
Treatment Pattern, Financial Burden, and Outcomes in Elderly Patients with Acute Myeloid Leukemia in Korea: A Nationwide Cohort Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source and Definition
2.2. Statistical Analysis
2.3. Ethics
3. Results
3.1. Study Population
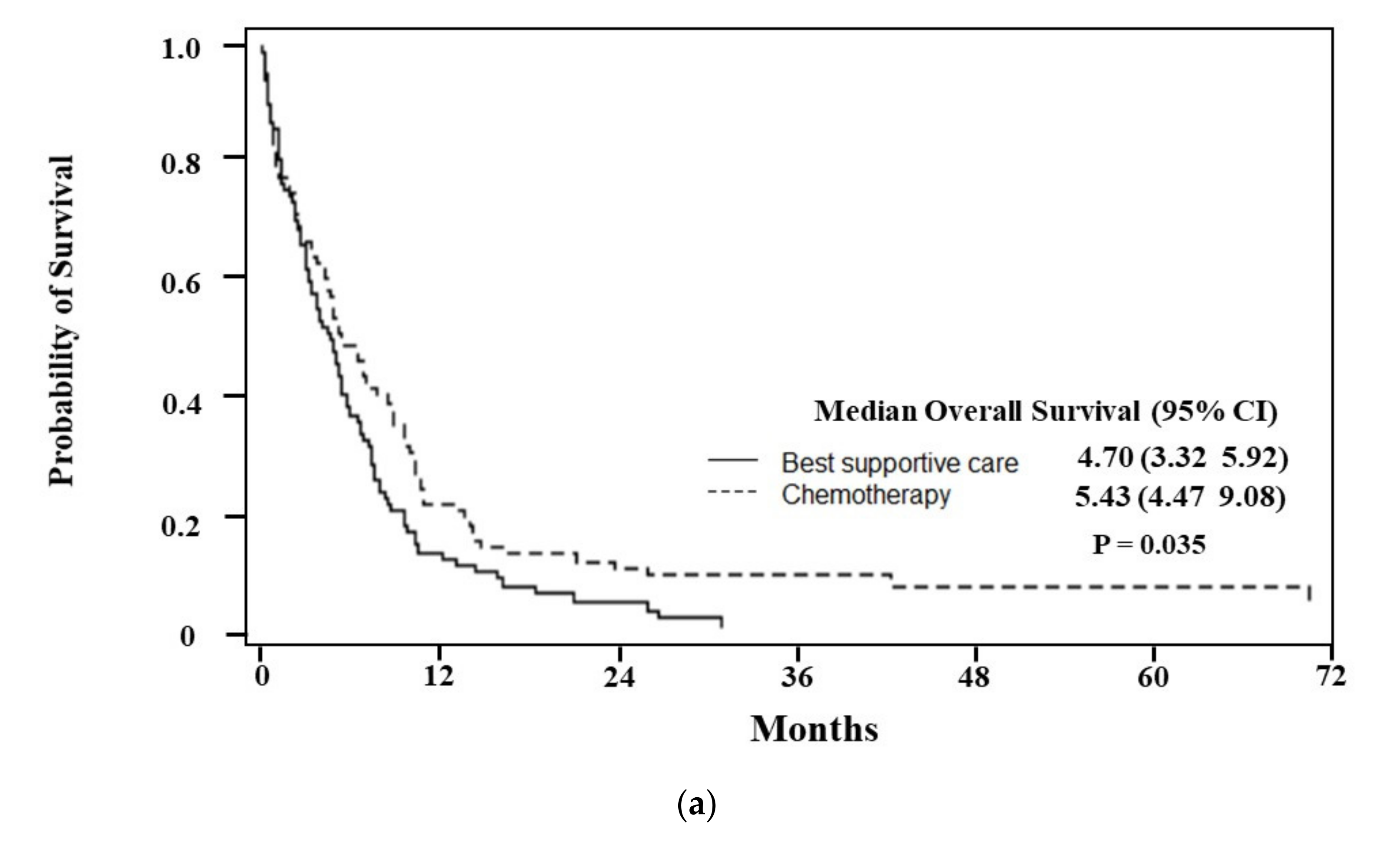
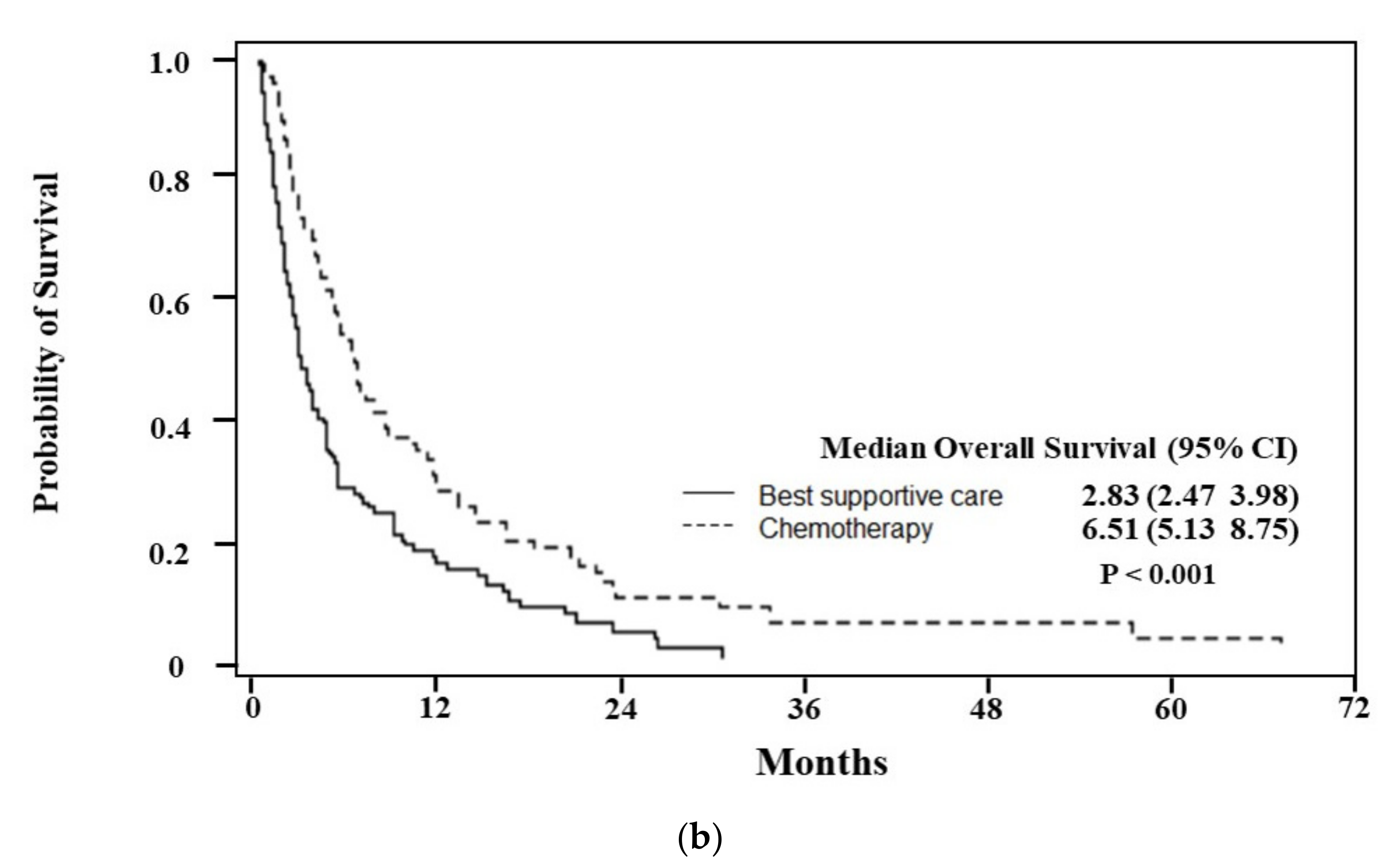
3.2. Treatment Pattern and Outcomes
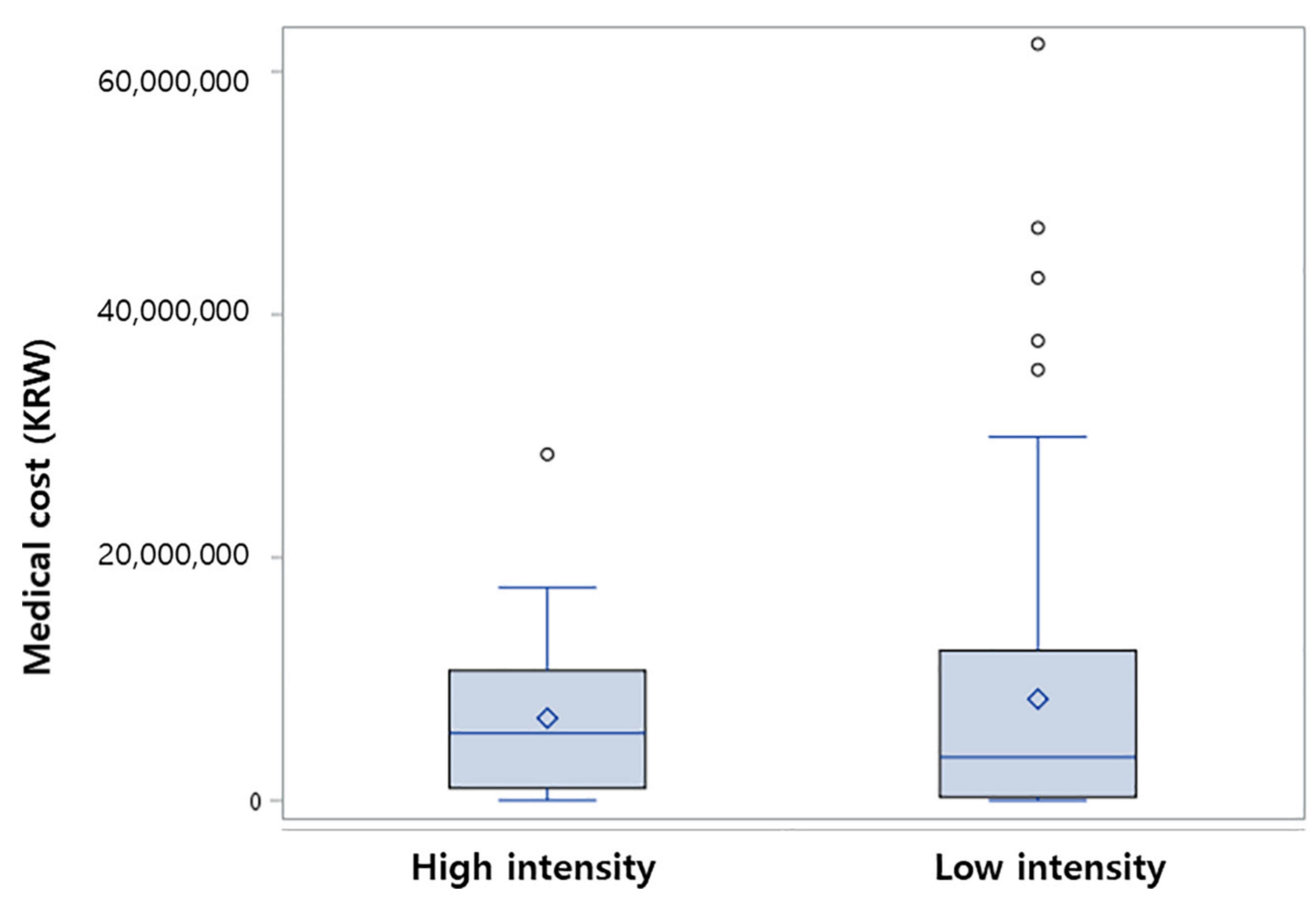
3.3. Medical Cost
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Park, E.H.; Lee, H.; Won, Y.J.; Ju, H.Y.; Oh, C.M.; Ingabire, C.; Kong, H.J.; Park, B.K.; Yoon, J.Y.; Eom, H.S.; et al. Nationwide statistical analysis of myeloid malignancies in Korea: Incidence and survival rate from 1999 to 2012. Blood Res. 2015, 50, 204–217. [Google Scholar] [CrossRef] [Green Version]
- Juliusson, G.; Antunovic, P.; Derolf, A.; Lehmann, S.; Möllgård, L.; Stockelberg, D.; Tidefelt, U.; Wahlin, A.; Höglund, M. Age and acute myeloid leukemia: Real world data on decision to treat and outcomes from the Swedish Acute Leukemia Registry. Blood 2009, 113, 4179–4187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grimwade, D.; Walker, H.; Harrison, G.; Oliver, F.; Chatters, S.; Harrison, C.J.; Wheatley, K.; Burnett, A.K.; Goldstone, A.H. The predictive value of hierarchical cytogenetic classification in older adults with acute myeloid leukemia (AML): Analysis of 1065 patients entered into the United Kingdom Medical Research Council AML11 trial. Blood 2001, 98, 1312–1320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Appelbaum, F.R.; Gundacker, H.; Head, D.R.; Slovak, M.L.; Willman, C.L.; Godwin, J.E.; Anderson, J.E.; Petersdorf, S.H. Age and acute myeloid leukemia. Blood 2006, 107, 3481–3485. [Google Scholar] [CrossRef] [PubMed]
- Rao, A.V. Fitness in the elderly: How to make decisions regarding acute myeloid leukemia induction. Hematol. Am. Soc. Hematol. Educ. Program 2016, 2016, 339–347. [Google Scholar]
