
The Role of Family Health in Mediating the Association between Smartphone Use and Health Risk Behaviors among Chinese Adolescent Students: A National Cross-Sectional Study


 ,
,  ,
, 

Abstract
:1. Introduction
Study Purpose and Hypotheses
2. Materials and Methods
2.1. Participants and Procedures
2.2. Measures
2.2.1. The Chinese version of short-form of Family Health Scale (FHS-SF Chinese version)
2.2.2. Adolescent Health Risk Behaviors Scale (AHRBS)
2.2.3. Control Variables
2.3. Data Analyses
Statistical Analyses
3. Results
3.1. Socio-Demographic Information
3.2. Preliminary Analyses
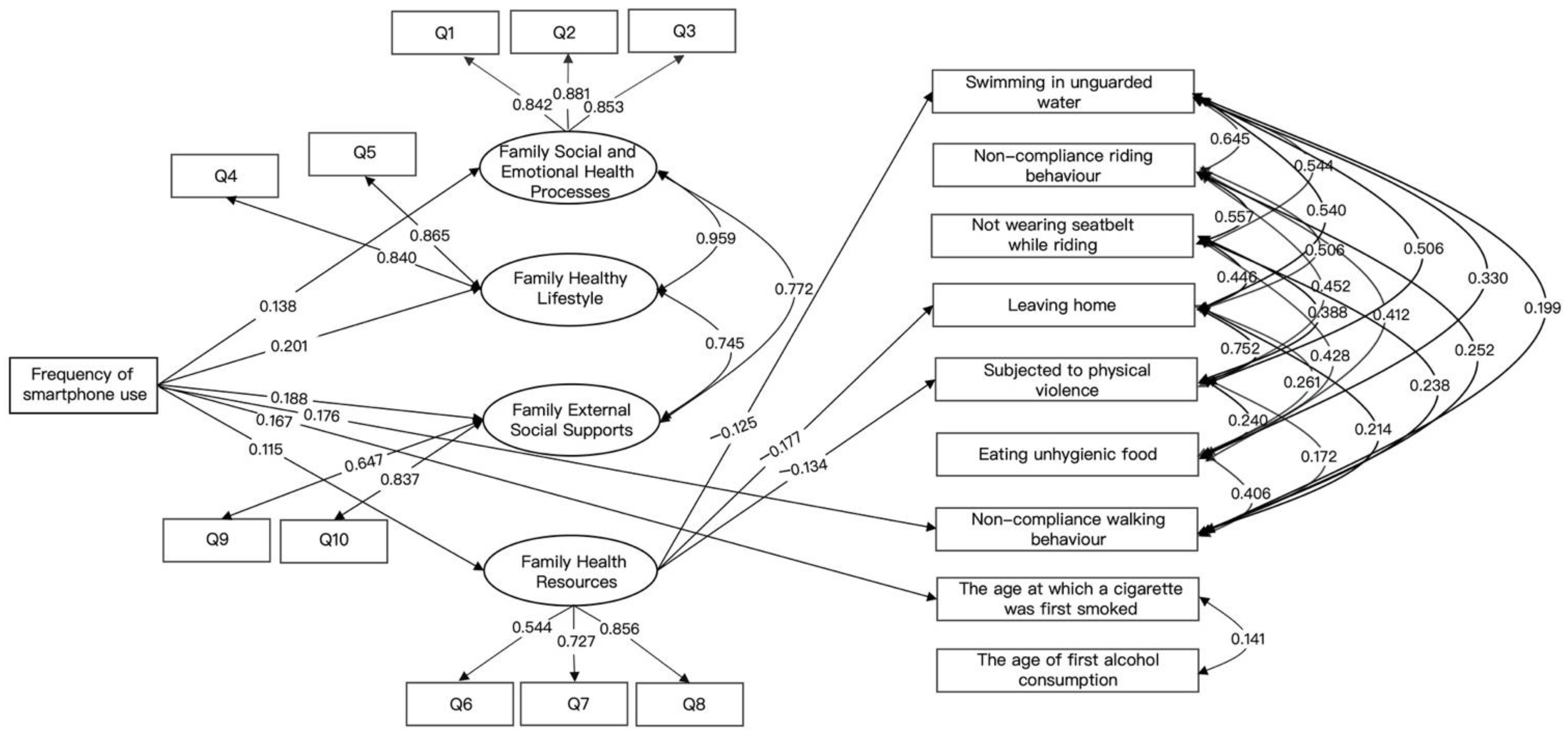
3.3. Indices of Structural Equation Model
3.4. Effect of Exogenous Latent Variables on Endogenous Variables
3.5. Effects among Endogenous Variables
3.6. Testing for the Mediating Effects of Family Health
4. Discussion
4.1. Suggestions
4.2. Limitations and Implications
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- With Recent Survey Data Showing that as of February 2022, the Number of Adolescent Internet Users Reached 13,725,600, with 82.9% of Adolescents Owning Their Own Internet Devices, and Smartphones Being the Highest Proportion of Adolescent Accessing the Internet at 65.0%.China Internet Network Information Center. National Study on Internet Use by Adolescents in 2020. Available online: http://www.cnnic.net.cn/NMediaFile/old_attach/P020210720571098696248.pdf (accessed on 22 May 2022).
