
Functioning of the EROS-R Scale in a Clinical Sample of Psychiatric Patients: New Psychometric Evidence from the Classical Test Theory and the Item Response Theory

 , and
, and
Abstract
:1. Introduction
2. Method
2.1. Design
2.2. Participants
3. Measures
3.1. Environmental Reward Observation Scale (EROS-R)
3.2. Generalized Anxiety Disorder Scale (GAD-7)
3.3. Patient Health Questionnaire (PHQ-9)
3.4. Procedure
3.5. Data Analysis
4. Results
4.1. Descriptive Analysis
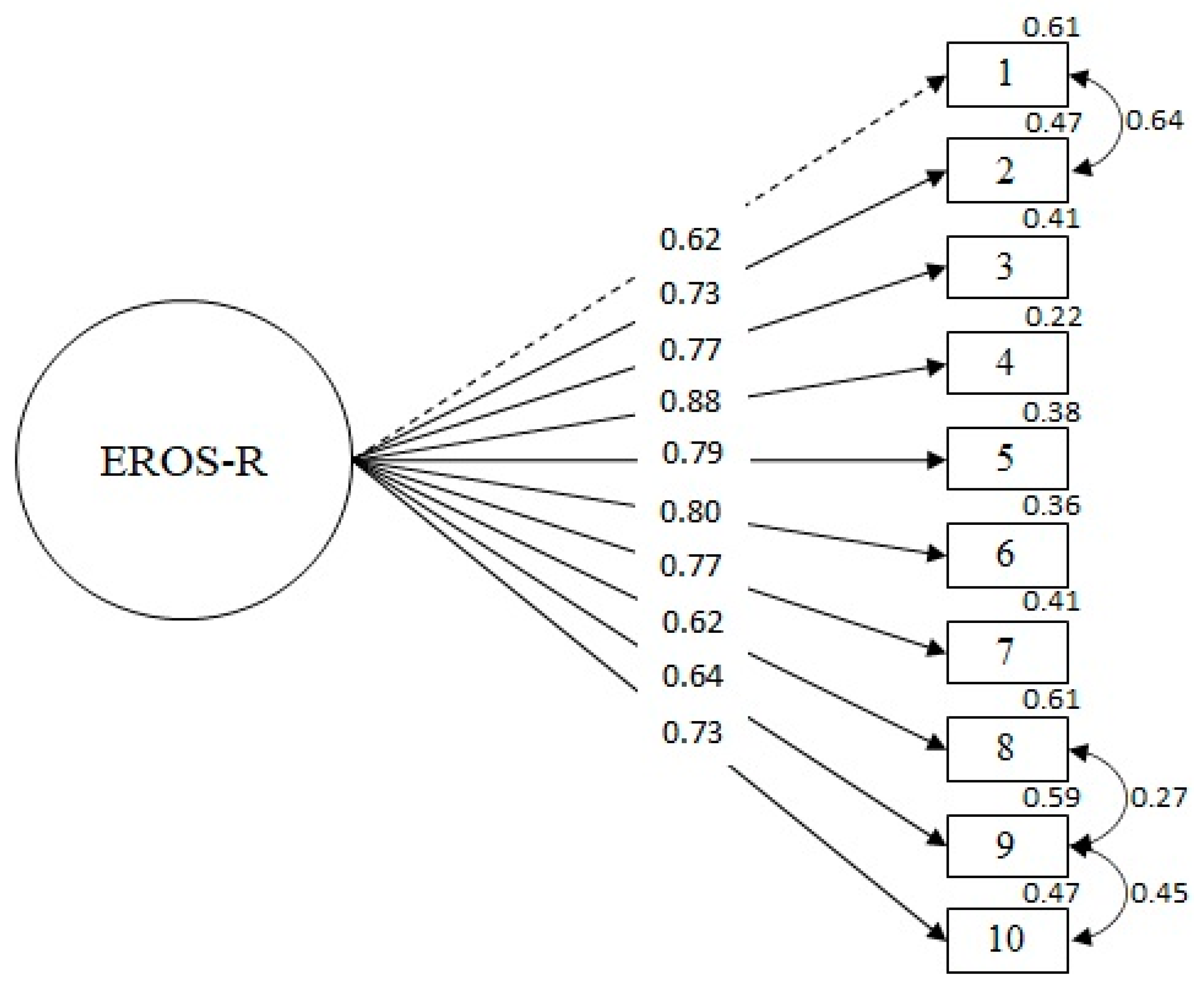
4.2. Validity Based on Internal Structure
4.3. Reliability
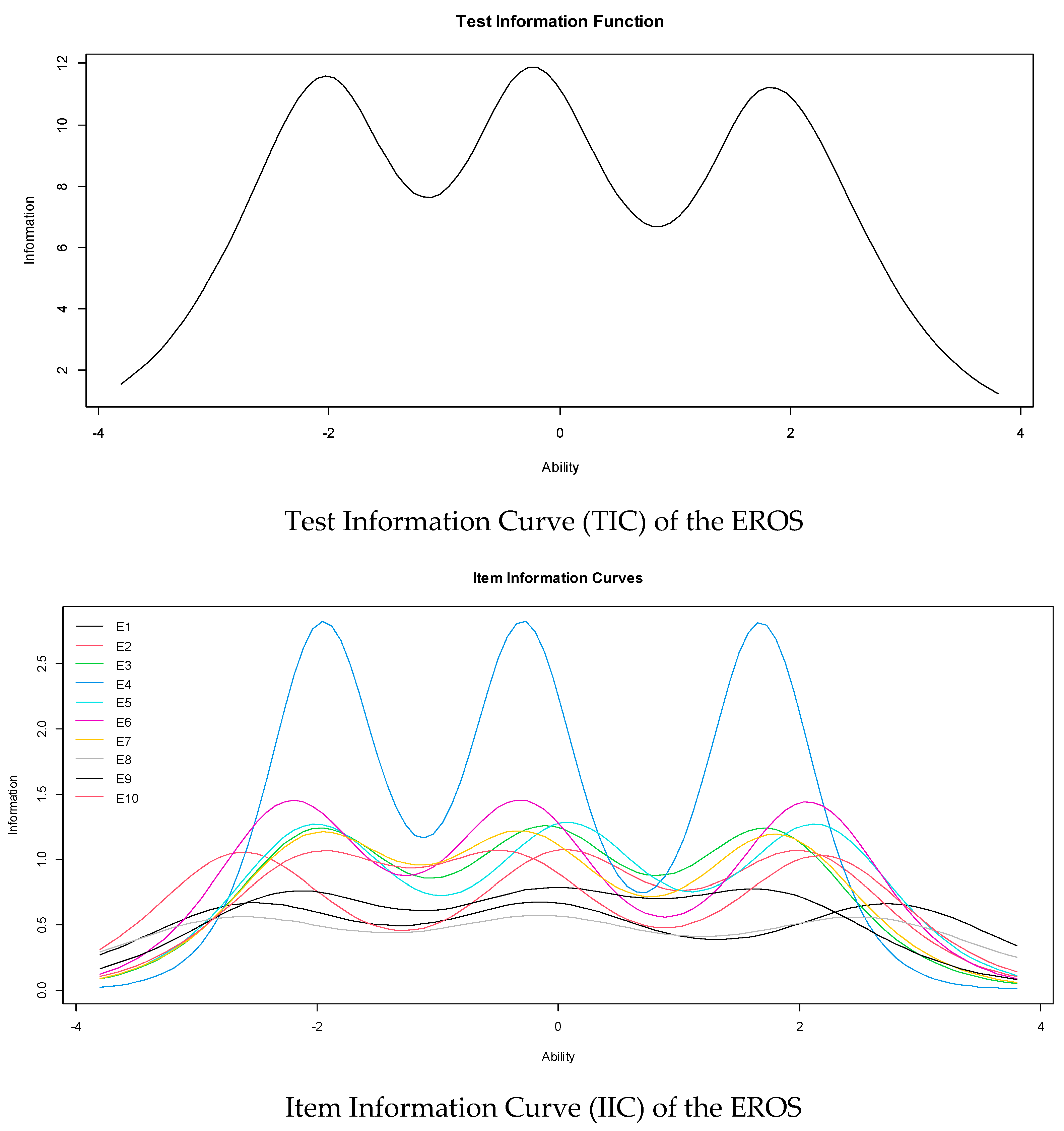
4.4. Item Response Theory Model
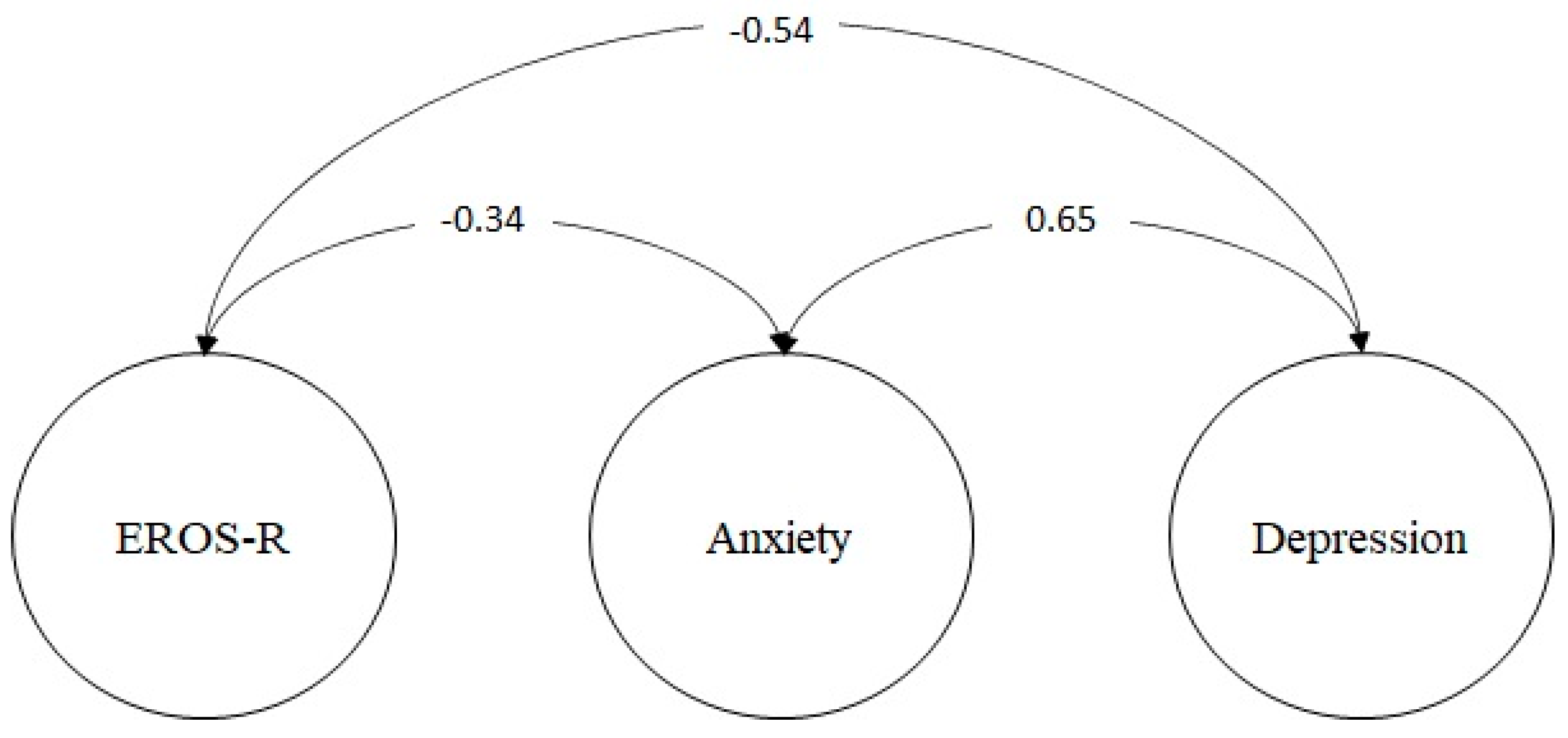
4.5. Validity Based on the Relationship to Other Constructs
5. Discussion
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hayes, S.C. Acceptance and commitment therapy, relational frame theory, and the third wave of behavioral and cognitive therapies. Behav. Ther. 2004, 35, 639–665. [Google Scholar] [CrossRef]
- Martin, F.; Oliver, T. Behavioral activation for children and adolescents: A systematic review of progress and promise. Eur. Child Adolesc. Psychiatry 2019, 28, 427–441. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Vispo, C.; Martínez, Ú.; López-Durán, A.; Fernández del Río, E.; Becoña, E. Effects of behavioural activation on substance use and depression: A systematic review. Subst. Abuse Treat. Prev. Policy 2018, 13, 36. [Google Scholar] [CrossRef] [PubMed]
- Tindall, L.; Mikocka-Walus, A.; McMillan, D.; Wright, B.; Hewitt, C.; Gascoyne, S. Is behavioural activation effective in the treatment of depression in young people? A systematic review and meta-analysis. Psychol. Psychother. Theory Res. Pract. 2017, 90, 770–796. [Google Scholar] [CrossRef]
- Orgeta, V.; Brede, J.; Livingston, G. Behavioural activation for depression in older people: Systematic review and meta-analysis. Br. J. Psychiatry 2017, 211, 274–279. [Google Scholar] [CrossRef]
- Oates, L.L.; Moghaddam, N.; Evangelou, N.; Das Nair, R. Behavioural activation treatment for depression in individuals with neurological conditions: A systematic review. Clin. Rehabil. 2020, 34, 310–319. [Google Scholar] [CrossRef]
- Martell, C.R.; Dimidjian, S.; Herman-Dunn, R. Behavioral Activation for Depression. In A Clinician’s Guide, 2nd ed.; The Guilford Press: New York, NY, USA, 2022. [Google Scholar]
- Lewinsohn, P.M. A behavioral approach to depresion. In The Psychology of Depression: Contemporary Theory and Research; Friedman, R.M., Katz, M.M., Eds.; Wiley: Hoboken, NJ, USA, 1974; pp. 157–185. [Google Scholar]
