



Comprehensive Multimorbidity Patterns in Older Patients Are Associated with Quality Indicators of Medication—MoPIM Cohort Study
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Methodology
2.1. Design and Setting
2.2. Data Acquisition and Variables
2.3. Sampling and Analysis
3. Results
3.1. Sociodemographic and Clinical Characteristics of the Cohort
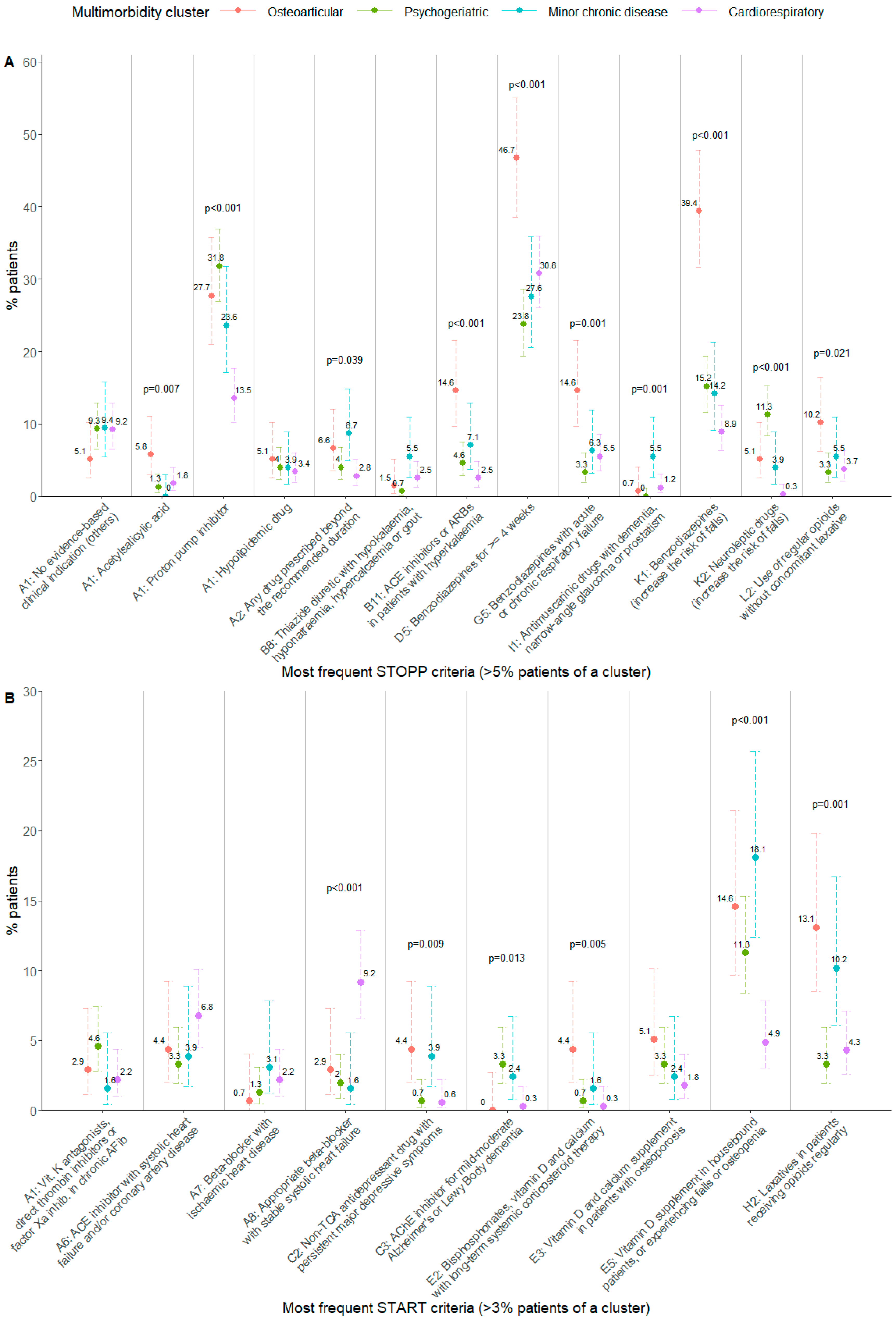
3.2. Relationship between Multimorbidity Clusters and Potentially Inappropriate Prescribing
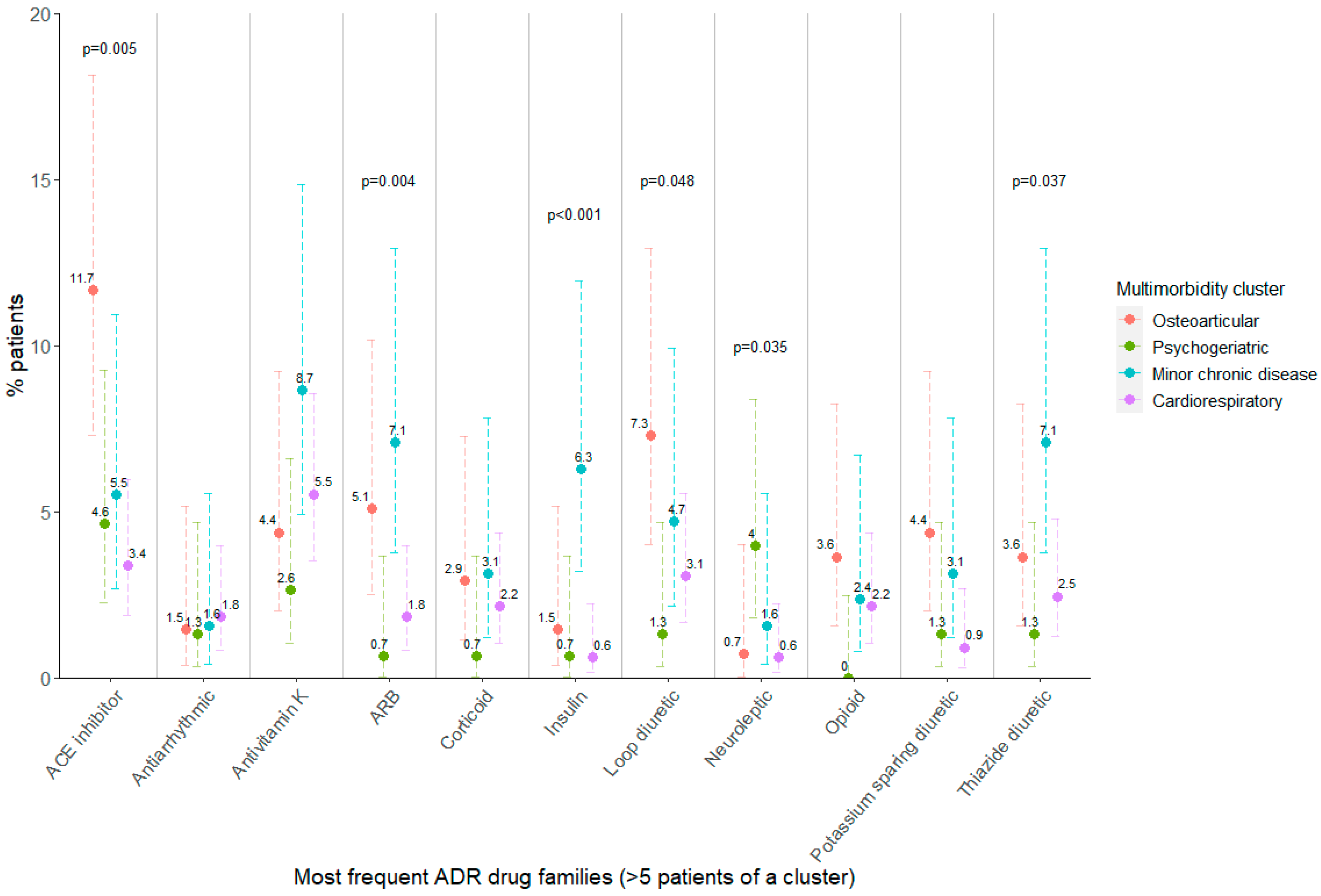
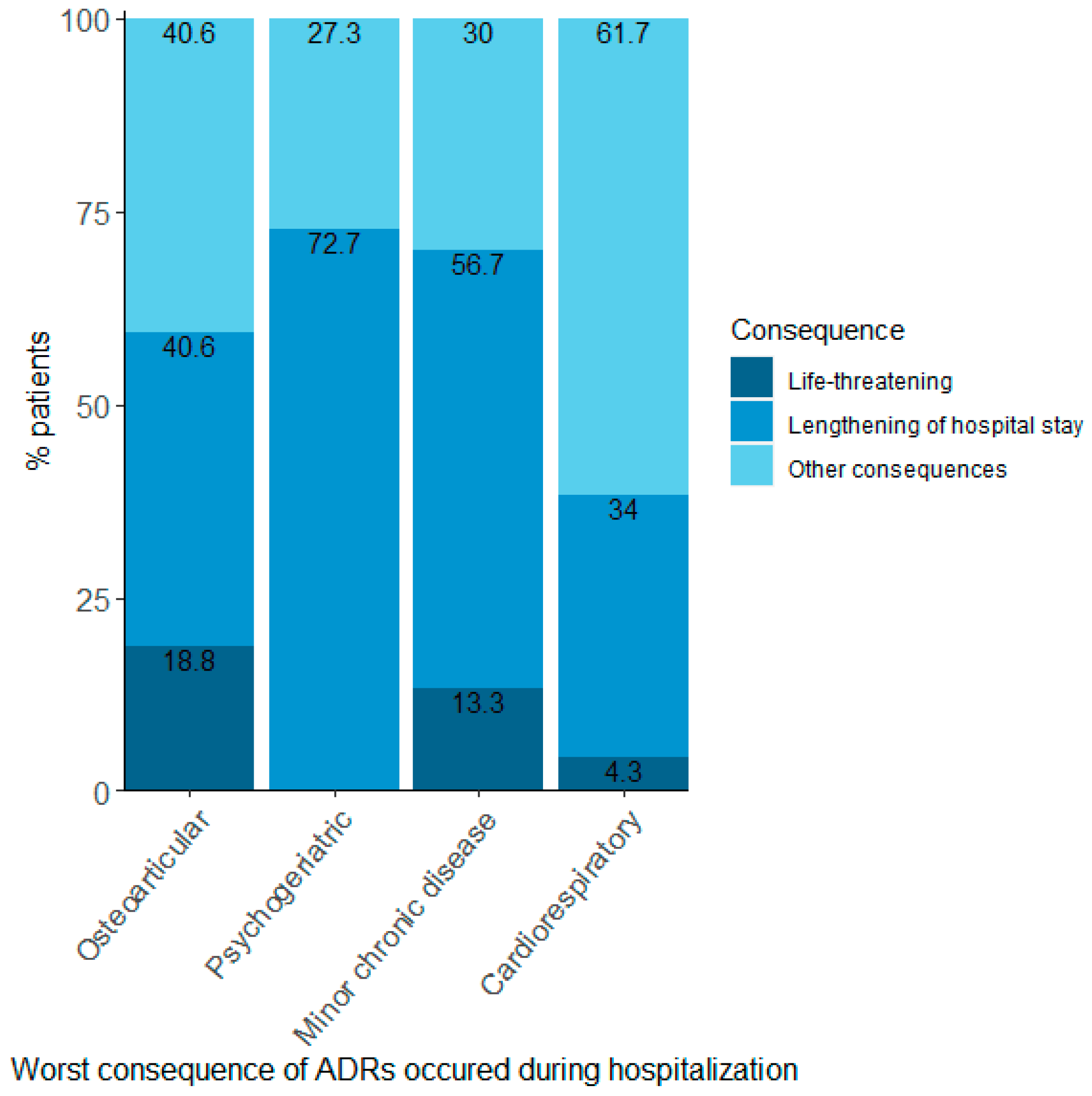
3.3. Relationship between Multimorbidity Clusters and Adverse Drug Reactions
4. Discussion