- Löwenberg, B.; Ossenkoppele, G.J.; van Putten, W.; Schouten, H.C.; Graux, C.; Ferrant, A.; Sonneveld, P.; Maertens, J.; Jongen-Lavrencic, M.; von Lilienfeld-Toal, M.; et al. High-dose daunorubicin in older patients with acute myeloid leukemia. N. Engl. J. Med. 2009, 361, 1235–1248. [Google Scholar] [CrossRef]
- Löwenberg, B.; Zittoun, R.; Kerkhofs, H.; Jehn, U.; Abels, J.; Debusscher, L.; Cauchie, C.; Peetermans, M.; Solbu, G.; Suciu, S.; et al. On the value of intensive remission-induction chemotherapy in elderly patients of 65+ years with acute myeloid leukemia: A randomized phase III study of the European Organization for Research and Treatment of Cancer Leukemia Group. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 1989, 7, 1268–1274. [Google Scholar] [CrossRef]
- Röllig, C.; Kramer, M.; Gabrecht, M.; Hänel, M.; Herbst, R.; Kaiser, U.; Schmitz, N.; Kullmer, J.; Fetscher, S.; Link, H.; et al. Randomized Comparison of Intermediate-Dose Cytarabine Plus Mitoxantrone (IMA) Versus Standard-Dose Cytarabine Plus Daunorubicin (DA) for Induction Therapy in AML Patients >60 Years. Results from the SAL 60+ Trial. Blood 2015, 126, 222. [Google Scholar] [CrossRef]
- Yi, H.G.; Lee, M.H.; Kim, C.S.; Hong, J.; Park, J.; Lee, J.H.; Han, B.R.; Kim, H.Y.; Zang, D.Y.; Kim, S.H.; et al. Clinical characteristics and treatment outcome of acute myeloid leukemia in elderly patients in Korea: A retrospective analysis. Blood Res. 2014, 49, 95–99. [Google Scholar] [CrossRef] [Green Version]
- Burnett, A.K.; Milligan, D.; Prentice, A.G.; Goldstone, A.H.; McMullin, M.F.; Hills, R.K.; Wheatley, K. A comparison of low-dose cytarabine and hydroxyurea with or without all-trans retinoic acid for acute myeloid leukemia and high-risk myelodysplastic syndrome in patients not considered fit for intensive treatment. Cancer Interdiscip. Int. J. Am. Cancer Soc. 2007, 109, 1114–1124. [Google Scholar] [CrossRef]
