
Gestational Diabetes Mellitus as an Effect Modifier of the Association of Gestational Weight Gain with Perinatal Outcomes: A Prospective Cohort Study in China

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Diagnosis of GDM
2.3. GWG and Covariates
2.4. Perinatal Outcomes
2.5. Statistical Analyses
3. Results
3.1. Characteristics of Study Participants
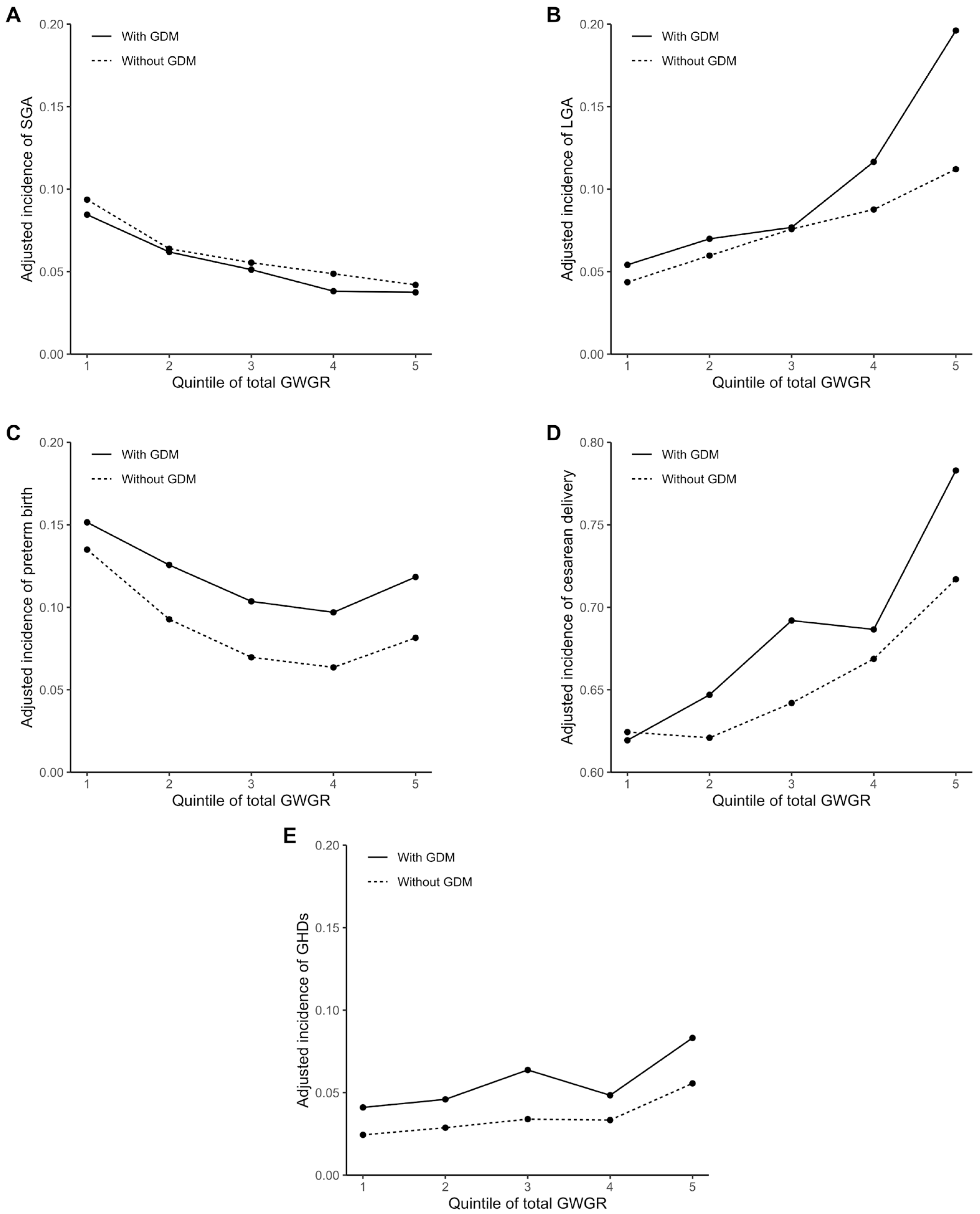
3.2. Incidences of Perinatal Outcomes with Total GWGR
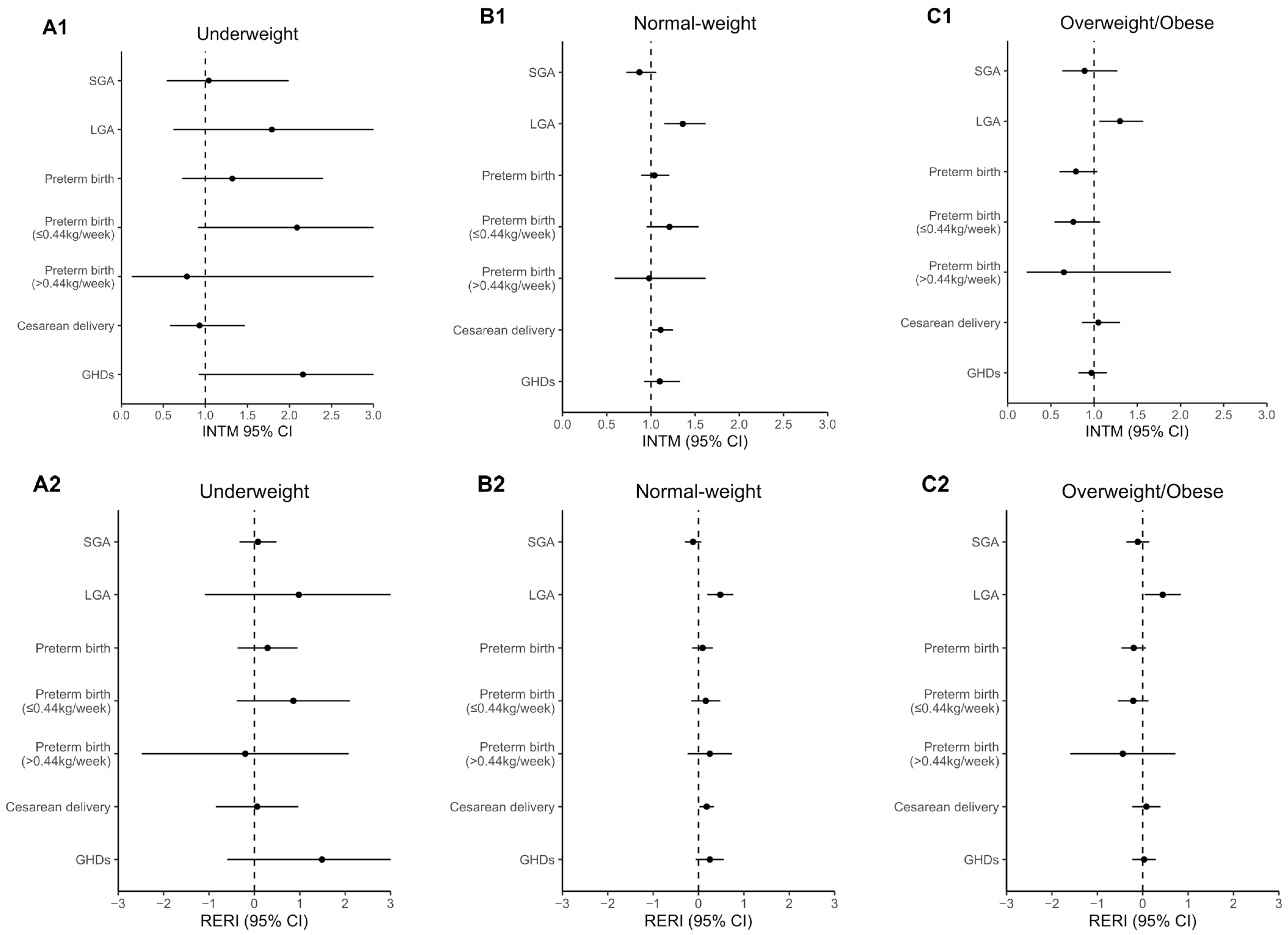
3.3. Modifying Effect of GDM on Association of Total GWGR with Perinatal Outcomes
3.4. Modifying Effect of GDM on Association of Trimester-Specific GWGR with Perinatal Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hod, M.; Kapur, A.; Sacks, D.A.; Hadar, E.; Agarwal, M.; Di Renzo, G.C.; Roura, L.C.; McIntyre, H.D.; Morris, J.L.; Divakar, H. The International Federation of Gynecology and Obstetrics (FIGO) initiative on gestational diabetes mellitus: A pragmatic guide for diagnosis, management, and care. Int. J. Gynaecol. Obs. 2015, 131, S173–S211. [Google Scholar] [CrossRef] [Green Version]
- Popova, P.; Castorino, K.; Grineva, E.N.; Kerr, D. Gestational diabetes mellitus diagnosis and treatment goals: Measurement and measures. Minerva Endocrinol. 2016, 41, 421–432. [Google Scholar]
- Cozma, M.-A.; Găman, M.-A.; Dobrică, E.-C.; Boroghină, S.C.; Iancu, M.A.; Crețoiu, S.M.; Simionescu, A.A. A glimpse at the size of the fetal liver—Is it connected with the evolution of gestational diabetes? Int. J. Mol. Sci. 2021, 22, 7866. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Zhang, X.; Zhou, M.; Juan, J.; Wang, X. Association of gestational diabetes mellitus with adverse pregnancy outcomes and its interaction with maternal age in Chinese urban women. J. Diabetes Res. 2021, 2021, e5516937. [Google Scholar] [CrossRef] [PubMed]
