1. Introduction
Asthma is one of the most common chronic diseases that affects long-term population health. Chronic airway inflammation and narrowing of lung airways, leading to respiratory symptoms such as coughing, chest tightness, and shortness of breath, are common characteristics of asthma that require in-patient admissions for severe symptoms [
1]. The data of the Global Health Data Exchange in 2017 showed that the incidence of asthma was 0.56%, whereas the prevalence and mortality rates were 3.57% and 0.006%, respectively. A high incidence was found in children aged 0–4 years, and a high prevalence was detected in children and adolescents aged 0–14 years [
2]. These findings indicate that asthma is the most common chronic disease in childhood, reflecting a main cause of childhood morbidity. Improvements in asthma care and a reduction in hospital admissions are important for disease management [
1]. Asthma admission rates in most European countries declined from 2001 to 2015 in children, adolescents, and adults [
3]. A total of 15–50% of pediatric patients were readmitted. In the USA, the risk factors associated with asthma readmission include being of African American race, public or lack of insurance, previous hospital admission, and complex chronic comorbidity [
4]. In the USA, the readmission hospitalization of children with asthma reached more than 40%. The readmission rate within 30 days totaled 2.5% [
5]. Differences in the mortality of children and young adult patients are due to socioeconomic status (SES) or a life-limiting condition (LLC) [
6]. The death rate of asthma patients decreased from 15 per million to 10 per million from 2001 to 2016. The highest death rate was observed in the elderly [
7].
In Thailand, asthma is one of the most common non-communicable diseases, especially among younger children. A Global Asthma Network (GAN) survey in Thailand revealed that the asthma prevalence in children was over 10% [
3], which supported the need for research into the hospital utilization and admission rates. The Global Initiative for Asthma (GINA) was established by the National Heart Lung and Blood Institute in collaboration with the World Health Organization in 1993. It comprises a network of individuals, organizations, and public health officials who publish information about health care patients with asthma. The GINA report, which emphasizes the Global Strategy for Asthma Management and Prevention, has been updated annually since 2002 [
1]; the GINA guideline was applied in the asthma care program under the Universal Coverage Scheme (UCS) of Thailand to improve the accessibility to health care service and quality of care for asthma patients.
Initially, the asthma care program called the “Easy Asthma Clinic” was established in field-testing areas of Thailand in 2004. It covered district hospitals in which the asthma care teams consisted of general practitioners, nurses, and pharmacists. In 2009, the program was expanded to a nationwide scale involving more than 900 hospitals with 99,535 asthma patients registered with 548,583 visits [
8]. In 2011, the program covered free-of-charge inhaled long-acting B2 agonists (LABAs) in combination with corticosteroids. In 2014, the program was integrated into the Rational Drug Use Hospital (RDU) project, which aimed to raise awareness among health personnel and patients [
8]. Although health insurance and asthma care programs have been implemented, national monitoring was performed for the health effects on asthma patients, particularly in children and young adults who were affected the most. Therefore, this study aimed to evaluate the effects of the asthma care program available under the UCS on asthma admissions per 100,000 population, variation in regional and seasonal asthma admissions, readmissions within 28 days, and the asthma-specific fatality rate of asthma patients aged 0–4, 5–14, 15–19, and 20–29 in the periods of 2009–2011, 2011–2014, and 2014–2016, compared with the 2007–2009 period as the baseline in Thailand.
2. Materials and Methods
2.1. Study Design and Setting
A retrospective study was conducted in Thailand in January 2018–June 2019. The proposal was approved by the Ethics Research Committee of Institutional Review Board of the National Center of Global Health and Medicine, Japan, and the Institute Ethics Committee of Faculty of Medicine, Prince of Songkla University, Thailand (REC.62-025-18-1). The de-identified data were obtained under the approval of the National Health Security Office (NHSO), Thailand, which is the public organization that responds to the UCS.