- Dombret, H.; Seymour, J.F.; Butrym, A.; Wierzbowska, A.; Selleslag, D.; Jang, J.H.; Kumar, R.; Cavenagh, J.; Schuh, A.C.; Candoni, A.; et al. International phase 3 study of azacitidine vs conventional care regimens in older patients with newly diagnosed AML with >30% blasts. Blood 2015, 126, 291–299. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kucukyurt, S.; Eskazan, A.E. New drugs approved for acute myeloid leukaemia in 2018. Br. J. Clin. Pharmacol. 2019, 85, 2689–2693. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cortes, J.; Perl, A.E.; Döhner, H.; Kantarjian, H.; Martinelli, G.; Kovacsovics, T.; Rousselot, P.; Steffen, B.; Dombret, H.; Estey, E.; et al. Quizartinib, an FLT3 inhibitor, as monotherapy in patients with relapsed or refractory acute myeloid leukaemia: An open-label, multicentre, single-arm, phase 2 trial. Lancet Oncol. 2018, 19, 889–903. [Google Scholar] [CrossRef]
- DiNardo, C.D.; Stein, E.M.; de Botton, S.; Roboz, G.J.; Altman, J.K.; Mims, A.S.; Swords, R.; Collins, R.H.; Mannis, G.N.; Pollyea, D.A.; et al. Durable Remissions with Ivosidenib in IDH1-Mutated Relapsed or Refractory AML. N. Engl. J. Med. 2018, 378, 2386–2398. [Google Scholar] [CrossRef]
- Stein, E.M.; DiNardo, C.D.; Pollyea, D.A.; Fathi, A.T.; Roboz, G.J.; Altman, J.K.; Stone, R.M.; DeAngelo, D.J.; Levine, R.L.; Flinn, I.W.; et al. Enasidenib in mutant IDH2 relapsed or refractory acute myeloid leukemia. Blood 2017, 130, 722–731. [Google Scholar] [CrossRef] [PubMed]
- Perl, A.E.; Martinelli, G.; Cortes, J.E.; Neubauer, A.; Berman, E.; Paolini, S.; Montesinos, P.; Baer, M.R.; Larson, R.A.; Ustun, C.; et al. Gilteritinib or Chemotherapy for Relapsed or Refractory FLT3-Mutated AML. N. Engl. J. Med. 2019, 381, 1728–1740. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.I.; Kim, Y.Y.; Yoon, J.L.; Won, C.W.; Ha, S.; Cho, K.D.; Park, B.R.; Bae, S.; Lee, E.J.; Park, S.Y.; et al. Cohort Profile: National health insurance service-senior (NHIS-senior) cohort in Korea. BMJ Open 2019, 9, e024344. [Google Scholar] [CrossRef] [PubMed]
