
Mental Health and Wellbeing in Young People in the UK during Lockdown (COVID-19)

Abstract
:1. Introduction
The Current Study
- Depression, depressogenic cognition (rumination), wellbeing, stress and sleep disturbance (collectively: mental wellbeing) and diet and exercise (health behaviours) would be poorer for young people during the lockdown, relative to pre-pandemic levels.
- Mental wellbeing would be worse for those in higher relative to lower lockdown restrictions.
- The negative effects of lockdown on mental wellbeing would persist from T1 to T2.
2. Materials and Methods
2.1. Sample Size Calculation
2.2. Participants
2.3. Measures
2.3.1. Retrospective Questions on Change
2.3.2. Depression
2.3.3. Wellbeing
2.3.4. Sleep Disturbance
2.3.5. Rumination
2.3.6. Perceived Stress
2.3.7. Lockdown Status
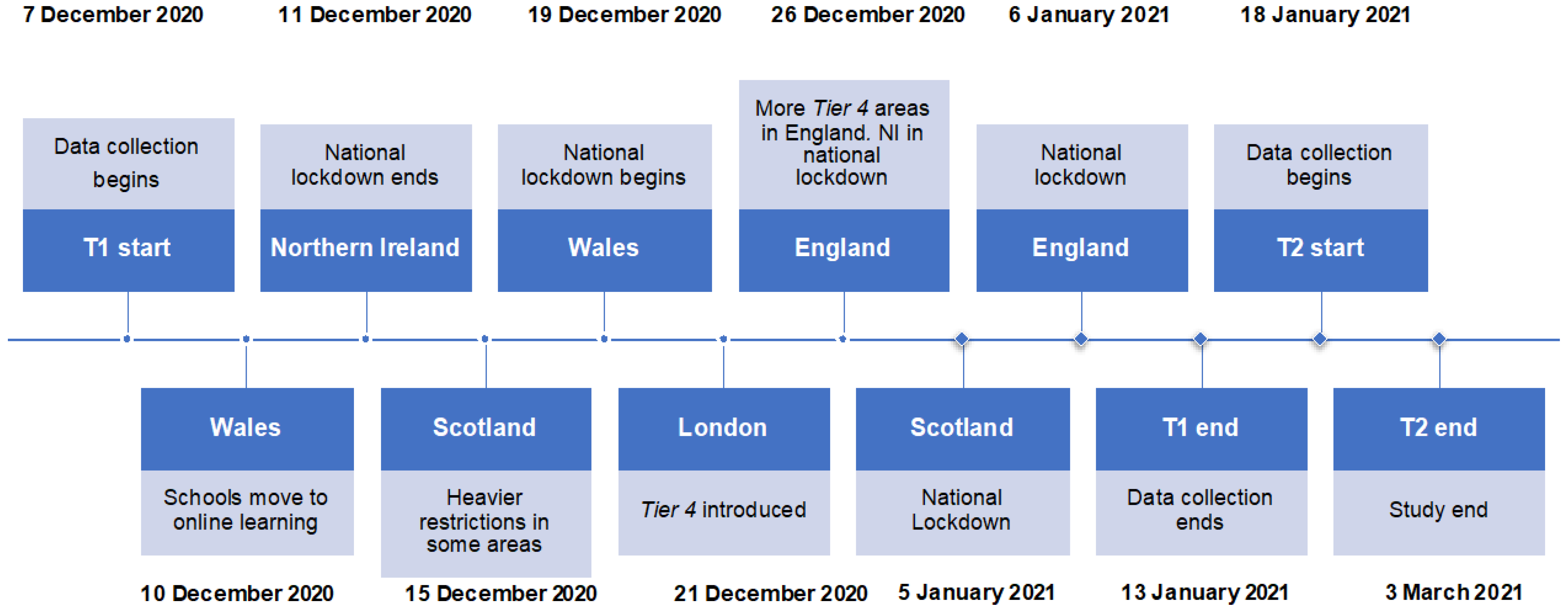
2.3.8. Procedure
2.3.9. Statistical Analysis
3. Results
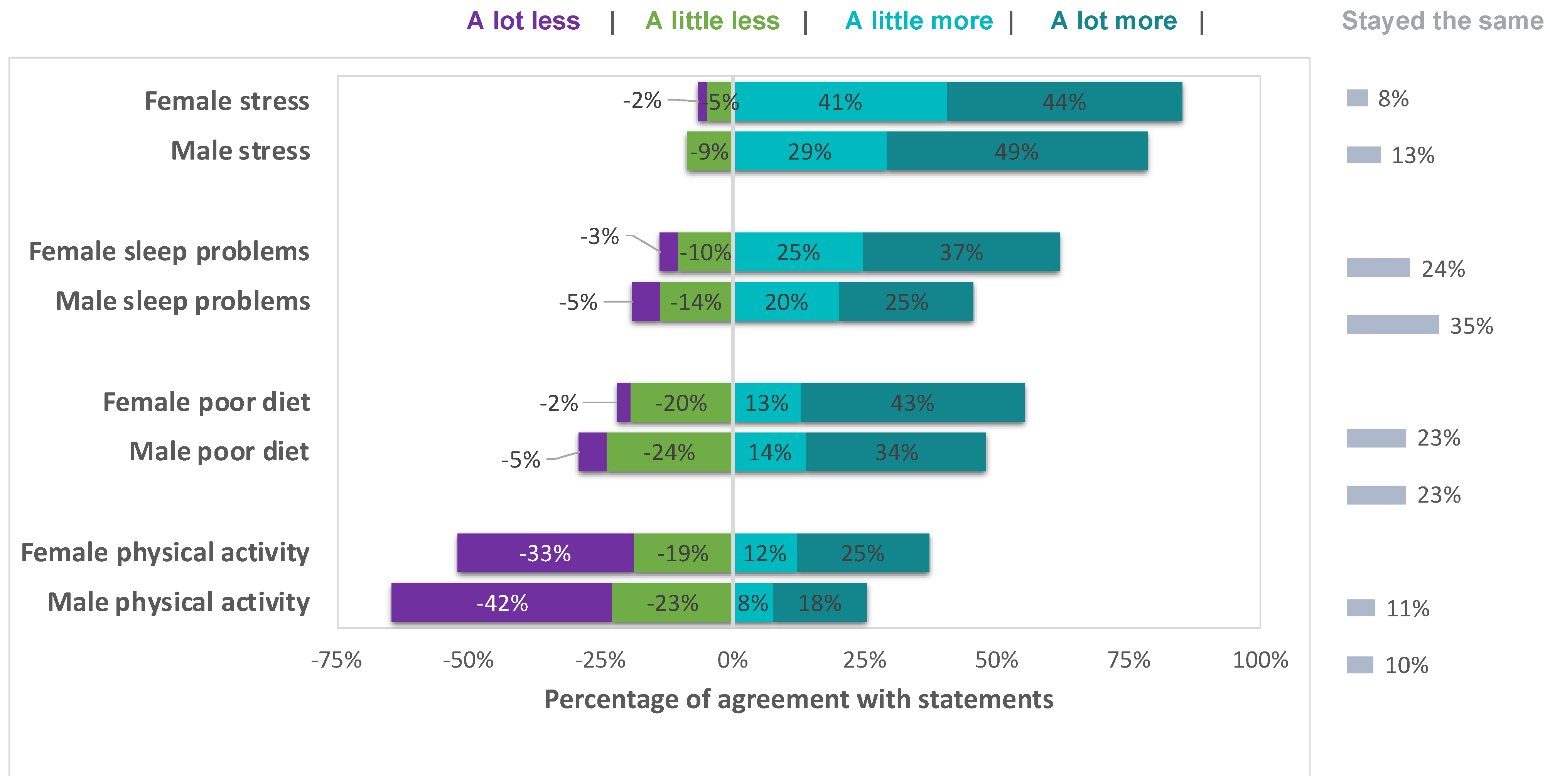
3.1. Retrospective Views on Change through the Pandemic
3.2. Proportion of Participants with Potential for Clinical Need
3.2.1. Depression
3.2.2. Wellbeing
3.2.3. Sleep Disturbance
3.2.4. Rumination
3.2.5. Stress
3.3. Cross-Sectional and Prospective Associations between Lockdown Restriction Severity and Mental Wellbeing
3.4. Effect of Age and Sex
4. Discussion
5. Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Agrawal, V.; Cantor, J.; Sood, N.; Whaley, C. The Impact of the COVID-19 Pandemic and Policy Responses on Excess Mortality; National Bureau of Economic Research: Cambridge, MA. USA, 2021. [Google Scholar]
- Morris, E.J.A.; Goldacre, R.; Spata, E.; Mafham, M.; Finan, P.J.; Shelton, J.; Richards, M.; Spencer, K.; Emberson, J.; Hollings, S.; et al. Impact of the COVID-19 Pandemic on the Detection and Management of Colorectal Cancer in England: A Population-Based Study. Lancet Gastroenterol. Hepatol. 2021, 6, 199–208. [Google Scholar] [CrossRef]
- Holland, K.M.; Jones, C.; Vivolo-Kantor, A.M.; Idaikkadar, N.; Zwald, M.; Hoots, B.; Yard, E.; D’Inverno, A.; Swedo, E.; Chen, M.S.; et al. Trends in US Emergency Department Visits for Mental Health, Overdose, and Violence Outcomes Before and During the COVID-19 Pandemic. JAMA Psychiatry 2021, 78, 372–379. [Google Scholar] [CrossRef]
- Ganesan, B.; Al-Jumaily, A.; Fong, K.N.K.; Prasad, P.; Meena, S.K.; Tong, R.K.-Y. Impact of Coronavirus Disease 2019 (COVID-19) Outbreak Quarantine, Isolation, and Lockdown Policies on Mental Health and Suicide. Front. Psychiatry 2021, 12, 565190. [Google Scholar] [CrossRef] [PubMed]
- Robb, C.E.; de Jager, C.A.; Ahmadi-Abhari, S.; Giannakopoulou, P.; Udeh-Momoh, C.; McKeand, J.; Price, G.; Car, J.; Majeed, A.; Ward, H.; et al. Associations of Social Isolation with Anxiety and Depression During the Early COVID-19 Pandemic: A Survey of Older Adults in London, UK. Front. Psychiatry 2020, 11, 591120. [Google Scholar] [CrossRef] [PubMed]
