
The Effect of the Referral System on the Accessibility of Healthcare Services: A Case Study of the Wuhan Metropolitan Development Zone

Abstract
:1. Introduction
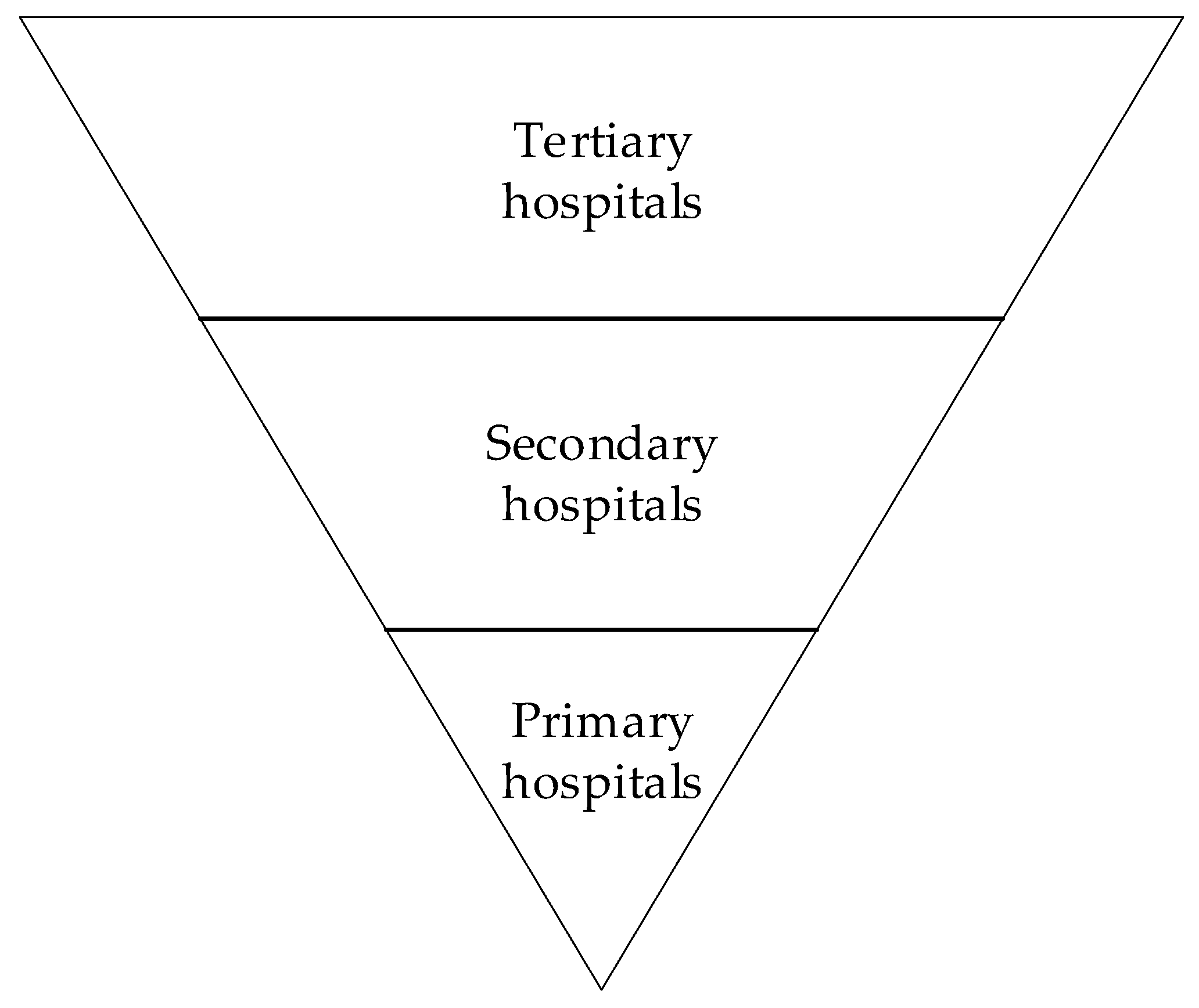
2. The Hierarchical Medical System and Referral System in China
3. Materials and Methods
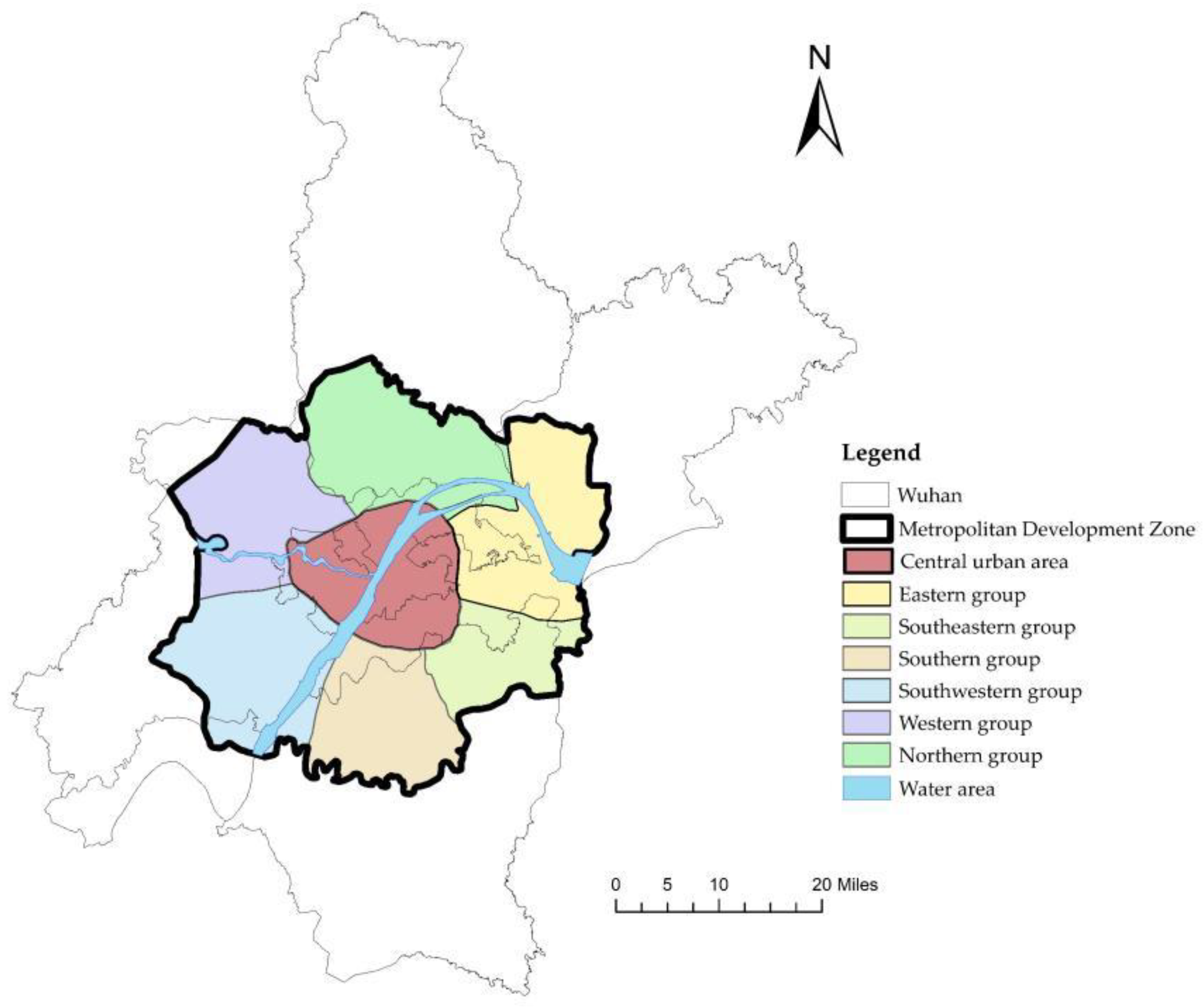
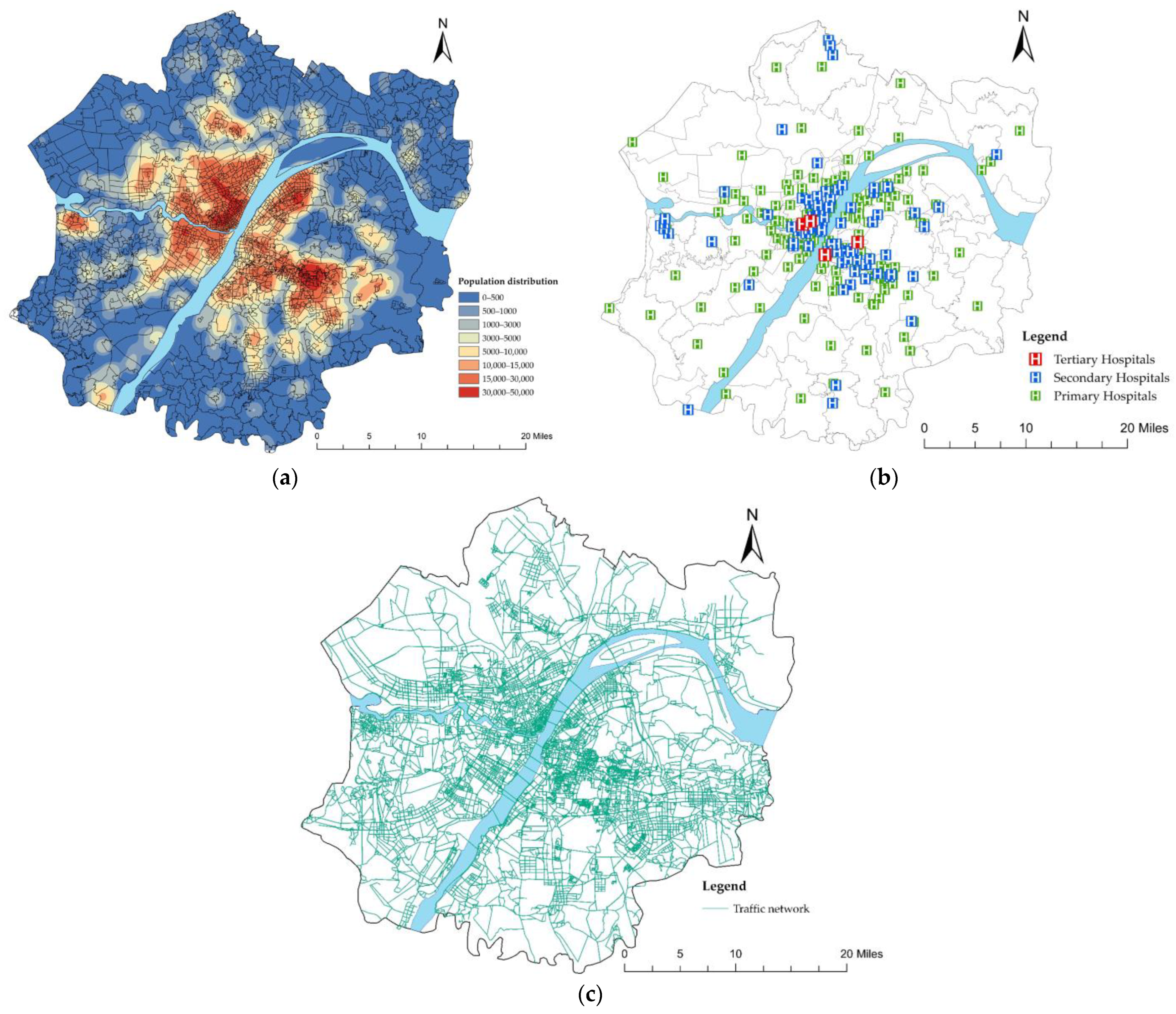
3.1. Study Area and Data
3.2. Method
3.2.1. Potential Model
3.2.2. Setting of Parameters and Standards
4. Result
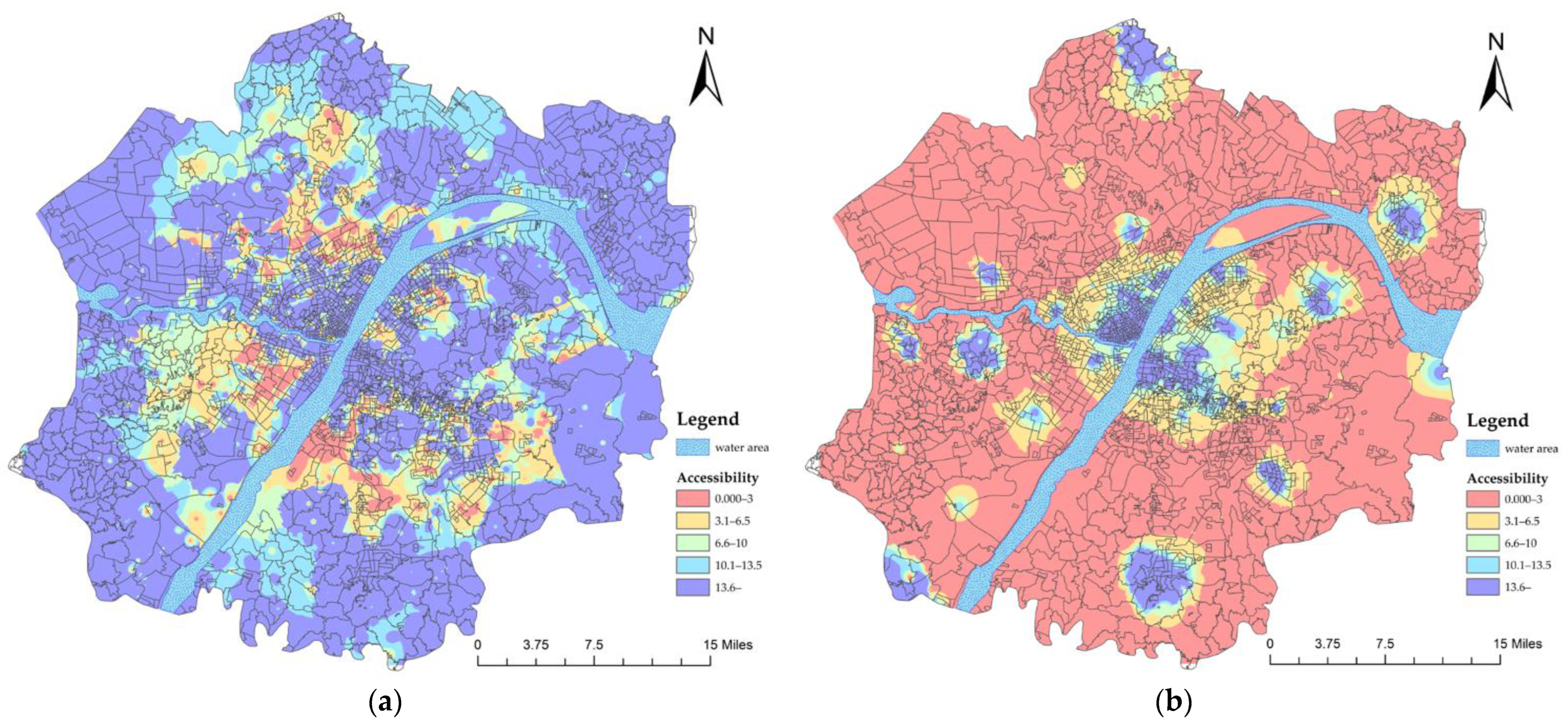
4.1. Healthcare Services Accessibility before the Referral System
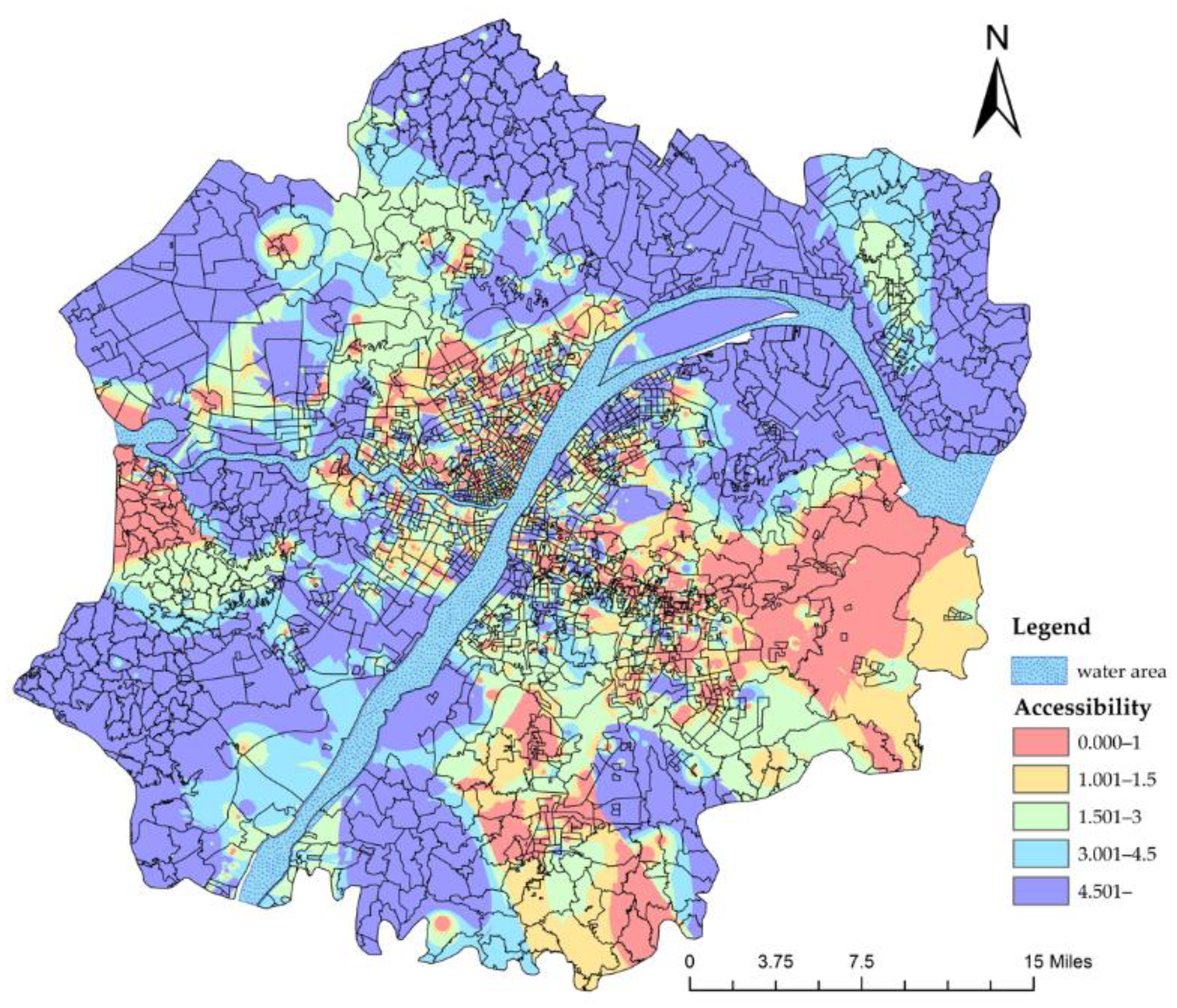
4.1.1. Accessibility of Secondary and Tertiary Hospitals
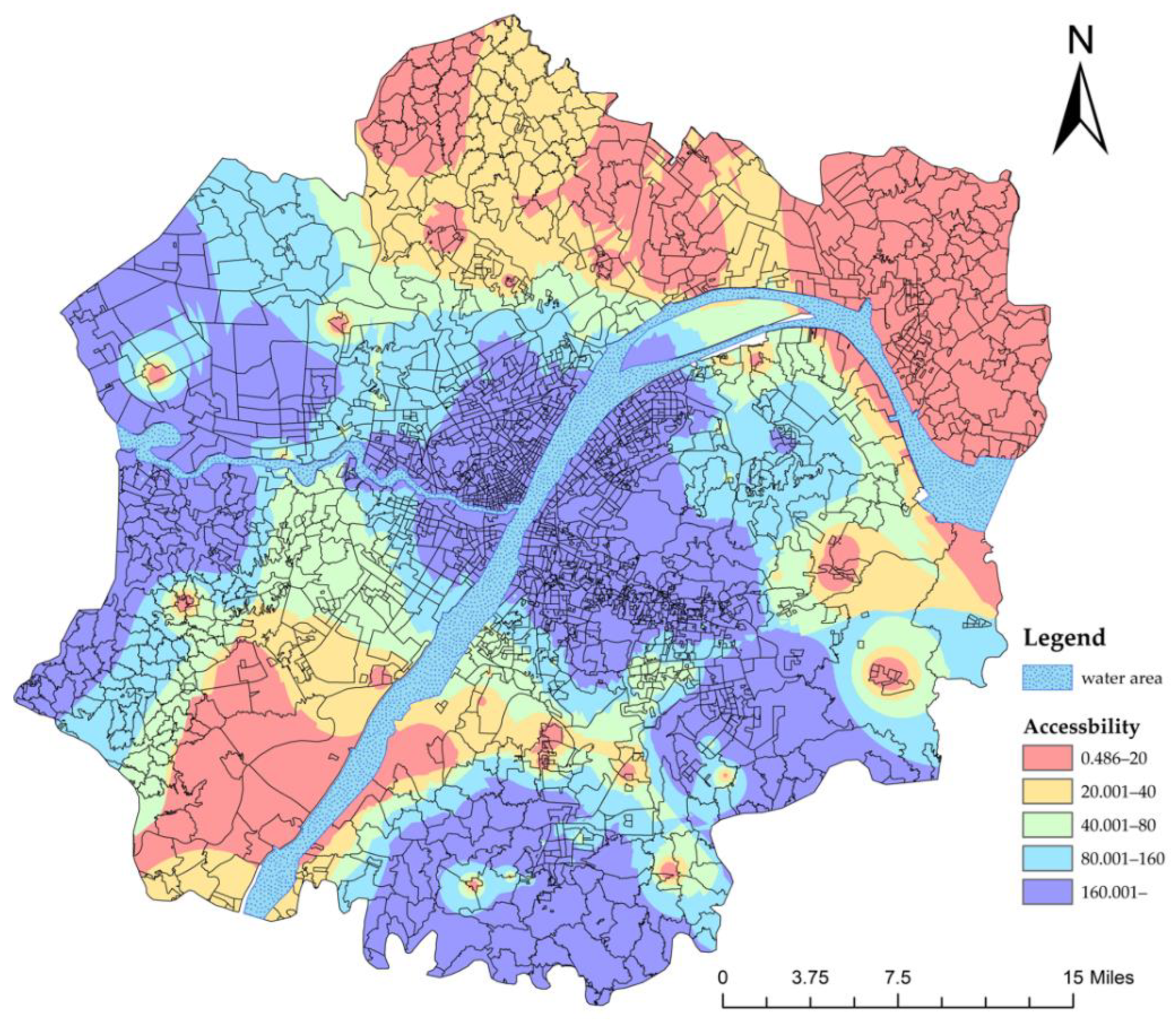
4.1.2. Accessibility of Primary Hospitals
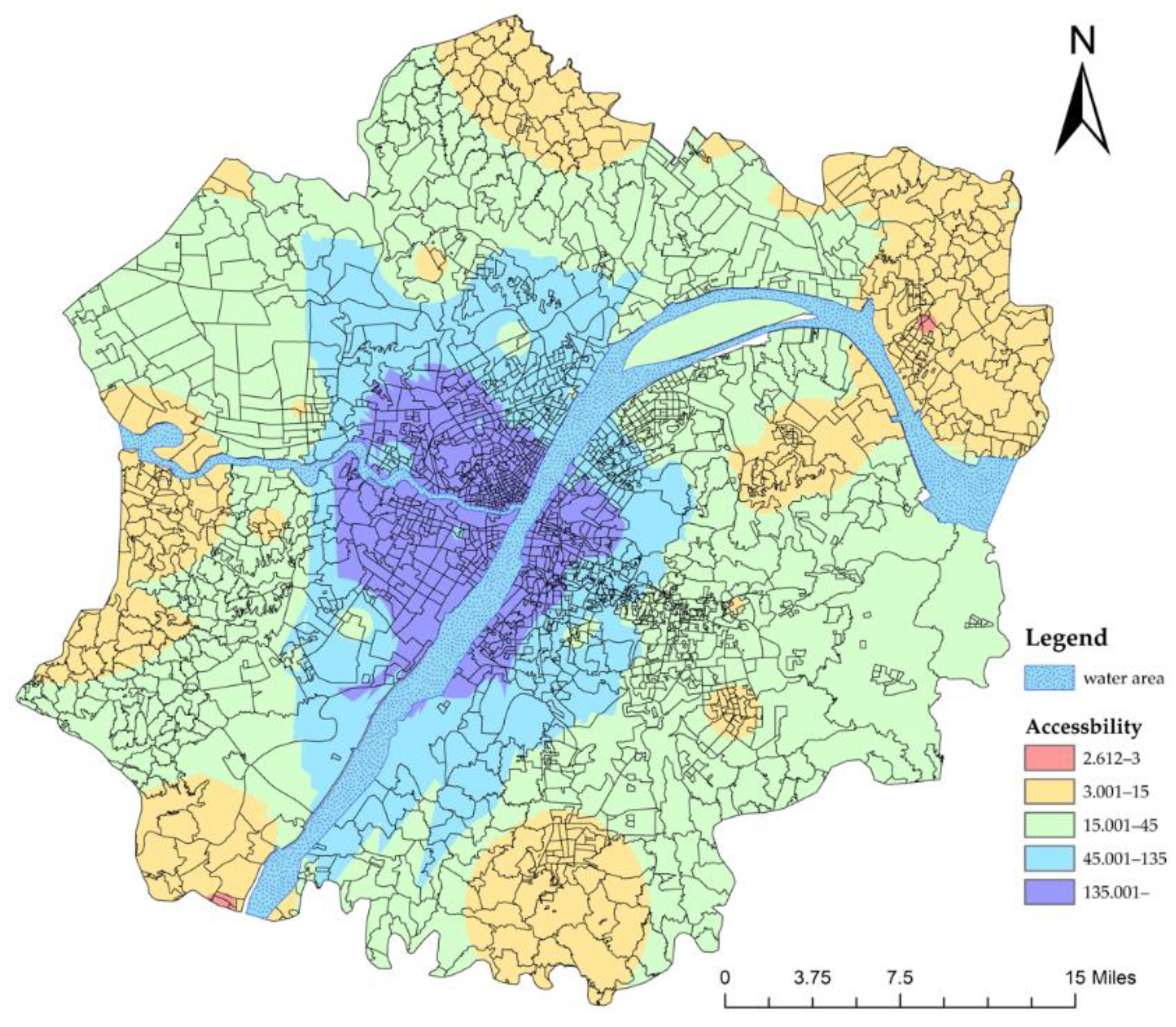
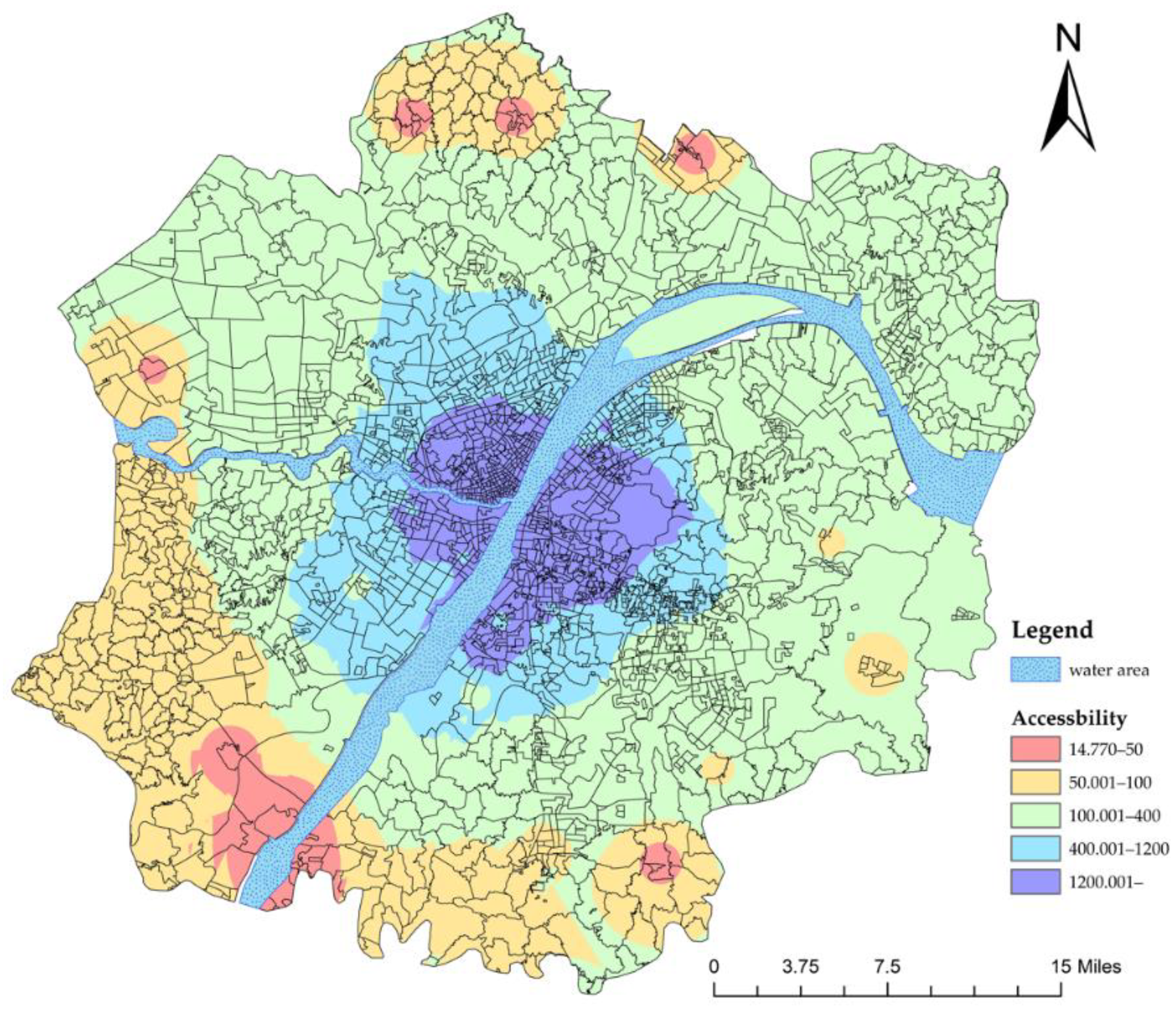
4.2. Health Services Accessibility after the Referral Reform
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ta, Y.; Zhu, Y.; Fu, H. Trends in access to health services, financial protection and satisfaction between 2010 and 2016: Has China achieved the goals of its health system reform? Soc. Sci. Med. 2020, 245, 112715. [Google Scholar] [CrossRef] [PubMed]
- Yuan, B.; Jian, W.; Martinez-Alvarez, M.; McKee, M.; Balabanova, D. Health system reforms in China a half century apart: Continuity but adaptation. Soc. Sci. Med. 2020, 265, 113421. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Rao, K.; Wu, S.; Liu, Q. Health Care in China: Improvement, Challenges, and Reform. Chest 2013, 143, 524–531. [Google Scholar] [CrossRef] [PubMed]
- Liu, G.G.; Vortherma, S.A.; Hong, X. China’s health reform update. Annu. Rev. Public Health 2017, 38, 431–448. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atella, V.; Brugiavini, A.; Pace, N. The health care system reform in China: Effects on out-of-pocket expenses and saving. China Econ. Rev. 2015, 34, 182–195. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Li, Z.; Shi, J.; Chang, A. Hospital referral and capacity strategies in the two-tier healthcare systems. Omega 2021, 100, 102229. [Google Scholar] [CrossRef]