- Quan, H.; Li, B.; Couris, C.M.; Fushimi, K.; Graham, P.; Hider, P.; Januel, J.M.; Sundararajan, V. Updating and validating the Charlson comorbidity index and score for risk adjustment in hospital discharge abstracts using data from 6 countries. Am. J. Epidemiol. 2011, 173, 676–682. [Google Scholar] [CrossRef] [Green Version]
- Meyers, J.; Yu, Y.; Kaye, J.A.; Davis, K.L. Medicare fee-for-service enrollees with primary acute myeloid leukemia: An analysis of treatment patterns, survival, and healthcare resource utilization and costs. Appl. Health Econ. Health Policy 2013, 11, 275–286. [Google Scholar] [CrossRef]
- Medeiros, B.C.; Satram-Hoang, S.; Hurst, D.; Hoang, K.Q.; Momin, F.; Reyes, C. Big data analysis of treatment patterns and outcomes among elderly acute myeloid leukemia patients in the United States. Ann. Hematol. 2015, 94, 1127–1138. [Google Scholar] [CrossRef] [Green Version]
- Kennedy, V.E.; Keegan, T.H.M.; Li, Q.; Maguire, F.B.; Muffly, L.S. Frontline treatment patterns and outcomes among older adults with acute myeloid leukemia: A population-based analysis in the modern era. Cancer 2022, 128, 139–149. [Google Scholar] [CrossRef] [PubMed]
- Juliusson, G. Most 70- to 79-year-old patients with acute myeloid leukemia do benefit from intensive treatment. Blood 2011, 117, 3473–3474. [Google Scholar] [CrossRef] [PubMed]
- Ossenkoppele, G.; Löwenberg, B. How I treat the older patient with acute myeloid leukemia. Blood 2015, 125, 767–774. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burnett, A.K.; Russell, N.; Hills, R.K.; Panoskaltsis, N.; Khwaja, A.; Hemmaway, C.; Cahalin, P.; Clark, R.E.; Milligan, D. A randomised comparison of the novel nucleoside analogue sapacitabine with low-dose cytarabine in older patients with acute myeloid leukaemia. Leukemia 2015, 29, 1312–1319. [Google Scholar] [CrossRef]
