
Impact of Face-to-Face Teaching in Addition to Electronic Learning on Personal Protective Equipment Doffing Proficiency in Student Paramedics: Randomized Controlled Trial

 ,
,  and
and
Abstract
:1. Introduction
1.1. Background and Importance
1.2. Objectives
2. Materials and Methods
2.1. Study Design and Setting
2.2. Online Platform
2.3. Randomization and Concealment of Allocation
2.4. Enrolment and Consent
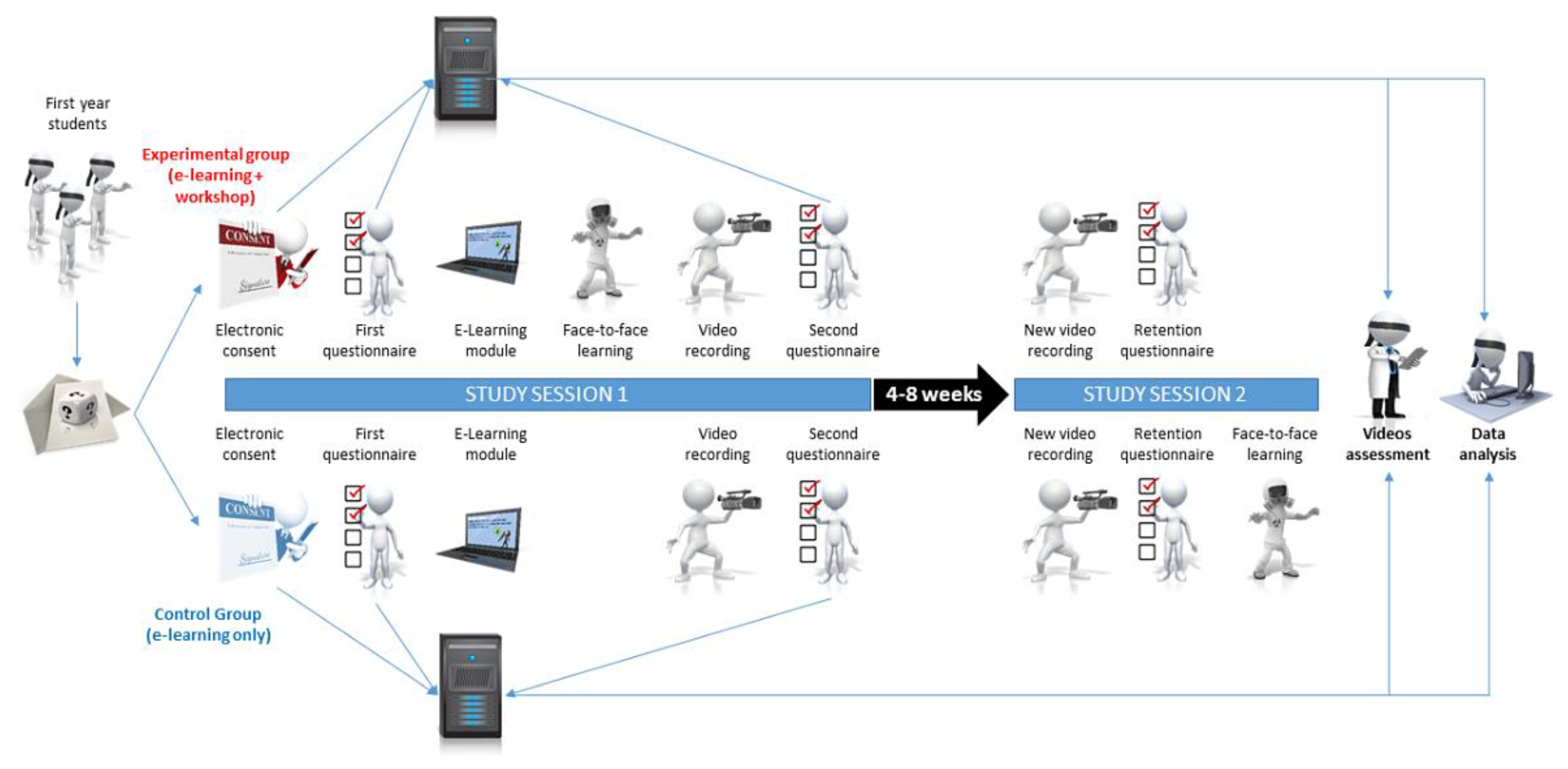
2.5. Study Sequence
2.6. Gamified E-Learning Module
2.7. Face-to-Face Learning
- (1)
- The instructor performed a complete doffing sequence without giving any comments;
- (2)
- The instructor performed a doffing sequence accompanied by step-by-step explanations (description of key points);
- (3)
- Learners were asked to guide the instructor through the doffing sequence, step by step;
- (4)
- Learners were asked to perform the complete doffing sequence before receiving individualized feedback. Each participant performed this step only once.