4.1. Main Important Results and Novelty
4.2. Clinical Implications
4.3. Comparison to Other Studies
4.4. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fortin, M.; Stewart, M.; Poitras, M.-E.; Almirall, J.; Maddocks, H. A Systematic Review of Prevalence Studies on Multimorbidity: Toward a More Uniform Methodology. Ann. Fam. Med. 2012, 10, 142–151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barnett, K.; Mercer, S.W.; Norbury, M.; Watt, G.; Wyke, S.; Guthrie, B. Epidemiology of multimorbidity and implications for health care, research, and medical education: A cross-sectional study. Lancet 2012, 380, 37–43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The Academy of Medical Sciences. Multimorbidity: A Priority For Global Health Research; The Academy of Medical Sciences: London, UK, 2018; Available online: https://acmedsci.ac.uk/file-download/82222577 (accessed on 8 August 2022).
- Rijken, M.; Struckmann, V.; Van Der Heide, I.; Hujala, A.; Barbabella, F.; Van Ginneken, E.; Schellevis, F. How to Improve Care For People with Multimorbidity in Europe? European Observatory on Health Systems and Policies: Brussels, Belgium, 2016; Available online: https://www.euro.who.int/en/about-us/partners/observatory/publications/policy-briefs-and-summaries/how-to-improve-care-for-people-with-multimorbidity-in-europe (accessed on 8 August 2022).