- Hayes, S.C.; Wilson, K.G.; Gifford, E.V.; Follette, V.M.; Strosahl, K. Experiential Avoidance and Behavioral Disorders: A Functional Dimensional Approach to Diagnosis and Treatment Kirk Strosahl Group Health Cooperative. J. Consult. Clin. Psychol. 1996, 64, 1152–1168. [Google Scholar] [CrossRef]
- Kanter, J.W.; Manos, R.C.; Bowe, W.M.; Baruch, D.E.; Busch, A.; Rusch, L.C. What is behavioral activation? A review of the empirical literature. Clin. Psychol. Rev. 2010, 30, 608–620. [Google Scholar] [CrossRef] [PubMed]
- Dimidjian, S.; Barrera, M.; Martell, C.; Muñoz, R.F.; Lewinsohn, P.M. The Origins and Current Status of Behavioral Activation Treatments for Depression. Annu. Rev. Clin. Psychol. 2011, 7, 1–38. [Google Scholar] [CrossRef] [PubMed]
- Hopko, D.R.; Lejuez, C.; Lepage, J.P.; Hopko, S.D.; McNeil, D.W. A Brief Behavioral Activation Treatment for Depression: A randomized pilot trial within an inpatient psychiatric hospital. Behav. Modif. 2003, 27, 458–469. [Google Scholar] [CrossRef]
- Curran, J.; Lawson, P.; Houghton, S.; Gournay, K. Implementing behavioural activation in inpatient psychiatric wards. J. Ment. Health Train. Educ. Pract. 2007, 2, 28–35. [Google Scholar] [CrossRef]
- Snarski, M.; Scogin, F.; DiNapoli, E.; Presnell, A.; McAlpine, J.; Marcinak, J. The Effects of Behavioral Activation Therapy with Inpatient Geriatric Psychiatry Patients. Behav. Ther. 2011, 42, 100–108. [Google Scholar] [CrossRef] [PubMed]
- Collado, A.; Castillo, S.D.; Maero, F.; Lejuez, C.; MacPherson, L. Pilot of the Brief Behavioral Activation Treatment for Depression in Latinos With Limited English Proficiency: Preliminary Evaluation of Efficacy and Acceptability. Behav. Ther. 2014, 45, 102–115. [Google Scholar] [CrossRef]
- Folke, F.; Hursti, T.; Tungström, S.; Söderberg, P.; Kanter, J.W.; Kuutmann, K.; Olofsson, H.; Ekselius, L. Behavioral activation in acute inpatient psychiatry: A multiple baseline evaluation. J. Behav. Ther. Exp. Psychiatry 2015, 46, 170–181. [Google Scholar] [CrossRef]
- LeComte, T.; Liberman, R.P.; Wallace, C.J. Identifying and Using Reinforcers to Enhance the Treatment of Persons with Serious Mental Illness. Psychiatr. Serv. 2000, 51, 1312–1314. [Google Scholar] [CrossRef]
- Hopko, D.R.; Sanchez, L.; Hopko, S.D.; Dvir, S.; Lejuez, C. Behavioral Activation and the Prevention of Suicidal Behaviors in Patients With Borderline Personality Disorder. J. Pers. Disord. 2003, 17, 460–478. [Google Scholar] [CrossRef]
- Armento, M.E.; Hopko, D.R. The Environmental Reward Observation Scale (EROS): Development, Validity, and Reliability. Behav. Ther. 2007, 38, 107–119. [Google Scholar] [CrossRef]
