0 | 0 | 0 | 0 | 0 | 1.5 | 1.5 | 1.5 | 13.5 | 45.0 | L |
| Hennein et al. 2021 | 2 | 0 | 2 | 1 | 1 | 1 | 1.5 | 1 | 0 | 0 | 0 | 0.5 | 2 | 0 | 1 | 13.0 | 43.3 | L |
| Sharma et al. 2021 | 2 | 1 | 1.5 | 1 | 1 | 2 | 2 | 0 | 0 | 0 | 0 | 0.5 | 1 | 0 | 1 | 13.0 | 43.3 | L |
| Huang et al. 2020 | 2 | 1 | 1 | 1 | 1 | 1 | 1.5 | 1 | 0 | 0 | 0 | 0.5 | 2 | 0 | 1 | 13.0 | 43.3 | L |
| Chan and Huak 2004 | 2 | 0 | 0.5 | 0.5 | 1 | 1 | 1.5 | 1.5 | 1 | 0 | 0 | 0 | 1 | 1 | 2 | 13.0 | 43.3 | L |
| Matsuishi et al. 2012 | 2 | 0 | 1.5 | 1 | 0.5 | 1 | 1.5 | 2 | 0 | 0 | 0 | 0.5 | 1 | 0 | 2 | 13.0 | 43.3 | L |
| Fiksenbaum et al. 2006 | 2 | 0 | 1 | 1 | 1 | 1 | 2 | 2 | 0 | 0 | 0 | 0 | 0.5 | 0 | 2 | 12.5 | 41.7 | L |
| Marjanovic et al. 2007 | 2 | 0 | 1 | 1 | 1 | 1 | 2 | 2 | 0 | 0 | 0 | 0 | 0.5 | 0 | 2 | 12.5 | 41.7 | L |
| Petrella et al. 2021 | 2 | 1 | 1 | 0 | 0 | 1 | 1.5 | 1 | 0 | 0 | 0 | 1.5 | 1.5 | 0 | 1.5 | 12.0 | 40.0 | L |
| Esmaeilzadeh et al. 2021 | 2 | 0 | 1.5 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 0.5 | 1 | 0.5 | 0.5 | 12.0 | 40.0 | L |
| Holton et al. 2020 | 2 | 0 | 1 | 1 | 0.5 | 1 | 2 | 0.5 | 0.5 | 0 | 0 | 0 | 1 | 1 | 1.5 | 12.0 | 40.0 | L |
| Kim and Choi 2016 | 2 | 0 | 1.5 | 1 | 0.5 | 1 | 1.5 | 1.5 | 0 | 0 | 0 | 0 | 1 | 0 | 2 | 12.0 | 40.0 | L |
| Kase et al. 2021 | 2 | 1 | 1 | 1 | 1 | 1 | 1.5 | 0 | 0 | 0 | 0 | 0.5 | 1.5 | 0 | 1 | 11.5 | 38.3 | L |
| Young et al. 2021 | 2 | 1 | 1 | 0 | 0 | 1 | 1.5 | 1 | 0 | 0 | 0 | 0.5 | 1.5 | 0 | 2 | 11.5 | 38.3 | L |
| Morgantini et al. 2020 | 2 | 1 | 1 | 1 | 1 | 1 | 1 | 0.5 | 0 | 0 | 0 | 0.5 | 1 | 0 | 1.5 | 11.5 | 38.3 | L |
| Demirjian et al. 2020 | 2 | 1 | 1.5 | 1 | 0.5 | 1 | 1 | 1 | 0 | 0 | 0 | 0 | 1 | 0 | 1.5 | 11.5 | 38.3 | L |
| Durmaz Engin et al. 2021 | 2 | 0 | 1 | 1 | 1 | 1 | 1.5 | 1 | 0 | 0 | 0 | 0.5 | 1 | 0 | 1 | 11.0 | 36.7 | L |
| Buch et al. 2021 | 2 | 0 | 1 | 1 | 0 | 1 | 1 | 2 | 0.5 | 0 | 0 | 1.5 | 0 | 0 | 0.5 | 10.5 | 35.0 | L |
| Shalhub et al. 2020 | 2 | 0 | 1 | 1 | 1 | 1 | 1.5 | 0 | 0 | 0 | 0 | 0.5 | 0.5 | 0 | 1.5 | 10.0 | 33.3 | L |
| Martinez-Caballero et al. 2021 | 2 | 0 | 1 | 0 | 0 | 1 | 1.5 | 1 | 0 | 0 | 0 | 1 | 1 | 0 | 1 | 9.5 | 31.7 | L |
| Temsah et al. 2021 | 2 | 1 | 0.5 | 0 | 0 | 1 | 1 | 0 | 0 | 0 | 0 | 0.5 | 1.5 | 0 | 2 | 9.5 | 31.7 | L |
| Zhang et al. 2020 | 1.5 | 0 | 1.5 | 1 | 0 | 1 | 1.5 | 1 | 0 | 0 | 0 | 0 | 1 | 0 | 1 | 9.5 | 31.7 | L |
| Cai et al. 2020 | 2 | 0 | 0.5 | 0.5 | 0 | 1 | 0 | 1 | 1 | 0 | 0 | 1 | 0 | 0.5 | 0.5 | 8.0 | 26.7 | L |
| Huffman et al. 2020 | 2 | 0 | 0.5 | 1 | 0.5 | 1 | 0 | 0.5 | 0 | 0 | 0 | 0 | 1 | 1 | 0 | 7.5 | 25.0 | L |
| Reidy et al. 2020 | 2 | 0 | 0.5 | 1 | 0 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 0.5 | 0 | 0.5 | 7.5 | 25.0 | L |