- Johnston, M.C.; Crilly, M.; Black, C.; Prescott, G.J.; Mercer, S.W. Defining and measuring multimorbidity: A systematic review of systematic reviews. Eur. J. Public Health 2019, 29, 182–189. [Google Scholar] [CrossRef] [PubMed]
- Prados-Torres, A.; Calderón-Larrañaga, A.; Hancco-Saavedra, J.; Poblador-Plou, B.; van den Akker, M. Multimorbidity patterns: A systematic review. J. Clin. Epidemiol. 2014, 67, 254–266. [Google Scholar] [CrossRef]
- Diederichs, C.; Berger, K.; Bartels, D.B. The Measurement of Multiple Chronic Diseases—A Systematic Review on Existing Multimorbidity Indices. J. Gerontol. Ser. A 2011, 66, 301–311. [Google Scholar] [CrossRef] [Green Version]
- Violán, C.; Foguet-Boreu, Q.; Fernández-Bertolín, S.; Guisado-Clavero, M.; Cabrera-Bean, M.; Formiga, F.; Valderas, J.M.; Roso-Llorach, A. Soft clustering using real-world data for the identification of multimorbidity patterns in an elderly population: Cross-sectional study in a Mediterranean population. BMJ Open 2019, 9, e029594. [Google Scholar] [CrossRef] [Green Version]
- Zacarías-Pons, L.; Vilalta-Franch, J.; Turró-Garriga, O.; Saez, M.; Garre-Olmo, J. Multimorbidity patterns and their related characteristics in European older adults: A longitudinal perspective. Arch. Gerontol. Geriatr. 2021, 95, 104428. [Google Scholar] [CrossRef]
- Ng, S.K.; Tawiah, R.; Sawyer, M.; Scuffham, P. Patterns of multimorbid health conditions: A systematic review of analytical methods and comparison analysis. Int. J. Epidemiol. 2018, 47, 1687–1704. [Google Scholar] [CrossRef] [Green Version]
- Juul-Larsen, H.G.; Andersen, O.; Bandholm, T.; Bodilsen, A.C.; Kallemose, T.; Jørgensen, L.M.; Klausen, H.H.; Gilkes, H.; Petersen, J. Differences in function and recovery profiles between patterns of multimorbidity among older medical patients the first year after an acute admission—An exploratory latent class analysis. Arch. Gerontol. Geriatr. 2019, 86, 103956. [Google Scholar] [CrossRef]
- Lleal, M.; Corral-Vázquez, C.; Baré, M.; Comet, R.; Herranz, S.; Baigorri, F.; Gimeno-Miguel, A.; Raurich, M.; Fortià, C.; Navarro, M.; et al. Multimorbidity patterns in COVID-19 patients and their relationship to infection severity: MRisk-COVID study. PLoS ONE 2022. under review. [Google Scholar]
- Zheng, D.D.; Loewenstein, D.A.; Christ, S.L.; Feaster, D.J.; Lam, B.L.; McCollister, K.E.; Curiel-Cid, R.E.; Lee, D.J. Multimorbidity patterns and their relationship to mortality in the US older adult population. PLoS ONE 2021, 16, e0245053. [Google Scholar] [CrossRef] [PubMed]
- Teh, R.O.; Menzies, O.H.; Connolly, M.J.; Doughty, R.N.; Wilkinson, T.J.; Pillai, A.; Lumley, T.; Ryan, C.; Rolleston, A.; Broad, J.; et al. Patterns of multi-morbidity and prediction of hospitalisation and all-cause mortality in advanced age. Age Ageing 2018, 47, 261–268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Juul-Larsen, H.G.; Christensen, L.D.; Bandholm, T.; Andersen, O.; Kallemose, T.; Jørgensen, L.M.; Petersen, J. Patterns of Multimorbidity and Differences in Healthcare Utilization and Complexity Among Acutely Hospitalized Medical Patients (≥65 Years)–A Latent Class Approach. Clin. Epidemiol. 2020, 2020, 245–259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carmona-Pírez, J.; Ioakeim-Skoufa, I.; Gimeno-Miguel, A.; Poblador-Plou, B.; González-Rubio, F.; Muñoyerro-Muñiz, D.; Rodríguez-Herrera, J.; Goicoechea-Salazar, J.A.; Prados-Torres, A.; Villegas-Portero, R. Multimorbidity Profiles and Infection Severity in COVID-19 Population Using Network Analysis in the Andalusian Health Population Database. Int. J. Environ. Res. Public Health 2022, 19, 3808. [Google Scholar] [CrossRef] [PubMed]
- Mangoni, A.A.; Jackson, S.H.D. Age-related changes in pharmacokinetics and pharmacodynamics: Basic principles and practical applications. Br. J. Clin. Pharmacol. 2003, 57, 6–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Motter, F.R.; Fritzen, J.S.; Hilmer, S.N.; Paniz, É.V.; Paniz, V.M.V. Potentially inappropriate medication in the elderly: A systematic review of validated explicit criteria. Eur. J. Clin. Pharmacol. 2018, 74, 679–700. [Google Scholar] [CrossRef] [PubMed]
