
Associations between Sex and Risk Factors for Predicting Chronic Kidney Disease

 ,
,  , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Materials
2.1. Participants
2.2. Instruments
2.3. Procedure and Data Analysis
3. Results
3.1. Risk Factors for Predicting CKD
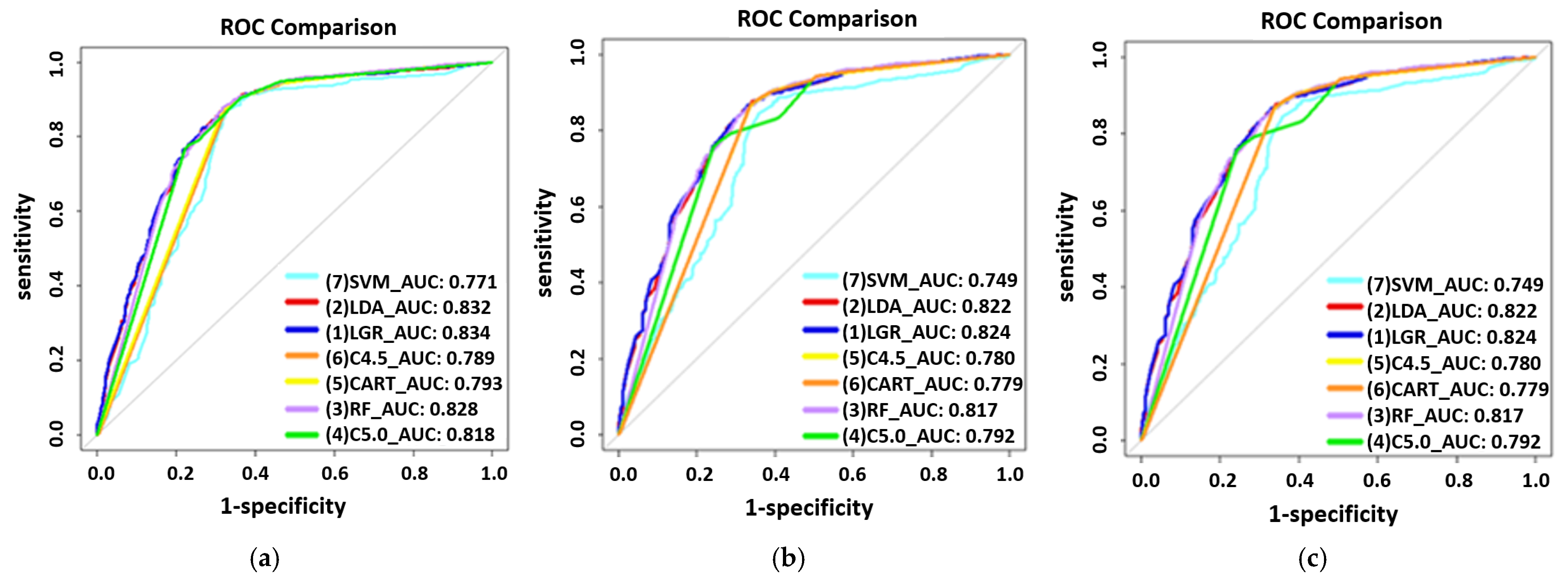
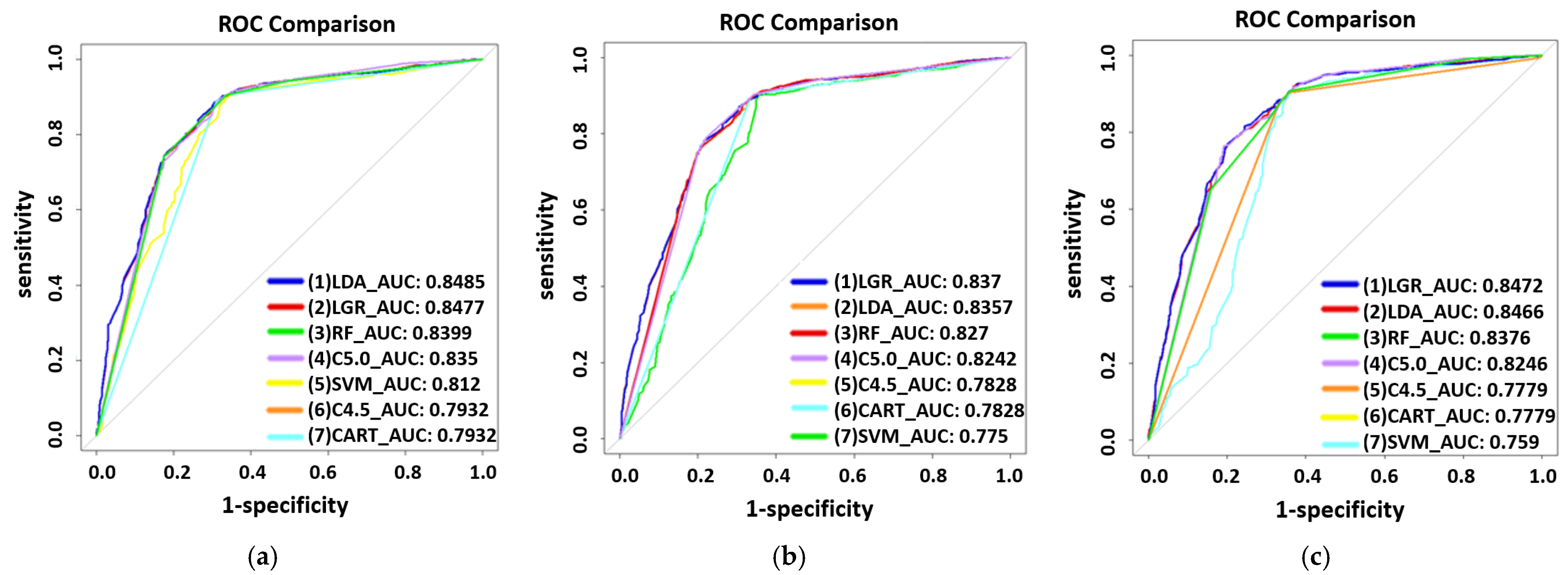
3.2. Prediction Models for CKD
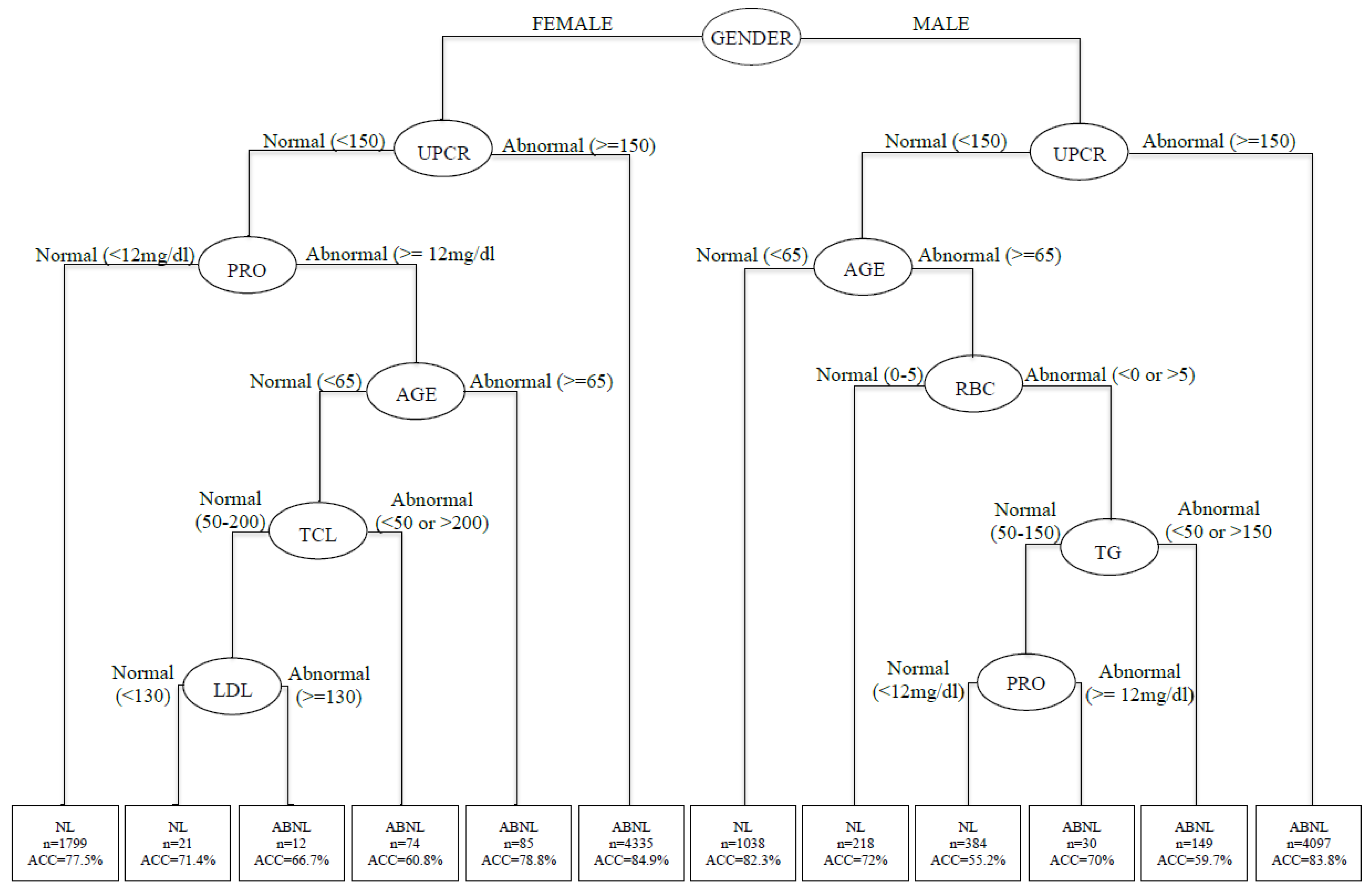
3.3. Decision Tree Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nordqvist, C. Chronic Kidney Disease: Causes, Symptoms and Treatments. Available online: http://www.medicalnewstoday.com/articles/172179.php (accessed on 21 November 2021).
- Smith, D. Chronic Kidney Disease: A Global Crisis. Available online: https://www.siemens-healthineers.com/en-be/news/chronic-kidney-disease.html (accessed on 21 November 2021).
- National Health Research Institutes. Annual Report on Kidney Disease in Taiwan. Available online: http://w3.nhri.org.tw/nhri_org/rl/lib/NewWeb/nhri/ebook/39000000448683.pdf (accessed on 27 September 2021).
- Official Journal of the International Society of Nephrology. KDIGO Clinical Practice Guideline for the Management of Blood Pressure in Chronic Kidney Disease. Available online: https://kdigo.org/wp-content/uploads/2016/10/KDIGO-2012-Blood-Pressure-Guideline-English.pdf (accessed on 27 May 2020).
- Hippisley-Cox, J.; Coupland, C. Predicting the risk of chronic Kidney Disease in men and women in England and Wales: Prospective derivation and external validation of the QKidney Scores. BMC Fam. Pract. 2010, 11, 49. [Google Scholar] [CrossRef] [Green Version]