- Farzaneh, M.; Fatemeh-Sadat, H.-B.; Afsaneh, D.; Farzad, S.; Saeed, M.; Mihnea-Alexandru, G. Comparison of the key modifiable factors in the first 1000 days predicting subsequent overweight and obesity in pre-school children in Tehran: A case-control study. Br. J. Nutr. 2021, 1–9. [Google Scholar] [CrossRef]
- Vounzoulaki, E.; Khunti, K.; Abner, S.C.; Tan, B.K.; Davies, M.J.; Gillies, C.L. Progression to Type 2 diabetes in women with a known history of gestational diabetes: Systematic review and meta-analysis. BMJ 2020, 369, m1361. [Google Scholar] [CrossRef]
- Scholtens, D.M.; Kuang, A.; Lowe, L.P.; Hamilton, J.; Lawrence, J.M.; Lebenthal, Y.; Brickman, W.J.; Clayton, P.; Ma, R.C.; McCance, D.; et al. Hyperglycemia and Adverse Pregnancy Outcome Follow-up Study (HAPO FUS): Maternal glycemia and childhood glucose metabolism. Diabetes Care 2019, 42, 381–392. [Google Scholar] [CrossRef] [Green Version]
- IDF Diabetes Atlas, 9th ed. Available online: https://diabetesatlas.org/atlas/ninth-edition/ (accessed on 2 January 2022).
- Gao, C.; Sun, X.; Lu, L.; Liu, F.; Yuan, J. Prevalence of gestational diabetes mellitus in mainland China: A systematic review and meta-analysis. J. Diabetes Investig. 2019, 10, 154–162. [Google Scholar] [CrossRef]
- Qi, Y.; Sun, X.; Tan, J.; Zhang, G.; Chen, M.; Xiong, Y.; Chen, P.; Liu, C.; Zou, K.; Liu, X. Excessive Gestational Weight Gain in the First and Second Trimester Is a Risk Factor for Gestational Diabetes Mellitus among Women Pregnant with Singletons: A Repeated Measures Analysis. J. Diabetes Investig. 2020, 11, 1651–1660. [Google Scholar] [CrossRef]
- Lan, X.; Zhang, Y.; Dong, H.; Zhang, J.; Zhou, F.; Bao, Y.; Zhao, R.; Cai, C.; Bai, D.; Pang, X.; et al. Excessive gestational weight gain in the first trimester is associated with risk of gestational diabetes mellitus: A prospective study from Southwest China. Public Health Nutr. 2020, 23, 394–401. [Google Scholar] [CrossRef]