- Anderson, M.; Jiang, J. Teens, social media & technology 2018. Pew Res. Cent. 2018, 31, 1673–1689. [Google Scholar]
- Rideout, V.; Robb, M.B. The Common Sense Census: Media Use by Tweens and Teens; Common Sense Media: San Francisco, CA, USA, 2019; Available online: https://www.commonsensemedia.org/research/the-common-sense-census-media-use-by-tweens-and-teens-2019 (accessed on 22 May 2022).
- Tao, F. (Ed.) Child and Adolescent Hygiene, 8th ed.; People’s Health: Beijing, China, 2017; pp. 144–146. [Google Scholar]
- Centers for Disease Control and Prevention. Youth Risk Behavior Surveillance System (YRBSS). Available online: https://www.cdc.gov/healthyyouth/data/yrbs/overview.htm (accessed on 10 March 2022).
- Sherman, L.E.; Greenfield, P.M.; Hernandez, L.M.; Dapretto, M. Peer influence via instagram: Effects on brain and behavior in adolescence and young adulthood. Child Dev. 2018, 89, 37–47. [Google Scholar] [CrossRef]
- Moreno, M.A.; Whitehill, J.M. Influence of social media on alcohol use in adolescents and young adults. Alcohol Res. Curr. Rev. 2014, 36, 91. [Google Scholar]
- Steele, J.R.; Brown, J.D. Adolescent room culture: Studying media in the context of everyday life. J. Youth Adolesc. 1995, 24, 551–576. [Google Scholar] [CrossRef]
- Sherman, L.E.; Payton, A.A.; Hernandez, L.M.; Greenfield, P.M.; Dapretto, M. The power of the like in adolescence: Effects of peer influence on neural and behavioral responses to social media. Psychol. Sci. 2016, 27, 1027–1035. [Google Scholar] [CrossRef]
- Eleuteri, S.; Saladino, V.; Verrastro, V. Identity, relationships, sexuality, and risky behaviors of adolescents in the context of social media. Sex. Relatsh. Ther. 2017, 32, 354–365. [Google Scholar] [CrossRef]
- Reid, D.; Weigle, P. Social media use among adolescents: Benefits and risks. Adolesc. Psychiatry 2014, 4, 73–80. [Google Scholar] [CrossRef]
- Marchant, A.; Hawton, K.; Stewart, A.; Montgomery, P.; Singaravelu, V.; Lloyd, K.; Purdy, N.; Daine, K.; John, A. A systematic review of the relationship between internet use, self-harm and suicidal behavior in young people: The good, the bad and the unknown. PLoS ONE 2017, 12, e0181722. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seabrook, E.M.; Kern, M.L.; Rickard, N.S. Social networking sites, depression, and anxiety: A systematic review. JMIR Ment. Health 2016, 3, e5842. [Google Scholar] [CrossRef] [Green Version]
- Spies Shapiro, L.A.; Margolin, G. Growing up wired: Social networking sites and adolescent psychosocial development. Clin. Child Fam. Psychol. Rev. 2014, 17, 1–18. [Google Scholar] [CrossRef] [Green Version]
- Subrahmanyam, K.; Greenfield, P. Online communication and adolescent relationships. Future Child. 2008, 18, 119–146. [Google Scholar] [CrossRef]
- Underwood, M.K.; Ehrenreich, S.E. The power and the pain of adolescents’ digital communication: Cyber victimization and the perils of lurking. Am. Psychol. 2017, 72, 144. [Google Scholar] [CrossRef]
- Valkenburg, P.M.; Peter, J. Online communication among adolescents: An integrated model of its attraction, opportunities, and risks. J. Adolesc. Health 2011, 48, 121–127. [Google Scholar] [CrossRef] [PubMed]