3.4. Quality of the Evidence on Intervention Effectiveness
4. Discussion
4.1. Theory or Implementation Failure?
4.2. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
| Concept * | Search Strategy |
|---|---|
| 1 | (depression or “depressive disorder” or anxiet* or anxious or “mental health” or “mental disorder*” or “adjustment disorder*” or (stress adj3 work*) or distress or ptsd or “post traumatic stress” or “post-traumatic stress” or “vicarious trauma*” or “secondary trauma*” or “compassion fatigue” or “compassion satisfaction” or traumatisation or traumatization or exhaustion or burnout or suicide or suicidal or fear).ti,ab,kw. OR anxiety disorders/ or depressive disorder/ or depressive disorder, major/ or “trauma and stressor related disorders”/ or stress disorders, traumatic/or stress disorders, post-traumatic/ OR emotions/ or bereavement/ or sadness/ or grief/ or guilt/ or loneliness/ or psychological distress/ or sadness/ OR exp adaptation, psychological/ or exp stress, psychological |
| 2 | ((interven* or program* or initiative* or approach* or project* or strateg* or reorganis* or reorganiz* or “re-organis*” or “re-organiz*” or redesign or “re-design” or restructuring or re-structuring or policy or policies or regulation* or guidance or guideline or standard or solution or change) adj5 (workplace or worker* or “work-place” or “workplace based” or “work-place based” or workload or workflow* or staff or personnel or employee* or occupation* or industry or “public sector” or “private sector” or employer or organization* or organisation* or task* or colleague* or coworker* or co-worker* or supervisor* or manager* or corporate or corporation or “iso-strain” or ((quantitative or mental or emotional or psychological) adj1 (demand* or workload)) or (job adj1 (control or demands or strain)) or “psychological strain” or “stress at work” or “stressful working condition” or “emotionally demanding work” or (decision* adj1 (latitude or authority or autonomy)) or (skill adj (discretion or utili#ation)) or “effort-reward” or “((social or corporate or organizational or organisational or company) adj1 (justice or leadership or trust))” or “team spirit” or harassment or violence or bullying or ((colleague* or coworker* or co-worker* or supervisor* or superior* or manager* or management) adj1 support) or ((corporate or safety or psychosocial) adj1 (climate or culture or environment)) or “flexible working conditions” or “work-life balance” or “work life balance” or “work-life conflict” or “work life conflict” or (work adj2 family) or “moral dilemma” or “moral injury” or “ethical dilemma” or “management practice*” or “corporate management” or “workplace management” or “work place management” or communication or transparency or purposeful)).ti,ab,kw. OR ergonomics/ or man-machine systems/ or organizational innovation/ OR Organizational culture/ |
| 3 | (efficien* or inefficien* or effective or efficacy or ineffective or evaluat* or assess*).ti,ab,kw. or ((intervention adj2 (trial* or study or studies)) or “Before and After Stud*” or “Before-After Stud*” or (pre adj5 post) or survey or surveys or questionnaire* or “focus group*” or interview*).ti,ab,kw. or comparative effectiveness research/ OR evaluation studies as topic/ OR program evaluation/ OR intervention studies/ OR Controlled Before-After Studies/ or (“Evaluation studies”).pt. |
| 4 | (H1N1 OR “middle east respiratory syndrome*” OR MERS OR SARS* OR “severe acute respiratory syndrome*” OR “SARS-CoV-2” OR “SARS-CoV” OR “COVID” OR “COVID-19” OR coronavirus* or pandemic* or epidemic* or influenza or flu or outbreak* or ebola or ebolavirus or zika or quarantine or confinement or ((health or sanitar*) adj1 (crisis or crises or emergenc*))).ti,ab,kw. Or COVID-19/ or epidemics/ or pandemics/ or disease outbreaks/ |
| Item | Scoring (Number of Points) |
|---|---|
| Was the research question or study objectives clear and explicitly stated? | |
| No research question or study objective was described | 0 |
| A research question or study objective was mentioned but was not clear | 1 |
| The research question and/or study objectives were clear and explicitly stated | 2 |
| Did the study include a control group? | |
| There was no control group | 0 |
| There was a control group, but it was not appropriate | 1 |
| There was an appropriate control group | 2 |
| Were study participants randomly assigned to the control or intervention group? If study participants were not randomly assigned, were workers’ baseline sociodemographic, occupational exposure and mental health outcome characteristics measured? | |
| Study participants were not randomly assigned to the control or intervention group and their baseline characteristics were not measured | 0 |
| Study participants were not randomly assigned to the control or intervention group but some of their baseline characteristics were measured (however, important baseline sociodemographic, occupational exposure or health characteristics are missing) | 1 |
| Study participants were randomly assigned to the control or intervention group OR baseline sociodemographic, occupational exposure and health characteristics were measured | 2 |
| Were relevant occupational exposures measured before (at baseline) and after (at follow-up) the intervention? | |
| Relevant occupational exposures were not measured | 0 |
| Some very relevant occupational exposures were not measured | 1 |
| Relevant occupational exposures were measured either only at baseline or at follow-up, but not at both time points | 1 |
| Relevant occupational exposures were measured at baseline and at follow-up, but not in the same participants (unpaired data) | 1 |
| Relevant occupational exposures were measured at baseline and at follow-up in the same participants (paired data) | 2 |
| Were occupational exposure measures appropriate, valid, reliable and sensitive to change? | |
| Occupational exposure measures were not appropriate | 0 |
| Occupational exposure measures seem appropriate, but there was no confirmation that they were valid, reliable and/or sensitive to change | 1 |
| Occupational exposure measures were appropriate, valid, reliable and sensitive to change | 2 |
| Was the mental health outcome measured before (at baseline) and after (at follow-up) the intervention? | |
| A mental health outcome was not measured | 0 |
| The mental health outcome was measured either only at baseline or at follow-up, but not at both time points | 1 |
| The mental health outcome was measured at baseline and at follow-up, but not in the same participants (unpaired data) | 1 |
| The mental health outcome was measured at baseline and at follow-up in the same participants (paired data) | 2 |
| Not applicable: study objective is to measure the effect of the intervention on occupational exposures, not mental health | 1 |
| Was the mental health outcome measure appropriate, valid, reliable and sensitive to change? | |
| The mental health outcome measure was not appropriate | 0 |
| The mental health outcome measure seems appropriate, but there was no confirmation that it was valid, reliable and/or sensitive to change | 1 |
| The mental health outcome measure was appropriate, valid, reliable and sensitive to change | 2 |