- Aoki, S.; Doi, S.; Horiuchi, S.; Takagaki, K.; Kawamura, A.; Umeno, R.; Fujita, M.; Kitagawa, N.; Sakano, Y. Mediating effect of environmental rewards on the relation between goal-directed behaviour and anhedonia. Curr. Psychol. 2019, 40, 3651–3658. [Google Scholar] [CrossRef]
- Doi, S.; Yokomitsu, K.; Sakano, Y. Relationships among Valued Action, Behavioral Activation, Avoidance, and Reinforcement in a Sample of College Students. Psychol. Rep. 2016, 118, 5–22. [Google Scholar] [CrossRef]
- Maitland, D.W.M.; Neilson, E.C.; Munoz, E.A.; Ybanez, A.; Murray, A.L. The Impact of an Enriched Environment on the Relationship Between Activation and Depression in Latinx and Non-Latinx Students. Psychol. Rec. 2019, 69, 541–550. [Google Scholar] [CrossRef]
- Vázquez, F.L.; López, L.; Blanco, V.; Otero, P.; Torres, Á.J.; Ferraces, M.J. The impact of decreased environmental reward in predicting depression severity in caregivers. An Psicol. 2019, 35, 357–363. [Google Scholar] [CrossRef]
- Takagaki, K.; Okamoto, Y.; Jinnin, R.; Mori, A.; Nishiyama, Y.; Yamamura, T.; Yokoyama, S.; Shiota, S.; Okamoto, Y.; Miyake, Y.; et al. Behavioral activation for late adolescents with subthreshold depression: A randomized controlled trial. Eur. Child Adolesc. Psychiatry 2016, 25, 1171–1182. [Google Scholar] [CrossRef] [PubMed]
- Kern, D.; Busch, A.; Schneider, K.L.; Miller, S.A.; Appelhans, B.M.; Waring, M.E.; Whited, M.C.; Pagoto, S. Psychosocial factors associated with treatment outcomes in women with obesity and major depressive disorder who received behavioral activation for depression. J. Behav. Med. 2019, 42, 522–533. [Google Scholar] [CrossRef]
- Otero, P.; Hita, I.; Torres, J.; Vázquez, F.L. Brief Psychological Intervention Through Mobile App and Conference Calls for the Prevention of Depression in Non-Professional Caregivers: A Pilot Study. Int. J. Environ. Res. Public Health 2020, 17, 4578. [Google Scholar] [CrossRef]
- Fernández-Rodríguez, C.; González-Fernández, S.; Coto-Lesmes, R.; Pedrosa, I. Behavioral Activation and Acceptance and Commitment Therapy in the Treatment of Anxiety and Depression in Cancer Survivors: A Randomized Clinical Trial. Behav. Modif. 2021, 45, 822–859. [Google Scholar] [CrossRef]
- Takagaki, K.; Jinnin, R.; Yokoyama, S.; Mori, A.; Kambara, K.; Okamoto, Y.; Miyake, Y.; Kagawa, F.; Okamoto, Y. Relations Among Clinical Factors After Behavioral Activation for Subthreshold Depression. Int. J. Cogn. Ther. 2021, 14, 612–622. [Google Scholar] [CrossRef]
- Barraca, J.; Pérez-Álvarez, M. Adaptación española del Environmental Reward Observation (EROS). Ansiedad Estrés 2010, 16, 95–107. [Google Scholar]
- Fernández-Rodríguez, C.; González-Fernández, S.; Pedrosa, I. Psychometric validation of the Environmental Reward Observation Scale (EROS) in breast cancer survivors. Anales Psicología Ann. Psychol. 2020, 36, 74–83. [Google Scholar] [CrossRef]