- Vannucci, A.; McCauley Ohannessian, C. Social media use subgroups differentially predict psychosocial well-being during early adolescence. J. Youth Adolesc. 2019, 48, 1469–1493. [Google Scholar] [CrossRef] [Green Version]
- Moreno, M.A.; D’Angelo, J.; Whitehill, J. Social media and alcohol: Summary of research, intervention ideas and future study. directions. Media Commun. 2016, 4, 50–59. [Google Scholar] [CrossRef] [Green Version]
- Moreno, M.A.; Christakis, D.A.; Egan, K.G.; Jelenchick, L.A.; Cox, E.; Young, H.; Villiard, H.; Becker, T. A pilot evaluation of associations between displayed depression references on Facebook and self-reported depression using a clinical scale. J. Behav. Health Serv. Res. 2012, 39, 295–304. [Google Scholar] [CrossRef] [Green Version]
- Guntuku, S.C.; Yaden, D.B.; Kern, M.L.; Ungar, L.H.; Eichstaedt, J.C. Detecting depression and mental illness on social media: An integrative review. Curr. Opin. Behav. Sci. 2017, 18, 43–49. [Google Scholar] [CrossRef]
- Yonker, L.M.; Zan, S.; Scirica, C.V.; Jethwani, K.; Kinane, T.B. “Friending” teens: Systematic review of social media in adolescent and young adult health care. J. Med. Internet Res. 2015, 17, e3692. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Touitou, Y.; Touitou, D.; Reinberg, A. Disruption of adolescents’ circadian clock: The vicious circle of media use, exposure to light at night, sleep loss and risk behaviors. J. Physiol. -Paris 2016, 110, 467–479. [Google Scholar] [CrossRef] [PubMed]
- Kenney, E.L.; Gortmaker, S.L. United States adolescents’ television, computer, videogame, smartphone, and tablet use: Associations with sugary drinks, sleep, physical activity, and obesity. J. Pediatrics 2017, 182, 144–149. [Google Scholar] [CrossRef] [Green Version]
- Kim, E.; Kim, H.R. Associations between and Smartphone Use and Sugar-sweetened Beverage Intake among Korea Adoles. cents: The 13th Korea Youth Risk Behavior Survey. J. Korea Acad. Ind. Coop. Soc. 2020, 21, 578–587. [Google Scholar]
- Williams, A.L.; Merten, M.J. iFamily: Internet and social media technology in the family context. Fam. Consum. Sci. Res. J. 2011, 40, 150–170. [Google Scholar] [CrossRef]
- Turkle, S. Reclaiming Conversation: The Power of Talk in a Digital Age; Penguin: London, UK, 2016. [Google Scholar]
- Media, C.S. Dealing with Devices: The Parent-Teen Dynamic; Common Sense Media: San Francisco, CA, USA, 2016. [Google Scholar]
- Steinberg, L. A dual systems model of adolescent risk-taking. Dev. Psychobiol. J. Int. Soc. Dev. Psychobiol. 2010, 52, 216–224. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Maternal, Newborn, Child and Adolescent Health and Ageing. Available online: https://platform.who.int/data/maternal-newborn-child-adolescent-ageing/adolescent-data/adolescent---risk-factors (accessed on 10 March 2022).
- World Health Organization. Violent Discipline. Available online: https://data.unicef.org/topic/child-protection/violence/violent-discipline/ (accessed on 10 March 2022).