| Not applicable: study objective is to measure the effect of the intervention on occupational exposures, not mental health | 1 |
| Was the length of follow-up after the end of implementation of the intervention appropriate? | |
| The length of follow-up after the end of implementation of the intervention was not indicated | 0 |
| The follow-up was done before the end of intervention implementation or the length of follow-up was too short to allow for an effect on the health outcome (or on another measured outcome) to be demonstrated | 1 |
| The length of follow-up after the end of implementation of the intervention was appropriate | 2 |
| Was study participation rate after recruitment documented and adequate for the experimental and control groups? | |
| Study participation rate after recruitment was not documented or was <60% | 0 |
| Study participation rate after recruitment was between 60 and 79% | 1 |
| Study participation rate after recruitment was ≥80% | 2 |
| Was the loss of study participants to follow-up in the experimental and control groups acceptable? | |
| The loss to follow-up was not documented or was >30% | 0 |
| The loss to follow-up was between 21 and 30% | 1 |
| The loss to follow-up was ≤20% | 2 |
| Were the participants who dropped out of the study (drop-outs) comparable to those who completed the study (completers)? | |
| A comparison of the characteristics of drop-outs and completers was not documented | 0 |
| There were important differences in the characteristics of drop-outs and completers, but this was not considered in the analyses | 1 |
| There were no important differences in the characteristics of drop-outs and completers, and this was documented OR the loss to follow-up was ≤20% | 2 |
| Was the implementation of intended changes documented and were changes implemented as intended? | |
| The implementation of changes was not documented | 0 |
| The implementation of changes was documented but they were not implemented or only some intended changes were implemented | 1 |
| The implementation of changes was documented and the majority of intended changes were implemented | 2 |
| Were potential confounders of the effect of the intervention on the mental health outcome (ex. history of mental illness, intervention compliance) and on the work exposures measured considered and properly taken into account in the analysis (ex. adjustment, stratification) or interpretation of results? | |
| No potential confounders were measured | 0 |
| Important confounders were not measured or measured confounders were not properly taken into account in the analysis or were only considered in interpretation of results | 1 |
| Potential confounders were measured and properly taken into account in the analysis | 2 |
| Were contextual factors and co-interventions that could influence the results considered in the analysis or in the interpretation of the results? | |
| No contextual factors or co-interventions that could influence the results were documented | 0 |
| Only a few relevant contextual factors or co-interventions were documented or considered in the analysis or in the interpretation of the results | 1 |
| Relevant contextual factors and co-interventions were documented and considered, either in the analysis or in the interpretation of the results | 2 |
| Was the statistical analysis appropriate for measuring the effectiveness of the intervention? | |
| The analysis was inadequately described, precluding us from evaluating its appropriateness or the analysis was inappropriate | 0 |
| The statistical power of the study or at least one other important element of analysis was inappropriate | 1 |
| The analysis and power of the study were appropriate | 2 |
References
- Chênevert, D.; Jézéquel, M. L’épuisement des professionnels de la santé au Québec. Gestion 2018, 43, 72–75. (In French) [Google Scholar] [CrossRef]
- Dewa, C.S.; Jacobs, P.; Thanh, N.X.; Loong, D. An estimate of the cost of burnout on early retirement and reduction in clinical hours of practicing physicians in Canada. BMC Health Serv. Res. 2014, 14, 254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eaton, L. Health workforce burn-out. Bull. World Health Organ. 2019, 97, 585–586. [Google Scholar] [CrossRef]
- Hamidi, M.S.; Bohman, B.; Sandborg, C.; Smith-Coggins, R.; de Vries, P.; Albert, M.S.; Murphy, M.L.; Welle, D.; Trockel, M.T. Estimating institutional physician turnover attributable to self-reported burnout and associated financial burden: A case study. BMC Health Serv. Res. 2018, 18, 851. [Google Scholar] [CrossRef] [Green Version]
- Shah, M.K.; Gandrakota, N.; Cimiotti, J.P.; Ghose, N.; Moore, M.; Ali, M.K. Prevalence of and factors associated with nurse burnout in the US. JAMA Netw. Open 2021, 4, e2036469. [Google Scholar] [CrossRef] [PubMed]
- Bell, V.; Wade, D. Mental health of clinical staff working in high-risk epidemic and pandemic health emergencies a rapid review of the evidence and living meta-analysis. Soc. Psychiatry Psychiatr. Epidemiol. 2020, 56, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Kisely, S.; Warren, N.; McMahon, L.; Dalais, C.; Henry, I.; Siskind, D. Occurrence, prevention, and management of the psychological effects of emerging virus outbreaks on healthcare workers: Rapid review and meta-analysis. Br. Med. J. BMJ 2020, 369, m1642. [Google Scholar] [CrossRef]
- Jauvin, N.; Feillou, I. Prendre le temps de reconnaître et de comprendre la charge émotionnelle chez les soignants: Vers des pistes d’intervention en temps de pandémie. Cah. Francoph. Soins Palliatifs 2021, 20, 23–30. [Google Scholar]
- Carazo, S.; Pelletier, M.; Talbot, D.; Jauvin, N.; De Serres, G.; Vézina, M. Psychological distress of healthcare workers in Québec (Canada) during the second and the third pandemic waves. J. Occup. Environ. Med. 2022, 64, 495–503. [Google Scholar] [CrossRef]
- De Serres, G.; Carazo, S.; Lorcy, A.; Villeneuve, J.; Laliberté, D.; Martin, R.; Deshaies, P.; Bellemare, D.; Tissot, F.; Adib, G.; et al. Enquête Epidémiologique sur les Travailleurs de la Santé Atteints par la COVID-19 au Printemps 2020; Research Report; Institut national de santé publique du Québec: Quebec City, QC, Canada, 2020; ISBN 978-2-550-87681-6. Available online: https://www.inspq.qc.ca/publications/3061-enquete-epidemiologique-travailleurs-sante-covid19 (accessed on 13 April 2022).
- Godlee, F. Protect our healthcare workers. Br. Med. J. BMJ 2020, 369, m1324. [Google Scholar] [CrossRef] [Green Version]
- Pelletier, M.; Carazo, S.; Jauvin, N.; Talbot, D.; De Serres, G.; Vézina, M. Étude sur la Détresse Psychologique des Travailleurs de la Santé Atteints de la COVID-19 au Quebec Durant la Deuxième Vague Pandémique; Research Report; Institut national de santé publique du Québec: Quebec City, QC, Canada, 2021; ISBN 978-2-550-89211-3. Available online: https://www.inspq.qc.ca/publications/3135-detresse-psychologique-travailleurs-sante-atteints-covid19 (accessed on 13 April 2022).
- Protecteur du Citoyen. The Québec Ombudsman’s Status Report: COVID-19 in CHSLDs during the First Wave of the Pandemic; Protecteur du Citoyen: Quebec City, QC, Canada, 2020; Available online: https://protecteurducitoyen.qc.ca/sites/default/files/pdf/rapports_speciaux/progress-report-chslds-covid-19.pdf (accessed on 13 April 2022).
