
Healthcare Utilization and Adherence to Treatment Recommendations among Children with Type 1 Diabetes in Poland during the COVID-19 Pandemic



Abstract
:1. Introduction
1.1. T1D in Poland
1.2. SARS-CoV-2 Pandemic in Poland—Effect on the Healthcare System
2. Materials and Methods
2.1. Study Design
2.2. Source of Data
2.3. Scope of Data Analysis
- The number of patients (persons under 19 years of age with diagnosis E.10 according to ICD-10) including (NHF data):
- The number of patients at the end of the accounting/reporting period.
- The number of new patients/diagnoses in the accounting/reporting period.
- The number of persons under 19 years of age:
- In the general population (CSO data);
- Beneficiaries of healthcare services provided under the universal health insurance scheme (NHF data).
- The number of patients from pt. 1 above who during the accounting/reporting year were provided with (NHF data):
- One diabetes consultation;
- Two diabetes consultations;
- Three diabetes consultations;
- Four diabetes consultations;
- Healthcare services associated with hospitalization in the diabetic ward.
- The number of persons (separately from points 1 and 2 above) who during the accounting/reporting year were provided with specific healthcare services (NHF data):
- Ophthalmological consultation (examination for retinopathy);
- Neurological consultation (diagnosis of neuropathy);
- Mental health advice (psychological/psychiatric care).
3. Results
3.1. Population of Children with T1D