- Halbesma, N.; Brantsma, A.H.; Bakker, S.J.; Jansen, D.F.; Stolk, R.P.; De Zeeuw, D.; De Jong, P.E.; Gansevoort, R.T.; for the PREVEND study group. Gender differences in predictors of the decline of renal function in the general population. Kidney Int. 2008, 74, 505–512. [Google Scholar] [CrossRef] [Green Version]
- Go, A.S.; Chertow, G.M.; Fan, D.; McCulloch, C.E.; Hsu, C.-Y. Chronic Kidney Disease and the Risks of Death, Cardiovascular Events, and Hospitalization. N. Engl. J. Med. 2004, 351, 1296–1305. [Google Scholar] [CrossRef]
- Albertus, P.; Morgenstern, H.; Robinson, B.; Saran, R. Risk of ESRD in the United States. Am. J. Kidney Dis. 2016, 68, 862–872. [Google Scholar] [CrossRef] [Green Version]
- Hutchens, M.P.; Fujiyoshi, T.; Komers, R.; Herson, P.S.; Anderson, S. Estrogen protects renal endothelial barrier function from ischemia-reperfusion in vitro and in vivo. Am. J. Physiol. Physiol. 2012, 303, F377–F385. [Google Scholar] [CrossRef] [Green Version]
- Elliot, S.J.; Karl, M.; Berho, M.; Potier, M.; Zheng, F.; Leclercq, B.; Striker, G.E.; Striker, L.J. Estrogen Deficiency Accelerates Progression of Glomerulosclerosis in Susceptible Mice. Am. J. Pathol. 2003, 162, 1441–1448. [Google Scholar] [CrossRef] [Green Version]
- Ricardo, A.C.; Yang, W.; Sha, D.; Appel, L.J.; Chen, J.; Krousel-Wood, M.; Manoharan, A.; Steigerwalt, S.; Wright, J.; Rahman, M.; et al. Sex-Related Disparities in CKD Progression. J. Am. Soc. Nephrol. 2019, 30, 137–146. [Google Scholar] [CrossRef] [Green Version]