2.8. Primary Outcome
2.9. Secondary Outcomes
2.10. Blinded Data Collection and Assessment
2.11. Data Availability
2.12. Sample Size
2.13. Statistical Analysis
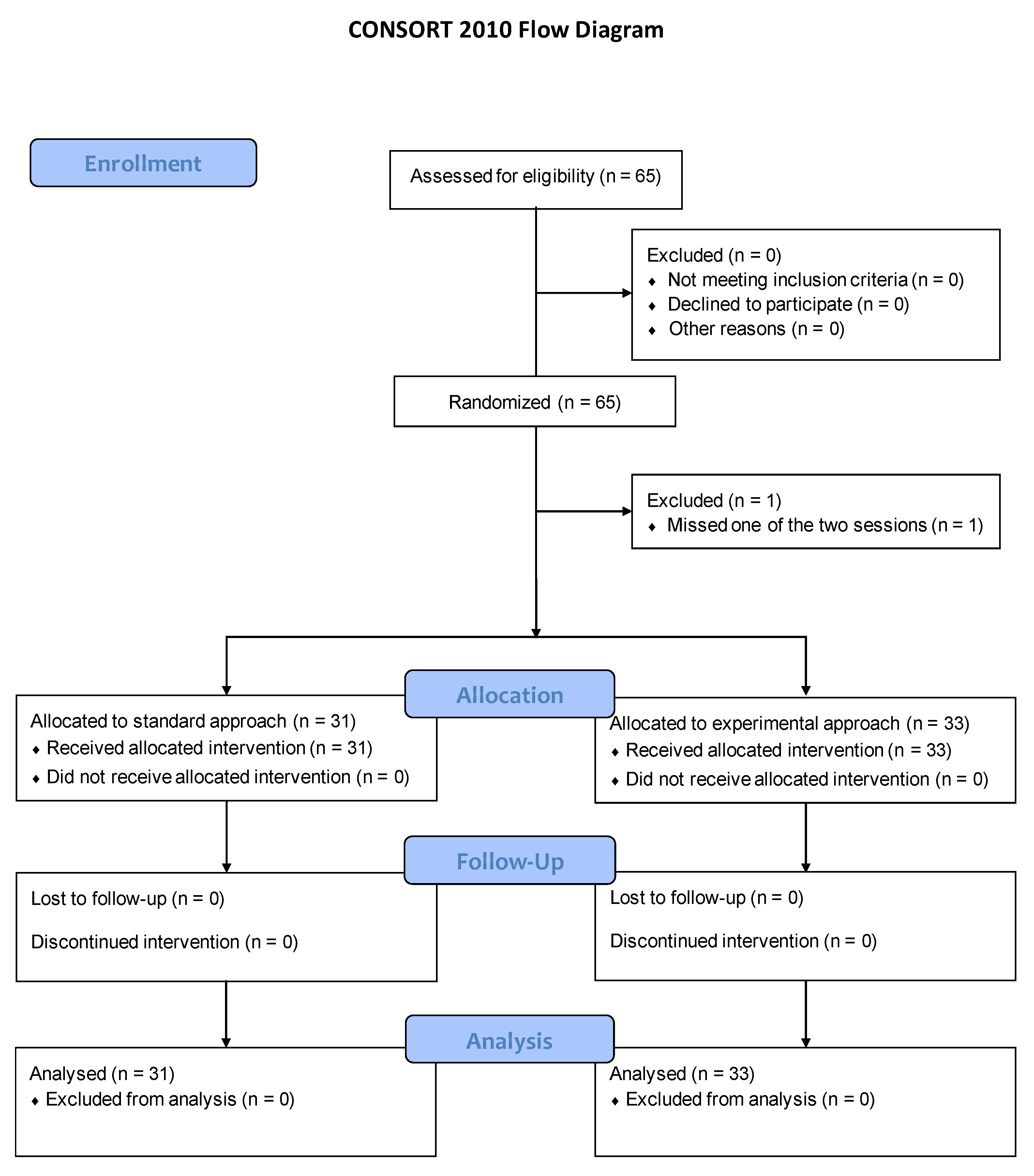
2.14. Protocol Deviations
3. Results
4. Discussion
4.1. Main Considerations
4.2. Limitations and Strengths
4.3. Perspectives and Practical Implications
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cash, R.E.; Rivard, M.K.; Camargo, C.A.; Powell, J.R.; Panchal, A.R. Emergency Medical Services Personnel Awareness and Training about Personal Protective Equipment during the COVID-19 Pandemic. Prehospital Emerg. Care 2021, 25, 777–784. [Google Scholar] [CrossRef] [PubMed]
- Lamhoot, T.; Ben Shoshan, N.; Eisenberg, H.; Fainberg, G.; Mhiliya, M.; Cohen, N.; Bisker-Kassif, O.; Barak, O.; Weiniger, C.; Capua, T. Emergency Department Impaired Adherence to Personal Protective Equipment Donning and Doffing Protocols during the COVID-19 Pandemic. Isr. J. Health Policy Res. 2021, 10, 41. [Google Scholar] [CrossRef] [PubMed]
- Abbas, M.; Robalo Nunes, T.; Martischang, R.; Zingg, W.; Iten, A.; Pittet, D.; Harbarth, S. Nosocomial Transmission and Outbreaks of Coronavirus Disease 2019: The Need to Protect Both Patients and Healthcare Workers. Antimicrob. Resist. Infect. Control 2021, 10, 7. [Google Scholar] [CrossRef] [PubMed]
- Barycka, K.; Torlinski, T.; Filipiak, K.J.; Jaguszewski, M.; Nadolny, K.; Szarpak, L. Risk of Self-Contamination among Healthcare Workers in the COVID-19 Pandemic. Am. J. Emerg. Med. 2021, 46, 751–752. [Google Scholar] [CrossRef]
- Suen, L.K.P.; Guo, Y.P.; Tong, D.W.K.; Leung, P.H.M.; Lung, D.; Ng, M.S.P.; Lai, T.K.H.; Lo, K.Y.K.; Au-Yeung, C.H.; Yu, W. Self-Contamination during Doffing of Personal Protective Equipment by Healthcare Workers to Prevent Ebola Transmission. Antimicrob. Resist. Infect. Control 2018, 7, 157. [Google Scholar] [CrossRef] [Green Version]
- Tomas, M.; Kundrapu, S.; Thota, P.; Sunkesula, V.; Cadnum, J.; Mana, T.; Jencson, A.; O’Donnell, M.; Zabarsky, T.; Hecker, M.; et al. Contamination of Health Care Personnel During Removal of Personal Protective Equipment. JAMA Int. Med. 2015, 175, 1904–1910. [Google Scholar] [CrossRef] [Green Version]
- Beam, E.L.; Gibbs, S.G.; Boulter, K.C.; Beckerdite, M.E.; Smith, P.W. A Method for Evaluating Health Care Workers’ Personal Protective Equipment Technique. Am. J. Infect. Control 2011, 39, 415–420. [Google Scholar] [CrossRef]
- Kang, J.; O’Donnell, J.M.; Colaianne, B.; Bircher, N.; Ren, D.; Smith, K.J. Use of Personal Protective Equipment among Health Care Personnel: Results of Clinical Observations and Simulations. Am. J. Infect. Control 2017, 45, 17–23. [Google Scholar] [CrossRef]
- Okamoto, K.; Rhee, Y.; Schoeny, M.; Lolans, K.; Cheng, J.; Reddy, S.; Weinstein, R.A.; Hayden, M.K.; Popovich, K.J.; Centers for Disease Control and Prevention Epicenters Program. Impact of Doffing Errors on Healthcare Worker Self-Contamination When Caring for Patients on Contact Precautions. Infect. Control Hosp. Epidemiol. 2019, 40, 559–565. [Google Scholar] [CrossRef]
- Casanova, L.M.; Teal, L.J.; Sickbert-Bennett, E.E.; Anderson, D.J.; Sexton, D.J.; Rutala, W.A.; Weber, D.J. CDC Prevention Epicenters Program Assessment of Self-Contamination during Removal of Personal Protective Equipment for Ebola Patient Care. Infect. Control Hosp. Epidemiol 2016, 37, 1156–1161. [Google Scholar] [CrossRef]