- Gray, N.S.; O’Connor, C.; Knowles, J.; Pink, J.; Simkiss, N.J.; Williams, S.D.; Snowden, R.J. The Influence of the COVID-19 Pandemic on Mental Well-Being and Psychological Distress: Impact Upon a Single Country. Front. Psychiatry 2020, 11, 594115. [Google Scholar] [CrossRef] [PubMed]
- Ma, L.; Mazidi, M.; Li, K.; Li, Y.; Chen, S.; Kirwan, R.; Zhou, H.; Yan, N.; Rahman, A.; Wang, W.; et al. Prevalence of Mental Health Problems among Children and Adolescents during the COVID-19 Pandemic: A Systematic Review and Meta-Analysis. J. Affect. Disord. 2021, 293, 78–89. [Google Scholar] [CrossRef]
- Ingram, J.; Maciejewski, G.; Hand, C.J. Changes in Diet, Sleep, and Physical Activity Are Associated with Differences in Negative Mood During COVID-19 Lockdown. Front. Psychol. 2020, 11, 2328. [Google Scholar] [CrossRef]
- Evans, S.; Alkan, E.; Bhangoo, J.K.; Tenenbaum, H.; Ng-Knight, T. Effects of the COVID-19 Lockdown on Mental Health, Wellbeing, Sleep, and Alcohol Use in a UK Student Sample. Psychiatry Res. 2021, 298, 113819. [Google Scholar] [CrossRef]
- Fancourt, D.; Steptoe, A.; Bu, F. Trajectories of Anxiety and Depressive Symptoms during Enforced Isolation Due to COVID-19 in England: A Longitudinal Observational Study. Lancet Psychiatry 2021, 8, 141–149. [Google Scholar] [CrossRef]
- Jamieson, D.; Kannis-Dymand, L.; Beaudequin, D.A.; Schwenn, P.; Shan, Z.; McLoughlin, L.T.; Lagopoulos, J.; Hermens, D.F. Can Measures of Sleep Quality or White Matter Structural Integrity Predict Level of Worry or Rumination in Adolescents Facing Stressful Situations? Lessons from the COVID-19 Pandemic. J. Adolesc. 2021, 91, 110–118. [Google Scholar] [CrossRef] [PubMed]
- Albery, I.P.; Spada, M.M.; Nikčević, A.V. The COVID-19 Anxiety Syndrome and Selective Attentional Bias towards COVID-19-Related Stimuli in UK Residents during the 2020–2021 Pandemic. Clin. Psychol. Psychother. 2021, 28, 1367–1378. [Google Scholar] [CrossRef] [PubMed]
- Baiano, C.; Zappullo, I.; Conson, M.; The LabNPEE Group. Tendency to Worry and Fear of Mental Health during Italy’s COVID-19 Lockdown. Int. J. Environ. Res. Public Health 2020, 17, 5928. [Google Scholar] [CrossRef] [PubMed]
- Breslau, J.; Finucane, M.L.; Locker, A.R.; Baird, M.D.; Roth, E.A.; Collins, R.L. A Longitudinal Study of Psychological Distress in the United States before and during the COVID-19 Pandemic. Prev. Med. 2021, 143, 106362. [Google Scholar] [CrossRef]
- Benke, C.; Autenrieth, L.K.; Asselmann, E.; Pané-Farré, C.A. Lockdown, Quarantine Measures, and Social Distancing: Associations with Depression, Anxiety and Distress at the Beginning of the COVID-19 Pandemic among Adults from Germany. Psychiatry Res. 2020, 293, 113462. [Google Scholar] [CrossRef]
- Ozamiz-Etxebarria, N.; Dosil-Santamaria, M.; Picaza-Gorrochategui, M.; Idoiaga-Mondragon, N. Stress, Anxiety, and Depression Levels in the Initial Stage of the COVID-19 Outbreak in a Population Sample in the Northern Spain. Cad. Saúde Pública 2020, 36, e00054020. [Google Scholar] [CrossRef]
- Pierce, M.; Hope, H.; Ford, T.; Hatch, S.; Hotopf, M.; John, A.; Kontopantelis, E.; Webb, R.; Wessely, S.; McManus, S.; et al. Mental Health before and during the COVID-19 Pandemic: A Longitudinal Probability Sample Survey of the UK Population. Lancet Psychiatry 2020, 7, 883–892. [Google Scholar] [CrossRef]