- Barnes, R.A.; Wong, T.; Ross, G.P.; Griffiths, M.M.; Smart, C.E.; Collins, C.E.; MacDonald-Wicks, L.; Flack, J.R. Excessive weight gain before and during gestational diabetes mellitus management: What is the impact? Diabetes Care 2020, 43, 74–81. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, K.M.; Yaktine, A.L. (Eds.) Weight Gain during Pregnancy: Reexamining the Guidelines; National Academies Press (US): Washington, DC, USA, 2009; ISBN 978-0-309-13113-1. [Google Scholar]
- Goldstein, R.F.; Abell, S.K.; Ranasinha, S.; Misso, M.; Boyle, J.A.; Black, M.H.; Li, N.; Hu, G.; Corrado, F.; Rode, L.; et al. Association of gestational weight gain with maternal and infant outcomes: A systematic review and meta-analysis. JAMA 2017, 317, 2207–2225. [Google Scholar] [CrossRef] [PubMed]
- Viecceli, C.; Remonti, L.R.; Hirakata, V.N.; Mastella, L.S.; Gnielka, V.; Oppermann, M.L.R.; Silveiro, S.P.; Reichelt, A.J. Weight gain adequacy and pregnancy outcomes in gestational diabetes: A meta-analysis. Obes. Rev. 2017, 18, 567–580. [Google Scholar] [CrossRef] [PubMed]
- Black, M.H.; Sacks, D.A.; Xiang, A.H.; Lawrence, J.M. The relative contribution of prepregnancy overweight and obesity, gestational weight gain, and IADPSG-defined gestational diabetes mellitus to fetal overgrowth. Diabetes Care 2013, 36, 56–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, L.; Zhang, J.; Sun, H.; Dong, H.; Li, R.; Cai, C.; Gao, Y.; Wu, C.; Lan, X.; Zeng, G. Association of gestational weight gain with cesarean section: A prospective birth cohort study in Southwest China. BMC Pregnancy Childbirth 2021, 21, 57. [Google Scholar] [CrossRef]
- University Hospital Advanced Age Pregnant Cohort. Available online: https://clinicaltrials.gov/ct2/show/NCT03220750 (accessed on 4 April 2021).