- Kattah, A.G.; Garovic, V.D. Understanding sex differences in progression and prognosis of chronic kidney disease. Ann. Transl. Med. 2020, 8, 897. [Google Scholar] [CrossRef] [PubMed]
- Roberti, J.; Cummings, A.; Myall, M.; Harvey, J.; Lippiett, K.; Hunt, K.; Cicora, F.; Alonso, J.P.; May, C. Work of being an adult patient with chronic kidney disease: A systematic review of qualitative studies. BMJ Open 2018, 8, e023507. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moyer, V.A.; U.S. Preventive Services Task Force. Screening for chronic kidney disease: U.S. Preventive Services Task Force recommendation statement. Ann. Intern. Med. 2012, 157, 567–570. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tseng, C.-J.; Lu, C.-J.; Chang, C.-C.; Chen, G.-D.; Cheewakriangkrai, C. Integration of data mining classification techniques and ensemble learning to identify risk factors and diagnose ovarian cancer recurrence. Artif. Intell. Med. 2017, 78, 47–54. [Google Scholar] [CrossRef]
- Ting, W.C.; Lu YC, A.; Lu, C.J.; Cheewakriangkrai, C.; Chang, C.C. Recurrence impact of primary site and pathologic stage in patients diagnosed with colorectal cancer. J. Qual. 2018, 25, 166–184. [Google Scholar]
- Chang, C.C.; Chen, S.H. Developing a novel machine learning-based classification scheme for predicting SPCs in breast cancer survivors. Front. Genet. 2019, 10, 848. [Google Scholar] [CrossRef]