- Mathisen, J.; Nguyen, T.-L.; Jensen, J.H.; Rugulies, R.; Rod, N.H. Reducing employee turnover in hospitals: Estimating the effects of hypothetical improvements in the psychosocial work environment. Scand. J. Work. Environ. Health 2021, 47, 456–465. [Google Scholar] [CrossRef] [PubMed]
- Panagioti, M.; Panagopoulou, E.; Bower, P.; Lewith, G.; Kontopantelis, E.; Chew-Graham, C.; Dawson, S.; van Marwijk, H.; Geraghty, K.; Esmail, A. Controlled interventions to reduce burnout in physicians: A systematic review and meta-analysis. JAMA Intern. Med. 2017, 177, 195–205. [Google Scholar] [CrossRef] [PubMed]
- Muller, A.E.; Hafstad, E.V.; Himmels, J.P.W.; Flottorp, S.; Stensland, S.Ø.; Stroobants, S.; Van de Velde, S.; Vist, G.E. The mental health impact of the covid-19 pandemic on healthcare workers, and interventions to help them: A rapid systematic review. Psychiatry Res. 2020, 293, 113441. [Google Scholar] [CrossRef] [PubMed]
- Pollock, A.; Campbell, P.; Cheyne, J.; Cowie, J.; Davis, B.; McCallum, J.; McGill, K.; Elders, A.; Hagen, S.; McClurg, D.; et al. Interventions to support the resilience and mental health of frontline health and social care professionals during and after a disease outbreak, epidemic or pandemic: A mixed methods systematic review. Cochrane Database Syst. Rev. 2020, 11, CD013779. [Google Scholar] [CrossRef]
- Soklaridis, S.; Lin, E.; Lalani, Y.; Rodak, T.; Sockalingam, S. Mental health interventions and supports during COVID-19 and other medical pandemics: A rapid systematic review of the evidence. Gen. Hosp. Psychiatry 2020, 66, 133–146. [Google Scholar] [CrossRef]
- Chen, R.; Chou, K.-R.; Huang, Y.-J.; Wang, T.-S.; Liu, S.-Y.; Ho, L.-Y. Effects of a SARS prevention programme in Taiwan on nursing staff’s anxiety, depression and sleep quality: A longitudinal survey. Int. J. Nurs. Stud. 2006, 43, 215–225. [Google Scholar] [CrossRef]
- Zaçe, D.; Hoxhaj, I.; Orfino, A.; Viteritti, A.M.; Janiri, L.; Di Pietro, M.L. Interventions to address mental health issues in healthcare workers during infectious disease outbreaks: A systematic review. J. Psychiatr. Res. 2021, 136, 319–333. [Google Scholar] [CrossRef]
- Sauter, S.L.; Brightwell, S.W.; Colligan, M.J.; Hurrell, J.J., Jr.; Katz, T.M.; LeGrande, D.E.; Lessin, N.; Lippin, R.A.; Lipscomb, J.A.; Murphy, L.R.; et al. The Changing Organization of Work and the Safety and Health of Working People: Knowledge Gaps and Research Directions; Report No. 2002-116; Department of Health and Human Services, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health (NIOSH): Cincinnati, OH, USA, 2002. [Google Scholar]
- Johnson, J.V.; Hall, E.M. Job strain, work place social support, and cardiovascular disease: A cross-sectional study of a random sample of the Swedish working population. Am. J. Public Health 1998, 78, 1336–1342. [Google Scholar] [CrossRef] [Green Version]
- Karasek, R.A. Job demands, job decision latitude, and mental strain: Implications for job redesign. Adm. Sci. Q. 1979, 24, 285–308. [Google Scholar] [CrossRef]
- Karasek, R.A.; Theorell, T. Healthy Work: Stress, Productivity, and the Reconstruction of Working Life; Basic Books: New York, NY, USA, 1990. [Google Scholar]
- Kristensen, T.S.; Hannerz, H.; Høgh, A.; Borg, V. The Copenhagen Psychosocial Questionnaire-a tool for the assessment and improvement of the psychosocial work environment. Scand. J. Work Environ. Health 2005, 31, 438–449. [Google Scholar] [CrossRef] [Green Version]
- Niedhammer, I.; Bertrais, S.; Witt, K. Psychosocial work exposures and health outcomes: A meta-review of 72 literature reviews with meta-analysis. Scand. J. Work Environ. Health 2021, 47, 489–508. [Google Scholar] [CrossRef] [PubMed]
- Pejtersen, J.H.; Kristensen, T.S.; Borg, V.; Bjorner, J.B. The second version of the Copenhagen Psychosocial Questionnaire. Scand. J. Public Health 2010, 38 (Suppl. S3), 8–24. [Google Scholar] [CrossRef] [PubMed]
- Siegrist, J.; Starke, D.; Chandola, T.; Godin, I.; Marmot, M.; Niedhammer, I.; Peter, R. The measurement of effort-reward imbalance at work: European comparisons. Soc. Sci. Med. 2004, 58, 1483–1499. [Google Scholar] [CrossRef]
- Siegrist, J. Adverse health effects of high-effort/low-reward conditions. J. Occup. Health Psychol. 1996, 1, 27–41. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Br. Med. J. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Kristensen, T.S. Intervention studies in occupational epidemiology. Occup. Environ. Med. 2005, 62, 205–210. [Google Scholar] [CrossRef] [Green Version]
- Neumann, W.P.; Eklund, J.; Hansson, B.; Lindbeck, L. Effect assessment in work environment interventions: A methodological reflection. Ergonomics 2010, 53, 130–137. [Google Scholar] [CrossRef]
- Stock, S.R.; Nicolakakis, N.; Vézina, N.; Vézina, M.; Gilbert, L.; Turcot, A.; Sultan-Taieb, H.; Sinden, K.; Denis, M.-A.; Delga, C.; et al. Are work organization interventions effective in preventing or reducing work-related musculoskeletal disorders? A systematic review of the literature. Scand. J. Work Environ. Health 2018, 44, 113–133. [Google Scholar] [CrossRef]