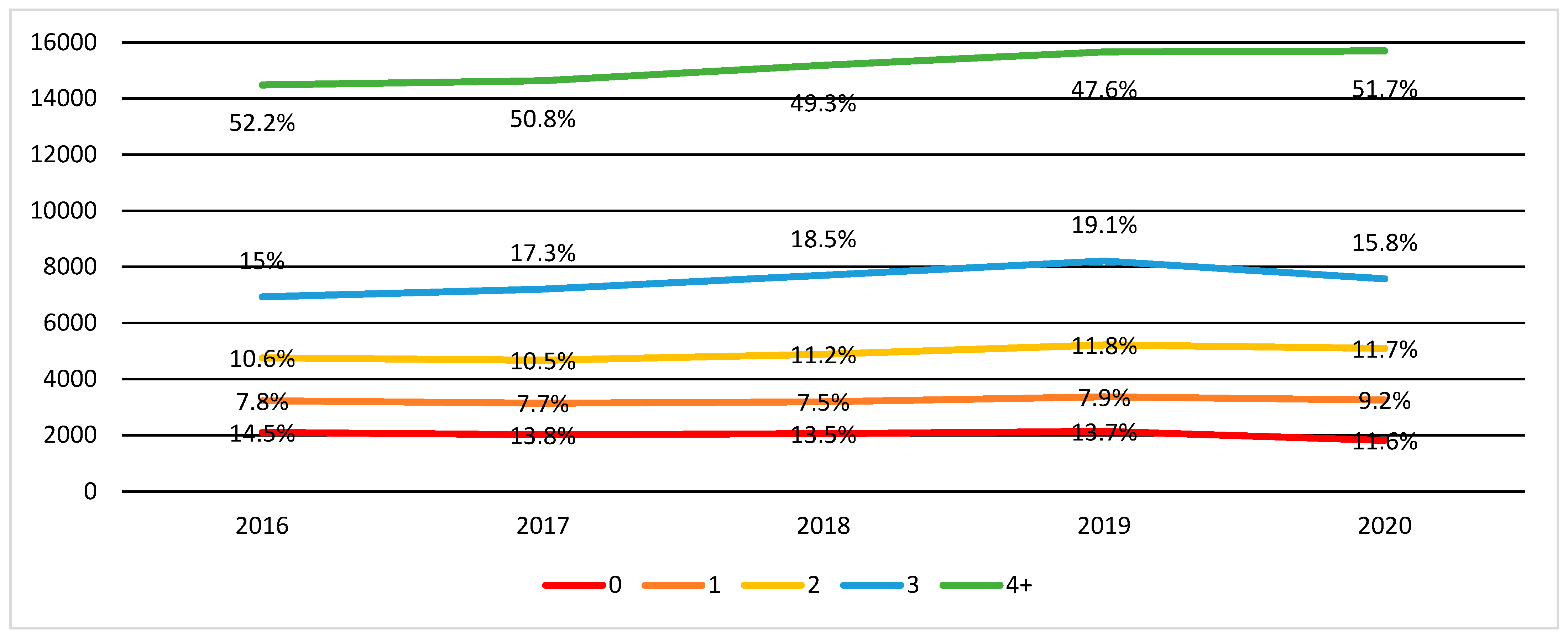
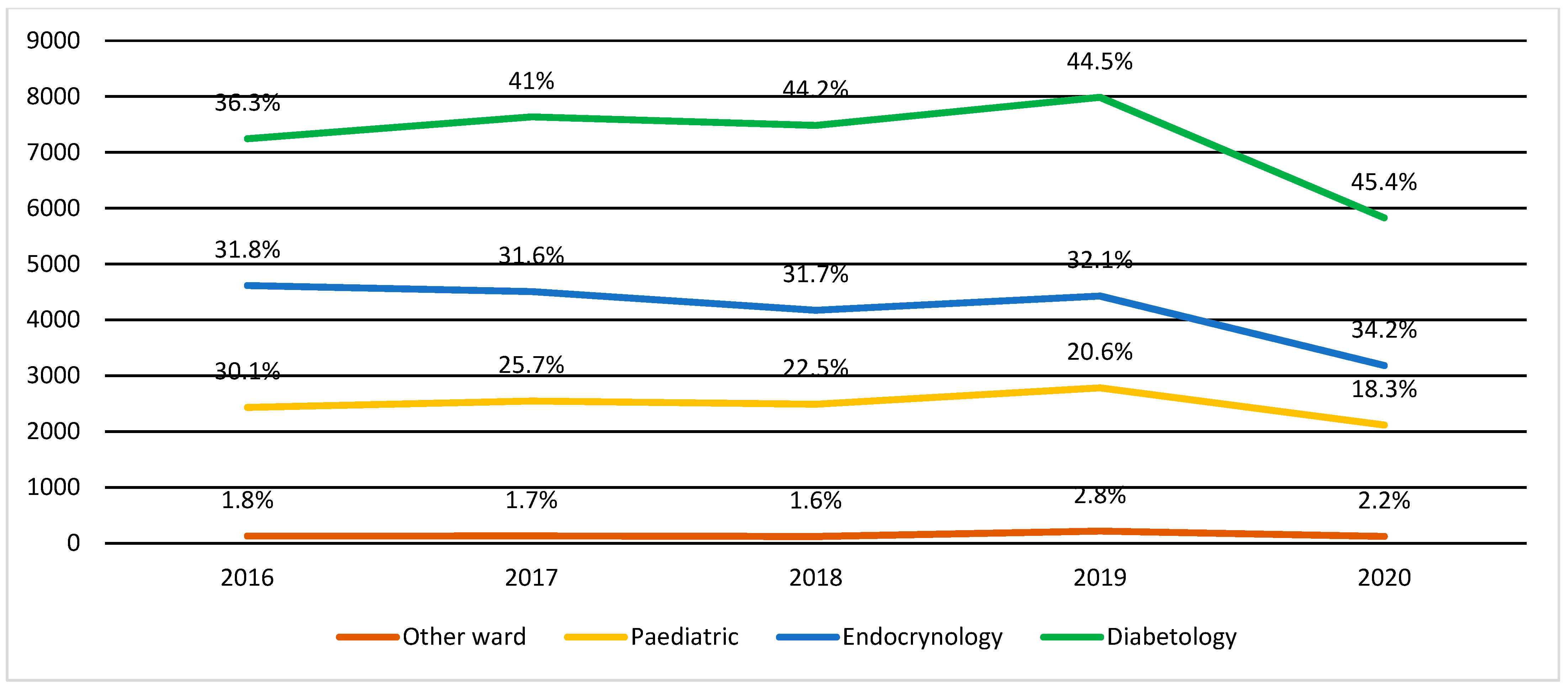
3.2. Out- and Inpatient Care for Children with T1D
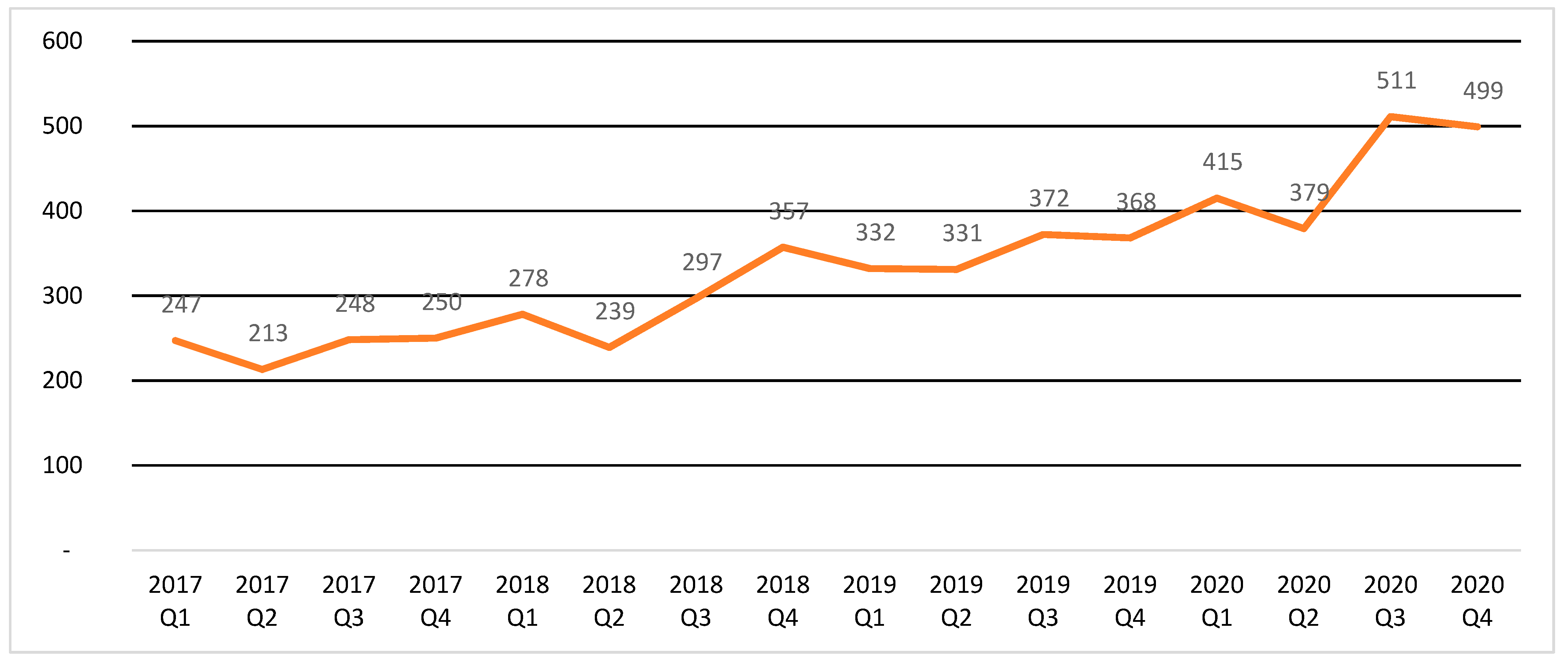
3.3. DKA
3.4. Utilization of Other Health Services
4. Discussion
4.1. Outpatient Care Utilization
4.2. Inpatient Care Utilization
4.3. COVID-19 Pandemic’s Influence on Adherence and Healthcare Utilization
4.4. Practical Implications
4.5. Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Knip, M.; Siljander, H. Autoimmune mechanisms in type 1 diabetes. Autoimmun. Rev. 2008, 7, 550–557. [Google Scholar] [CrossRef] [PubMed]
- Banday, M.Z.; Sameer, A.S.; Nissar, S. Pathophysiology of diabetes: An overview. Avicenna J. Med. 2020, 10, 174–188. [Google Scholar] [CrossRef] [PubMed]
- ADA American Diabetes Association. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes—2021. Diabetes Care 2021, 44 (Suppl. 1), S15–S33. [Google Scholar] [CrossRef] [PubMed]
- Zimmet, P.Z. Diabetes and its drivers: The largest epidemic in human history? Clin. Diabetes Endocrinol. 2017, 3, 1. [Google Scholar] [CrossRef] [Green Version]
- Papatheodorou, K.; Banach, M.; Bekiari, E.; Rizzo, M.; Edmonds, M. Complications of Diabetes 2017. J. Diabetes Res. 2018, 2018, 3086167. [Google Scholar] [CrossRef]
- Lopez-Bastida, J.; López-Siguero, J.P.; Oliva-Moreno, J.; Perez-Nieves, M.; Villoro, R.; Dilla, T.; Vázquez, L.A. Social economic costs of type 1 diabetes mellitus in pediatric patients in Spain: CHRYSTAL observational study. Diabetes Res. Clin. Pract. 2017, 127, 59–69. [Google Scholar] [CrossRef] [Green Version]