- Scaglioni, S.; De Cosmi, V.; Ciappolino, V.; Parazzini, F.; Brambilla, P.; Agostoni, C. Factors influencing children’s eating behaviours. Nutrients 2018, 10, 706. [Google Scholar] [CrossRef] [Green Version]
- Anyanwu, F.C.; Akinsola, H.A.; Tugli, A.K.; Obisie-Nmehielle, N. A qualitative assessment of the influence of family dynamics on adolescents’ sexual risk behaviour in a migration-affected community. Int. J. Qual. Stud. Health Well Being 2020, 15, 1717322. [Google Scholar] [CrossRef] [Green Version]
- Schneider, L.A.; King, D.L.; Delfabbro, P.H. Family factors in adolescent problematic Internet gaming: A systematic review. J. Behav. Addict. 2017, 6, 321–333. [Google Scholar] [CrossRef] [Green Version]
- Ali, M.M.; Dean, D., Jr. The influence of nonresident fathers on adolescent and young adult cigarette smoking. Fam. Syst. Health 2015, 33, 314. [Google Scholar] [CrossRef]
- Thomas, R.E.; Baker, P.R.; Thomas, B.C.; Lorenzetti, D.L. Family-based programmes for preventing smoking by children and adolescents. Cochrane Database Syst. Rev. 2015, 2, 1465–1858. [Google Scholar] [CrossRef] [Green Version]
- Liu, K.S.; Chen, J.Y.; Ng, M.Y.; Yeung, M.H.; Bedford, L.E.; Lam, C.L. How does the family influence adolescent eating habits in terms of knowledge, attitudes and practices? A global systematic review of qualitative studies. Nutrients 2021, 13, 3717. [Google Scholar] [CrossRef]
- Council on Communications and Media; Strasburger, V.C.; Hogan, M.J.; Mulligan, D.A.; Ameenuddin, N.; Christakis, D.A.; Cross, C.; Fagbuyi, D.B.; Hill, D.L.; Levine, A.E. Children, adolescents, and the media. Pediatrics 2013, 132, 958–961. [Google Scholar] [CrossRef] [Green Version]
- Shah, J.; Das, P.; Muthiah, N.; Milanaik, R. New age technology and social media: Adolescent psychosocial implications and. the need for protective measures. Curr. Opin. Pediatrics 2019, 31, 148–156. [Google Scholar] [CrossRef] [PubMed]
- Hill, D.; Ameenuddin, N.; Chassiakos, Y.L.R.; Cross, C.; Radesky, J.; Hutchinson, J.; Levine, A.; Boyd, R.; Mendelson, R.; Moreno, M. Media use in school-aged children and adolescents. Pediatrics 2016, 138, 5. [Google Scholar] [CrossRef] [Green Version]
- Office of the Seventh National Population Census Leading Group of the State Council. National Bureau of Statistics Office. The Seventh National Census Bulletin (No. 2)—National Populat. Available online: http://www.stats.gov.cn/tjsj./zxfb/202105/t202105101817178.html (accessed on 10 July 2022).