- Corsonello, A.; Pedone, C.; Incalzi, R.A. Age-Related Pharmacokinetic and Pharmacodynamic Changes and Related Risk of Adverse Drug Reactions. Curr. Med. Chem. 2010, 17, 571–584. [Google Scholar] [CrossRef]
- Boparai, M.K.; Korc-Grodzicki, B. Prescribing for Older Adults. Mt. Sinai J. Med. A J. Transl. Pers. Med. 2011, 78, 613–626. [Google Scholar] [CrossRef]
- O’Mahony, D.; O’Sullivan, D.; Byrne, S.; O’Connor, M.N.; Ryan, C.; Gallagher, P. STOPP/START criteria for potentially inappropriate prescribing in older people: Version 2. Age Ageing 2014, 44, 213–218. [Google Scholar] [CrossRef] [Green Version]
- Cadogan, C.A.; Ryan, C.; Hughes, C.M. Appropriate Polypharmacy and Medicine Safety: When Many is not Too Many. Drug Saf. 2016, 39, 109–116. [Google Scholar] [CrossRef] [Green Version]
- Cherubini, A.; Corsonello, A.; Lattanzio, F. Underprescription of Beneficial Medicines in Older People: Causes, Consequences and Prevention. Drugs Aging 2012, 29, 463–475. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Regueiro, R.; Fonseca-Aizpuru, E.; López-Colina, G.; Álvarez-Uría, A.; Rodríguez-Ávila, E.; Morís-De-La-Tassa, J. Prescripción inadecuada y efectos adversos a medicamentos en pacientes de edad avanzada. Rev. Clín. Esp. 2011, 211, 400–406. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, H.; Gallagher, P.; Ryan, C.; Byrne, S.; O’Mahony, D. Potentially Inappropriate Medications Defined by STOPP Criteria and the Risk of Adverse Drug Events in Older Hospitalized Patients. Arch. Intern. Med. 2011, 171, 1013–1019. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mekonnen, A.B.; Redley, B.; de Courten, B.; Manias, E. Potentially inappropriate prescribing and its associations with health-related and system-related outcomes in hospitalised older adults: A systematic review and meta-analysis. Br. J. Clin. Pharmacol. 2021, 87, 4150–4172. [Google Scholar] [CrossRef]
- Oscanoa, T.J.; Lizaraso, F.; Carvajal, A. Hospital admissions due to adverse drug reactions in the elderly. A meta-analysis. Eur. J. Clin. Pharmacol. 2017, 73, 759–770. [Google Scholar] [CrossRef]
- Cabré, M.; Elias, L.; Garcia, M.; Palomera, E.; Serra-Prat, M. Avoidable hospitalizations due to adverse drug reactions in an acute geriatric unit. Analysis of 3,292 patients. Med. Clín. 2018, 150, 209–214. [Google Scholar] [CrossRef]
- Jennings, E.L.M.; Murphy, K.D.; Gallagher, P.; O’Mahony, D. In-hospital adverse drug reactions in older adults; prevalence, presentation and associated drugs—A systematic review and meta-analysis. Age Ageing 2020, 49, 948–958. [Google Scholar] [CrossRef]
- Baré, M.; Herranz, S.; Jordana, R.; Gorgas, M.Q.; Ortonobes, S.; Sevilla, D.; De Jaime, E.; Ibarra, O.; Martín, C. Multimorbidity patterns in chronic older patients, potentially inappropriate prescribing and adverse drug reactions: Protocol of the multicentre prospective cohort study MoPIM. BMJ Open 2020, 10, e033322. [Google Scholar] [CrossRef] [Green Version]
- Baré, M.; Herranz, S.; Roso-Llorach, A.; Jordana, R.; Violán, C.; Lleal, M.; Roura-Poch, P.; Arellano, M.; Estrada, R.; Nazco, G.J. Multimorbidity patterns of chronic conditions and geriatric syndromes in older patients from the MoPIM multicentre cohort study. BMJ Open 2021, 11, e049334. [Google Scholar] [CrossRef]
- Mahoney, F.I.; Barthel, D.W. Functional evaluation: The Barthel Index. Md. State Med. J. 1965, 14, 61–65. [Google Scholar]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef] [PubMed]
- WHO Centre for Health Development. A Glossary of Terms for Community Health Care and Services for Older Persons; WHO Kobe Centre for Health Development Ageing and Health Technical Report; World Health Organization: Geneva, Switzerland, 2004; Available online: http://apps.who.int/iris/bitstream/handle/10665/68896/WHO_WKC_Tech.Ser._04.2.pdf (accessed on 27 October 2022).
- European Medicines Agency; Heads of Medicines Agencies. Guideline on Good Pharmacovigilance Practices (GVP) Module VI–Management and Reporting of Adverse Reactions to Medicinal Products (Rev 1); European Medicines Agency: Amsterdam, The Netherlands, 2014.