- O’Connell, J.M.; Manson, S. Understanding the Economic Costs of Diabetes and Prediabetes and What We May Learn About Reducing the Health and Economic Burden of These Conditions. Diabetes Care 2019, 42, 1609–1611. [Google Scholar] [CrossRef] [Green Version]
- Van den Boom, L.; Karges, B.; Auzanneau, M.; Rami-Merhar, B.; Lilienthal, E.; von Sengbusch, S.; Datz, N.; Schröder, C.; Kapellen, T.; Laimer, M.; et al. Temporal Trends and Contemporary Use of Insulin Pump Therapy and Glucose Monitoring Among Children, Adolescents, and Adults With Type 1 Diabetes Between 1995 and 2017. Diabetes Care 2019, 42, 2050–2056. [Google Scholar] [CrossRef]
- Araszkiewicz, A.; Bandurska-Stankiewicz, E.; Budzyński, A.; Cypryk, K.; Czech, A.; Czupryniak, L.; Zozulińska-Ziółkiewicz, D. Zalecenia kliniczne dotyczące postępowania u chorych na cukrzycę 2020—Stanowisko PTD. Diabetol. Prakt. 2020, 6, 1–106. [Google Scholar]
- Lee, J.M.; Sundaram, V.; Sanders, L.; Chamberlain, L.; Wise, P. Health care utilization and costs of publicly-insured children with diabetes in California. J. Paediatr. 2015, 167, 449–454. [Google Scholar] [CrossRef]
- Kaufman, F.R.; Halvorson, M.; Carpenter, S. Association between diabetes control and visits to a multidisciplinary pediatric diabetes clinic. Pediatrics 1999, 103, 948–951. [Google Scholar] [CrossRef]
- Sandford, K.; Rivers, A.S. Treatment Adherence Perception Questionnaire: Assessing patient perceptions regarding their adherence to medical treatment plans. Psychol. Assess. 2020, 32, 227–238. [Google Scholar] [CrossRef] [PubMed]