- Vilca, L.W.; Echebaudes-Ilizarbe, R.I.; Aquino-Hidalgo, J.M.; Ventura-León, J.; Martinez-Munive, R.; White, M. Psychometric Properties of the Environmental Reward Observation Scale: Study on Its Internal Structure, Factor Invariance, and Method Effect Associated with Its Negative Items. Psychol. Rep. 2022, 125, 649–675. [Google Scholar] [CrossRef]
- Zanon, C.; Hutz, C.; Yoo, H.; Hambleton, R.K. An application of item response theory to psychological test development. Psicol. Reflexão Crítica 2016, 29, 1–10. [Google Scholar] [CrossRef]
- Ato, M.; López-García, J.J.; Benavente, A. Un sistema de clasificación de los diseños de investigación en psicología. An. Psicol. Ann. Psychol. 2013, 29, 1038–1059. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.W.; Löwe, B. A Brief Measure for Assessing Generalized Anxiety Disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Campayo, J.; Zamorano, E.; A Ruiz, M.; Pardo, A.; Perez-Paramo, M.; Lopez-Gomez, V.; Freire, O.; Rejas, J. Cultural adaptation into Spanish of the generalized anxiety disorder-7 (GAD-7) scale as a screening tool. Health Qual. Life Outcomes 2010, 8, 8. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B. Validation and utility of a self-report version of PRIME-MD: The PHQ primary care study. Primary Care Evaluation of Mental Disorders. Patient Health Questionnaire. JAMA 1999, 282, 1737–1744. [Google Scholar] [CrossRef]
- Zhong, Q.; Gelaye, B.; Fann, J.R.; Sanchez, S.E.; Williams, M.A. Cross-cultural validity of the Spanish version of PHQ-9 among pregnant Peruvian women: A Rasch item response theory analysis. J. Affect. Disord. 2014, 158, 148–153. [Google Scholar] [CrossRef]
- World Medical Association. World Medical Association Declaration of Helsinki Ethical Principles for Medical Research Involving Human Subjects. Clin. Rev. Educ. Spec. 2013, 27, 2191–2194. [Google Scholar] [CrossRef]
- Brown, T.A. Confirmatory Factor Analysis for Applied Research, 2nd ed.; The Guilford Press: New York, NY, USA, 2015. [Google Scholar]
- Kline, R.B. Principles and Practice of Structural Equation Modeling, 4th ed.; The Guilford Press: New York, NY, USA, 2015. [Google Scholar]
- Schumacker, R.E.; Lomax, R.G. A Beginner’s Guide to Structural Equation Modeling, 4th ed.; Routledge: London, UK, 2015. [Google Scholar]
- Cronbach, L.J. Coefficient alpha and the internal structure of tests. Psychometrika 1951, 16, 297–334. [Google Scholar] [CrossRef]
- Bentler, P.M. Alpha, Dimension-Free, and Model-Based Internal Consistency Reliability. Psychometrika 2009, 74, 137–143. [Google Scholar] [CrossRef]