- Mascolo, A.; Scavone, C.; Sessa, M.; di Mauro, G.; Cimmaruta, D.; Orlando, V.; Rossi, F.; Sportiello, L.; Capuano, A. Can causality assessment fulfill the new European definition of adverse drug reaction? A review of methods used in spontaneous reporting. Pharmacol. Res. 2017, 123, 122–129. [Google Scholar] [CrossRef] [PubMed]
- Quan, H.; Li, B.; Couris, C.M.; Fushimi, K.; Graham, P.; Hider, P.; Januel, J.-M.; Sundararajan, V. Updating and Validating the Charlson Comorbidity Index and Score for Risk Adjustment in Hospital Discharge Abstracts Using Data From 6 Countries. Am. J. Epidemiol. 2011, 173, 676–682. [Google Scholar] [CrossRef] [Green Version]
- Chavent, M.; Kuentz-Simonet, V.; Labenne, A.; Saracco, J. Multivariate analysis of mixed data: The R package PCAmixdata. arXiv 2014, arXiv:1411.4911. [Google Scholar]
- Bezdek, J.C.; Ehrlich, R.; Full, W. FCM: The fuzzy c-means clustering algorithm. Comput. Geosci. 1984, 10, 191–203. [Google Scholar] [CrossRef]
- Baré, M.; Lleal, M.; Ortonobes, S.; Gorgas, M.Q.; Sevilla-Sánchez, D.; Carballo, N.; De Jaime, E.; Herranz, S. Factors associated to potentially inappropriate prescribing in older patients according to STOPP/START criteria: MoPIM multicentre cohort study. BMC Geriatr. 2022, 22, 44. [Google Scholar] [CrossRef] [PubMed]
- Benjamini, Y.; Hochberg, Y. Controlling the False Discovery Rate: A Practical and Powerful Approach to Multiple Testing. J. R. Stat. Soc. Ser. B 1995, 57, 289–300. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing. 2020. Available online: https://www.r-project.org/ (accessed on 20 April 2022).
- Torres-Bondia, F.; De Batlle, J.; Galván, L.; Buti, M.; Barbé, F.; Piñol-Ripoll, G. Trends in the consumption rates of benzodiazepines and benzodiazepine-related drugs in the health region of Lleida from 2002 to 2015. BMC Public Health 2020, 20, 818. [Google Scholar] [CrossRef]
- Agencia Española de Medicamentos y Productos Sanitarios (AEMPS). Utilización de medicamentos ansiolíticos e hipnóticos en España [Use of anxiolytic and hypnotic drugs in Spain]. 2021. Available online: https://www.aemps.gob.es/medicamentos-de-uso-humano/observatorio-de-uso-de-medicamentos/informes-ansioliticos-hipnoticos/ (accessed on 6 October 2022).
- Gerlach, L.B.; Wiechers, I.R.; Maust, D.T. Prescription Benzodiazepine Use Among Older Adults: A Critical Review. Harv. Rev. Psychiatry 2018, 26, 264–273. [Google Scholar] [CrossRef]
- Markota, M.; Rummans, T.A.; Bostwick, J.M.; Lapid, M.I. Benzodiazepine Use in Older Adults: Dangers, Management, and Alternative Therapies. Mayo Clin. Proc. 2016, 91, 1632–1639. [Google Scholar] [CrossRef]
- Hadley, G.; Derry, S.; Moore, R.A.; Wiffen, P.J. Transdermal fentanyl for cancer pain. Cochrane Database Syst. Rev. 2013, 2018, CD010270. [Google Scholar] [CrossRef] [PubMed]
- Ackerman, S.J.; Knight, T.; Schein, J.; Carter, C.; Staats, P. Risk of Constipation in Patients Prescribed Fentanyl Transdermal System or Oxycodone Hydrochloride Controlled-Release in a California Medicaid Population. Consult. Pharm. 2004, 19, 118–132. [Google Scholar] [CrossRef] [PubMed]
- Oliveros, E.; Patel, H.; Kyung, S.; Fugar, S.; Goldberg, A.; Madan, N.; Williams, K.A. Hypertension in older adults: Assessment, management, and challenges. Clin. Cardiol. 2019, 43, 99–107. [Google Scholar] [CrossRef]
- Na Takuathung, M.; Sakuludomkan, W.; Khatsri, R.; Dukaew, N.; Kraivisitkul, N.; Ahmadmusa, B.; Mahakkanukrauh, C.; Wangthaweesap, K.; Onin, J.; Srichai, S.; et al. Adverse Effects of Angiotensin-Converting Enzyme Inhibitors in Humans: A Systematic Review and Meta-Analysis of 378 Randomized Controlled Trials. Int. J. Environ. Res. Public Health 2022, 19, 8373. [Google Scholar] [CrossRef] [PubMed]
- Townsend, R.R. Major Side Effects of Angiotensin-Converting Enzyme Inhibitors and Angiotensin II Receptor Blockers. UpToDate. Available online: https://www.uptodate.com/contents/major-side-effects-of-angiotensin-converting-enzyme-inhibitors-and-angiotensin-ii-receptor-blockers (accessed on 13 October 2022).