- Saran, S.; Gurjar, M.; Garg, A. Identifying and Implementing Strategies to Reduce the Risk of Self-Contamination of Healthcare Workers Caused by Doffing of PPE during COVID-19 Pandemic. Disaster Med. Public Health Prep. 2020, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Wundavalli, L.; Singh, S.; Singh, A.R.; Satpathy, S. How to Rapidly Design and Operationalise PPE Donning and Doffing Areas for a COVID-19 Care Facility: Quality Improvement Initiative. BMJ Open Qual. 2020, 9, e001022. [Google Scholar] [CrossRef] [PubMed]
- Moore, D.; Gamage, B.; Bryce, E.; Copes, R.; Yassi, A.; BC Interdisciplinary Respiratory Protection Study Group. Protecting Health Care Workers from SARS and Other Respiratory Pathogens: Organizational and Individual Factors That Affect Adherence to Infection Control Guidelines. Am. J. Infect. Control 2005, 33, 88–96. [Google Scholar] [CrossRef] [PubMed]
- Savoia, E.; Argentini, G.; Gori, D.; Neri, E.; Piltch-Loeb, R.; Fantini, M.P. Factors Associated with Access and Use of PPE during COVID-19: A Cross-Sectional Study of Italian Physicians. PLoS ONE 2020, 15, e0239024. [Google Scholar] [CrossRef]
- Siegel, J.; Rhinehart, E.; Jackson, M.; Chiarello, L. 2007 Guideline for Isolation Precautions: Preventing Transmission of Infectious Agents in Health Care Settings. Am. J. Infect. Control 2007, 35, S65–S164. [Google Scholar] [CrossRef]
- Fischer, W.A.; Weber, D.; Wohl, D.A. Personal Protective Equipment: Protecting Health Care Providers in an Ebola Outbreak. Clin. Ther. 2015, 37, 2402–2410. [Google Scholar] [CrossRef] [Green Version]
- Hon, C.-Y.; Gamage, B.; Bryce, E.A.; LoChang, J.; Yassi, A.; Maultsaid, D.; Yu, S. Personal Protective Equipment in Health Care: Can Online Infection Control Courses Transfer Knowledge and Improve Proper Selection and Use? Am. J. Infect. Control 2008, 36, e33–e37. [Google Scholar] [CrossRef]
- Verbeek, J.H.; Rajamaki, B.; Ijaz, S.; Sauni, R.; Toomey, E.; Blackwood, B.; Tikka, C.; Ruotsalainen, J.H.; Kilinc Balci, F.S. Personal Protective Equipment for Preventing Highly Infectious Diseases Due to Exposure to Contaminated Body Fluids in Healthcare Staff. Cochrane Database Syst. Rev. 2020, 4, CD011621. [Google Scholar] [CrossRef]
- Suppan, M.; Gartner, B.; Golay, E.; Stuby, L.; White, M.; Cottet, P.; Abbas, M.; Iten, A.; Harbarth, S.; Suppan, L. Teaching Adequate Prehospital Use of Personal Protective Equipment during the COVID-19 Pandemic: Development of a Gamified e-Learning Module. JMIR Serious Games 2020, 8, e20173. [Google Scholar] [CrossRef]
- Suppan, L.; Stuby, L.; Gartner, B.; Larribau, R.; Iten, A.; Abbas, M.; Harbarth, S.; Suppan, M. Impact of an e-Learning Module on Personal Protective Equipment Knowledge in Student Paramedics: A Randomized Controlled Trial. Antimicrob. Resist. Infect. Control 2020, 9, 1–9. [Google Scholar] [CrossRef]
- Suppan, L.; Abbas, M.; Stuby, L.; Cottet, P.; Larribau, R.; Golay, E.; Iten, A.; Harbarth, S.; Gartner, B.; Suppan, M. Effect of an e-Learning Module on Personal Protective Equipment Proficiency among Prehospital Personnel: Web-Based Randomized Controlled Trial. J. Med. Internet Res. 2020, 22, e21265. [Google Scholar] [CrossRef] [PubMed]