- Green, S.B.; Yang, Y. Reliability of Summed Item Scores Using Structural Equation Modeling: An Alternative to Coefficient Alpha. Psychometrika 2009, 74, 155–167. [Google Scholar] [CrossRef]
- Raykov, T.; Hancock, G.R. Examining change in maximal reliability for multiple-component measuring instruments. Br. J. Math. Stat. Psychol. 2005, 58, 65–82. [Google Scholar] [CrossRef]
- Samejima, F. Graded Response Model. In Handbook of Modern Item Response Theory; van der Linden, W.J., Hambleton, R.K., Eds.; Springer: Berlin/Heidelberg, Germany, 1997; pp. 85–100. [Google Scholar] [CrossRef]
- Hambleton, R.K.; van der Linden, W.J.; Wells, C.S. IRT models for the analysis of polytomously scored data: Brief and selected history of model building advances. In Handbook of Polytomous Item Response Theory Models; Nering, M.L., Ostini, R., Eds.; Routledge/Taylor & Francis Group: Abingdon, UK, 2010; pp. 21–42. [Google Scholar]
- Cai, L.; Hansen, M. Limited-information goodness-of-fit testing of hierarchical item factor models. Br. J. Math. Stat. Psychol. 2013, 66, 245–276. [Google Scholar] [CrossRef]
- Maydeu-Olivares, A.; Joe, H. Assessing Approximate Fit in Categorical Data Analysis. Multivar. Behav. Res. 2014, 49, 305–328. [Google Scholar] [CrossRef] [PubMed]
- Lubbe, D.; Schuster, C. A Graded Response Model Framework for Questionnaires with Uniform Response Formats. Appl. Psychol. Meas. 2019, 43, 290–302. [Google Scholar] [CrossRef]
- Kang, T.; Chen, T.T. Performance of the Generalized S-X2 Item Fit Index for Polytomous IRT Models. J. Educ. Meas. 2008, 45, 391–406. [Google Scholar] [CrossRef]
- Reeve, B.B.; Hays, R.D.; Bjorner, J.B.; Cook, K.F.; Crane, P.K.; Teresi, J.A.; Thissen, D.; Revicki, D.A.; Weiss, D.J.; Hambleton, R.K.; et al. Psychometric evaluation and calibration of health-related quality of life item banks: Plans for the Patient-Reported Outcomes Measurement Information System (PROMIS). Med. Care 2007, 45 (Suppl. S1), S22–S31. [Google Scholar] [CrossRef]
- Bean, G.J.; Bowen, N.K. Item Response Theory and Confirmatory Factor Analysis: Complementary Approaches for Scale Development. J. Evid. Based Soc. Work 2021, 18, 597–618. [Google Scholar] [CrossRef]
- Rosseel, Y. lavaan: AnRPackage for Structural Equation Modeling. J. Stat. Softw. 2012, 48, 1–36. [Google Scholar] [CrossRef]
- Rizopoulos, D. ltm: An R Package for Latent Variable Modeling and Item Response Theory Analyses. J. Stat. Softw. 2006, 17, 1–25. [Google Scholar] [CrossRef]
- RStudio Team. RStudio: Integrated Development Environment for R; RStudio, Inc.: Boston, MA, USA, 2022; Available online: http://www.rstudio.com/ (accessed on 22 March 2022).