- Shih, C.-C.; Chen, S.-H.; Chen, G.-D.; Chang, C.-C.; Shih, Y.-L. Development of a Longitudinal Diagnosis and Prognosis in Patients with Chronic Kidney Disease: Intelligent Clinical Decision-making Scheme. Int. J. Environ. Res. Public Health 2021, 18, 12807. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.-C.; Huang, T.-H.; Shueng, P.-W.; Chen, S.-H.; Chen, C.-C.; Lu, C.-J.; Tseng, Y.-J. Developing a Stacked Ensemble-based Classification Scheme to Predict Second Primary Cancers in Head and Neck Cancer Survivors. Int. J. Environ. Res. Public Health 2021, 18, 12499. [Google Scholar] [CrossRef]
- Chang, C.-C.; Chen, C.-C.; Cheewakriangkrai, C.; Chen, Y.-C.; Yang, S.-F. Risk Prediction of Second Primary Endometrial Cancer in Obese Women: A Hospital-Based Cancer Registry Study. Int J Environ Res Public Health 2021, 18, 8997. [Google Scholar] [CrossRef] [PubMed]
- Chan, C.-L.; Chang, C.-C. Big Data, Decision Models, and Public Health. Int. J. Environ. Res. Public Health 2020, 17, 6723. [Google Scholar] [CrossRef] [PubMed]
- Grubinger, T.; Zeileis, A.; Pfeiffer, K.P. evtree: Evolutionary learning of globally optimal classification and regression trees in R.J. Stat. Softw. 2014, 61, 1–29. [Google Scholar] [CrossRef] [Green Version]
- Hornik, K.; Buchta, C.; Zeileis, A. Open-source machine learning: R meets Weka. Comput. Stat. 2009, 24, 225–232. [Google Scholar] [CrossRef] [Green Version]
- The National Health Insurance Statistics. 2017. Available online: https://www.nhi.gov.tw/english/Content_List.aspx?n=0D39BCF70F478274&topn=616B97F8DF2C3614 (accessed on 21 November 2021).