- Wang, F.; Wu, Y.; Sun, X.; Wang, D.; Ming, W.-K.; Sun, X.; Wu, Y. Reliability and validity of the Chinese version of a short form of the family health scale. BMC Prim. Care 2022, 23, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Bradley, B.J.; Greene, A.C. Do health and education agencies in the United States share responsibility for academic achieve ment and health? A review of 25 years of evidence about the relationship of adolescents’ academic achievement and health behaviors. J. Adolesc. Health 2013, 52, 523–532. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wright, C.; Kipping, R.; Hickman, M.; Campbell, R.; Heron, J. Effect of multiple risk behaviours in adolescence on educa. tional attainment at age 16 years: A UK birth cohort study. BMJ Open 2018, 8, e020182. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.H.-s.; Chun, J. Examining the effects of parental influence on adolescent smoking behaviors: A multilevel analysis of the Global School-Based Student Health Survey (2003–2011). Nicotine Tob. Res. 2016, 18, 934–942. [Google Scholar] [CrossRef] [PubMed]
- Shi, X.; Chen, T.; Ma, J. Analysis of family influencing factors of dietary behavior pattern of children and adolescents. Chin. J. Epidemiol. 2020, 41, 1291–1295. [Google Scholar] [CrossRef]
- Durkee, T.; Carli, V.; Floderus, B.; Wasserman, C.; Sarchiapone, M.; Apter, A.; Balazs, J.A.; Bobes, J.; Brunner, R.; Corcoran, P. Pathological internet use and risk-behaviors among European adolescents. Int. J. Environ. Res. Public Health 2016, 13, 294. [Google Scholar] [CrossRef] [Green Version]
- Jiang, Q.; Huang, X.; Tao, R. Examining factors influencing internet addiction and adolescent risk behaviors among excessive. Internet users. Health Commun. 2018, 33, 1434–1444. [Google Scholar] [CrossRef]
- Hair, J.F. Multivariate Data Analysis; Kennesaw State University: Kennesaw, GA, USA, 2009. [Google Scholar]
- Podsakoff, P.M.; Organ, D.W. Self-reports in organizational research: Problems and prospects. J. Manag. 1986, 12, 531–544. [Google Scholar] [CrossRef]
- Pourhoseingholi, M.A.; Baghestani, A.R.; Vahedi, M. How to control confounding effects by statistical analysis. Gas troenterol. Hepatol. Bed Bench 2012, 5, 79. [Google Scholar]
- Hu, L.T.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alterna tives. Struct. Equ. Modeling A Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Hayes, A.F. Beyond Baron and Kenny: Statistical mediation analysis in the new millennium. Commun. Monogr. 2009, 76, 408–420. [Google Scholar] [CrossRef]
- Zhao, X.; Lynch, J.G., Jr.; Chen, Q. Reconsidering Baron and Kenny: Myths and truths about mediation analysis. J. Consum. Res. 2010, 37, 197–206. [Google Scholar] [CrossRef]
- Mesch, G.S. The family and the Internet: The Israeli case. Soc. Sci. Q. 2003, 84, 1038–1050. [Google Scholar] [CrossRef]
- Mesch, G.S. Family relations and the Internet: Exploring a family boundaries approach. J. Fam. Commun. 2006, 6, 119–138. [Google Scholar] [CrossRef]