- Al-Balas, M.; Al-Balas, H.I.; Jaber, H.M.; Obeidat, K.; Al-Balas, H.; Aborajooh, E.A.; Al-Taher, R.; Al-Balas, B. Distance Learning in Clinical Medical Education amid COVID-19 Pandemic in Jordan: Current Situation, Challenges, and Perspectives. BMC Med. Educ. 2020, 20, 341. [Google Scholar] [CrossRef]
- Khurshid, Z.; De Brún, A.; Moore, G.; McAuliffe, E. Virtual Adaptation of Traditional Healthcare Quality Improvement Training in Response to COVID-19: A Rapid Narrative Review. Hum. Resour. Health 2020, 18, 81. [Google Scholar] [CrossRef] [PubMed]
- Vallée, A.; Blacher, J.; Cariou, A.; Sorbets, E. Blended Learning Compared to Traditional Learning in Medical Education: Systematic Review and Meta-Analysis. J. Med. Internet Res. 2020, 22, e16504. [Google Scholar] [CrossRef]
- Liu, Q.; Peng, W.; Zhang, F.; Hu, R.; Li, Y.; Yan, W. The Effectiveness of Blended Learning in Health Professions: Systematic Review and Meta-Analysis. J. Med. Internet Res. 2016, 18, e2. [Google Scholar] [CrossRef] [Green Version]
- McCutcheon, K.; O’Halloran, P.; Lohan, M. Online Learning versus Blended Learning of Clinical Supervisee Skills with Pre-Registration Nursing Students: A Randomised Controlled Trial. Int. J. Nurs. Stud. 2018, 82, 30–39. [Google Scholar] [CrossRef]
- Peyton, J.W.R. Teaching & Learning in Medical Practice; Manticore Europe Ltd.: Herts, UK, 1998; ISBN 978-1-900887-00-7. [Google Scholar]
- Giacomino, K.; Caliesch, R.; Sattelmayer, K.M. The Effectiveness of the Peyton’s 4-Step Teaching Approach on Skill Acquisition of Procedures in Health Professions Education: A Systematic Review and Meta-Analysis with Integrated Meta-Regression. PeerJ 2020, 8, e10129. [Google Scholar] [CrossRef]
- Stuby, L.; Jampen, L.; Sierro, J.; Paus, E.; Spichiger, T.; Suppan, L.; Thurre, D. Effect on Chest Compression Fraction of Continuous Manual Compressions with Asynchronous Ventilations Using an I-Gel® versus 30:2 Approach during Simulated Out-of-Hospital Cardiac Arrest: Protocol for a Manikin Multicenter Randomized Controlled Trial. Healthcare 2021, 9, 354. [Google Scholar] [CrossRef]
- Stuby, L.; Jampen, L.; Sierro, J.; Bergeron, M.; Paus, E.; Spichiger, T.; Suppan, L.; Thurre, D. Effect of Early Supraglottic Airway Device Insertion on Chest Compression Fraction during Simulated Out-of-Hospital Cardiac Arrest: Randomised Controlled Trial. J. Clin. Med. 2022, 11, 217. [Google Scholar] [CrossRef]
- Stuby, L.; Currat, L.; Gartner, B.; Mayoraz, M.; Harbarth, S.; Suppan, L.; Suppan, M. Impact of Face-to-Face Teaching in Addition to Electronic Learning on Personal Protective Equipment Doffing Proficiency in Student Paramedics: Protocol for a Randomized Controlled Trial. JMIR Res. Protoc 2021, 10, e26927. [Google Scholar] [CrossRef]
- Eysenbach, G.; CONSORT-EHEALTH Group. CONSORT-EHEALTH: Improving and Standardizing Evaluation Reports of Web-Based and Mobile Health Interventions. J. Med. Internet Res. 2011, 13, e126. [Google Scholar] [CrossRef] [PubMed]
- Eysenbach, G. Improving the Quality of Web Surveys: The Checklist for Reporting Results of Internet E-Surveys (CHERRIES). J. Med. Internet Res. 2004, 6, e34. [Google Scholar] [CrossRef] [PubMed]
- Online Study Platform. Available online: https://covid-ppe.anesth.ch/ (accessed on 24 November 2020).