- R Core Team. A Language and Environment for Statistical Computing, R version 3.6.1; R Foundation for Statistical Computing: Vienna, Austria, 2019; Available online: http://www.r-project.org/ (accessed on 22 March 2022).
- Saris, W.E.; Satorra, A.; Van Der Veld, W.M. Testing Structural Equation Models or Detection of Misspecifications? Struct. Equ. Model. 2009, 16, 561–582. [Google Scholar] [CrossRef]
- Hasson-Ohayon, I.; Arnon-Ribenfeld, N.; Hamm, J.A.; Lysaker, P.H. Agency before action: The application of behavioral activation in psychotherapy with persons with psychosis. Psychotherapy 2017, 54, 245–251. [Google Scholar] [CrossRef]
- González-Fernández, S.; Fernández-Rodríguez, C.; Paz-Caballero, M.D. Treating anxiety and depression of cancer survivors: Behavioral activation versus acceptance and commitment therapy. Psicothema 2018, 30, 14–20. [Google Scholar] [CrossRef]
- Okumura, A. Terapia grupal de Activación Conductual en pacientes de un centro de intervención comunitario de Lima, Perú. Acta Psicológica Peru. 2018, 2, 380–397. Available online: http://revistas.autonoma.edu.pe/index.php/ACPP/article/view/137/113 (accessed on 22 March 2022).
- Martínez-Vispo, C.; Rodríguez-Cano, R.; López-Durán, A.; Senra, C.; Del Río, E.F.; Becoña, E. Cognitive-behavioral treatment with behavioral activation for smoking cessation: Randomized controlled trial. PLoS ONE 2019, 14, e0214252. [Google Scholar] [CrossRef]
- Malhotra, N.K.; Kim, S.S.; Patil, A. Common Method Variance in IS Research: A Comparison of Alternative Approaches and a Reanalysis of Past Research. Manag. Sci. 2006, 52, 1865–1883. [Google Scholar] [CrossRef]
- Hair, J.F.; Anderson, R.E.; Babin, B.J.; Black, W.C. Multivariate Data Analysis: A Global Perspective, 7th ed.; Pearson Education: London, UK, 2010. [Google Scholar]
- Mueller, M.O.; Hancock, G.R. Structural equation modeling. In The Reviewer’s Guide to Quantitative Methods in the Social Sciences, 2nd ed.; Hancock, G.R., Stapleton, L.M., Mueller, R., Eds.; Routledge: London, UK, 2018. [Google Scholar]
- Gu, F.; Little, T.D.; Kingston, N.M. Misestimation of Reliability Using Coefficient Alpha and Structural Equation Modeling When Assumptions of Tau-Equivalence and Uncorrelated Errors Are Violated. Methodology 2013, 9, 30–40. [Google Scholar] [CrossRef]
- Dunn, T.J.; Baguley, T.; Brunsden, V. From alpha to omega: A practical solution to the pervasive problem of internal consistency estimation. Br. J. Psychol. 2014, 105, 399–412. [Google Scholar] [CrossRef]
- Crutzen, R.; Peters, G.-J.Y. Scale quality: Alpha is an inadequate estimate and factor-analytic evidence is needed first of all. Health Psychol. Rev. 2017, 11, 242–247. [Google Scholar] [CrossRef] [PubMed]
- McDowell, I. Measuring Health: A Guide to Rating Scales and Questionnaires, 3rd ed.; Oxford University Press: Oxford, UK, 2006. [Google Scholar] [CrossRef]
- Cuijpers, P.; van Straten, A.; Warmerdam, L. Behavioral activation treatments of depression: A meta-analysis. Clin. Psychol. Rev. 2007, 27, 318–326. [Google Scholar] [CrossRef]
- Manos, R.C.; Kanter, J.W.; Busch, A.M. A critical review of assessment strategies to measure the behavioral activation model of depression. Clin. Psychol. Rev. 2010, 30, 547–561. [Google Scholar] [CrossRef]
- Huys, Q.J.; A Pizzagalli, D.; Bogdan, R.; Dayan, P. Mapping anhedonia onto reinforcement learning: A behavioural meta-analysis. Biol. Mood Anxiety Disord. 2013, 3, 12. [Google Scholar] [CrossRef] [PubMed]