- Guyatt, G.; Oxman, A.D.; Akl, E.A.; Kunz, R.; Vist, G.; Brozek, J.; Norris, S.; Falck-Ytter, Y.; Glasziou, P.; DeBeer, H.; et al. GRADE guidelines: 1. Introduction-GRADE evidence profiles and summary of findings tables. J. Clin. Epidemiol. 2011, 64, 383–394. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.; Kunz, R.; Brozek, J.; Alonso-Coello, P.; Montori, V.; Akl, E.A.; Djulbegovic, B.; Falck-Ytter, Y.; et al. GRADE guidelines: 4. Rating the quality of evidence—Study limitations (risk of bias). J. Clin. Epidemiol. 2011, 64, 407–415. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Montori, V.; Vist, G.; Kunz, R.; Brozek, J.; Alonso-Coello, P.; Djulbegovic, B.; Atkins, D.; Falck-Ytter, Y.; et al. GRADE guidelines: 5. Rating the quality of evidence—Publication bias. J. Clin. Epidemiol. 2011, 64, 1277–1282. [Google Scholar] [CrossRef] [PubMed]
- Guyatt, G.H.; Oxman, A.D.; Kunz, R.; Brozek, J.; Alonso-Coello, P.; Rind, D.; Devereaux, P.; Montori, V.M.; Freyschuss, B.; Vist, G.; et al. GRADE guidelines 6. Rating the quality of evidence—Imprecision. J. Clin. Epidemiol. 2011, 64, 1283–1293. [Google Scholar] [CrossRef] [PubMed]
- Guyatt, G.H.; Oxman, A.D.; Kunz, R.; Woodcock, J.; Brozek, J.; Helfand, M.; Alonso-Coello, P.; Glasziou, P.; Jaeschke, R.; Akl, E.A.; et al. GRADE Working Group. GRADE guidelines: 7. Rating the quality of evidence—Inconsistency. J. Clin. Epidemiol. 2011, 64, 1294–1302. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Kunz, R.; Woodcock, J.; Brozek, J.; Helfand, M.; Alonso-Coello, P.; Falck-Ytter, Y.; Jaeschke, R.; Vist, G.; et al. GRADE Working Group. GRADE guidelines: 8. Rating the quality of evidence—Indirectness. J. Clin. Epidemiol. 2011, 64, 1303–1310. [Google Scholar] [CrossRef] [PubMed]
- Guyatt, G.H.; Oxman, A.D.; Sultan, S.; Glasziou, P.; Akl, E.A.; Alonso-Coello, P.; Atkins, D.; Kunz, R.; Brozek, J.; Montori, V.; et al. GRADE Working Group. GRADE guidelines: 9. Rating up the quality of evidence. J. Clin. Epidemiol. 2011, 64, 1311–1316. [Google Scholar] [CrossRef]
- Balshem, H.; Helfand, M.; Schünemann, H.J.; Oxman, A.D.; Kunz, R.; Brozek, J.; Vist, G.E.; Falck-Ytter, Y.; Meerpohl, J.; Norris, S.; et al. GRADE guidelines: 3. Rating the quality of evidence. J. Clin. Epidemiol. 2011, 64, 401–406. [Google Scholar] [CrossRef]
- Beneria, A.; Arnedo, M.; Contreras, S.; Pérez-Carrasco, M.; Garcia-Ruiz, I.; Rodríguez-Carballeira, M.; Raduà, J.; Rius, J.B. Impact of simulation-based teamwork training on COVID-19 distress in healthcare professionals. BMC Med. Educ. 2020, 20, 515. [Google Scholar] [CrossRef]
- Blake, H.; Yildirim, M.; Wood, B.; Knowles, S.; Mancini, H.; Coyne, E.; Cooper, J. COVID-Well: Evaluation of the implementation of supported wellbeing centres for hospital employees during the COVID-19 pandemic. Int. J. Environ. Res. Public Health 2020, 17, 9401. [Google Scholar] [CrossRef]
- Giordano, F.; Cipolla, A.; Ungar, M. Building resilience for healthcare professionals working in an Italian red zone during the COVID-19 outbreak: A pilot study. Stress Health 2021, 38, 234–248. [Google Scholar] [CrossRef]
- Zaghini, F.; Fiorini, J.; Livigni, L.; Carrabs, G.; Sili, A. A mixed methods study of an organization’s approach to the COVID-19 health care crisis. Nurs. Outlook 2021, 69, 793–804. [Google Scholar] [CrossRef]
- Zhu, Z.; Xu, S.; Wang, H.; Liu, Z.; Wu, J.; Li, G.; Miao, J.; Zhang, C.; Yang, Y.; Sun, W.; et al. COVID-19 in Wuhan: Sociodemographic characteristics and hospital support measures associated with the immediate psychological impact on healthcare workers. eClinicalMedicine 2020, 24, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Maunder, R.G.; Lancee, W.J.; Balderson, K.E.; Bennett, J.P.; Borgundvaag, B.; Evans, S.; Fernandes, C.M.B.; Goldbloom, D.S.; Gupta, M.; Hunter, J.J.; et al. Long-term psychological and occupational effects of providing hospital healthcare during SARS outbreak. Emerg. Infect. Dis. 2006, 12, 1924–1932. [Google Scholar] [CrossRef] [PubMed]
- Havermans, B.M.; Schelvis, R.M.C.; Boot, C.R.L.; Brouwers, E.P.M.; Anema, J.R.; van der Beek, A.J. Process variables in organizational stress management intervention evaluation research: A systematic review. Scand. J. Work Environ. Health 2016, 42, 371–381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rafferty, A.M.; Clarke, S.P.; Coles, J.; Ball, J.; James, P.; McKee, M.; Aiken, L.H. Outcomes of variation in hospital nurse staffing in English hospitals: Cross-sectional analysis of survey data and discharge records. Int. J. Nurs. Stud. 2007, 44, 175–182. [Google Scholar] [CrossRef] [Green Version]
- Messing, K.; Punnett, L.; Bond, M.; Alexanderson, K.; Pyle, J.; Zahm, S.; Wegman, D.; Stock, S.R.; de Grosbois, S. Be the fairest of them all: Challenges and recommendations for the treatment of gender in occupational health research. Am. J. Ind. Med. 2003, 43, 618–629. [Google Scholar] [CrossRef]
- Messing, K.; Stock, S.R.; Tissot, F. Should studies of risk factors for musculoskeletal disorders be stratified by gender? Lessons from the 1998 Québec Health and Social Survey. Scand. J. Work Environ. Health 2009, 5, 96–112, Erratum in Scand. J. Work Environ. Health 2009, 35, 400. [Google Scholar] [CrossRef] [Green Version]
- Silverstein, B.; Fan, Z.J.; Smith, C.K.; Bao, S.; Howard, N.; Spielholz, P.; Bonauto, D.K.; Viikari-Juntura, E. Gender adjustment or stratification in discerning upper extremity musculoskeletal disorder risk? Scand. J. Work. Environ. Health 2009, 35, 113–126. [Google Scholar] [CrossRef] [Green Version]
- Milan, A.; Keown, L.-A.; Robles Urquijo, C. Women in Canada: A Gender-Based Statistical Report: Families, Living Arrangements and Unpaid Work. Minister of Industry. Statistics Canada. Catalogue no. 89-503-X. 2011. Available online: https://www150.statcan.gc.ca/n1/en/pub/89-503-x/89-503-x2010001-eng.pdf?st=2-O-KyWe (accessed on 13 April 2022).