- Create a Blocked Randomisation List|Sealed Envelope. Available online: https://www.sealedenvelope.com/simple-randomiser/v1/lists (accessed on 6 December 2020).
- Keamk—Create Random and Balanced Teams. Available online: https://www.keamk.com/ (accessed on 5 January 2021).
- Verschueren, S.; van Aalst, J.; Bangels, A.-M.; Toelen, J.; Allegaert, K.; Buffel, C.; Vander Stichele, G. Development of CliniPup, a Serious Game Aimed at Reducing Perioperative Anxiety and Pain in Children: Mixed Methods Study. JMIR Serious Games 2019, 7, e12429. [Google Scholar] [CrossRef] [PubMed]
- Verschueren, S.; Buffel, C.; Stichele, G.V. Developing Theory-Driven, Evidence-Based Serious Games for Health: Framework Based on Research Community Insights. JMIR Serious Games 2019, 7, e11565. [Google Scholar] [CrossRef] [PubMed]
- Salway, R.J.; Williams, T.; Londono, C.; Roblin, P.; Koenig, K.; Arquilla, B. Comparing Training Techniques in Personal Protective Equipment Use. Prehosp. Disaster Med. 2020, 35, 364–371. [Google Scholar] [CrossRef] [PubMed]
- Hung, P.-P.; Choi, K.-S.; Chiang, V.C.-L. Using Interactive Computer Simulation for Teaching the Proper Use of Personal Protective Equipment. Comput. Inform. Nurs. 2015, 33, 49–57. [Google Scholar] [CrossRef]
- Bleasdale, S.C.; Sikka, M.K.; Moritz, D.C.; Fritzen-Pedicini, C.; Stiehl, E.; Brosseau, L.M.; Jones, R.M. Experience of Chicagoland Acute Care Hospitals in Preparing for Ebola Virus Disease, 2014–2015. J. Occup. Environ. Hyg. 2019, 16, 582–591. [Google Scholar] [CrossRef]
- Li, Y.; Wang, Y.; Li, Y.; Zhong, M.; Liu, H.; Wu, C.; Gao, X.; Xia, Z.; Ma, W. Comparison of Repeated Video Display vs Combined Video Display and Live Demonstration as Training Methods to Healthcare Providers for Donning and Doffing Personal Protective Equipment: A Randomized Controlled Trial. Risk Manag. Healthc. Policy 2020, 13, 2325–2335. [Google Scholar] [CrossRef]
- Kwon, J.H.; Burnham, C.-A.D.; Reske, K.A.; Liang, S.Y.; Hink, T.; Wallace, M.A.; Shupe, A.; Seiler, S.; Cass, C.; Fraser, V.J.; et al. Assessment of Healthcare Worker Protocol Deviations and Self-Contamination During Personal Protective Equipment Donning and Doffing. Infect. Control Hosp. Epidemiol. 2017, 38, 1077–1083. [Google Scholar] [CrossRef] [Green Version]
- Casanova, L.; Alfano-Sobsey, E.; Rutala, W.A.; Weber, D.J.; Sobsey, M. Virus Transfer from Personal Protective Equipment to Healthcare Employees’ Skin and Clothing. Emerg. Infect. Dis. 2008, 14, 1291–1293. [Google Scholar] [CrossRef]
- Mitchell, A.; Spencer, M.; Edmiston, C. Role of Healthcare Apparel and Other Healthcare Textiles in the Transmission of Pathogens: A Review of the Literature. J. Hosp. Infect. 2015, 90, 285–292. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.-L.; Yang, S.; Luo, H.-X.; You, J.-P. The Error-Prone Operational Steps and Key Sites of Self-Contamination during Donning and Doffing of Personal Protective Equipment by Health Care Workers. Disaster Med. Public Health Prep. 2021, 1–6. [Google Scholar] [CrossRef]