- Xiao, Y.; Chen, X.; Li, Q.; Jia, P.; Li, L.; Chen, Z. Towards healthy China 2030: Modeling health care accessibility with patient referral. Soc. Sci. Med. 2021, 276, 113834. [Google Scholar] [CrossRef]
- Wu, Y.; Yan, X.; Zhao, S.; Wang, J.; Ran, J.; Dong, D.; Wang, M.; Fung, H.; Yeoh, E.; Chung, B.Y. Association of time to diagnosis with socioeconomic position and geographical accessibility to healthcare among symptomatic COVID-19 patients: A retrospective study in Hong Kong. Health Place 2020, 66, 102465. [Google Scholar] [CrossRef]
- Ghorbanzadeh, M.; Kim, K.; Ozguven, E.E.; Horner, M.W. Spatial accessibility assessment of COVID-19 patients to healthcare facilities: A case study of Florida. Travel Behav. Soc. 2021, 24, 95–101. [Google Scholar] [CrossRef]
- Li, H.; Yu, W. Enhancing community system in China’s recent health reform: An effort to improve equity in essential health care. Health Policy 2011, 99, 167–173. [Google Scholar] [CrossRef]
- Hu, H.; Liang, H.; Wang, H. Longitudinal study of the earliest pilot of tiered healthcare system reforms in China: Will the new type of chronic disease management be effective? Soc. Sci. Med. 2021, 285, 114284. [Google Scholar] [CrossRef] [PubMed]
- Su, S.; Li, Z.; Xu, M.; Cai, Z.; Weng, M. A geo-big data approach to intra-urban food deserts: Transit-varying accessibility, social inequalities, and implications for urban planning. Habitat Int. 2017, 64, 22–40. [Google Scholar] [CrossRef]
- Xu, W.; Yang, L. Evaluating the urban land use plan with transit accessibility. Sustain. Cities Soc. 2019, 45, 474–485. [Google Scholar] [CrossRef]
- Penchansky, R.; Thomas, J.W. The concept of access: Definition and relationship to consumer satisfaction. Med. Care 1981, 19, 127–140. [Google Scholar] [CrossRef] [PubMed]