- Biswas, A.; Harbin, S.; Irvin, E.; Johnston, H.; Begum, M.; Tiong, M.; Apedaile, D.; Koehoorn, M.; Smith, P. Sex and gender differences in occupational hazard exposures: A scoping review of the recent literature. Curr. Environ. Health Rep. 2021, 8, 267–280. [Google Scholar] [CrossRef]
- Hoffmann, D.E.; Tarzian, A.J. The girl who cried pain: A bias against women in the treatment of pain. J. Law Med. Ethics 2001, 29, 13–27. [Google Scholar] [CrossRef] [Green Version]
- Lippel, K. Preserving workers’ dignity in workers’ compensation systems: An international perspective. Am. J. Ind. Med. 2012, 55, 519–536. [Google Scholar] [CrossRef]
- Sagar-Ouriaghli, I.; Godfrey, E.; Bridge, L.; Meade, L.; Brown, J.S.L. Improving mental health service utilization among men: A systematic review and synthesis of behavior change techniques within interventions targeting help-seeking. Am. J. Men’s Health 2019, 13, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Sultan-Taïeb, H.; St-Hilaire, F.; Lefebvre, R.; Biron, C.; Vézina, M.; Brisson, C. Taking account of gender differences when designing interventions in occupational health? Lessons from a study of the “Healthy Enterprise” Standard in Québec. New Solut. J. Environ. Occup. Health Policy 2017, 27, 261–381. [Google Scholar] [CrossRef]
- Nielsen, K.; Miraglia, M. What works for whom in which circumstances? On the need to move beyond the ‘what works?’ question in organizational intervention research. Hum. Relat. 2017, 70, 40–62. [Google Scholar] [CrossRef] [Green Version]
- Biron, C.; Karanika-Murray, M. Process evaluation for organizational stress and well-being interventions: Implications for theory, method, and practice. Int. J. Stress Manag. 2014, 21, 85–111. [Google Scholar] [CrossRef] [Green Version]
- Rivilis, I.; Van Eerd, D.; Cullen, K.; Cole, D.C.; Irvin, E.; Tyson, J.; Mahood, Q. Effectiveness of participatory ergonomic interventions on health outcomes: A systematic review. Appl. Ergon. 2008, 39, 342–358. [Google Scholar] [CrossRef]
- Bourbonnais, R.; Brisson, C.; Vézina, M. Long-term effects of an intervention on psychosocial work factors among healthcare professionals in a hospital setting. Occup. Environ. Med. 2011, 68, 479–486. [Google Scholar] [CrossRef]
- Jauvin, N.; Freeman, A.; Côté, N.; Biron, C.; Duchesne, A.; Allaire, E. Une Démarche Paritaire de Prévention Pour Contrer les Effets du Travail Emotionnellement Exigeant dans les Centres Jeunesse; Research Report; Institut de Recherche Robert-Sauvé en santé et en sécurité du travail: Montreal, QC, Canada, 2019; Available online: https://www.irsst.qc.ca/publications-et-outils/publication/i/101021/n/travail-emotionnellement-exigeant (accessed on 13 April 2022).
- Jauvin, N.; Bourbonnais, R.; Vézina, M.; Brisson, C.; Hegg-Deloye, S. Interventions to prevent mental health problems at work: Facilitating and hindering factors. In Creating Healthy Workplaces: Stress Reduction, Improved Well-Being, and Organizational Effectiveness; Biron, C., Burke, R., Cooper, C.L., Eds.; Gower Publishing Ltd.: Farnham, UK, 2014; pp. 239–260. [Google Scholar]
- Nielsen, K.; Randall, T. Opening the black box: Presenting a model for evaluating organizational-level interventions. Eur. J. Work. Organ. Psychol. 2013, 22, 601–617. [Google Scholar] [CrossRef]
- St-Vincent, M.; Vézina, N.; Bellemare, M.; Denis, D.; Ledoux, E.; Imbeau, D. l’Intervention en Ergonomie; Éditions MultiMondes: Quebec City, QC, Canada, 2011; Available online: https://www.irsst.qc.ca/publications-et-outils/publication/i/100608/n/intervention-en-ergonomie-intervention-ergo (accessed on 13 April 2022).
- Abildgaard, J.H.; Nielsen, K.; Wåhlin-Jacobsen, C.D.; Maltesen, T.; Christensen, K.B.; Holtermann, A. ‘Same, but different’: A mixed-methods realist evaluation of a cluster-randomized controlled participatory organizational intervention. Hum. Relat. 2020, 73, 1339–1365. [Google Scholar] [CrossRef]
- Ruotsalainen, J.H.; Verbeek, J.H.; Mariné, A.; Serra, C. Preventing occupational stress in healthcare workers. Cochrane Database Syst. Rev. 2015, 4, CD002892. [Google Scholar] [CrossRef] [PubMed]

| Intervention 1 | Intervention Effect 1 on Mental Health or Psychosocial Work Exposure Indicators | Quality of the Evidence 2 on Intervention Effectiveness and Justification of Rating |
|---|---|---|
| Simulation-based teamwork training program (25 h) (Beneria et al. 2020) [42] | ↑ likelihood of anxiety and depression (HADS > 12) post-program in workers having had contact with COVID-19 patients: AOR 2.56, 95% CI: 1.03–6.36; p = 0.043. AOR not reported for all workers who received the training program or for those who received it but had had no contact with COVID-19 patients. | Very low Observational design, serious risks of selection and confounding bias (48% participation rate for control group, important confounders omitted, i.e., history of mental illness, psychosocial work exposures) |
| Wellbeing centers supported by wellbeing buddies (4–5 months) (Blake et al. 2020) [43] | ↑ mental wellbeing of 1.93 points on WEMWBS scale that ranges from 14 to 70 points: mean WEMWBS score (SD) is 47.04 (9.49) for center users and 45.11 (9.35) for non-users; p = 0.02 | Very low Observational design, serious risks of selection and confounding bias (<5% participation rate, confounding factors not considered in analysis) |
| ↑ work engagement of 0.19 points on dedication subscale of UWES-9 ranging from 0 to 6 points: mean score (SD) is 5.02 (1.38) for center users and 4.83 (1.15) for non-users; p = 0.08 | Very low Observational design, serious risks of selection and confounding bias (<5% participation rate, confounding factors not considered in analysis) | |
| ≠ % presenteeism past 12 months among center users vs. non-users: no, never: 16.31 vs. 14.97 yes, once: 17.05 vs. 12.76 yes, 2 to 5 times: 16.92 vs. 12.64 yes, >5 times: 4.53 vs. 4.41 p = 0.28 | Very low Observational design, serious risks of selection and confounding bias (<5% participation rate, confounding factors not considered in analysis) | |
| ≠ % with intention to quit among center users (16.31%) and non-users (15.09%); p = 0.25 | Very low Observational design, serious risks of selection and confounding bias (<5% participation rate, confounding factors not considered in analysis) | |