- Dennis, M.; Russell, N.; Hills, R.K.; Hemmaway, C.; Panoskaltsis, N.; McMullin, M.F.; Kjeldsen, L.; Dignum, H.; Thomas, I.F.; Clark, R.E.; et al. Vosaroxin and vosaroxin plus low-dose Ara-C (LDAC) vs low-dose Ara-C alone in older patients with acute myeloid leukemia. Blood 2015, 125, 2923–2932. [Google Scholar] [CrossRef] [Green Version]
- Thomas, X.; Elhamri, M.; Heiblig, M. Emerging pharmacotherapies for elderly acute myeloid leukemia patients. Expert Rev. Hematol. 2020, 13, 619–643. [Google Scholar] [CrossRef]
- Arthur, C.; Jeffrey, A.; Yip, E.; Katsioulas, V.; Nalpantidis, A.; Kerridge, I.; Greenwood, M.; Coyle, L.; Mackinlay, N.; Fay, K.; et al. Prolonged administration of low-dose cytarabine and thioguanine in elderly patients with acute myeloid leukaemia (AML) achieves high complete remission rates and prolonged survival. Leuk. Lymphoma 2020, 61, 831–839. [Google Scholar] [CrossRef]
- Menzin, J.; Lang, K.; Earle, C.C.; Kerney, D.; Mallick, R. The outcomes and costs of acute myeloid leukemia among the elderly. Arch. Intern. Med. 2002, 162, 1597–1603. [Google Scholar] [CrossRef] [Green Version]
- Bell, J.A.; Galaznik, A.; Farrelly, E.; Blazer, M.; Murty, S.; Ogbonnaya, A.; Eaddy, M.; Fram, R.J.; Faller, D.V.; Kota, V. Economic burden of elderly patients with acute myeloid leukemia treated in routine clinical care in the United States. Leuk. Res. 2018, 71, 27–33. [Google Scholar] [CrossRef]
- Batty, N.; Yin, Y.; Wetzler, M. Decitabine is more cost effective than cytarabine and daunorubicin in elderly acute myeloid leukemia patients. J. Cancer Res. Ther. 2014, 2, 68–73. [Google Scholar]