- Fink, G.; Tediosi, F.; Felder, S. Burden of COVID-19 restrictions: National, regional and global estimates. EClinicalMedicine 2022, 45, 101305. [Google Scholar] [CrossRef] [PubMed]
- NFZ o Zdrowiu. Cukrzyca (NFH on Health. Diabetes). Available online: https://ezdrowie.gov.pl/portal/home/zdrowe-dane/raporty/nfz-o-zdrowiu-cukrzyca (accessed on 20 December 2021).
- Nieszporska, S. Priorities in the Polish health care system. Eur. J. Health Econ. 2017, 18, 1–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ubezpieczenie NFZ (NFH Health Insurance Coverage). Available online: https://www.nfz.gov.pl/dla-pacjenta/ubezpieczenia-w-nfz/ (accessed on 20 December 2021).
- Rozporządzenie Ministra Zdrowia z dnia 6 listopadfa 2013 r. w sprawie świadczeń gwarantowanych z zakresu ambulatoryjnej opieki specjalistycznej (Regulation of the Minister of Health of 6 November 2013 on Guaranteed Health Services in the Field of Specialist Outpatient Care). Available online: https://isap.sejm.gov.pl/isap.nsf/DocDetails.xsp?id=WDU20160000357 (accessed on 20 December 2021).
- OECD/European Union. Health at a Glance: Europe 2020: State of Health in the EU Cycle; OECD Publishing: Paris, France, 2020. [Google Scholar]
- Polskie Towarzystwo Diabetologiczne. Nowy Koronawirus SARS-CoV-2, COVID-19 a Cukrzyca. 2020. Available online: https://cukrzyca.info.pl/aktualnosci/nowy_koronawirus_sars_cov_2_covid_19_a_cukrzyca (accessed on 20 December 2021).