- Mumma, J.M.; Durso, F.T.; Ferguson, A.N.; Gipson, C.L.; Casanova, L.; Erukunuakpor, K.; Kraft, C.S.; Walsh, V.L.; Zimring, C.; DuBose, J.; et al. Human Factors Risk Analyses of a Doffing Protocol for Ebola-Level Personal Protective Equipment: Mapping Errors to Contamination. Clin. Infect. Dis. 2018, 66, 950–958. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pittet, D.; Hugonnet, S.; Harbarth, S.; Mourouga, P.; Sauvan, V.; Touveneau, S.; Perneger, T.V. Effectiveness of a Hospital-Wide Programme to Improve Compliance with Hand Hygiene. Infection Control Programme. Lancet 2000, 356, 1307–1312. [Google Scholar] [CrossRef]
- Boyce, J.M.; Pittet, D. Guideline for Hand Hygiene in Health-Care Settings: Recommendations of the Healthcare Infection Control Practices Advisory Committee and the HICPAC/SHEA/APIC/IDSA Hand Hygiene Task Force. Infect. Control. Hosp. Epidemiol. 2002, 23, S3–S40. [Google Scholar] [CrossRef]
- Doronina, O.; Jones, D.; Martello, M.; Biron, A.; Lavoie-Tremblay, M. A Systematic Review on the Effectiveness of Interventions to Improve Hand Hygiene Compliance of Nurses in the Hospital Setting. J. Nurs. Sch. 2017, 49, 143–152. [Google Scholar] [CrossRef] [Green Version]
- Rayson, D.; Basinda, N.; Pius, R.A.; Seni, J. Comparison of Hand Hygiene Compliance Self-Assessment and Microbiological Hand Contamination among Healthcare Workers in Mwanza Region, Tanzania. Infect. Prev. Pract. 2021, 3, 100181. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, R.; Roth, V.; Gravel, D.; Astrakianakis, G.; Bryce, E.; Forgie, S.; Johnston, L.; Taylor, G.; Vearncombe, M. Canadian Nosocomial Infection Surveillance Program Are Health Care Workers Protected? An Observational Study of Selection and Removal of Personal Protective Equipment in Canadian Acute Care Hospitals. Am. J. Infect. Control 2013, 41, 240–244. [Google Scholar] [CrossRef]
- Kim, L.E.; Jeffe, D.B.; Evanoff, B.A.; Mutha, S.; Freeman, B.; Fraser, J. Improved Compliance with Universal Precautions in the Operating Room Following an Educational Intervention. Infect. Control Hosp. Epidemiol. 2001, 22, 522–524. [Google Scholar] [CrossRef]
- Sedgwick, P.; Greenwood, N. Understanding the Hawthorne Effect. BMJ 2015, 351, h4672. [Google Scholar] [CrossRef] [Green Version]
- Campbell, J.P.; Maxey, V.A.; Watson, W.A. Hawthorne Effect: Implications for Prehospital Research. Ann. Emerg. Med. 1995, 26, 590–594. [Google Scholar] [CrossRef]
- Hagel, S.; Reischke, J.; Kesselmeier, M.; Winning, J.; Gastmeier, P.; Brunkhorst, F.M.; Scherag, A.; Pletz, M.W. Quantifying the Hawthorne Effect in Hand Hygiene Compliance Through Comparing Direct Observation with Automated Hand Hygiene Monitoring. Infect. Control Hosp. Epidemiol. 2015, 36, 957–962. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mortelmans, L.J.M.; Gaakeer, M.I.; Dieltiens, G.; Anseeuw, K.; Sabbe, M.B. Are Dutch Hospitals Prepared for Chemical, Biological, or Radionuclear Incidents? A Survey Study. Prehosp. Disaster Med. 2017, 32, 483–491. [Google Scholar] [CrossRef] [PubMed]
- Felemban, E.M.; Youssef, H.A.M.; Al Thobaity, A. Factors Affecting the Decontamination Process in Hospitals in Saudi Arabia. Risk Manag. Healthc. Policy 2021, 14, 357–363. [Google Scholar] [CrossRef]
- Abelairas-Gómez, C.; Martinez-Isasi, S.; Barcala-Furelos, R.; Varela-Casal, C.; Carballo-Fazanes, A.; Pichel-López, M.; Fernández Méndez, F.; Otero-Agra, M.; Sanchez Santos, L.; Rodriguez-Nuñez, A. Training Frequency for Educating Schoolchildren in Basic Life Support: Very Brief 4-Month Rolling-Refreshers versus Annual Retraining-a 2-Year Prospective Longitudinal Trial. BMJ Open 2021, 11, e052478. [Google Scholar] [CrossRef]