- Yang, Y.-S.; Yen, J.-Y.; Ko, C.-H.; Cheng, C.-P.; Yen, C.-F. The association between problematic cellular phone use and risky behaviors and low self-esteem among Taiwanese adolescents. BMC Public Health 2010, 10, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.-G.; Park, J.; Kim, H.-T.; Pan, Z.; Lee, Y.; McIntyre, R.S. The relationship between smartphone addiction and symptoms of depression, anxiety, and attention-deficit/hyperactivity in South Korean adolescents. Ann. Gen. Psychiatry 2019, 18, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Chang, F.-C.; Miao, N.-F.; Lee, C.-M.; Chen, P.-H.; Chiu, C.-H.; Lee, S.-C. The association of media exposure and media liter acy with adolescent alcohol and tobacco use. J. Health Psychol. 2016, 21, 513–525. [Google Scholar] [CrossRef]
- Walsh, F. Strengthening Family Resilience; Guilford Publications: New York, NY, USA, 2015. [Google Scholar]
- Acuña, M.A.; Kataoka, S. Family communication styles and resilience among adolescents. Soc. Work. 2017, 62, 261–269. [Google Scholar] [CrossRef]
- Chew, J.; Carpenter, J.; Haase, A.M. Young people’s experiences of living with epilepsy: The significance of family resilience. Soc. Work. Health Care 2018, 57, 332–354. [Google Scholar] [CrossRef] [Green Version]
- Hoffmann, J.P.; Warnick, E. Do family dinners reduce the risk for early adolescent substance use? A propensity score analysis. J. Health Soc. Behav. 2013, 54, 335–352. [Google Scholar] [CrossRef] [PubMed]
- Lam, C.B.; McHale, S.M. Developmental patterns and parental correlates of youth leisure-time physical activity. J. Fam. Psychol. 2015, 29, 100–107. [Google Scholar] [CrossRef] [PubMed]
- Reiss, F.; Meyrose, A.-K.; Otto, C.; Lampert, T.; Klasen, F.; Ravens-Sieberer, U. Socioeconomic status, stressful life situations and mental health problems in children and adolescents: Results of the German BELLA cohort-study. PLoS ONE 2019, 14, e0213700. [Google Scholar] [CrossRef] [PubMed]
- Robinson, L.R.; Holbrook, J.R.; Bitsko, R.H.; Hartwig, S.A.; Kaminski, J.W.; Ghandour, R.M.; Peacock, G.; Heggs, A.; Boyle, C.A. Differences in health care, family, and community factors associated with mental, behavioral, and developmental disorders among children aged 2–8 years in rural and urban areas—United States, 2011–2012. MMWR Surveill. Summ. 2017, 66, 1. [Google Scholar] [CrossRef] [Green Version]
- Gaete, J.; Rojas-Barahona, C.A.; Olivares, E.; Chen, M.-Y. The influence of parental healthy behaviors on healthy lifestyles of early adolescents. Rev. Med. De Chile 2016, 144, 870–878. [Google Scholar] [CrossRef] [PubMed]
- Rhodes, R.E.; Guerrero, M.D.; Vanderloo, L.M.; Barbeau, K.; Birken, C.S.; Chaput, J.-P.; Faulkner, G.; Janssen, I.; Madigan, S.; Mâsse, L.C. Development of a consensus statement on the role of the family in the physical activity, sedentary, and sleep behaviours of children and youth. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 1–31. [Google Scholar] [CrossRef] [PubMed]
- China Internet Network Information Center. 2020 National Youth Internet Usage Study Report. Available online: http://www.cnnic.net.cn/n4/2022/0401/c116-1126.html (accessed on 6 August 2022).
- Mourra, G.N.; Senecal, S.; Fredette, M.; Lepore, F.; Faubert, J.; Bellavance, F.; Cameron, A.-F.; Labonté-LeMoyne, E.; Léger, P.-M. Using a smartphone while walking: The cost of smartphone-addiction proneness. Addict. Behav. 2020, 106, 106346. [Google Scholar] [CrossRef]
- del Carmen Pérez-Fuentes, M.; Gázquez-Linares, J.J.; del Mar Molero-Jurado, M.; Martos-Martinez, Á.; Barragán-Martín, A.B.; del Mar Simón-Márquez, M. Student burnout and engagement: Relationship with adolescent use of alcohol and attitudes towards authority. Int. J. Clin. Health Psychol. 2021, 21, 100225. [Google Scholar] [CrossRef]