- Kludacz-Alessandri, M.; Hawrysz, L.; Korneta, P.; Gierszewska, G.; Pomaranik, W.; Walczak, R. The impact of medical teleconsultations on general practitioner-patient communication during COVID-19: A case study from Poland. PLoS ONE 2021, 16, e0254960. [Google Scholar] [CrossRef]
- Czeisler, M.É.; Marynak, K.; Clarke, K.E.; Salah, Z.; Shakya, I.; Thierry, J.M.; Howard, M.E. Delay or avoidance of medical care because of COVID-19—Related Concerns—United States. Morb. Mortal. Wkly. Rep. 2020, 69, 1250–1257. [Google Scholar] [CrossRef]
- Dżygało, K.; Nowaczyk, J.; Szwilling, A.; Kowalska, A. Increased frequency of severe diabetic ketoacidosis at type 1 diabetes onset among children during COVID-19 pandemic lockdown: An observational cohort study. Pediatric Endocrinol. Diabetes Metab. 2020, 26, 167–175. [Google Scholar] [CrossRef]
- Kamrath, C.; Mönkemöller, K.; Biester, T.; Rohrer, T.R.; Warncke, K.; Hammersen, J.; Holl, R.W. Ketoacidosis in children and adolescents with newly diagnosed type 1 diabetes during the COVID-19 pandemic in Germany. JAMA 2020, 324, 801–804. [Google Scholar] [CrossRef]
- Vellanki, P.; Umpierrez, G.E. Diabetic ketoacidosis risk during the COVID-19 pandemic. Lancet Diabetes Endocrinol. 2021, 9, 643–644. [Google Scholar] [CrossRef]
- McGlacken-Byrne, S.M.; Drew, S.E.; Turner, K.; Peters, C.; Amin, R. The SARS-CoV-2 pandemic is associated with increased severity of presentation of childhood-onset type 1 diabetes mellitus: A multi-centre study of the first COVID-19 wave. Diabet. Med. 2021, 38, e14640. [Google Scholar] [CrossRef]
- Myśliwiec, A.; Jarosz-Chobot, P.; Małgorzata Myśliwiec, M. Paediatric diabetes care: Inpatient care in the Maps of Health Needs of Poland in 2014. Clin. Diabetol. 2018, 7, 259–271. [Google Scholar] [CrossRef]
- Mayer-Davis, E.J.; Kahkoska, A.R.; Jefferies, C.; Dabelea, D.; Balde, N.; Gong, C.X.; Craig, M.E. ISPAD Clinical Practice Consensus Guidelines 2018: Definition, epidemiology, and classification of diabetes in children and adolescents. Pediatric Diabetes 2018, 19, 7. [Google Scholar] [CrossRef] [PubMed]
- Noczyńska, A. Edukacja w Cukrzycy Typu 1; Via Medica: Gdańsk, Poland, 2015. [Google Scholar]
- Datye, K.A.; Moore, D.J.; Russell, W.E.; Jaser, S.S. A review of adolescent adherence in type 1 diabetes and the untapped potential of diabetes providers to improve outcomes. Curr. Diabetes Rep. 2015, 15, 51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Phelan, H.; Clapin, H.; Bruns, L.; Cameron, F.J.; Cotterill, A.M.; Couper, J.J.; Craig, M.E. The Australasian Diabetes Data Network: First national audit of children and adolescents with type 1 diabetes. Med. J. Aust. 2017, 206, 121–125. [Google Scholar] [CrossRef]
- Svoren, B.M.; Butler, D.; Levine, B.S.; Anderson, B.J.; Laffel, L. Reducing acute adverse outcomes in youths with type 1 diabetes: A randomized, controlled trial. Pediatrics 2003, 112, 914–922. [Google Scholar] [CrossRef]
- Grover, S.; Bhadada, S.; Kate, N.; Sarkar, S.; Bhansali, A.; Avasthi, A.; Goel, R. Coping and caregiving experience of parents of children and adolescents with type-1 diabetes: An exploratory study. Perspect. Clin. Res. 2016, 7, 32. [Google Scholar] [CrossRef]
- Grudziąż-Sękowska, J.; Zamarlik, M.; Sękowski, K. Assessment of Selected Aspects of the Quality of Life of Children with Type 1 Diabetes Mellitus in Poland. Int. J. Environ. Res. Public Health 2021, 18, 2107. [Google Scholar] [CrossRef]
- Simm, P.J.; Wong, N.; Fraser, L.; Kearney, J.; Fenton, J.; Jachno, K.; Cameron, F.J. Geography does not limit optimal diabetes care: Use of a tertiary centre model of care in an outreach service for type 1 diabetes mellitus. J. Paediatr. Child Health 2014, 50, 471–475. [Google Scholar] [CrossRef]