- Lewis, G.; Jones, P.B.; Goodyer, I.M. The ROOTS Study: A 10-Year Review of Findings on Adolescent Depression, and Recommendations for Future Longitudinal Research. Soc. Psychiatry Psychiatr. Epidemiol. 2016, 51, 161–170. [Google Scholar] [CrossRef] [Green Version]
- Townsend, E. Self-Harm in Young People. Evid.-Based Ment. Health 2014, 17, 97–99. [Google Scholar] [CrossRef]
- Jones, P.B. Adult Mental Health Disorders and Their Age at Onset. Br. J. Psychiatry 2013, 202, s5–s10. [Google Scholar] [CrossRef]
- Kessler, R.C.; Berglund, P.; Demler, O.; Jin, R.; Merikangas, K.R.; Walters, E.E. Lifetime Prevalence and Age-of-Onset Distributions of DSM-IV Disorders in the National Comorbidity Survey Replication. Arch. Gen. Psychiatry 2005, 62, 593–602. [Google Scholar] [CrossRef] [Green Version]
- Herrman, H.; Kieling, C.; McGorry, P.; Horton, R.; Sargent, J.; Patel, V. Reducing the Global Burden of Depression: A Lancet–World Psychiatric Association Commission. Lancet 2019, 393, e42–e43. [Google Scholar] [CrossRef]
- Hale, D.R.; Bevilacqua, L.; Viner, R.M. Adolescent Health and Adult Education and Employment: A Systematic Review. Pediatrics 2015, 136, 128–140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kessler, R.C. The Costs of Depression. Psychiatr. Clin. N Am. 2012, 35, 1–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Samaritans. Economic Disruption and Young Adults; Samaritans: Brierley Hill, UK, 2021; pp. 2–40. Available online: https://media.samaritans.org/documents/Samaritans_EconomicDisruptionReport_2021.pdf (accessed on 4 January 2022).
- Hakulinen, C.; Elovainio, M.; Arffman, M.; Lumme, S.; Pirkola, S.; Keskimäki, I.; Manderbacka, K.; Böckerman, P. Mental Disorders and Long-term Labour Market Outcomes: Nationwide Cohort Study of 2 055 720 Individuals. Acta Psychiatr. Scand. 2019, 140, 371–381. [Google Scholar] [CrossRef]
- Thorley, C. Not by Degress: Improving Student Mental Health in the UK’s Universities. IPPR 2017, 3–71. Available online: https://www.ippr.org/files/2017-09/1504645674_not-by-degrees-170905.pdf (accessed on 4 January 2022).
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The Psychological Impact of Quarantine and How to Reduce It: Rapid Review of the Evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [Green Version]
- Usher, K.; Jackson, D.; Durkin, J.; Gyamfi, N.; Bhullar, N. Pandemic-Related Behaviours and Psychological Outcomes; A Rapid Literature Review to Explain COVID-19 Behaviours. Int. J. Ment. Health Nurs. 2020, 29, 1018–1034. [Google Scholar] [CrossRef]
- Ludvigsson, J.F. Systematic Review of COVID-19 in Children Shows Milder Cases and a Better Prognosis than Adults. Acta Paediatr. 2020, 109, 1088–1095. [Google Scholar] [CrossRef]
- Bhopal, S.S.; Bagaria, J.; Olabi, B.; Bhopal, R. Children and Young People Remain at Low Risk of COVID-19 Mortality. Lancet Child Adolesc. Health 2021, 5, e12–e13. [Google Scholar] [CrossRef]