2.2. Data Sources and Management
Two sources of databases from the NHSO, including the UCS register and in-patient databases under the UCS for asthma patients, from the fiscal year 2007 (starting in October 2007) to the fiscal year 2016 (ending in September 2016), were retrieved based on the International Classification of Diseases-10 using the principal diagnosis (pdx) of J45 and J46 (J45: asthma, J45.0: predominantly allergic asthma, J45.1: non-allergic asthma, J45.2: bronchial hyperresponsiveness, J45.8: mixed asthma, J45.9: asthma, unspecified, J46: status asthmatics). All data of asthma patients aged 0–29 years were encrypted using a personal identification number by the staff of the NHSO before providing the data to the researchers for analysis. The data from two databases were verified and cleaned for mismatched and missing data. The asthma patients were categorized into four age groups: 0–4, 5–14, 15–19, and 20–29 years. Given the different implementations of service delivery in asthma care programs in 2009, 2011, and 2014, four time periods of health effect assessment were classified as the fiscal periods of 2009–2011 (easily accessible asthma clinics in most district hospitals), 2011–2014 (free treatment of inhaled LABAs in combination with corticosteroids for asthma), and 2014–2016 (integration of asthma care with the RDU project, which aimed to raise awareness among health personnel and patients), respectively. The data during the fiscal year of 2007–2008 were considered as the baseline rate. The definition of the year period in this study was the fiscal year starting from October to September of each year.
2.3. Data Analysis
The data were analyzed using the STATA program version 14 (StataCorp, College Station, TX, USA). The outcome measures were asthma admissions per 100,000 population, regional and seasonal variation in hospital admission rates, readmission rates within 28 days, and case fatality rates of asthma from 2007 to 2016. Hospital admissions per 100,000 population were calculated by dividing the number of asthma admissions with the total population registered in the UCS in the same age groups and periods and then multiplying the result by 100,000. Regional variations in hospital admissions were analyzed and presented in the geographic map of Thailand, and seasonal variations were calculated in months rather than seasons because the seasons in Thailand are heterogeneous; thus, reflecting the same seasons across health regions was difficult. Readmissions within 28 days were calculated by dividing the number of readmissions within 28 days with the number of hospital admissions multiplied by 100. Case fatality rates were calculated by dividing the number of deaths from asthma in a hospital with the number of admissions multiplied by 100. The differences in asthma outcomes of patients aged 0–4, 5–14, 15–19, and 20–29 years in the different periods of 2009–2011, 2011–2014, and 2014–2016 compared with the results for the period of 2007–2009 were analyzed using one-way analysis of variance. A p value less than 0.05 was considered significant.
4. Discussion
The asthma care program, which was implemented at a nationwide level in Thailand, improved the accessibility to health care services and the quality of care for asthma patients under the UCS organized by the NHSO. The positive health effect of the asthma care program was not only on hospital admissions per 100,000 population but also on readmission rates and asthma-specific fatality rates over the time of the policy changes. Asthma contributed 0.4% to all hospital admissions, and the hospital admissions per 100,000 population continuously decreased. High hospital admission rates were observed during rainy seasons and in the south of Thailand. The hospital admission rate was the highest in patients aged 0–4 years, but the readmission rate within 28 days and case fatality rate were high in patients aged 20–29 years. The hospital admissions per 100,000 population in children aged 0–4 years decreased from 470.8 to 288.1 per 100,000 population between 2010 and 2014.
The findings of our study were supported by the relevant beneficiaries of asthma treatment using the GINA guidelines at district-level hospitals and well-trained asthma care teams. The medical teams consisted of general practitioners, nurses, and pharmacists. The reimbursement for LABAs in combination with corticosteroids and reimbursed expenses of medical care for hospitals from 2010 to 2012 showed a reduction in hospitalization in 2011 [
9]. However, pediatric patients aged more than 5 years were controlled with a controller dose of ICS with LABAs. In addition, the use of LABAs in patients in aged 0–4 years was limited for safety. In addition, the declining trend in asthma admission rates was consistent with the information in the Global Asthma Report, which showed that the asthma admission rates of 30 European countries declined from 2001 to 2015. The asthma admission rate in Latvia was 148 per 100,000 population, decreasing by 3.12% per year. Similarly, children in Kenya showed the highest incident of asthma between 1995 and 2001. The International Study of Asthma and Allergies in Childhood showed that the prevalence of asthma in children aged 13–14 years increased from 10.4 to 13.8% in Eldoret and from 17.1 to 18.0% in Nairobi [
3]. Asthma was one of main causes of hospitalization in children aged less than 5 years in our study, the same as the finding of a previous study, mostly in low- and middle-income countries (LMICs) [
10]. The National Health Interview Survey data in the USA revealed that 47.2% of children under 5 years of age experienced asthma attacks in 2019 [
11]. In addition, the percentage of children with asthma declined significantly from 2001 to 2016 in the United States [
12]. In contrast, Dan Xu and team reported that asthma in children 6 years and older experienced more triggers than children 5 years and younger in Hangzhou. These triggers included exercise, emotional changes, house dust, pollen, renovation works at home, mosquito-repellent incense, and pets [
13].