- Surowiec, P.; Matejko, B.; Kopka, M.; Filemonowicz-Skoczek, A.; Klupa, T.; Cyganek, K.; Malecki, M.T. Low prevalence of diabetic retinopathy in patients with long-term type 1 diabetes and current good glycemic control-one-center retrospective assessment. Endocrine 2022, 75, 427–436. [Google Scholar] [CrossRef]
- Gibbons, C.H. Treatment-induced neuropathy of diabetes—Long term implications in type 1 diabetes. J. Diabetes Its Complicat. 2017, 31, 715–720. [Google Scholar] [CrossRef]
- Wang, S.Y.; Andrews, C.A.; Gardner, T.W.; Wood, M.; Singer, K.; Stein, J.D. Ophthalmic screening patterns among youths with diabetes enrolled in a large US managed care network. JAMA Ophthalmol. 2017, 135, 432–438. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martín, D.E.A.; Martín, M.B.R.; Gómez, M.Á.Á.; Valverde, R.Y.; Martín-Frías, M.; Blanco, M.A.; Castellanos, R.B. Impact of diabetes education on type 1 diabetes mellitus control in children. Endocrinol. Nutr. 2016, 63, 536–542. [Google Scholar] [CrossRef] [PubMed]
- Powell, P.W.; Chen, R.; Kumar, A.; Streisand, R.; Holmes, C.S. Sociodemographic effects on biological, disease care, and diabetes knowledge factors in youth with type 1 diabetes. J. Child Health Care 2013, 17, 174–185. [Google Scholar] [CrossRef] [PubMed]
- Usher-Smith, J.A.; Thompson, M.; Ercole, A.; Walter, F.M. Variation between countries in the frequency of diabetic ketoacidosis at first presentation of type 1 diabetes in children: A systematic review. Diabetologia 2012, 55, 2878–2894. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kalla Vyas, A.; Oud, L. Temporal patterns of hospitalizations for diabetic ketoacidosis in children and adolescents. PLoS ONE 2021, 16, e0245012. [Google Scholar] [CrossRef] [PubMed]
- Henriksen, O.M.; Røder, M.E.; Prahl, J.B.; Svendsen, O.L. Diabetic ketoacidosis in Denmark: Incidence and mortality estimated from public health registries. Diabetes Res. Clin. Pract. 2007, 76, 51–56. [Google Scholar] [CrossRef]
- Ramphul, K.; Joynauth, J. An Update on the Incidence and Burden of Diabetic Ketoacidosis in the US. Diabetes Care 2020, 43, e196–e197. [Google Scholar] [CrossRef]
- Núñez, A.; Sreeganga, S.D.; Ramaprasad, A. Access to Healthcare during COVID-19. Int. J. Environ. Res. Public Health 2021, 18, 2980. [Google Scholar] [CrossRef]
- Barchetta, I.; Cimini, F.A.; Bertoccini, L.; Ceccarelli, V.; Spaccarotella, M.; Baroni, M.G.; Cavallo, M.G. Effects of work status changes and perceived stress on glycaemic control in individuals with type 1 diabetes during COVID-19 lockdown in Italy. Diabetes Res. Clin. Pract. 2020, 170, 108513. [Google Scholar] [CrossRef]
- Ruissen, M.M.; Regeer, H.; Landstra, C.P.; Schroijen, M.; Jazet, I.; Nijhoff, M.F.; de Koning, E.J. Increased stress, weight gain and less exercise in relation to glycemic control in people with type 1 and type 2 diabetes during the COVID-19 pandemic. BMJ Open Diabetes Res. Care 2021, 9, e002035. [Google Scholar] [CrossRef]
- Beliard, K.; Ebekozien, O.; Demeterco-Berggren, C.; Alonso, G.T.; Gallagher, M.P.; Clements, M.; Rapaport, R. Increased DKA at presentation among newly diagnosed type 1 diabetes patients with or without COVID-19: Data from a multi-site surveillance registry. J. Diabetes 2021, 13, 270–272. [Google Scholar] [CrossRef] [PubMed]
- Rabbone, I.; Schiaffini, R.; Cherubini, V.; Maffeis, C.; Scaramuzza, A. Has COVID-19 delayed the diagnosis and worsened the presentation of type 1 diabetes in children? Diabetes Care 2020, 43, 2870–2872. [Google Scholar] [CrossRef] [PubMed]