- Spiegelhalter, D. Use of “Normal” Risk to Improve Understanding of Dangers of Covid-19. BMJ 2020, 370, m3259. [Google Scholar] [CrossRef]
- Buonsenso, D.; Roland, D.; De Rose, C.; Vásquez-Hoyos, P.; Ramly, B.; Chakakala-Chaziya, J.N.; Munro, A.; González-Dambrauskas, S. Schools Closures during the COVID-19 Pandemic. Pediatric Infect. Dis. J. 2021, 40, E146–E150. [Google Scholar] [CrossRef]
- Loades, M.E.; Chatburn, E.; Higson-Sweeney, N.; Reynolds, S.; Shafran, R.; Brigden, A.; Linney, C.; McManus, M.N.; Borwick, C.; Crawley, E. Rapid Systematic Review: The Impact of Social Isolation and Loneliness on the Mental Health of Children and Adolescents in the Context of COVID-19. J. Am. Acad. Child Adolesc. Psychiatry 2020, 59, 1218–1239.e3. [Google Scholar] [CrossRef] [PubMed]
- Bueno-Notivol, J.; Gracia-García, P.; Olaya, B.; Lasheras, I.; López-Antón, R.; Santabárbara, J. Prevalence of Depression during the COVID-19 Outbreak: A Meta-Analysis of Community-Based Studies. Int. J. Clin. Health Psychol. 2021, 21, 100196. [Google Scholar] [CrossRef]
- González-Sanguino, C.; Ausín, B.; Castellanos, M.Á.; Saiz, J.; López-Gómez, A.; Ugidos, C.; Muñoz, M. Mental Health Consequences during the Initial Stage of the 2020 Coronavirus Pandemic (COVID-19) in Spain. Brain Behav. Immun. 2020, 87, 172–176. [Google Scholar] [CrossRef] [PubMed]
- Stroud, I.; Gutman, L.M. Longitudinal Changes in the Mental Health of UK Young Male and Female Adults during the COVID-19 Pandemic. Psychiatry Res. 2021, 303, 114074. [Google Scholar] [CrossRef]
- Pancani, L.; Marinucci, M.; Aureli, N.; Riva, P. Forced Social Isolation and Mental Health: A Study on 1,006 Italians Under COVID-19 Lockdown. Front. Psychol. 2021, 12, 663799. [Google Scholar] [CrossRef]
- Pouso, S.; Borja, Á.; Fleming, L.E.; Gómez-Baggethun, E.; White, M.P.; Uyarra, M.C. Contact with Blue-Green Spaces during the COVID-19 Pandemic Lockdown Beneficial for Mental Health. Sci. Total Environ. 2021, 756, 143984. [Google Scholar] [CrossRef]
- Ribeiro, J.D.; Franklin, J.C.; Fox, K.R.; Bentley, K.H.; Kleiman, E.M.; Chang, B.P.; Nock, M.K. Self-Injurious Thoughts and Behaviors as Risk Factors for Future Suicide Ideation, Attempts, and Death: A Meta-Analysis of Longitudinal Studies. Psychol. Med. 2016, 46, 225–236. [Google Scholar] [CrossRef]
- Kroenke, K.; Strine, T.W.; Spitzer, R.L.; Williams, J.B.W.; Berry, J.T.; Mokdad, A.H. The PHQ-8 as a Measure of Current Depression in the General Population. J. Affect. Disord. 2009, 114, 163–173. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.W. The PHQ-9. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Wu, Y.; Levis, B.; Riehm, K.E.; Saadat, N.; Levis, A.W.; Azar, M.; Rice, D.B.; Boruff, J.; Cuijpers, P.; Gilbody, S.; et al. Equivalency of the Diagnostic Accuracy of the PHQ-8 and PHQ-9: A Systematic Review and Individual Participant Data Meta-Analysis. Psychol. Med. 2020, 50, 1368–1380. [Google Scholar] [CrossRef]