- Korbut, A.I.; Klimontov, V.V.; Vinogradov, I.V.; Romanov, V.V. Risk factors and urinary biomarkers of non-albuminuric and albuminuric chronic kidney disease in patients with type 2 diabetes. World J. Diabetes 2019, 10, 517–533. [Google Scholar] [CrossRef]
- Haroun, M.K.; Jaar, B.G.; Hoffman, S.C.; Comstock, G.W.; Klag, M.J.; Coresh, J. Risk factors for chronic kidney disease: A prospective study of 23,534 men and women in Washington County, Maryland. J. Am. Soc. Nephrol. 2003, 14, 2934–2941. [Google Scholar] [CrossRef] [Green Version]
- Neugarten, J.; Golestaneh, L. Influence of Sex on the Progression of Chronic Kidney Disease. Mayo Clin. Proc. 2019, 94, 1339–1356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Price, C.P.; Newall, R.G.; Boyd, J.C. Use of Protein: Creatinine Ratio Measurements on Random Urine Samples for Prediction of Significant Proteinuria: A Systematic Review. Clin. Chem. 2005, 51, 1577–1586. [Google Scholar] [CrossRef] [Green Version]
- Hogg, R.J.; Furth, S.; Lemley, K.V.; Portman, R.; Schwartz, G.J.; Coresh, J.; Levey, A.S. National Kidney Foundation’s Kidney Disease Outcomes Quality Initiative clinical practice guidelines for chronic kidney disease in children and adolescents: Evaluation, classification, and stratification. Pediatrics 2003, 111, 1416–1421. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abebe, J.; Eigbefoh, J.; Isabu, P.; Okogbenin, S.; Eifediyi, R.; Okusanya, B. Accuracy of urine dipsticks, 2-h and 12-h urine collections for protein measurement as compared with the 24-h collection. J. Obstet. Gynaecol. 2008, 28, 496–500. [Google Scholar] [CrossRef]
- Kim, M.; Kim, C.S.; Bae, E.H.; Ma, S.K.; Kim, S.W. Risk factors for peptic ulcer disease in patients with end-stage renal disease receiving dialysis. Kidney Res. Clin. Pr. 2019, 38, 81–89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muntner, P.; Coresh, J.; Smith, J.C.; Eckfeldt, J.; Klag, M.J. Plasma lipids and risk of developing renal dysfunction: The Atherosclerosis Risk in Communities Study. Kidney Int. 2000, 58, 293–301. [Google Scholar] [CrossRef] [Green Version]
- Tangri, N.; Stevens, L.A.; Griffith, J.; Tighiouart, H.; Djurdjev, O.; Naimark, D.; Levin, A.; Levey, A.S. A Predictive Model for Progression of Chronic Kidney Disease to Kidney Failure. JAMA 2011, 305, 1553–1559. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brück, K.; Stel, V.S.; Gambaro, G.; Hallan, S.; Völzke, H.; Ärnlöv, J.; Kastarinen, M.; Guessous, I.; Vinhas, J.; Stengel, B.; et al. CKD Prevalence Varies across the European General Population. J. Am. Soc. Nephrol. 2016, 27, 2135–2147. [Google Scholar] [CrossRef]
- Matsushita, K.; Van der Velde, M.; Astor, B.C.; Woodward, M.; Levey, A.S.; De Jong, P.E.; Gansevoort, R.T. Chronic Kidney Disease Prognosis Consortium: Association of estimated glomerular filtration rate and albuminuria with all-cause and cardiovascular mortality in general population cohorts: A collaborative meta-analysis. Lancet 2010, 375, 2073–2081. [Google Scholar]