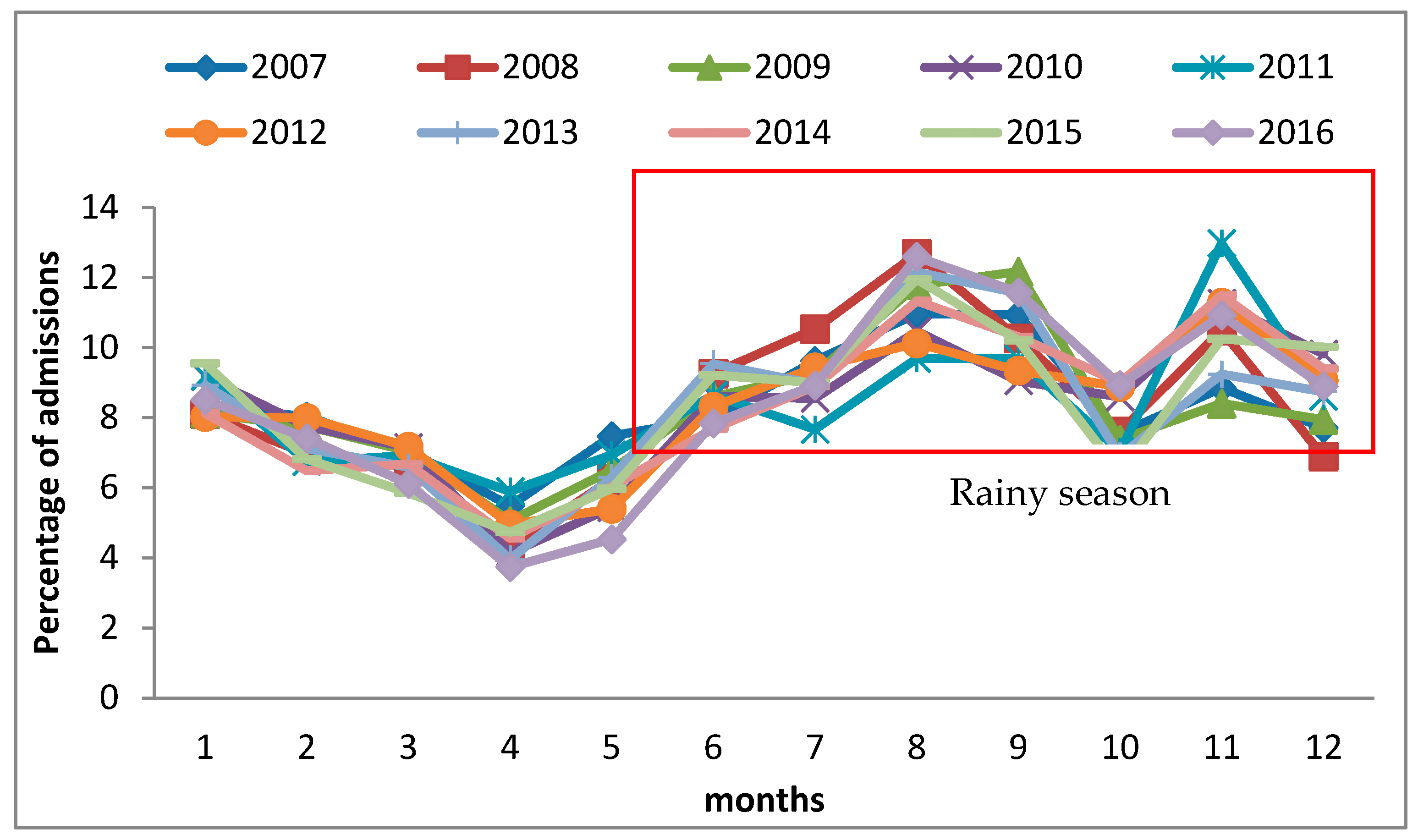
Hospital admission rates were the highest in the south of Thailand compared with those in other health regions. The rainy season there mostly occurred for 6–8 months per year, specifically from May/June to December. This season is caused by cold air, which created a relatively stable bad weather front over the southern area for several months. Considering the seasonal variation of asthma in Thailand, the greatest proportion of total asthma-related hospital admissions occurred in August, which was also part of the rainy season. This condition led to the highest hospitalization in these health regions. In the rainy season, there are various viruses and bacteria in the environment, which is reflected in an increase in viral infection. Outbreaks of cold and flu relate to high asthma hospitalizations in this season. The seasonal patterns were valuable for asthma patient management and can be used to alert patients of the increased risk in different seasons. Asthma usually presents symptoms during the rainy season. The changing weather moisture, which causes mold, is the main cause of acute asthma. This condition was associated with the Children’s Hospital of Michigan’s observation that with as little as a 10% rise in humidity, an increase in hospital visits for asthma occurred [
14]. The effect of meteorological factors on hospitalization in adults revealed that temperature was the only factor associated with asthma hospitalization or emergency department visits. Temperature and relative humidity were associated with hospitalization in six studies (37%). Thunderstorms were a possible factor associated with asthma hospitalization in adults in four studies (25%) [
15]. The treatment for asthma in the emergency department of the River State University Teaching Hospital, Port Harcourt, Nigeria, was more frequent in the rainy season (April–September) at 63.9%, with a peak in May [
16].
In our study, the readmission rate within 28 days was 3.8–8.7%, with the highest value observed in patients aged 20–29 years, whereas the hospital admission rate was the highest in those who were aged 1–4 years. However, various factors were used to describe the high readmission rate in patients aged 20–29 years. Such a condition might have been caused by complications, co-morbid disease conditions, or other factors. Continuing research efforts should be exerted to find proof to support these assumptions. About 15–50% of pediatric patients were readmitted. The risk factors associated with asthma readmission in the USA include being of African American descent, public or lack of insurance, previous hospital admission, and complex chronic comorbidity [