- Chen, B.Y.; Chen, X.P.; Kwan, M.P.; Schwanen, T. Evaluating spatial accessibility to healthcare services under travel time uncertainty: A reliability-based floating catchment area approach. J. Transp. Geogr. 2020, 87, 102794. [Google Scholar] [CrossRef]
- Pharr, J.R.; James, T.; Yeung, Y.L. Accessibility and accommodations for patients with mobility disabilities in a large healthcare system: How are we doing? Disabil. Health J. 2019, 12, 679–684. [Google Scholar] [CrossRef]
- Gao, P.; Lee, C.; Murphy, D. Good for your fiscal health? The effect of the affordable care act on healthcare borrowing costs. J. Financ. Econ. 2022, 145, 464–488. [Google Scholar] [CrossRef]
- Vlugt, A.; Curl, A.; Scheiner, J. The influence of travel attitudes on perceived walking accessibility and walking behaviour. Travel Behav. Soc. 2022, 27, 47–56. [Google Scholar] [CrossRef]
- Wang, F.H. Measurement, optimization, and impact of health care accessibility: A methodological review. Ann. Assoc. Am. Geogr. 2012, 102, 1104–1112. [Google Scholar] [CrossRef] [Green Version]
- Kilinc, M.S.; Milburn, A.B.; Stamm, J.L.H. Measuring potential spatial accessibility of home healthcare services. Soc. Econ. Plan. Sci. 2017, 59, 13–25. [Google Scholar] [CrossRef]
- Neutens, T. Accessibility, equity and health care: Review and research directions for transport geographers. J. Transp. Geogr. 2015, 43, 14–27. [Google Scholar] [CrossRef]
- Núñez, F.; Albornoz, E.; León, J.; Zumelzu, A. Socially sustainable mobility: Strategic analysis to identify accessibility barriers. Sustain. Cities Soc. 2022, 76, 103420. [Google Scholar] [CrossRef]
- Zhan, D.S.; Zhang, W.Z.; Chen, L.; Yu, X.F.; Dang, X.Y. Research progress and its enlightenment of urban public service facilities allocation. Prog. Geogr. 2019, 38, 506–519. [Google Scholar]
- Neutens, T.; Delafontaine, M.; Scott, D.M.; Maeyer, P.D.A. GIS based method to identify spatiotemporal gaps in public service delivery. Appl. Geogr. 2012, 32, 253–264. [Google Scholar] [CrossRef] [Green Version]