- Jaynes, M.; Kumar, A.B. The risks of long-term use of proton pump inhibitors: A critical review. Ther. Adv. Drug Saf. 2018, 10, 2042098618809927. [Google Scholar] [CrossRef] [PubMed]
- Al-Aly, Z.; Maddukuri, G.; Xie, Y. Proton Pump Inhibitors and the Kidney: Implications of Current Evidence for Clinical Practice and When and How to Deprescribe. Am. J. Kidney Dis. 2020, 75, 497–507. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.-H.; Hsu, W.-T.; Lai, C.-C.; Esmaily-Fard, A.; Tsai, Y.-W.; Chiu, C.-C.; Wang, J.; Chang, S.-S.; Lee, C. Use of antipsychotics increases the risk of fracture: A systematic review and meta-analysis. Osteoporos. Int. 2017, 28, 1167–1178. [Google Scholar] [CrossRef]
- Nosè, M.; Recla, E.; Trifirò, G.; Barbui, C. Antipsychotic drug exposure and risk of pneumonia: A systematic review and meta-analysis of observational studies. Pharmacoepidemiol. Drug Saf. 2015, 24, 812–820. [Google Scholar] [CrossRef]
- Zhai, Y.; Yin, S.; Zhang, D. Association between Antipsychotic Drugs and Mortality in Older Persons with Alzheimer’s Disease: A Systematic Review and Meta-Analysis. J. Alzheimer’s Dis. 2016, 52, 631–639. [Google Scholar] [CrossRef]
- Atti, A.; Gozzi, B.F.; Zuliani, G.; Bernabei, V.; Scudellari, P.; Berardi, D.; De Ronchi, D.; Tarricone, I.; Menchetti, M. A systematic review of metabolic side effects related to the use of antipsychotic drugs in dementia. Int. Psychogeriatr. 2013, 26, 19–37. [Google Scholar] [CrossRef]
- Yang, Y.-L.; Xiang, Z.-J.; Yang, J.-H.; Wang, W.-J.; Xu, Z.-C.; Xiang, R.-L. Association of β-blocker use with survival and pulmonary function in patients with chronic obstructive pulmonary and cardiovascular disease: A systematic review and meta-analysis. Eur. Heart J. 2020, 41, 4415–4422. [Google Scholar] [CrossRef] [PubMed]
- Jungo, K.T.; Streit, S.; Lauffenburger, J.C. Patient factors associated with new prescribing of potentially inappropriate medications in multimorbid US older adults using multiple medications. BMC Geriatr. 2021, 21, 163. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.Q.; Ying, K.; Lun, P.; Tan, K.T.; Ang, W.; Munro, Y.; Ding, Y.Y. Intervention elements to reduce inappropriate prescribing for older adults with multimorbidity receiving outpatient care: A scoping review. BMJ Open 2020, 10, e039543. [Google Scholar] [CrossRef]
- O’Mahony, D.; Gallagher, P.F.; Lavan, A.H. Methods to reduce prescribing errors in elderly patients with multimorbidity. Clin. Interv. Aging 2016, 11, 857–866. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Mahony, D.; O’Connor, M.N.; Eustace, J.; Byrne, S.; Petrovic, M.; Gallagher, P. The adverse drug reaction risk in older persons (ADRROP) prediction scale: Derivation and prospective validation of an ADR risk assessment tool in older multi-morbid patients. Eur. Geriatr. Med. 2018, 9, 191–199. [Google Scholar] [CrossRef]
- Laatikainen, O.; Sneck, S.; Turpeinen, M. Medication-related adverse events in health care—What have we learned? A narrative overview of the current knowledge. Eur. J. Clin. Pharmacol. 2021, 78, 159–170. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Osteo-Articular | Psycho-Geriatric | Minor Chronic Disease | Cardio-Respiratory | ||
|---|---|---|---|---|---|
| n (%) | 137 (18.5) | 151 (20.4) | 127 (17.2) | 325 (43.9) | |
| Age at the time of admission (years, mean ± SD) | 84.3 ± 6.3 | 85.1 ± 6.9 | 83.1 ± 7.2 | 84.1 ± 7.2 | |
| Sex, n (%) | Female | 104 (75.9) | 85 (56.3) | 50 (39.4) | 155 (47.7) |
| Male | 33 (24.1) | 66 (43.7) | 77 (60.6) | 170 (52.3) | |
| Barthel Index (mean ± SD) | 61.6 ± 24.7 | 34.6 ± 31.4 | 77.4 ± 25.6 | 75.9 ± 27.2 | |
| No. of chronic pathologies (mean ± SD) | 11.5 ± 3.6 | 7.7 ± 3.1 | 10.2 ± 3.1 | 7.2 ± 2.3 | |