| Multi-component SARS prevention program: scheduling and staffing adjustments, IPC measures and protocols, latest PPE, daily information, training, mental health team and clinic for workers (3 months) (Chen et al. 2006) [19] | ↓ anxiety level from moderate before SARS patient care (T0) to mild two weeks (T1) and one month (T2) under prevention program to no anxiety at final time point (T3), Zung’s self-rating anxiety scale: Mean anxiety score (SD)
| Very low Observational design, serious risks of selection and confounding bias (participation rate ND, unclear if all measured covariables were included in models, other potential confounders not measured, i.e., program compliance, medication use for anxiety, work exposures, e.g., changing work schedules mentioned in discussion, other factors outside work) |
| ↓ depression level from moderate before SARS patient care (T0) to mild two weeks (T1) and one month (T2) under prevention program to no depression at final time point (T3), Zung’s self-rating depression scale: Mean depression score (SD)
| Very low Observational design, serious risks of selection and confounding bias (participation rate ND, unclear if all measured covariables were included in models, other potential confounders not measured, i.e., program compliance, medication use for depression, work exposures, e.g., changing work schedules mentioned in discussion, other factors outside work) | |
| ↑ sleep quality under prevention program, but sleep quality remains poor, i.e., PSQI > 5, at all time points Mean sleep quality score (SD)
| Very low Observational design, serious risks of selection and confounding bias (participation rate ND, unclear if all measured covariables were included in models, other potential confounders not measured, i.e., program compliance, work exposures, e.g., changing work schedules mentioned in discussion, other factors outside work) | |
| Multi-component COVID-19 prevention program: recognition measures (2 weeks) (Zhu et al. 2020) [46] | Recognition measures are associated with 24% ↓ likelihood of anxiety (GAD-7 ≥ 8) compared to not having received recognition measures: AOR (95% CI): 0.76 (0.60–0.97); p = 0.03 | Low Observational design |
| Recognition measures are associated with 31% ↓ likelihood of depression (PHQ-9 ≥ 10) compared to not having received recognition measures: AOR (95% CI): 0.69 (0.52–0.90); p = 0.007 | Low Observational design | |
| Recognition measures are associated with 24% ↓ likelihood of acute stress in the past 7 days caused by a traumatic event, COVID-19 being the specific event (IES-R > 33), compared to not having received recognition measures: AOR (95% CI): 0.76 (0.60–0.97); p = 0.024 | Low Observational design | |
| Multi-component COVID-19 prevention program: satisfaction with IPC measures (2 weeks) (Zhu et al. 2020) [46] | Satisfaction with IPC measures is associated with 35% ↓ likelihood of anxiety (GAD-7 ≥ 8) compared to not being satisfied: AOR (95% CI): 0.65 (0.50–0.85); p = 0.002 | Low Observational design |
| Satisfaction with IPC measures is associated with 30% ↓ likelihood of depression (PHQ-9 ≥ 10) compared to not being satisfied: AOR (95% CI): 0.70 (0.51–0.95); p = 0.02 | Low Observational design | |
| Satisfaction with IPC measures is associated with 31% ↓ likelihood of acute stress in the past 7 days caused by a traumatic event, COVID-19 being the specific event (IES-R > 33) compared to not being satisfied: AOR (95% CI): 0.69 (0.53–0.89); p = 0.004 | Low Observational design | |
| Multi-component COVID-19 prevention program: satisfaction with logistic support (shuttle service, meals/hydration and accommodation) (2 weeks) (Zhu et al. 2020) [46] | Satisfaction with logistic support is associated with 31% ↓ likelihood of anxiety (GAD-7 ≥ 8) compared to not being satisfied: AOR (95% CI): 0.69 (0.50–0.96); p = 0.03 | Low Observational design |
| Satisfaction with logistic support is associated with 33% ↓ likelihood of depression (PHQ-9 ≥ 10) compared to not being satisfied: AOR (95% CI): 0.67 (0.47–0.97); p = 0.03 | Low Observational design | |
| Effect of satisfaction with logistic support on likelihood of acute stress in the past 7 days caused by a traumatic event, COVID-19 being the specific event (IES-R > 33), not reported because not significant in univariate analysis | Low Observational design | |
| Multi-component COVID-19 prevention program: satisfaction with work shift arrangements (2 weeks) (Zhu et al. 2020) [46] | Effect of satisfaction with work shift arrangements on likelihood of anxiety not reported because not significant in univariate analysis | Low Observational design |
| Satisfaction with work shift arrangements is associated with 52% ↓ likelihood of depression (PHQ-9 ≥ 10) compared to not being satisfied: AOR (95% CI): 0.48 (0.34–0.67); p < 0.001 | Low Observational design | |
| Satisfaction with work shift arrangements is associated with 55% ↓ likelihood of acute stress in the past 7 days caused by a traumatic event, COVID-19 being the specific event (IES-R > 33), compared to not being satisfied: AOR (95% CI): 0.45 (0.33–0.63); p < 0.001 | Low Observational design | |
| “R2 for Leaders” resilience training program intended to equip healthcare leaders to better lead their staff and organization by identifying and implementing individual resilience and organization-level prevention programs (12 virtual 2-h weekly sessions over 3 months) (Giordano et al. 2021) [44] | ↓ emotional exhaustion level in healthcare leaders post-program: mean MBI-EE score (SD): T1: 6.31 (1.35) vs. T2: 5.37 (1.20); p = 0.020; Hedge’s g (corrected Cohen’s d for small samples < 50) = −0.30 | Very low Observational design, serious risks of selection and confounding bias (participation rate ND, potential confounders not considered in analyses), potentially inadequate power |
| ≠ emotional exhaustion level in staff post-program (no clinically or statistically significant difference): mean MBI-EE score (SD): T1: 4.70 (1.63) vs. T2: 4.35 (1.64); p = 0.098 | Very low Observational design, serious risks of selection and confounding bias (participation rate ND, potential confounders not considered in analyses), potentially inadequate power | |
| ≠ quality of leaders’ psychosocial work environment post-program: mean HSE-MSIT score (SD) on scale of 22 to 110: T1: 50.50 (15.33) vs. T2: 50.56 (15.17); p = 0.966 | Very low Observational design, serious risks of selection and confounding bias (participation rate ND, potential confounders not considered in analyses), potentially inadequate power | |