- Clarke, A.; Friede, T.; Putz, R.; Ashdown, J.; Martin, S.; Blake, A.; Adi, Y.; Parkinson, J.; Flynn, P.; Platt, S.; et al. Warwick-Edinburgh Mental Well-Being Scale (WEMWBS): Validated for Teenage School Students in England and Scotland. A Mixed Methods Assessment. BMC Public Health 2011, 11, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Stewart-Brown, S.; Tennant, A.; Tennant, R.; Platt, S.; Parkinson, J.; Weich, S. Internal Construct Validity of the Warwick-Edinburgh Mental Well-Being Scale (WEMWBS): A Rasch Analysis Using Data from the Scottish Health Education Population Survey. Health Qual. Life Outcomes 2009, 7, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tennant, R.; Hiller, L.; Fishwick, R.; Platt, S.; Joseph, S.; Weich, S.; Parkinson, J.; Secker, J.; Stewart-Brown, S. The Warwick-Edinburgh Mental Well-Being Scale (WEMWBS): Development and UK Validation. Health Qual. Life Outcomes 2007, 5, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Ng Fat, L.; Scholes, S.; Boniface, S.; Mindell, J.; Stewart-Brown, S. Evaluating and Establishing National Norms for Mental Wellbeing Using the Short Warwick–Edinburgh Mental Well-Being Scale (SWEMWBS): Findings from the Health Survey for England. Qual. Life Res. 2017, 26, 1129–1144. [Google Scholar] [CrossRef] [Green Version]
- Juhola, J.; Arokoski, J.P.A.; Ervasti, J.; Kivimäki, M.; Vahtera, J.; Myllyntausta, S.; Saltychev, M. Internal Consistency and Factor Structure of Jenkins Sleep Scale: Cross-Sectional Cohort Study among 80 000 Adults. BMJ Open 2021, 11, 43276. [Google Scholar] [CrossRef]
- Monterrosa-Castro, Á.; Portela-Buelvas, K.; Salguedo-Madrid, M.; Mo-Carrascal, J.; Duran-Méndez Leidy, C. Instruments to Study Sleep Disorders in Climacteric Women. Sleep Sci. 2016, 9, 169–178. [Google Scholar] [CrossRef] [Green Version]
- Tibubos, A.N.; Zenger, M.; Schmalbach, B.; Beutel, M.E.; Brähler, E. Measurement Invariance, Validation and Normative Data of the Jenkins Sleep Scale-4 (JSS-4) in the German General Population across the Life Span. J. Psychosom. Res. 2020, 130, 109933. [Google Scholar] [CrossRef]
- Nolen-Hoeksema, S.; Morrow, J. A Prospective Study of Depression and Posttraumatic Stress Symptoms After a Natural Disaster: The 1989 Loma Prieta Earthquake. J. Personal. Soc. Psychol. 1991, 61, 115–121. [Google Scholar] [CrossRef]
- Treynor, W.; Gonzalez, R.; Nolen-Hoeksema, S. Rumination Reconsidered: A Psychometric Analysis. Cogn. Ther. Res. 2003, 27, 247–259. [Google Scholar] [CrossRef]
- Roelofs, J.; Muris, P.; Huibers, M.; Peeters, F.; Arntz, A. On the Measurement of Rumination: A Psychometric Evaluation of the Ruminative Response Scale and the Rumination on Sadness Scale in Undergraduates. J. Behav. Ther. Exp. Psychiatry 2006, 37, 299–313. [Google Scholar] [CrossRef]
- Cohen, S.; Williamson, G. Perceived Stress in a Probability Sample of the United States. Soc. Psychol. Health 1988, 13, 31–67. [Google Scholar]
- Vallejo, M.A.; Vallejo-Slocker, L.; Fernández-Abascal, E.G.; Mañanes, G. Determining Factors for Stress Perception Assessed with the Perceived Stress Scale (PSS-4) in Spanish and Other European Samples. Front. Psychol. 2018, 9. [Google Scholar] [CrossRef]