- Dejen, A.; Soni, S.; Semaw, F. Spatial accessibility analysis of healthcare service centers in Gamo Gofa Zone, Ethiopia through Geospatial technique. Remote Sens. Appl. Soc. Environ. 2019, 13, 466–473. [Google Scholar] [CrossRef]
- Cho, H.; Choi, J.; No, W.; Oh, M.; Kim, Y. Accessibility of welfare facilities for elderly people in Daejeon, South Korea considering public transportation accessibility. Transp. Res. Interdiscip. Perspect. 2021, 12, 100514. [Google Scholar] [CrossRef]
- Chen, G.; Wang, C.C.; Jin, P.; Xia, B.; Xiao, L.; Chen, S.; Luo, J. Evaluation of healthcare inequity for older adults: A spatio-temporal perspective. J. Transp. Health 2020, 19, 100911. [Google Scholar] [CrossRef]
- Sabokbar, H.F.; Mohammadi, H.; Tahmasbi, S.; Raffi, Y.; Hosseini, A. Measuring spatial accessibility and equity to healthcare services using fuzzy inference system. Appl. Geogr. 2021, 136, 102584. [Google Scholar] [CrossRef]
- Zhao, P.; Li, S.; Liu, D. Unequable spatial accessibility to hospitals in developing megacities: New evidence from Beijing. Health Place 2020, 65, 102406. [Google Scholar] [CrossRef]
- Pot, F.J.; Wee, B.; Tillema, T. Perceived accessibility: What it is and why it differs from calculated accessibility measures based on spatial data. J. Transp. Geogr. 2021, 94, 103090. [Google Scholar] [CrossRef]
- Kotavaara, O.; Nivala, A.; Lankila, T.; Houtari, T.; Delmelle, E.; Antikainen, H. Geographical accessibility to primary health care in Finland-Grid-based multimodal assessment. Appl. Geogr. 2021, 136, 102583. [Google Scholar] [CrossRef]
- Boisjoly, G.; Deboosere, R.; Wasfi, R.; Orpana, H.; Manaugh, K.; Buliung, R.; El-Geneidy, A. Measuring accessibility to hospitals by public transport: An assessment of eight Canadian metropolitan regions. J. Transp. Health 2020, 18, 100916. [Google Scholar] [CrossRef]