| ↑ quality of staff’s psychosocial work environment post-program: mean HSE-MSIT score (SD) on scale of 22 to 110: T1: 50.18 (10.56) vs. T2: 46.93 (10.75); p = 0.028; Cohen’s d = −0.29 | Very low Observational design, serious risks of selection and confounding bias (participation rate ND, potential confounders not considered in analyses), potentially inadequate power | |
| Multi-component COVID-19 prevention program: reorganized wards (e.g., increased ICU beds), procedures (e.g., cleaning and disinfection) and internal paths, increased nurse-to-patient ratios in COVID units, PPE training, other training, promoted participatory approach, autonomy and conscientiousness through continuous clinical and organizational audits, lectures, workshops and meetings, psychological help desk for staff, staff COVID-19 testing (4 months) (Zaghini et al. 2021) [45] | ≠ quality of emotional life post-program: mean score on emotional subscale of NQoL-SAT-P (SD) that ranges from 1 to 4: T0: 3.13 (.49) vs. T1: 3.16 (.52); p = 0.334 | Low Observational design, risk of confounding bias (several potential confounders ND (i.e., level of adherence to the intervention) or not integrated in analyses (i.e., age, having children)) |
| ↑ quality of the psychosocial work environment post-program: mean HSE-MSIT score (SD) on scale of 1 to 5: T0: 2.46 (0.40) vs. T1: 2.32 (0.50); p < 0.001 | Low Observational design, risk of confounding bias (several potential confounders ND (i.e., level of adherence to the intervention) or not integrated in analyses (i.e., age, having children)) | |
| ≠ work demands (workload, time pressure) post-program: mean HSE-MSIT subscale score (SD) on scale of 1 to 5: T0: 2.81 (0.48) vs. T1: 2.79 (0.58); p = 0.601 | Low Observational design, risk of confounding bias (several potential confounders ND (i.e., level of adherence to the intervention) or not integrated in analyses (i.e., age, having children)) | |
| ↑ job control post-program: mean HSE-MSIT subscale score (SD) on scale of 1 to 5: T0: 2.76 (0.67) vs. T1: 2.65 (0.65); p = 0.020 | Low Observational design, risk of confounding bias (several potential confounders ND (i.e., level of adherence to the intervention) or not integrated in analyses (i.e., age, having children)) | |
| ↑ managerial support post-program: mean HSE-MSIT subscale score (SD) on scale of 1 to 5: T0: 2.34 (0.88) vs. T1: 2.17 (0.98); p = 0.020 | Low Observational design, risk of confounding bias (several potential confounders ND (i.e., level of adherence to the intervention) or not integrated in analyses (i.e., age, having children)) | |
| ↑ peer support post-program: mean HSE-MSIT subscale score (SD) on scale of 1 to 5: T0: 2.12 (0.67) vs. T1: 1.93 (0.69); p = 0.001 | Low Observational design, risk of confounding bias (several potential confounders ND (i.e., level of adherence to the intervention) or not integrated in analyses (i.e., age, having children)) | |
| ↑ quality of relationships at work (harassment, tension, bullying) post-program: mean HSE-MSIT subscale score (SD) on scale of 1 to 5: T0: 2.23 (0.88) vs. T1: 2.04 (0.68); p = 0.001 | Low Observational design, risk of confounding bias (several potential confounders ND (i.e., level of adherence to the intervention) or not integrated in analyses (i.e., age, having children)) | |
| ≠ role clarity at work post-program: mean HSE-MSIT subscale score (SD) on scale of 1 to 5: T0: 1.71 (0.52) vs. T1: 1.69 (0.60); p = 0.798 | Low Observational design, risk of confounding bias (several potential confounders ND (i.e., level of adherence to the intervention) or not integrated in analyses (i.e., age, having children)) | |
| Improvement in how organizational change is managed and communicated at work post-program: mean HSE-MSIT subscale score (SD) on scale of 1 to 5: T0: 2.98 (0.49) vs. T1: 2.46 (0.79); p < 0.001 | Low Observational design, risk of confounding bias (several potential confounders ND (i.e., level of adherence to the intervention) or not integrated in analyses (i.e., age, having children)) | |
| Study reporting on the association between perception of adequate PPE, training and support and mental health indicators 13–25 months after SARS outbreak (no intervention described per se) (Maunder et al. 2006) [47] | 20% ↓ likelihood of post-traumatic stress (IES-R ≥ 26) post-outbreak, multivariate logistic regression model: β = −0.22; p = 0.01 | Low Observational design |
| 24% ↓ likelihood of emotional exhaustion (MBI-EE ≥ 27) post-outbreak, multivariate logistic regression model: β = −0.27; p = 0.002 | Low Observational design | |
| Likelihood of psychological distress (K10 ≥ 16) not reported because the “Training, protection and support” indicator was not significant in univariate models | Low Observational design |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nicolakakis, N.; Lafantaisie, M.; Letellier, M.-C.; Biron, C.; Vézina, M.; Jauvin, N.; Vivion, M.; Pelletier, M. Are Organizational Interventions Effective in Protecting Healthcare Worker Mental Health during Epidemics/Pandemics? A Systematic Literature Review. Int. J. Environ. Res. Public Health 2022, 19, 9653. https://doi.org/10.3390/ijerph19159653
Nicolakakis N, Lafantaisie M, Letellier M-C, Biron C, Vézina M, Jauvin N, Vivion M, Pelletier M. Are Organizational Interventions Effective in Protecting Healthcare Worker Mental Health during Epidemics/Pandemics? A Systematic Literature Review. International Journal of Environmental Research and Public Health. 2022; 19(15):9653. https://doi.org/10.3390/ijerph19159653
Chicago/Turabian StyleNicolakakis, Nektaria, Maude Lafantaisie, Marie-Claude Letellier, Caroline Biron, Michel Vézina, Nathalie Jauvin, Maryline Vivion, and Mariève Pelletier. 2022. "Are Organizational Interventions Effective in Protecting Healthcare Worker Mental Health during Epidemics/Pandemics? A Systematic Literature Review" International Journal of Environmental Research and Public Health 19, no. 15: 9653. https://doi.org/10.3390/ijerph19159653
APA StyleNicolakakis, N., Lafantaisie, M., Letellier, M. -C., Biron, C., Vézina, M., Jauvin, N., Vivion, M., & Pelletier, M. (2022). Are Organizational Interventions Effective in Protecting Healthcare Worker Mental Health during Epidemics/Pandemics? A Systematic Literature Review. International Journal of Environmental Research and Public Health, 19(15), 9653. https://doi.org/10.3390/ijerph19159653