- Anderzén, J.; Samuelsson, U.; Gudbjörnsdottir, S.; Hanberger, L.; Åkesson, K. Teenagers with poor metabolic control already have a higher risk of microvascular complications as young adults. J. Diabetes Its Complicat. 2016, 30, 533–536. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mesa, A.; Viñals, C.; Pueyo, I.; Roca, D.; Vidal, M.; Giménez, M.; Conget, I. The impact of strict COVID-19 lockdown in Spain on glycemic profiles in patients with type 1 Diabetes prone to hypoglycemia using standalone continuous glucose monitoring. Diabetes Res. Clin. Pract. 2020, 167, 108354. [Google Scholar] [CrossRef] [PubMed]
- Fernández, E.; Cortazar, A.; Bellido, V. Impact of COVID-19 lockdown on glycemic control in patients with type 1 diabetes. Diabetes Res. Clin. Pract. 2020, 166, 108348. [Google Scholar] [CrossRef]
- Bonora, B.M.; Boscari, F.; Avogaro, A.; Bruttomesso, D.; Fadini, G.P. Glycaemic control among people with type 1 diabetes during lockdown for the SARS-CoV-2 outbreak in Italy. Diabetes Ther. 2020, 11, 1369–1379. [Google Scholar] [CrossRef]
- Parise, M.; Tartaglione, L.; Cutruzzolà, A.; Maiorino, M.I.; Esposito, K.; Pitocco, D.; Irace, C. Teleassistance for patients with type 1 diabetes during the COVID-19 pandemic: Results of a pilot study. J. Med. Internet Res. 2021, 23, e24552. [Google Scholar] [CrossRef]
- Ludvigsson, J. Effect of COVID-19 pandemic on the treatment of Type 1 diabetes in children. Acta Paediatr. 2021, 110, 933–934. [Google Scholar] [CrossRef]
- Papautsky, E.L.; Rice, D.R.; Ghoneima, H.; McKowen, A.L.W.; Anderson, N.; Wootton, A.R.; Veldhuis, C. Characterizing health care delays and interruptions in the United States during the COVID-19 pandemic: An internet-based, cross-sectional survey study. J. Med. Internet Res. 2021, 23, e25446. [Google Scholar] [CrossRef]
- Schiller, T.; Zornitzki, T.; Ostrovsky, V.; Sapojnik, D.; Cohen, L.; Kunyavski, T.; Kirzhner, A. Following the COVID-19 Experience, Many Patients with Type 1 Diabetes Wish to Use Telemedicine in a Hybrid Format. Int. J. Environ. Res. Public Health 2021, 18, 11309. [Google Scholar] [CrossRef]
- Katzow, M.W.; Steinway, C.; Jan, S. Telemedicine and health disparities during COVID-19. Pediatrics 2020, 146, e20201586. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Year | The General Population (Pop.) < 19 Years Old | Public Health System Patients < 19 Years Old | Public Health System Patients with T1D (%) | |
|---|---|---|---|---|
| No. | % of Pop. | % of All Patients < 19 Years Old | ||
| 2016 | 7,286,480 | 7,070,670 | 97.0% | 0.2% |
| 2017 | 7,299,996 | 7,088,663 | 97.1% | 0.2% |
| 2018 | 7,311,538 | 7,085,435 | 96.9% | 0.2% |
| 2019 | 7,314,617 | 7,056,062 | 96.5% | 0.2% |
| 2020 | 7,307,098 | 6,513,836 | 89.1% | 0.2% |
| Year | Total Number of T1D Cases at the End of Year 1 | Newly Diagnosed Cases— Nominal (Yearly) 2 | Newly Diagnosed Cases—Per 100 Thousand Population < 19 Years Old (Yearly) 2 |
|---|---|---|---|
| 2016 | 14,288 | 1228 | 16.85 |
| 2017 | 14,634 | 1407 | 19.27 |
| 2018 | 15,182 | 1486 | 20.32 |
| 2019 | 15,663 | 1346 | 18.40 |
| 2020 | 15,693 | 1135 | 15.53 |
| Health Service Used/Yearly | 2016 | 2017 | 2018 | 2019 | 2020 |
|---|---|---|---|---|---|
| Number of Patients Diagnosed with E10 (Absolute Number and Percentage from the Population of T1D Patients < 19 Years of Age at that Time) | |||||
| 1 diabetes consultation | 1107 | 1126 | 1137 | 1229 | 1441 |
| (7.7) | (7.7) | (7.5) | (7.8) | (9.2) | |
| 2 diabetes consultations | 1355 | 1531 | 1696 | 1849 | 1834 |
| (9.5) | (10.5) | (11.2) | (11.8) | (11.7) | |
| 3 diabetes consultations | 2170 | 2531 | 2810 | 2989 | 2480 |
| (15.2) | (17.3) | (18.5) | (19.1) | (15.8) | |
| 4 or more diabetes consultations | 7553 | 7429 | 7483 | 7455 | 8120 |
| (52.9) | (50.8) | (49.3) | (47.6) | (51.7) | |