- Jin, C.; Cheng, J.; Lu, Y.; Huang, Z.; Cao, F. Spatial inequity in access to healthcare facilities at a county level in a developing country: A case study of Deqing County, Zhejiang, China. Int. J. Equity Health 2015, 14, 67. [Google Scholar] [CrossRef] [Green Version]
- Hu, R.; Dong, S.; Zhao, Y.; Hu, H.; Li, Z. Assessing potential spatial accessibility of health services in rural China: A case study of Donghai County. Int. J. Equity Health 2013, 12, 35. [Google Scholar] [CrossRef] [Green Version]
- Mishra, P.S.; Paotunthang, N.; Marbaniang, S.P. Geographical divide led inequality in accessing maternal healthcare services between hills and valley regions of Manipur state, India. Clin. Epidemiol. Global Health 2021, 11, 100744. [Google Scholar] [CrossRef]
- Qin, C.; Liu, M.; Guo, X.; Liu, J. Human Resources in Primary Health-Care Institutions before and after the New Health-Care Reform in China from 2003 to 2019: An Interrupted Time Series Analysis, in International Journal of Environmental Research and Public Health. Int. J. Environ. Res. Public Health 2022, 19, 6042. [Google Scholar] [CrossRef]
- Ma, C.; Wang, W.; Yuan, Y.; Sun, Y.; Xu, F. Perceptions of hierarchical medical system and associated factors in key primary care practitioners. Chin. Gen. Pract. 2022, 25, 822–828. [Google Scholar]
- Yip, W.; Fu, H.; Chen, A.T.; Zhai, T.; Jian, W.; Xu, R.; Pan, J.; Hu, M.; Zhou, Z.; Chen, Q.; et al. 10 years of health-care reform in China: Progress and gaps in Universal Health Coverage. Lancet. 2019, 394, 1192–1204. [Google Scholar] [CrossRef]
- Ma, X.; Ren, F.; Du, Q.; Liu, P.; Li, L.; Xi, Y.; Jia, P. Incorporating multiple travel modes into a floating catchment area framework to analyse patterns of accessibility to hierarchical healthcare facilities. J. Transp. Health 2019, 15, 100675. [Google Scholar] [CrossRef]
- Li, X.; Lu, J.; Hu, S.; Cheng, K.K.; Maeseneer, J.D.; Meng, Q.; Mossialos, E.; Xu, D.R.; Yip, W.; Zhang, H.; et al. The primary health-care system in China. Lancet. 2017, 390, 2584–2594. [Google Scholar] [CrossRef]