- Wu, M.T.; Lam, K.K.; Lee, W.C.; Hsu, K.T.; Wu, C.H.; Cheng, B.C.; Lee, C.T. Albuminuria, proteinuria, and urinary albumin to protein ratio in chronic kidney disease. J. Clin. Lab. Anal. 2012, 26, 82–92. [Google Scholar] [CrossRef] [PubMed]
- Van Der Velde, M.; Matsushita, K.; Coresh, J.; Astor, B.C.; Woodward, M.; Levey, A.S.; de Jong, P.E.; Coresh, J. Chronic Kidney Disease Prognosis Consortium. Lower estimated glomerular filtration rate and higher albuminuria are associated with all-cause and cardiovascular mortality. A collaborative meta-analysis of high-risk population cohorts. Kidney Int. 2011, 79, 1341–1352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carrero, J.J.; Hecking, M.; Chesnaye, N.C.; Jager, K.J. Sex and gender disparities in the epidemiology and outcomes of chronic kidney disease. Nat. Rev. Nephrol. 2018, 14, 151–164. [Google Scholar] [CrossRef] [PubMed]
- Tong, A.; Evangelidis, N.; Kurnikowski, A.; Lewandowski, M.J.; Bretschneider, P.; Oberbauer, R.; Baumgart, A.; Scholes-Robertson, A.; Stamm, T.; Carrero, J.J.; et al. Hecking, MNephrologists’ Perspectives on Gender Disparities in CKD and Dialysis. Kidney Int. Rep. 2021; in press. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Stages | Description | GFR Value |
|---|---|---|
| 1 | CKD with normal or high GFR | ≥90 mL/min/1.73 m2 |
| 2 | Mild CKD | 60–89.9 mL/min/1.73 m2 |
| 3 | Moderate CKD | 30–59.9 mL/min/1.73 m2 |
| 3a | 45–59.9 mL/min/1.73 m2 | |
| 3b | 30–44.9 mL/min/1.73 m2 | |
| 4 | Severe CKD | 15–29.9 mL/min/1.73 m2 |
| 5 | End stage CKD | <15 mL/min/1.73 m2 |
| Variables | Name | Normal Range |
|---|---|---|
| X1 | Gender | 1 male/2 female |
| X2 | Age | Continuous |
| X3 | RBC | 0–5 |
| X4 | GLU | 70–100 |
| X5 | TG | 50–150 |
| X6 | T-CHO | 50–200 |
| X7 | HDL | >40 |
| X8 | LDL | <130 |
| X9 | ALB | 3.5–5.0 |
| X10 | PRO | Random < 12 mg/dL |
| X11 | UPCR | <150 |
| Y | eGFR | 1. <90 mL/min/1.73 |
| 2. ≥90 mL/min/1.73 m2 |
| Items | Healthy | CKD | p-Value | χ2 |
|---|---|---|---|---|
| n (%) | 14,169 (73.5%) | 5101 (26.5%) | ||
| Gender | ||||
| Male | 5608 (39.6%) | 2465 (48.3%) | <0.001 ** | 117.817 |
| Female | 8561 (60.4%) | 2636 (51.7%) | ||
| Age | ||||
| Mean (±SD) | 63.37 ± 11.56 | 69.19 ± 10.74 | <0.001 * | 699.271 |
| RBC | ||||
| Normal | 11,460 (80.9%) | 3917 (76.8%) | <0.001 ** | 38.956 |
| Abnormal | 2709 (19.1%) | 1184 (23.2%) | ||
| GLU | ||||
| Normal | 2667 (18.8%) | 1055 (20.7%) | 0.004 ** | 8.321 |
| Abnormal | 11,502 (81.2%) | 4046 (79.3%) | ||
| TG | ||||
| Normal | 5878 (41.5%) | 2012 (39.4%) | 0.011 * | 6.466 |
| Abnormal | 8291 (58.5%) | 3089 (60.6%) | ||
| T-CHO | ||||
| Normal | 9198 (64.9%) | 3284 (64.4%) | 0.491 | 0.474 |
| Abnormal | 4971 (35.1%) | 1817 (35.6%) | ||
| HDL | ||||
| Normal | 11,954 (84.4%) | 4369 (85.6%) | 0.029 * | 4.763 |