- Safra, L.; Chevallier, C.; Palminteri, S. Depressive symptoms are associated with blunted reward learning in social contexts. PLoS Comput. Biol. 2019, 15, e1007224. [Google Scholar] [CrossRef] [PubMed]
- McCauley, E.; Gudmundsen, G.; Schloredt, K.; Martell, C.; Rhew, I.; Hubley, S.; Dimidjian, S. The Adolescent Behavioral Activation Program: Adapting Behavioral Activation as a Treatment for Depression in Adolescence. J. Clin. Child Adolesc. Psychol. 2015, 45, 291–304. [Google Scholar] [CrossRef]
- Stein, A.T.; Carl, E.; Cuijpers, P.; Karyotaki, E.; Smits, J.A.J. Looking beyond depression: A meta-analysis of the effect of behavioral activation on depression, anxiety, and activation. Psychol. Med. 2021, 51, 1491–1504. [Google Scholar] [CrossRef]
- Grant, D.M.; White, E.J. The Influence of Anxiety on Cognitive Control Processes. In Oxford Research Encyclopedia of Psychology; Oxford University Press: Oxford, UK, 2016. [Google Scholar] [CrossRef]
- Harlé, K.M.; Guo, D.; Zhang, S.; Paulus, M.P.; Yu, A.J. Anhedonia and anxiety underlying depressive symptomatology have distinct effects on reward-based decision-making. PLoS ONE 2017, 12, e0186473. [Google Scholar] [CrossRef] [PubMed]
- Colosi, R. Negatively worded questions cause respondent confusion. In Proceedings of the Survey Research Methods Section; American Statistical Association: Suitland Road, Suitland, 2005; pp. 2896–2903. [Google Scholar]
- Merritt, S.M. The Two-Factor Solution to Allen and Meyer’s (1990) Affective Commitment Scale: Effects of Negatively Worded Items. J. Bus. Psychol. 2012, 27, 421–436. [Google Scholar] [CrossRef]
- Weems, G.H.; Onwuegbuzie, A.J.; Collins, K.M. The Role of Reading Comprehension in Responses to Positively and Negatively Worded Items on Rating Scales. Eval. Res. Educ. 2006, 19, 3–20. [Google Scholar] [CrossRef]
- Meisenberg, G.; Williams, A. Are acquiescent and extreme response styles related to low intelligence and education? Pers. Individ. Differ. 2008, 44, 1539–1550. [Google Scholar] [CrossRef]
- Hayes, S.C.; Hofmann, S.G. Process-Based CBT: The Science and Core Clinical Competencies of Cognitive Behavioral Therapy; New Harbinger Publications: Oakland, CA, USA, 2018. [Google Scholar]
- Hofmann, S.G.; Hayes, S.C. The Future of Intervention Science: Process-Based Therapy. Clin. Psychol. Sci. 2019, 7, 37–59. [Google Scholar] [CrossRef]
- Tull, M.T.; Gratz, K.L.; Latzman, R.D.; Kimbrel, N.A.; Lejuez, C. Reinforcement Sensitivity Theory and emotion regulation difficulties: A multimodal investigation. Pers. Individ. Differ. 2010, 49, 989–994. [Google Scholar] [CrossRef]
- Ryba, M.M.; Hopko, D.R. Gender Differences in Depression: Assessing Mediational Effects of Overt Behaviors and Environmental Reward through Daily Diary Monitoring. Depress. Res. Treat. 2012, 2012, 865679. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Items | E1 | E2 | E3 | E4 | E5 | E6 | E7 | E8 | E9 | E10 |
|---|---|---|---|---|---|---|---|---|---|---|
| E1 | 1 | |||||||||
| E2 | 0.80 | 1 | ||||||||
| E3 | 0.50 | 0.62 | 1 | |||||||
| E4 | 0.63 | 0.65 | 0.67 | 1 | ||||||
| E5 | 0.55 | 0.60 | 0.55 | 0.73 | 1 | |||||
| E6 | 0.41 | 0.53 | 0.52 | 0.73 | 0.70 | 1 | ||||
| E7 | 0.43 | 0.52 | 0.58 | 0.64 | 0.59 | 0.62 | 1 | |||
| E8 | 0.30 | 0.42 | 0.56 | 0.48 | 0.41 | 0.51 | 0.51 | 1 | ||
| E9 | 0.40 | 0.35 | 0.53 | 0.56 | 0.42 | 0.56 | 0.53 | 0.56 | 1 | |
| E10 | 0.43 | 0.52 | 0.53 | 0.58 | 0.50 | 0.57 | 0.66 | 0.53 | 0.70 | 1 |
| M | 2.60 | 2.59 | 2.63 | 2.68 | 2.52 | 2.63 | 2.66 | 2.56 | 2.63 | 2.70 |
| SD | 0.64 | 0.68 | 0.70 | 0.63 | 0.67 | 0.62 | 0.67 | 0.63 | 0.73 | 0.59 |