- Saad, R.; Sampaio Favarato, M.H.; Ferreira de Paiva, E.; do Patrocinio Tenorio Nunes, M. Medical Student Skill Retention after Cardiopulmonary Resuscitation Training: A Cross-Sectional Simulation Study. Simul. Healthc. 2019, 14, 351–358. [Google Scholar] [CrossRef]
- Lee, J.; Lee, E.-H.; Chae, D. EHealth Literacy Instruments: Systematic Review of Measurement Properties. J. Med. Internet Res. 2021, 23, e30644. [Google Scholar] [CrossRef]
- Karnoe, A.; Furstrand, D.; Christensen, K.B.; Norgaard, O.; Kayser, L. Assessing Competencies Needed to Engage with Digital Health Services: Development of the eHealth Literacy Assessment Toolkit. J. Med. Internet Res. 2018, 20, e178. [Google Scholar] [CrossRef] [Green Version]
- Matthews, B. Digital Literacy in UK Health Education: What Can Be Learnt from International Research? Contemp. Educ. Technol. 2021, 13, ep317. [Google Scholar] [CrossRef]
- Cheng, L.; Chen, L.; Xiao, L.; Zhang, J.; Cheng, Y.; Zhou, L.; Peng, Y.; Liu, L. Problems and Solutions of Personal Protective Equipment Doffing in COVID-19. Open Med. 2020, 15, 605–612. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| E-Learning (n = 31) | Blended Learning (n = 33) | |
|---|---|---|
| Age, in years, median (Q1;Q3) | 24 (22;26) | 27 (23;28) |
| Gender, n (%) | ||
| Male | 13 (41.9) | 13 (39.4) |
| Female | 18 (58.1) | 20 (60.6) |
| Other | 0 (0.0) | 0 (0.0) |
| Location, n (%) | ||
| Geneva | 8 (25.8) | 10 (30.3) |
| Bern (French-speaking) | 5 (16.1) | 5 (15.2) |
| Bern (German-speaking) | 18 (58.1) | 18 (54.6) |
| Actively working in an ambulance service, n (%) | 24 (77.4) | 24 (72.7) |
| Canton of practice of those currently working, n (%) | ||
| Aargau | 4 (16.7) | 1 (4.2) |
| Basel | 0 (0.0) | 3 (12.5) |
| Bern | 13 (54.2) | 12 (50.0) |
| Fribourg | 0 (0.0) | 2 (8.3) |
| Geneva | 1 (4.2) | 0 (0.0) |
| Neuchâtel | 1 (4.2) | 1 (4.2) |
| Solothurn | 1 (4.2) | 2 (8.3) |
| Vaud | 2 (8.3) | 2 (8.3) |
| Valais | 2 (8.3) | 1 (4.2) |
| VARK scores, median (Q1;Q3) | ||
| visual | 7 (5;9) | 6 (4;7) |
| aural | 8 (5;11) | 8 (6;11) |
| read | 5 (3;6) | 5 (3;7) |
| kinesthetic | 9 (7;11) | 9 (8;10) |
| E-Learning (n = 31) | Blended Learning (n = 33) | p-Value | |
|---|---|---|---|
| Correct sequence among participants actively working, % (95%CI) | 8.3% (1.0 to 27.0) | 29.2% (12.6 to 51.1) | 0.14 |
| Correct sequence among participants not actively working, % (95%CI) | 14.3% (0.3 to 57.9) | 44.4% (13.7 to 78.8) | 0.31 |
| E-Learning (n = 31) | Blended Learning (n = 33) | p-Value | |
|---|---|---|---|
| Time required to perform the doffing procedure at first session, in seconds, median (Q1;Q3) | 133 (107;151) | 129 (118;164) | 0.59 |
| Time required to perform the doffing procedure remotely, in seconds, median (Q1;Q3) | 113 (93;135) | 124 (113;144) | 0.08 |
| Correct computerized sequence at first session in contaminated zone (knowledge at acquisition), % (95%CI) | 80.6% (62.5 to 92.5) | 90.9% (75.0 to 98.1) | 0.30 |
| Correct computerized sequence at first session in non-contaminated zone (knowledge at acquisition), % (95%CI) | 77.4% (58.9 to 90.4) | 72.7% (54.7 to 86.7) | 0.78 |