- Tang, C.; Dong, X.; Lian, Y.; Tang, D. Do Chinese hospital services constitute an oligopoly? Evidence of the rich-club phenomenon in a patient referral network. Future Gener. Comput. Syst. 2020, 105, 492–501. [Google Scholar]
- Lu, C.; Zhang, Z.; Lan, X. Impact of China’s referral reform on the equity and spatial accessibility of healthcare resources: A case study of Beijing. Soc. Sci. Med. 2019, 235, 112386. [Google Scholar] [CrossRef]
- Li, M.; Zhang, Y.; Lu, Y.; Yu, W.; Nong, X.; Zhang, L. Factors influencing two-way referral between hospitals and the community in China: A system dynamics simulation model. Simulation 2018, 94, 765–782. [Google Scholar] [CrossRef] [Green Version]
- Li, Q.; Chen, F.; Yang, M.; Lu, L.; Pan, J.; Li, X.; Meng, Q. The effect of China’s national essential medicine policy on health expenses: Evidence from a national study. INQUIRY J. Health Care Org. Provis. Financ. 2018, 55, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Siegel, M.; Koller, D.; Vogt, V.; Sundmacher, L. Developing a composite index of spatial accessibility across different health care sectors: A German example. Health Policy 2016, 120, 205–212. [Google Scholar] [CrossRef]
- Arif, I. Educational attainment, corruption, and migration: An empirical analysis from a gravity model. Econ. Model. 2022, 110, 105802. [Google Scholar] [CrossRef]
- Wang, F.; Luo, W. Assessing spatial and nonspatial factors for healthcare access: Towards an integrated approach to defining health professional shortage areas. Health Place 2005, 11, 131–146. [Google Scholar] [CrossRef]
- Peeters, D.; Thomas, I. Distance Predicting functions and applied location-allocation models. Geogr. Syst. 2000, 2, 167–184. [Google Scholar] [CrossRef]
- Cheng, M.; Lian, Y.J. Spatial accessibility of urban medical facilities based on improved potential model: A case study of Yangpu District in Shanghai. Prog. Geogr. 2018, 37, 266–275. [Google Scholar]