| Abnormal | 2215 (15.6%) | 732 (14.4%) | ||
| HDL | ||||
| Normal | 11,400 (80.5%) | 4095 (80.3%) | 0.782 | 0.076 |
| Abnormal | 2769 (19.5%) | 1006 (19.7%) | ||
| ALB | ||||
| Normal | 14,162 (100.0%) | 5097 (99.9%) | 0.457 | 0.553 |
| Abnormal | 7 (0.0%) | 4 (0.1%) | ||
| PRO | ||||
| Normal | 9203 (65.0%) | 915 (17.9%) | <0.001 * | 3324.451 |
| Abnormal | 4966 (35.0%) | 4186(82.1%) | ||
| UPCR | ||||
| Normal | 12,364 (87.3%) | 1639 (32.1%) | <0.001 * | 5739.411 |
| Abnormal | 1805 (12.7%) | 3462 (67.9%) | ||
| Rule No. | The Composition of Risk Factors | No. | Status | Accuracy |
|---|---|---|---|---|
| 1 | Gender (Female) + UPCR (<150) + PRO (<12) | 1799 | Non-CKD | 77.5% |
| 2 | Gender (Female) + UPCR (<150) + PRO (≥12) + Age (<65) + T-CHO (50–200) + LDL (<130) | 21 | Non-CKD | 71.4% |
| 3 | Gender (Female) + UPCR (<150) + PRO (≥12) + Age (<65) + T-CHO (50–200) + LDL (≥130) | 12 | CKD | 66.7% |
| 4 | Gender (Female) + UPCR (<150) + PRO (≥12) + Age (<65) + T-CHO (<50 or >200) | 74 | CKD | 60.8% |
| 5 | Gender (Female) + UPCR (<150) + PRO (≥12) + Age (≥65) | 85 | CKD | 78.8% |
| 6 | Gender (Female) + UPCR (≥150) | 4335 | CKD | 84.9% |
| 7 | Gender (Male) + UPCR (<150) + Age (<65) | 1038 | Non-CKD | 82.3% |
| 8 | Gender (Male) + UPCR (<150) + Age (≥65) + RBC (0–5) | 218 | Non-CKD | 72% |
| 9 | Gender (Male) + UPCR (<150) + Age (≥65) + RBC (<0 or >5) + TG (50–150) + PRO (<12) | 384 | Non-CKD | 55.2% |
| 10 | Gender (Male) + UPCR (<150) + Age (≥65) + RBC (<0 or >5) + TG (50–150) + PRO (≥12) | 30 | CKD | 70% |
| 11 | Gender (Male) + UPCR (<150) + Age (≥ 65) + RBC (<0 or >5) + TG (<50 or >200) | 149 | CKD | 59.7% |
| 12 | Gender (Male) + UPCR (≥ 150) | 4097 | CKD | 83.8% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kao, H.-Y.; Chang, C.-C.; Chang, C.-F.; Chen, Y.-C.; Cheewakriangkrai, C.; Tu, Y.-L. Associations between Sex and Risk Factors for Predicting Chronic Kidney Disease. Int. J. Environ. Res. Public Health 2022, 19, 1219. https://doi.org/10.3390/ijerph19031219
Kao H-Y, Chang C-C, Chang C-F, Chen Y-C, Cheewakriangkrai C, Tu Y-L. Associations between Sex and Risk Factors for Predicting Chronic Kidney Disease. International Journal of Environmental Research and Public Health. 2022; 19(3):1219. https://doi.org/10.3390/ijerph19031219
Chicago/Turabian StyleKao, Hao-Yun, Chi-Chang Chang, Chin-Fang Chang, Ying-Chen Chen, Chalong Cheewakriangkrai, and Ya-Ling Tu. 2022. "Associations between Sex and Risk Factors for Predicting Chronic Kidney Disease" International Journal of Environmental Research and Public Health 19, no. 3: 1219. https://doi.org/10.3390/ijerph19031219
APA StyleKao, H. -Y., Chang, C. -C., Chang, C. -F., Chen, Y. -C., Cheewakriangkrai, C., & Tu, Y. -L. (2022). Associations between Sex and Risk Factors for Predicting Chronic Kidney Disease. International Journal of Environmental Research and Public Health, 19(3), 1219. https://doi.org/10.3390/ijerph19031219