| g1 | −0.06 | 0.22 | −0.06 | −0.13 | −0.23 | −0.26 | −0.46 | 0.03 | 0.19 | −0.83 |
| g2 | −0.19 | −0.31 | −0.19 | −0.07 | −0.16 | −0.03 | 0.24 | −0.25 | −0.43 | 0.84 |
| Items | Item Parameters | Item Fit | Model Fit Indices | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| a | b1 | b2 | b3 | S-X2 (df) | p | RMSEA.S-X2 | M2 (df) | p | RMSEA | SRMSR | TLI | CFI | |
| E1 | 1.62 | −2.55 | −0.12 | 2.75 | 13.65 (13) | 0.399 | 0.015 | 29.05 (15) | 0.016 | 0.064 | 0.068 | 0.95 | 0.97 |
| E2 | 2.05 | −2.62 | 0.04 | 2.08 | 14.60 (14) | 0.406 | 0.014 | ||||||
| E3 | 2.21 | −1.99 | −0.11 | 1.74 | 24.32 (16) | 0.083 | 0.048 | ||||||
| E4 | 3.35 | −1.95 | −0.29 | 1.67 | 13.96 (12) | 0.303 | 0.027 | ||||||
| E5 | 2.25 | −2.02 | 0.08 | 2.14 | 20.55 (13) | 0.082 | 0.051 | ||||||
| E6 | 2.40 | −2.21 | −0.31 | 2.07 | 21.09 (13) | 0.071 | 0.052 | ||||||
| E7 | 2.17 | −1.99 | −0.29 | 1.81 | 28.13 (14) | 0.014 | 0.060 | ||||||
| E8 | 1.48 | −2.68 | −0.14 | 2.52 | 15.74 (16) | 0.472 | 0.000 | ||||||
| E9 | 1.72 | −2.19 | −0.08 | 1.74 | 17.09 (18) | 0.516 | 0.000 | ||||||
| E10 | 2.02 | −2.03 | −0.41 | 2.18 | 21.94 (14) | 0.080 | 0.050 | ||||||
| Structural Model | |||||||
|---|---|---|---|---|---|---|---|
| χ2 | df | p | RMSEA | CI 90% | SRMR | CFI | TLI |
| 581.02 | 293 | 0.000 | 0.066 | 0.058–0.074 | 0.086 | 0.92 | 0.91 |
| Measurement Models | |||||||
| Items | EROS-R | Anxiety | Depression | ||||
| λ (error) | λ (error) | λ (error) | |||||
| 1 | 0.65 (0.57) | 0.73 (0.47) | 0.56 (0.68) | ||||
| 2 | 0.70 (0.51) | 0.75 (0.43) | 0.72 (0.49) | ||||
| 3 | 0.72 (0.47) | 0.77 (0.40) | 0.67 (0.54) | ||||
| 4 | 0.89 (0.22) | 0.77 (0.41) | 0.65 (0.57) | ||||
| 5 | 0.79 (0.37) | 0.78 (0.39) | 0.58 (0.66) | ||||
| 6 | 0.80 (0.36) | 0.58 (0.66) | 0.59 (0.66) | ||||
| 7 | 0.74 (0.44) | 0.69 (0.51) | 0.52 (0.72) | ||||
| 8 | 0.61 (0.63) | 0.51 (0.73) | |||||
| 9 | 0.70 (0.51) | 0.81 (0.34) | |||||
| 10 | 0.79 (0.38) | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vilca, L.W.; Chambi-Mamani, E.L.; Quispe-Kana, E.D.; Hernández-López, M.; Caycho-Rodríguez, T. Functioning of the EROS-R Scale in a Clinical Sample of Psychiatric Patients: New Psychometric Evidence from the Classical Test Theory and the Item Response Theory. Int. J. Environ. Res. Public Health 2022, 19, 10062. https://doi.org/10.3390/ijerph191610062
Vilca LW, Chambi-Mamani EL, Quispe-Kana ED, Hernández-López M, Caycho-Rodríguez T. Functioning of the EROS-R Scale in a Clinical Sample of Psychiatric Patients: New Psychometric Evidence from the Classical Test Theory and the Item Response Theory. International Journal of Environmental Research and Public Health. 2022; 19(16):10062. https://doi.org/10.3390/ijerph191610062
Chicago/Turabian StyleVilca, Lindsey W., Evelyn L. Chambi-Mamani, Emely D. Quispe-Kana, Mónica Hernández-López, and Tomás Caycho-Rodríguez. 2022. "Functioning of the EROS-R Scale in a Clinical Sample of Psychiatric Patients: New Psychometric Evidence from the Classical Test Theory and the Item Response Theory" International Journal of Environmental Research and Public Health 19, no. 16: 10062. https://doi.org/10.3390/ijerph191610062
APA StyleVilca, L. W., Chambi-Mamani, E. L., Quispe-Kana, E. D., Hernández-López, M., & Caycho-Rodríguez, T. (2022). Functioning of the EROS-R Scale in a Clinical Sample of Psychiatric Patients: New Psychometric Evidence from the Classical Test Theory and the Item Response Theory. International Journal of Environmental Research and Public Health, 19(16), 10062. https://doi.org/10.3390/ijerph191610062