- Roebroek, L.; Koning, I.M. The reciprocal relation between adolescents’ school engagement and alcohol consumption, and the role of parental support. Prev. Sci. 2016, 17, 218–226. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| M ± SD | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. CSOS | 1.000 | |||||||||||||||||
| 2. FEI | 0.095 * | 1.000 | ||||||||||||||||
| 3. FOPCU | 4.18 ± 1.176 | 0.186 ** | 0.078 * | 1.000 | ||||||||||||||
| 4. FOSU | 2.94 ± 1.405 | 0.180 ** | 0.187 ** | 0.365 ** | 1.000 | |||||||||||||
| 5. FSAEHP | 11.90 ± 2.500 | −0.076 * | 0.119 ** | 0.102 ** | 0.136 ** | 1.000 | ||||||||||||
| 6. FHL | 8.09 ± 1.652 | −0.099 ** | 0.075 * | 0.060 | 0.165 ** | 0.830 ** | 1.000 | |||||||||||
| 7. FHR | 11.15 ± 2.868 | −0.031 | 0.261 ** | 0.017 | 0.085 * | 0.267 ** | 0.271 ** | 1.000 | ||||||||||
| 8. FESS | 7.70 ± 1.664 | −0.042 | 0.068 | 0.159 ** | 0.209 ** | 0.615 ** | 0.590 ** | 0.181 ** | 1.000 | |||||||||
| 9. SIUW | 1.51 ± 0.811 | 0.058 | −0.015 | 0.062 | −0.077 * | −0.068 | −0.072 | −0.125 ** | −0.049 | 1.000 | ||||||||
| 10. NRB | 1.71 ± 0.972 | 0.024 | −0.027 | 0.036 | −0.030 | −0.036 | −0.045 | −0.092 * | −0.045 | 0.649 ** | 1.000 | |||||||
| 11. NWSWR | 1.76 ± 1.031 | 0.032 | 0.009 | 0.053 | −0.013 | −0.078 * | −0.035 | −0.070 | −0.023 | 0.545 ** | 0.547 ** | 1.000 | ||||||
| 12. LH | 2.13 ± 0.557 | 0.022 | −0.009 | 0.022 | −0.126 ** | −0.175 ** | −0.161 ** | −0.192 ** | −0.130 ** | 0.556 ** | 0.509 ** | 0.458 ** | 1.000 | |||||
| 13. STPV | 2.19 ± 0.645 | −0.034 | −0.059 | −0.018 | −0.121 ** | −0.206 ** | −0.179 ** | −0.168 ** | −0.105 ** | 0.514 ** | 0.448 ** | 0.403 ** | 0.764 ** | 1.000 | ||||
| 14. NWB | 2.78 ± 1.747 | 0.210 ** | 0.060 | 0.173 ** | −0.002 | −0.081 * | −0.057 | −0.038 | −0.040 | 0.196 ** | 0.244 ** | 0.251 ** | 0.208 ** | 0.154 ** | 1.000 | |||
| 15. EUF | 2.23 ± 1.299 | 0.040 | −0.080 * | −0.003 | −0.002 | −0.105 ** | −0.070 | −0.034 | −0.051 | 0.331 ** | 0.404 ** | 0.440 ** | 0.271 ** | 0.258 ** | 0.399 ** | 1.000 | ||
| 16. TAAWACWFS | 1.04 ± 0.274 | 0.023 | 0.004 | 0.108 | 0.023 | −0.104 ** | −0.116** | −0.032 | −0.101 ** | 0.041 ** | 0.092 * | 0.080 * | −0.005 | 0.016 | 0.070 | 0.011 | 1.000 | |
| 17. TAOFAC | 1.32 ± 0.752 | 0.228 ** | 0.030 | 0.046 | 0.164** | −0.122 ** | −0.141 ** | −0.035 | −0.070 | −0.002 | 0.051 | 0.049 | 0.027 | 0.015 | 0.193 ** | 0.088 ** | 0.206 ** | 1.000 |
| Using Time of Smartphone per Week | |||||||
|---|---|---|---|---|---|---|---|
| Variables | Item | Total | Never Use | ≤1 Day | 2~3 Days | 4~5 Days | 6~7 Days |
| Number | 693 | 32 | 48 | 92 | 113 | 408 | |
| Percent (%) | 100% | 4.6% | 6.9% | 13.3% | 16.3% | 58.9% | |
| Gender | |||||||
| Male | Number | 315 | 12 | 25 | 54 | 56 | 168 |
| Percent (%) | 45.5% | 3.8% | 7.9% | 17.1% | 17.8% | 53.3% | |
| Female | Number | 378 | 20 | 23 | 38 | 57 | 240 |
| Percent (%) | 54.5% | 5.3% | 6.1% | 10.1% | 15.1% | 63.5% | |
| Location | |||||||
| Rural area | Number | 215 | 12 | 21 | 27 | 44 | 111 |
| Percent (%) | 31.1% | 5.6% | 9.8% | 12.6% | 20.5% | 51.6% | |
| Town | Number | 478 | 20 | 27 | 65 | 69 | 297 |
| Percent (%) | 69.0% | 4.2% | 6.0% | 14.0% | 14.4% | 62.1% | |
| Current stage of schooling | |||||||