| No consultations | 2103 | 2017 | 2056 | 2141 | 1818 |
| (14.7) | (13.8) | (13.5) | (13.7) | (11.6) | |
| Health Service Used/Yearly | 2016 | 2017 | 2018 | 2019 | 2020 |
|---|---|---|---|---|---|
| Number of Patients Diagnosed with E10 (Absolute Number and Percentage from the Population of T1D Patients < 19 Years of Age at that Time) | |||||
| Hospitalization for: | 6924 | 7270 | 7131 | 7595 | 5548 |
| (48.5) | (49.7) | (47.0) | (48.5) | (35.4) | |
| Diabetes care unit for children | 2629 | 3127 | 3308 | 3556 | 2644 |
| (18.4) | (21.4) | (21.8) | (22.7) | (16.8) | |
| Pediatric endocrinology ward | 2181 | 1960 | 1683 | 1645 | 1065 |
| (15.3) | (13.4) | (11.1) | (10.5) | (6.8) | |
| Pediatric ward | 2305 | 2415 | 2369 | 2564 | 1993 |
| (16.1) | (16.5) | (15.6) | (16.4) | (12.7) | |
| Other wards | 130 | 133 | 122 | 220 | 125 |
| (0.9) | (0.9) | (0.8) | (1.4) | (0.8) | |
| Number of patients diagnosed with ketoacidosis 1 | n/a | 860 | 1038 | 1151 | 1404 |
| (5.9) | (6.8) | (7.3) | (8.9) | ||
| (Diagnosis E10.1 according to ICD-10) 2 | n/a | n/a | n/a | 981 | 1153 |
| (6.3) | (7.3) | ||||
| Health Service Used/Yearly | 2016 | 2017 | 2018 | 2019 | 2020 |
|---|---|---|---|---|---|
| Total Number of Patients/Number of Patients with Diagnosis E10 (Absolute Number and Percentage from the General Population and the Population of T1D Patients < 19 Years of Age) | |||||
| Ophthalmological consultation with fundus examination | 4027/2 (0.055/0.014) | 4379/0 (0.060/0) | 4037/2 (0.055/0.015) | 4278/3 (0.058/0.019) | 3272/0 (0.045/0) |
| Neurological consultations | 176,319/35 (2.42/0.2450) | 171,533/42 (2.35/0.287) | 163,568/40 (2.237/0.263) | 156,102/45 (2.134/0.287) | 130,122/33 (1.781/0.210) |
| Mental healthcare services: | |||||
| Medical diagnostic consultation | 50,750/3 (0.696/0.021) | 49,966/3 (0.684/0.021) | 49,393/9 (0.676/0.059) | 51,339/8 (0.702/0.051) | 40,224/9 (0.550/0.057) |
| Medical therapeutic consultation | 51,042/5 (0.701/0.035) | 52,358/7 (0.717/0.048) | 53,292/7 (0.729/0.046) | 52,093/8 (0.712/0.51) | 51,419/14 (0.704/0.089) |
| Psychological diagnostic consultation | 26,382/2 (0.362/0.014) | 24,600/1 (0.337/0.007) | 23,068/4 (0.316/0.026) | 24,797/2 (0.339/0.013) | 18,196/3 (0.249/0.019) |
| Psychological therapeutic consultation | 28,107/0 (0.386/0) | 27,876/1 (0.382/0.007) | 27,215/2 (0.372/0.013) | 28,191/1 (0.385/0.006) | 27,840/2 (0.381/0.013) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grudziąż-Sękowska, J.; Sękowski, K.; Kobuszewski, B. Healthcare Utilization and Adherence to Treatment Recommendations among Children with Type 1 Diabetes in Poland during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2022, 19, 4798. https://doi.org/10.3390/ijerph19084798
Grudziąż-Sękowska J, Sękowski K, Kobuszewski B. Healthcare Utilization and Adherence to Treatment Recommendations among Children with Type 1 Diabetes in Poland during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2022; 19(8):4798. https://doi.org/10.3390/ijerph19084798
Chicago/Turabian StyleGrudziąż-Sękowska, Justyna, Kuba Sękowski, and Bartosz Kobuszewski. 2022. "Healthcare Utilization and Adherence to Treatment Recommendations among Children with Type 1 Diabetes in Poland during the COVID-19 Pandemic" International Journal of Environmental Research and Public Health 19, no. 8: 4798. https://doi.org/10.3390/ijerph19084798
APA StyleGrudziąż-Sękowska, J., Sękowski, K., & Kobuszewski, B. (2022). Healthcare Utilization and Adherence to Treatment Recommendations among Children with Type 1 Diabetes in Poland during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health, 19(8), 4798. https://doi.org/10.3390/ijerph19084798