4]. In the USA, the hospitalization readmission rate for children with asthma was more than 40%. The readmission rate within 30 days was 2.5% [
5]. From 2009 to 2013, asthma admissions in the USA totaled 1,220,047. The readmission rate within 30 days was more than 5% [
17]. Among children who were hospitalized for asthma, around 20% were readmitted the next year. The readmission rate was 5.7 to 9.1% within three months. The readmission rate reduced when families received comprehensive education before discharge. In addition, the potential prevention of asthma by primary care reduced the problems [
18].
The case fatality rates in this study decreased over 10 years, accounting for 0.08% in 2008 and 0.04% in 2016, respectively. The highest rates were observed in patients aged 20–29 years. The age-standardized asthma mortality rate calculated by the GAN was 3% on average among asthma patients aged from 5 to 34 years in 2015. Thailand had the fifth highest mortality rate, according to World Bank 2014, among LMICs in terms of age-standardized results for 2011–2015. The Global Asthma Report also suggested that health authorities in all countries should report the rates of asthma deaths in children to monitor the progress in asthma care and provide an early warning of epidemics of fatal asthma [
3]. Similarly, the death rate for asthma decreased from 15 per million to 10 per million in 2001 to 2016. The highest death rate was observed in the elderly [
7]. However, the mortality of children and young adult patients were different in terms of the SES or LLC [
6]. On the other hand, aside from the asthma treatment policy resulting in hospital-related reduction in hospitalization, other effects might have occurred.
Our study supports the availability and accessibility of quality care for asthma in children and young adults as important advocacy and policy to ensure the improvement of the health and wellbeing of the population. However, several limitations were noted. First, this study was the secondary analysis of existing databases; therefore, some potential factors were not retrieved; for example, confounding effects could not be avoided. Second, the decreased hospital admissions for asthma patients may also be associated with other factors. However, the UCS covered almost all the population in Thailand, supporting the accessibility of seeking care at primary care units and outpatient care that may be related to preventable or avoidable hospitalization. Third, emergency admissions could not be extracted from the databases used. Finally, the policy of the asthma care program was implemented in only 75% of all hospitals, whereas the inpatient data of all hospitals were analyzed.


 ,
, 



{kind=link}
{kind=link}
{kind=link}