- Enders, C.K.; Bandalos, D.L. The Relative Performance of Full Information Maximum Likelihood Estimation for Missing Data in Structural Equation Models. Struct. Equ. Model. Multidiscip. J. 2001, 8, 430–457. [Google Scholar] [CrossRef]
- Cheng, P.; Casement, M.D.; Kalmbach, D.A.; Cuamatzi Castelan, A.; Drake, C.L. Self-Efficacy in Insomnia Symptom Management after Digital CBT-I Mediates Insomnia Severity during the COVID-19 Pandemic. Behav. Sleep Med. 2021, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.; Chen, A.; Chen, Y. College Students’ Stress and Health in the COVID-19 Pandemic: The Role of Academic Workload, Separation from School, and Fears of Contagion. PLoS ONE 2021, 16, e0246676. [Google Scholar] [CrossRef]
- Wu, T.; Jia, X.; Shi, H.; Niu, J.; Yin, X.; Xie, J.; Wang, X. Prevalence of Mental Health Problems during the COVID-19 Pandemic: A Systematic Review and Meta-Analysis. J. Affect. Disord. 2021, 281, 91–98. [Google Scholar] [CrossRef]
- Wittchen, H.U.; Jacobi, F.; Rehm, J.; Gustavsson, A.; Svensson, M.; Jönsson, B.; Olesen, J.; Allgulander, C.; Alonso, J.; Faravelli, C.; et al. The Size and Burden of Mental Disorders and Other Disorders of the Brain in Europe 2010. Eur. Neuropsychopharmacol. 2011, 21, 655–679. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Depression and Other Common Mental Disorders; Global Health Estimates: Geneva, Switzerland, 2017. [Google Scholar]
- Liu, D.; Ren, Y.; Yan, F.; Li, Y.; Xu, X.; Yu, X.; Qu, W.; Wang, Z.; Tian, B.; Yang, F.; et al. Psychological Impact and Predisposing Factors of the Coronavirus Disease 2019 (COVID-19) Pandemic on General Public in China. SSRN Electron. J. 2020, in press. [Google Scholar] [CrossRef]
- Kohls, E.; Baldofski, S.; Moeller, R.; Klemm, S.-L.; Rummel-Kluge, C. Mental Health, Social and Emotional Well-Being, and Perceived Burdens of University Students During COVID-19 Pandemic Lockdown in Germany. Front. Psychiatry 2021, 12, 643957. [Google Scholar] [CrossRef]
- Karing, C. Prevalence and Predictors of Anxiety, Depression and Stress among University Students during the Period of the First Lockdown in Germany. J. Affect. Disord. Rep. 2021, 5, 100174. [Google Scholar] [CrossRef]
- Kokou-Kpolou, C.K.; Megalakaki, O.; Laimou, D.; Kousouri, M. Insomnia during COVID-19 Pandemic and Lockdown: Prevalence, Severity, and Associated Risk Factors in French Population. Psychiatry Res. 2020, 290, 113128. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Zhao, N. Generalized Anxiety Disorder, Depressive Symptoms and Sleep Quality during COVID-19 Outbreak in China: A Web-Based Cross-Sectional Survey. Psychiatry Res. 2020, 288, 112954. [Google Scholar] [CrossRef]
- Voitsidis, P.; Gliatas, I.; Bairachtari, V.; Papadopoulou, K.; Papageorgiou, G.; Parlapani, E.; Syngelakis, M.; Holeva, V.; Diakogiannis, I. Insomnia during the COVID-19 Pandemic in a Greek Population. Psychiatry Res. 2020, 289, 113076. [Google Scholar] [CrossRef]