- Alibhai, S.M.; Breunis, H.; Timilshina, N.; Brignardello-Petersen, R.; Tomlinson, G.; Mohamedali, H.; Gupta, V.; Minden, M.D.; Li, M.; Buckstein, R.; et al. Quality of life and physical function in adults treated with intensive chemotherapy for acute myeloid leukemia improve over time independent of age. J. Geriatr. Oncol. 2015, 6, 262–271. [Google Scholar] [CrossRef] [PubMed]
- Timilshina, N.; Breunis, H.; Brandwein, J.M.; Minden, M.D.; Gupta, V.; O’Neill, S.; Tomlinson, G.A.; Buckstein, R.; Li, M.; Alibhai, S.M.H. Do quality of life or physical function at diagnosis predict short-term outcomes during intensive chemotherapy in AML? Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2014, 25, 883–888. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Chemotherapy, N (%) | Best Supportive Care, N (%) | Total | p Value |
|---|---|---|---|---|
| All patients | 195 (41.4) | 276 (58.6) | 471 | |
| Treatment details | ||||
| High-intensity chemotherapy | 28 (14.4) | |||
| Low dose cytarabine | 137 (70.3) | |||
| Hypomethylating agents | 9 (4.6) | |||
| All-trans retinoic acid | 21 (10.8) | |||
| Hydroxyurea | 77 (27.9) | |||
| Best supportive care only | 199 (72.1) | |||
| Age | <0.0001 | |||
| Median (IQR) | 65 (62–69) | 69 (65–73) | ||
| 60–69 years | 148 (51.21) | 141 (48.79) | 289 | |
| 70–79 years | 43 (26.06) | 122 (73.94) | 165 | |
| ≥80 years | 4 (23.53) | 13 (76.47) | 17 | |
| Gender | 0.4247 | |||
| Female | 109 (43.08) | 144 (56.92) | 218 | |
| Male | 86 (39.45) | 132 (60.55) | 253 | |
| CCI | 0.0293 | |||
| 0–1 | 96 (47.06) | 108 (52.94) | 204 | |
| ≥2 | 99 (37.08) | 168 (62.92) | 267 |
| High-Intensity Treatment | Low-Intensity Treatment | p Value | |
|---|---|---|---|
| Total, N | 28 | 146 | |
| Frequency of ER visit (No. of ER visit/No. of patient) | 4.214 | 3.712 | |
| Induction mortality (<8 weeks), N (%) | 0 (0) | 23 (15.8) | |
| Overall survival, median (95% CI) | 9.84 months (5.59–13.95) | 5.23 months (4.47–6.97) | 0.1008 |