| No. of geriatric syndromes (mean ± SD) | 7.7 ± 1.8 | 9.1 ± 2.0 | 5.3 ± 2.8 | 4.2 ± 2.0 | |
| No. of chronic prescriptions (mean ± SD) | 12.3 ± 4.58 | 9.5 ± 3.81 | 11.1 ± 4.0 | 10.1 ± 4.1 | |
| Updated Charlson Comorbidity Index, age-adjusted, n (%) | 2–5 | 27 (19.7) | 22 (14.6) | 29 (22.8) | 70 (21.5) |
| 6–8 | 77 (56.2) | 87 (57.6) | 62 (48.8) | 185 (56.9) | |
| 9–14 | 33 (24.1) | 42 (27.8) | 36 (28.3) | 70 (21.5) | |
| Household, n (%) | Alone | 27 (19.7) | 15 (9.9) | 21 (16.5) | 59 (18.2) |
| Nursing home | 17 (12.4) | 35 (23.2) | 8 (6.3) | 35 (10.8) | |
| With relatives/other people | 93 (67.9) | 101 (66.9) | 98 (77.2) | 231 (71.1) | |
| Chronic pathology exacerbation 3 months prior to admission, n (%) | No | 26 (19.0) | 37 (24.5) | 30 (23.6) | 132 (40.6) |
| Yes | 111 (81.0) | 114 (75.5) | 97 (76.4) | 193 (59.4) | |
| Destination at discharge, n (%) | Home | 85 (62.0) | 72 (47.7) | 93 (73.2) | 218 (67.1) |
| Nursing home | 18 (13.1) | 35 (23.2) | 13 (10.2) | 39 (12.0) | |
| Another hospital | 16 (11.7) | 16 (10.6) | 16 (12.6) | 53 (16.3) | |
| Death | 18 (13.1) | 28 (18.5) | 5 (3.9) | 15 (4.6) |
| Osteo-Articular | Psycho-Geriatric | Minor Chronic Disease | Cardio-Respiratory | p-Value | |
|---|---|---|---|---|---|
| n (%) | 137 (18.5) | 151 (20.4) | 127 (17.2) | 325 (43.9) | |
| Any STOPP/START PIP | 130 (94.9) | 118 (78.1) | 106 (83.5) | 249 (76.6) | <0.001 |
| Any STOPP PIMs | 117 (85.4) | 109 (72.2) | 91 (71.7) | 225 (69.2) | 0.002 |
| Any START PPOs | 93 (67.9) | 87 (57.6) | 79 (62.2) | 148 (45.5) | <0.001 |
| Osteo-Articular | Psycho-Geriatric | Minor Chronic Disease | Cardio-Respiratory | p-Value | |
|---|---|---|---|---|---|
| n (%) | 137 (18.5) | 151 (20.4) | 127 (17.2) | 325 (43.9) | |
| Any ADR | 66 (48.2) | 31 (20.5) | 60 (47.2) | 88 (27.1) | <0.001 |
| Any ADR at admission | 45 (32.8) | 22 (14.6) | 39 (30.7) | 47 (14.5) | <0.001 |
| Any ADR during hospitalisation | 32 (23.4) | 11 (7.3) | 30 (23.6) | 47 (14.5) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lleal, M.; Baré, M.; Ortonobes, S.; Sevilla-Sánchez, D.; Jordana, R.; Herranz, S.; Gorgas, M.Q.; Espaulella-Ferrer, M.; Arellano, M.; de Antonio, M.; et al. Comprehensive Multimorbidity Patterns in Older Patients Are Associated with Quality Indicators of Medication—MoPIM Cohort Study. Int. J. Environ. Res. Public Health 2022, 19, 15902. https://doi.org/10.3390/ijerph192315902
Lleal M, Baré M, Ortonobes S, Sevilla-Sánchez D, Jordana R, Herranz S, Gorgas MQ, Espaulella-Ferrer M, Arellano M, de Antonio M, et al. Comprehensive Multimorbidity Patterns in Older Patients Are Associated with Quality Indicators of Medication—MoPIM Cohort Study. International Journal of Environmental Research and Public Health. 2022; 19(23):15902. https://doi.org/10.3390/ijerph192315902
Chicago/Turabian StyleLleal, Marina, Marisa Baré, Sara Ortonobes, Daniel Sevilla-Sánchez, Rosa Jordana, Susana Herranz, Maria Queralt Gorgas, Mariona Espaulella-Ferrer, Marta Arellano, Marta de Antonio, and et al. 2022. "Comprehensive Multimorbidity Patterns in Older Patients Are Associated with Quality Indicators of Medication—MoPIM Cohort Study" International Journal of Environmental Research and Public Health 19, no. 23: 15902. https://doi.org/10.3390/ijerph192315902
APA StyleLleal, M., Baré, M., Ortonobes, S., Sevilla-Sánchez, D., Jordana, R., Herranz, S., Gorgas, M. Q., Espaulella-Ferrer, M., Arellano, M., de Antonio, M., Nazco, G. J., Hernández-Luis, R., & on behalf of the MoPIM Study Group. (2022). Comprehensive Multimorbidity Patterns in Older Patients Are Associated with Quality Indicators of Medication—MoPIM Cohort Study. International Journal of Environmental Research and Public Health, 19(23), 15902. https://doi.org/10.3390/ijerph192315902