- Tang, P.F.; Xiang, J.J.; Luo, J.; Chen, G.L. Spatial accessibility analysis of primary schools at the county level based on the improved potential model: A case study of Xiantao City, Hubei Province. Prog. Geogr. 2017, 36, 697–708. [Google Scholar]
- Zhang, Y.; Cao, M.; Cheng, L.; Gao, X.; Vos, J.D. Exploring the temporal variations in accessibility to health services for older adults: A case study in Greater London. J. Transp. Health 2022, 24, 101334. [Google Scholar] [CrossRef]
- Mayaud, J.R.; Tran, M.; Nuttall, R. An urban data framework for assessing equity in cities: Comparing accessibility to healthcare facilities in Cascadia. Comput. Environ. Urban Syst. 2019, 78, 101401. [Google Scholar] [CrossRef]
- Sharma, G.; Patil, G.R. Public transit accessibility approach to understand the equity for public healthcare services: A case study of Greater Mumbai. J. Transp. Geogr. 2021, 94, 103123. [Google Scholar] [CrossRef]
- Xing, J.; Ng, S.T. Analyzing spatiotemporal accessibility patterns to tertiary healthcare services by integrating total travel cost into an improved E3SFCA method in Changsha, China. Cities 2022, 122, 103541. [Google Scholar] [CrossRef]
- Cheng, L.; Yan, M.; Vos, J.D.; Witlox, F. Examining geographical accessibility to multi-tier hospital care services for the elderly: A focus on spatial equity. J. Transp. Health 2020, 19, 100926. [Google Scholar] [CrossRef]
- Yan, X.; Shan, L.; He, S.; Zhang, J. Cross-city patient mobility and healthcare equity and efficiency: Evidence from Hefei, China. Travel Behav. Soc. 2022, 28, 1–12. [Google Scholar] [CrossRef]
- Cheng, G.; Zeng, X.; Duan, L.; Lu, X.; Sun, H.; Jiang, T.; Li, Y. Spatial difference analysis for accessibility to high level hospitals based on travel time in Shenzhen, China. Habitat Int. 2016, 53, 485–494. [Google Scholar] [CrossRef] [Green Version]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Accessibility (Standard Value = 6.5) | Number of Communities | Proportion |