| HR (95% CI) | p Value | Adjusted HR * (95% CI) | p Value | |
|---|---|---|---|---|
| Age < 70 | 0.656 (0.537–0.801) | <0.0001 | 0.673 (0.547–0.828) | 0.0002 |
| CCI < 2 | 1.017 (0.835–1.238) | 0.8690 | 1.010 (0.829–1.231) | 0.9178 |
| Chemotherapy | 0.823 (0.674–1.005) | 0.0555 | 0.911 (0.740–1.121) | 0.3774 |
| High-Intensity Chemotherapy, Median (IQR) | Low-Intensity Chemotherapy, Median (IQR) | p Value | |
|---|---|---|---|
| Duration (days) | 37.0 (22–41) | 22.5 (9–41) | 0.0120 |
| Total Cost (KRW, won) | 5,540,645 (1,014,570–10,701,350) | 3,566,285 (285,830–12,352,900) | 0.8313 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ha, H.; Jeong, Y.; Lim, J.H.; Suh, Y.J. Treatment Pattern, Financial Burden, and Outcomes in Elderly Patients with Acute Myeloid Leukemia in Korea: A Nationwide Cohort Study. Int. J. Environ. Res. Public Health 2022, 19, 2317. https://doi.org/10.3390/ijerph19042317
Ha H, Jeong Y, Lim JH, Suh YJ. Treatment Pattern, Financial Burden, and Outcomes in Elderly Patients with Acute Myeloid Leukemia in Korea: A Nationwide Cohort Study. International Journal of Environmental Research and Public Health. 2022; 19(4):2317. https://doi.org/10.3390/ijerph19042317
Chicago/Turabian StyleHa, Hyerim, Yujin Jeong, Joo Han Lim, and Young Ju Suh. 2022. "Treatment Pattern, Financial Burden, and Outcomes in Elderly Patients with Acute Myeloid Leukemia in Korea: A Nationwide Cohort Study" International Journal of Environmental Research and Public Health 19, no. 4: 2317. https://doi.org/10.3390/ijerph19042317
APA StyleHa, H., Jeong, Y., Lim, J. H., & Suh, Y. J. (2022). Treatment Pattern, Financial Burden, and Outcomes in Elderly Patients with Acute Myeloid Leukemia in Korea: A Nationwide Cohort Study. International Journal of Environmental Research and Public Health, 19(4), 2317. https://doi.org/10.3390/ijerph19042317