| Correct computerized full sequence at first session (knowledge at acquisition), % (95%CI) | 64.5% (45.4 to 80.8) | 66.7% (48.2 to 82.0) | 1.00 |
| Correct computerized sequence remotely in contaminated zone at second session (knowledge retention), % (95%CI) | 38.7% (21.8 to 57.8) | 66.7% (48.2 to 82.0) | 0.04 |
| Correct computerized sequence at second session in non-contaminated zone (knowledge retention), % (95%CI) | 64.5% (45.4 to 80.8) | 75.7% (57.7 to 88.9) | 0.42 |
| Correct computerized full sequence at second session (knowledge retention), % (95%CI) | 35.5% (19.2 to 54.6) | 48.5% (30.8 to 66.4) | 0.32 |
| Doffing sequences correctly performed remotely at second session (skill retention), % (95%CI) | 3.2% (0.1 to 16.8) | 24.2% (11.1 to 42.3) | 0.03 |
| E-Learning (n = 31) | Blended Learning (n = 33) | p-Value | |
|---|---|---|---|
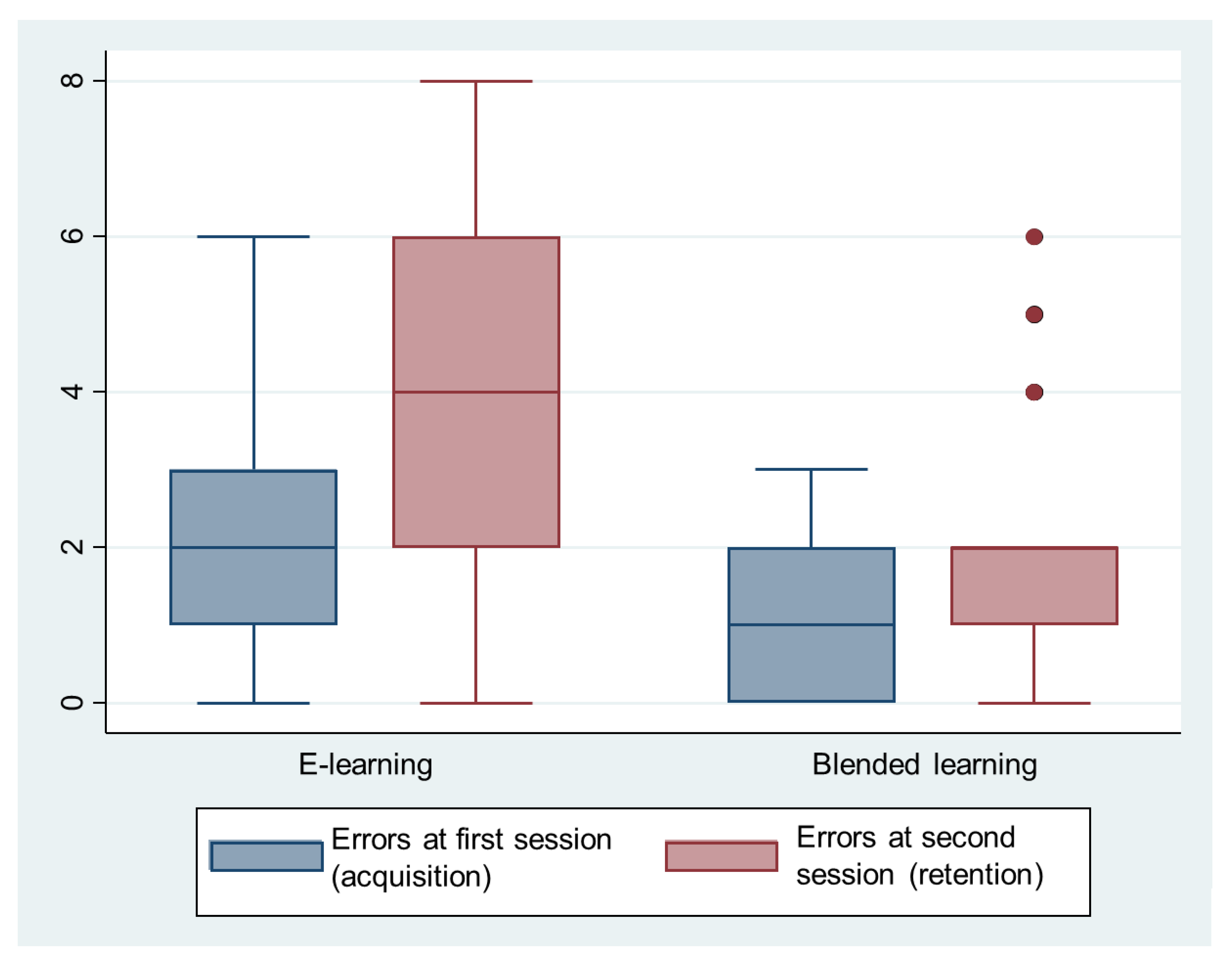
| Number of errors in the procedure at acquisition, median (Q1;Q3) | 2 (1;3) | 1 (0;2) | <0.001 |
| Number of errors in the procedure at retention, median (Q1;Q3) | 4 (2;6) | 2 (1;2) | <0.001 |
| Correct hand disinfection at acquisition, % (95%CI) | 45.2% (27.3 to 64.0) | 63.6% (45.1 to 79.6) | 0.21 |
| Correct hand disinfection at retention, % (95%CI) | 41.9% (24.5 to 60.9) | 57.6% (39.2 to 74.5) | 0.32 |
| E-Learning (n = 31) | Blended Learning (n = 33) | p-Value | |
|---|---|---|---|
| French-speaking participants with third-year student as instructor (n = 28), % (95%CI) | 7.7% (0.2 to 36.0) | 46.7% (21.3 to 73.4) | 0.04 |
| German-speaking participants with teacher as instructor (n = 36), % (95%CI) | 11.1% (1.4 to 34.7) | 22.2% (6.4 to 47.6) | 0.66 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Currat, L.; Suppan, M.; Gartner, B.A.; Daniel, E.; Mayoraz, M.; Harbarth, S.; Suppan, L.; Stuby, L. Impact of Face-to-Face Teaching in Addition to Electronic Learning on Personal Protective Equipment Doffing Proficiency in Student Paramedics: Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2022, 19, 3077. https://doi.org/10.3390/ijerph19053077
Currat L, Suppan M, Gartner BA, Daniel E, Mayoraz M, Harbarth S, Suppan L, Stuby L. Impact of Face-to-Face Teaching in Addition to Electronic Learning on Personal Protective Equipment Doffing Proficiency in Student Paramedics: Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2022; 19(5):3077. https://doi.org/10.3390/ijerph19053077
Chicago/Turabian StyleCurrat, Ludivine, Mélanie Suppan, Birgit Andrea Gartner, Emmanuel Daniel, Mathieu Mayoraz, Stephan Harbarth, Laurent Suppan, and Loric Stuby. 2022. "Impact of Face-to-Face Teaching in Addition to Electronic Learning on Personal Protective Equipment Doffing Proficiency in Student Paramedics: Randomized Controlled Trial" International Journal of Environmental Research and Public Health 19, no. 5: 3077. https://doi.org/10.3390/ijerph19053077
APA StyleCurrat, L., Suppan, M., Gartner, B. A., Daniel, E., Mayoraz, M., Harbarth, S., Suppan, L., & Stuby, L. (2022). Impact of Face-to-Face Teaching in Addition to Electronic Learning on Personal Protective Equipment Doffing Proficiency in Student Paramedics: Randomized Controlled Trial. International Journal of Environmental Research and Public Health, 19(5), 3077. https://doi.org/10.3390/ijerph19053077