- Heneghan, C.; Brassey, J.; Jefferson, T. The Impact of Pandemic Restrictions on Childhood Mental Health: A Review of the Literature. medRxiv 2021. [Google Scholar]
- Miles, D.K.; Stedman, M.; Heald, A.H. Stay at Home, Protect the National Health Service, Save Lives: A Cost Benefit Analysis of the Lockdown in the United Kingdom. Int. J. Clin. Pract. 2021, 75, e13674. [Google Scholar] [CrossRef] [PubMed]
- Allen, D.W. Covid Lockdown Cost/Benefits: A Critical Assessment of the Literature. Int. J. Econ. Bus. 2021, 1–32. [Google Scholar] [CrossRef]
- Crawley, E.; Loades, M.; Feder, G.; Logan, S.; Redwood, S.; Macleod, J. Wider Collateral Damage to Children in the UK Because of the Social Distancing Measures Designed to Reduce the Impact of COVID-19 in Adults. BMJ Paediatr. Open 2020, 4, e000701. [Google Scholar] [CrossRef]
- Viner, R.; Russell, S.; Saulle, R.; Croker, H.; Stansfeld, C.; Packer, J.; Nicholls, D.; Goddings, A.-L.; Bonell, C.; Hudson, L.; et al. Impacts of School Closures on Physical and Mental Health of Children and Young People: A Systematic Review. medRxiv 2021. [Google Scholar] [CrossRef]
- Melnick, E.R.; Ioannidis, J.P.A. Should Governments Continue Lockdown to Slow the Spread of Covid-19? BMJ 2020, 369, m1924. [Google Scholar] [CrossRef]
- Bendavid, E.; Oh, C.; Bhattacharya, J. Assessing Mandatory Stay-at-Home and Business Closure Effects on the Spread of COVID-19. Eur. J. Clin. Investig. 2020, 51, e13484. [Google Scholar] [CrossRef]
- Coccia, M. The Relation between Length of Lockdown, Numbers of Infected People and Deaths of Covid-19, and Economic Growth of Countries: Lessons Learned to Cope with Future Pandemics Similar to Covid-19 and to Constrain the Deterioration of Economic System. Sci. Total Environ. 2021, 775, 145801. [Google Scholar] [CrossRef]
- Wood, S.N. Inferring UK COVID-19 Fatal Infection Trajectories from Daily Mortality Data: Were Infections Already in Decline before the UK Lockdowns? Biometrics 2021. [Google Scholar] [CrossRef] [PubMed]
- Racine, N.; Korczak, D.J.; Madigan, S. Evidence Suggests Children Are Being Left behind in COVID-19 Mental Health Research. Eur. Child Adolesc. Psychiatry 2020, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Piquero, A.R.; Jennings, W.G.; Jemison, E.; Kaukinen, C.; Knaul, F.M. Domestic Violence during the COVID-19 Pandemic—Evidence from a Systematic Review and Meta-Analysis. J. Crim. Justice 2021, 74, 101806. [Google Scholar] [CrossRef]
- Zhu, Y.; Xie, J.; Yu, Y. Effect of Home Isolation on Domestic Violence and Divorce in China during COVID-19 Pandemic. Psychiatry Res. 2021, 306, 114234. [Google Scholar] [CrossRef]
- Sonuga-Barke, E.; Fearon, P. Do Lockdowns Scar? Three Putative Mechanisms through Which COVID-19 Mitigation Policies Could Cause Long-term Harm to Young People’s Mental Health. Wiley Online Libr. 2021, 62, 1375–1378. [Google Scholar] [CrossRef] [PubMed]
- McDaid, D. Viewpoint: Investing in Strategies to Support Mental Health Recovery from the COVID-19 Pandemic. Eur. Psychiatry 2021, 64, e32. [Google Scholar] [CrossRef] [PubMed]