|---|---|---|
| Up to the standard | 154 | 7.91% |
| Not up to the standard | 1793 | 92.09% |
| Accessibility (Standard Value = 1) | Number of Communities | Proportion |
|---|---|---|
| Up to the standard | 1833 | 94.6% |
| Not up to the standard | 104 | 5.4% |
| Accessibility (Standard Value = 20) | Number of Communities | Proportion |
|---|---|---|
| Up to the standard | 1803 | 92.6% |
| Not up to the standard | 144 | 7.4% |
| Accessibility (Standard Value = 3) | Number of Communities | Proportion |
|---|---|---|
| Up to the standard | 1945 | 99.9% |
| Not up to the standard | 2 | 0.1% |
| Accessibility (Standard Value = 50) | Number of Communities | Proportion |
|---|---|---|
| Up to the standard | 1926 | 98.3% |
| Not up to the standard | 33 | 1.7% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, Y.; Wu, J. The Effect of the Referral System on the Accessibility of Healthcare Services: A Case Study of the Wuhan Metropolitan Development Zone. Int. J. Environ. Res. Public Health 2022, 19, 10441. https://doi.org/10.3390/ijerph191610441
Chen Y, Wu J. The Effect of the Referral System on the Accessibility of Healthcare Services: A Case Study of the Wuhan Metropolitan Development Zone. International Journal of Environmental Research and Public Health. 2022; 19(16):10441. https://doi.org/10.3390/ijerph191610441
Chicago/Turabian StyleChen, Ying, and Jiale Wu. 2022. "The Effect of the Referral System on the Accessibility of Healthcare Services: A Case Study of the Wuhan Metropolitan Development Zone" International Journal of Environmental Research and Public Health 19, no. 16: 10441. https://doi.org/10.3390/ijerph191610441
APA StyleChen, Y., & Wu, J. (2022). The Effect of the Referral System on the Accessibility of Healthcare Services: A Case Study of the Wuhan Metropolitan Development Zone. International Journal of Environmental Research and Public Health, 19(16), 10441. https://doi.org/10.3390/ijerph191610441