| Primary school | Number | 99 | 13 | 12 | 13 | 22 | 39 |
| Percent (%) | 14.3% | 13.1% | 12.1% | 13.1% | 22.2% | 39.4% | |
| Junior high school | Number | 215 | 12 | 14 | 30 | 38 | 121 |
| Percent (%) | 31.0% | 5.6% | 7.0% | 14.0% | 17.7% | 56.3% | |
| Senior middle school | Number | 359 | 6 | 22 | 47 | 53 | 231 |
| Percent (%) | 51.8% | 1.7% | 6.1% | 13.1% | 14.8% | 64.3% | |
| Technical secondary school | Number | 20 | 1 | 0 | 2 | 0 | 17 |
| Percent (%) | 2.9% | 5.0% | 0 | 10% | 0 | 85.0% | |
| Monthly per capita family income | |||||||
| ≤1500 | Number | 86 | 3 | 10 | 15 | 13 | 45 |
| Percent (%) | 12.4% | 3.5% | 11.6% | 17.4% | 15.1% | 52.3% | |
| 1501–6000 | Number | 405 | 14 | 29 | 54 | 70 | 238 |
| Percent (%) | 58.4% | 0.3% | 7.2% | 13.3% | 17.3% | 58.8% | |
| 6001–10,500 | Number | 150 | 14 | 7 | 18 | 21 | 90 |
| Percent (%) | 21.6% | 9.3% | 4.7% | 12% | 14% | 60% | |
| 10,501–15,000 | Number | 26 | 1 | 2 | 0 | 5 | 18 |
| Percent (%) | 3.8% | 3.8% | 7.7% | 0 | 19.2% | 69.2% | |
| ≥15,001 | Number | 26 | 0 | 0 | 5 | 4 | 17 |
| Percent (%) | 3.8% | 0 | 0 | 19.2% | 15.4% | 65.4% | |
| Fitting Indicators | X2 | DF | X2/DF | RMSEA | SRMR | CFI | TLI |
|---|---|---|---|---|---|---|---|
| Standard | ≤3 good fit; ≤5 reasonable fit | ≤0.08 | ≤0.05 good fit; ≤0.07 reasonable fit | ≥0.9 | ≥0.9 | ||
| results | 372.911 | 110 | 3.390 | 0.059 | 0.048 | 0.958 | 0.905 |
| Path | S.C. | S.E. | T.E. | D.E. | I.E. | P.E. | 95% Confidence Intervals | |
|---|---|---|---|---|---|---|---|---|
| Lower Limit | Upper Limit | |||||||
| FOSU—FHR—SIUW | −0.014 | 0.009 | −0.125 ** | - | −0.014 * | 11.2% | −0.042 | −0.002 |
| FOSU—FHR—LH | −0.020 | 0.011 | −0.161 ** | - | −0.020 * | 12.4% | −0.049 | −0.005 |
| FOSU—FHR—STPV | −0.015 | 0.010 | −0.130 * | - | −0.015 * | 11.5% | −0.043 | −0.002 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gong, F.; Lei, Z.; Gong, Z.; Min, H.; Ge, P.; Guo, Y.; Ming, W.-K.; Sun, X.; Wu, Y. The Role of Family Health in Mediating the Association between Smartphone Use and Health Risk Behaviors among Chinese Adolescent Students: A National Cross-Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 13378. https://doi.org/10.3390/ijerph192013378
Gong F, Lei Z, Gong Z, Min H, Ge P, Guo Y, Ming W-K, Sun X, Wu Y. The Role of Family Health in Mediating the Association between Smartphone Use and Health Risk Behaviors among Chinese Adolescent Students: A National Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2022; 19(20):13378. https://doi.org/10.3390/ijerph192013378
Chicago/Turabian StyleGong, Fangmin, Zhaowen Lei, Zhuliu Gong, Hewei Min, Pu Ge, Yi Guo, Wai-Kit Ming, Xinying Sun, and Yibo Wu. 2022. "The Role of Family Health in Mediating the Association between Smartphone Use and Health Risk Behaviors among Chinese Adolescent Students: A National Cross-Sectional Study" International Journal of Environmental Research and Public Health 19, no. 20: 13378. https://doi.org/10.3390/ijerph192013378
APA StyleGong, F., Lei, Z., Gong, Z., Min, H., Ge, P., Guo, Y., Ming, W. -K., Sun, X., & Wu, Y. (2022). The Role of Family Health in Mediating the Association between Smartphone Use and Health Risk Behaviors among Chinese Adolescent Students: A National Cross-Sectional Study. International Journal of Environmental Research and Public Health, 19(20), 13378. https://doi.org/10.3390/ijerph192013378