- Adhanom Ghebreyesus, T. Addressing Mental Health Needs: An Integral Part of COVID-19 Response. World Psychiatry 2020, 19, 129–130. [Google Scholar] [CrossRef]
- Franklin, J.C.; Ribeiro, J.D.; Fox, K.R.; Bentley, K.H.; Kleiman, E.M.; Huang, X.; Musacchio, K.M.; Jaroszewski, A.C.; Chang, B.P.; Nock, M.K. Risk Factors for Suicidal Thoughts and Behaviors: A Meta-Analysis of 50 Years of Research. Psychol. Bull. 2017, 143, 187–232. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Participants without Missing Data (n = 254) | Participants with Missing Data (n = 135) | p-Value a | |
|---|---|---|---|
| Demographics | |||
| Age (mean, sd) | 21.12 (1.60) | 20.88 (1.65) | 0.17 |
| Gender (%, female) | 73.08 | 81.60 | 0.05 |
| Year of study (%) | 0.18 | ||
| Year 1 | 22.98 | 25.78 | |
| Year 2 | 20.97 | 30.47 | |
| Year 3 | 35.48 | 28.91 | |
| Year 4 | 8.87 | 5.47 | |
| Postgraduate | 11.69 | 9.38 | |
| PHQ (mead, sd) | 11.12 (5.42) | 10.29 (6.06) | 0.39 |
| WELL | 17.06 (7.94) | 17.69 (6.84) | 0.42 |
| PSS | 9.41 (2.62) | 9.66 (2.96) | 0.34 |
| RUM | 11.29 (3.64) | 11.09 (3.94) | 0.63 |
| JSS | 8.29 (5.23) | 8.91 (4.73) | 0.60 |
| Variables | Lower Restrictions (Mean, SD) | Higher Restrictions (Mean, SD) | p-Value for Difference Test (One-Way ANOVA) |
|---|---|---|---|
| PHQ | |||
| T1 | 10.14 (5.46) | 11.88 (5.73) | 0.007 |
| T2 | 9.31 (5.71) | 11.15 (5.24) | 0.014 |
| WMWBS | |||
| T1 | 20.35 (3.97) | 18.35 (4.47) | <0.001 |
| T2 | 21.18 (4.58) | 18.96 (4.50) | <0.001 |
| PSS | |||
| T1 | 9.21 (2.86) | 10.05 (2.51) | 0.006 |
| T2 | 10.16 (3.03) | 11.07 (2.72) | 0.019 |
| RUM | |||
| T1 | 10.92 (3.62) | 11.80 (3.96) | 0.046 |
| T2 | 10.36 (3.74) | 11.55 (3.56) | 0.017 |
| JSS | |||
| T1 | 8.51 (4.86) | 9.18 (4.83) | 0.210 |
| T2 | 7.56 (4.46) | 9.18 (4.89) | 0.009 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Owens, M.; Townsend, E.; Hall, E.; Bhatia, T.; Fitzgibbon, R.; Miller-Lakin, F. Mental Health and Wellbeing in Young People in the UK during Lockdown (COVID-19). Int. J. Environ. Res. Public Health 2022, 19, 1132. https://doi.org/10.3390/ijerph19031132
Owens M, Townsend E, Hall E, Bhatia T, Fitzgibbon R, Miller-Lakin F. Mental Health and Wellbeing in Young People in the UK during Lockdown (COVID-19). International Journal of Environmental Research and Public Health. 2022; 19(3):1132. https://doi.org/10.3390/ijerph19031132
Chicago/Turabian StyleOwens, Matthew, Ellen Townsend, Eleanor Hall, Tanisha Bhatia, Rosie Fitzgibbon, and Francesca Miller-Lakin. 2022. "Mental Health and Wellbeing in Young People in the UK during Lockdown (COVID-19)" International Journal of Environmental Research and Public Health 19, no. 3: 1132. https://doi.org/10.3390/ijerph19031132
APA StyleOwens, M., Townsend, E., Hall, E., Bhatia, T., Fitzgibbon, R., & Miller-Lakin, F. (2022). Mental Health and Wellbeing in Young People in the UK during Lockdown (COVID-19). International Journal of Environmental Research and Public Health, 19(3), 1132. https://doi.org/10.3390/ijerph19031132