- International Association of Diabetes and Pregnancy Study Groups Consensus Panel; Metzger, B.E.; Gabbe, S.G.; Persson, B.; Buchanan, T.A.; Catalano, P.A.; Damm, P.; Dyer, A.R.; Leiva, A.D.; Hod, M.; et al. International association of diabetes and pregnancy study groups recommendations on the diagnosis and classification of hyperglycemia in pregnancy. Diabetes Care 2010, 33, 676–682. [Google Scholar] [CrossRef] [Green Version]
- WHO. Body Mass Index Classification. Available online: https://www.euro.who.int/en/health-topics/disease-prevention/nutrition/a-healthy-lifestyle/body-mass-index-bmi (accessed on 4 January 2022).
- Hu, J.; Aris, I.M.; Oken, E.; Ma, Y.; Ding, N.; Gao, M.; Wei, X.; Wen, D. Association of total and trimester-specific gestational weight gain rate with early infancy weight status: A prospective birth cohort study in China. Nutrients 2019, 11, 280. [Google Scholar] [CrossRef] [Green Version]
- Zhu, L.; Zhang, R.; Zhang, S.; Shi, W.; Yan, W.; Wang, X.; Lyu, Q.; Liu, L.; Zhou, Q.; Qiu, Q.; et al. Chinese neonatal birth weight curve for different gestational age. Zhonghua Er Ke Za Zhi 2015, 53, 97–103. [Google Scholar]
- Li, Y.; Gao, Q.; Li, L.; Shen, Y.; Lu, Q.; Huang, J.; Sun, C.; Wang, H.; Qiao, N.; Wang, C.; et al. Additive interaction of snoring and body mass index on the prevalence of metabolic syndrome among Chinese coal mine employees: A cross-sectional study. BMC Endocr. Disord. 2019, 19, 28. [Google Scholar] [CrossRef]
- Kalilani, L.; Atashili, J. Measuring additive interaction using odds ratios. Epidemiol Perspect. Innov. 2006, 3, 5. [Google Scholar] [CrossRef] [Green Version]
- Knol, M.J.; van der Tweel, I.; Grobbee, D.E.; Numans, M.E.; Geerlings, M.I. Estimating interaction on an additive scale between continuous determinants in a logistic regression model. Int. J. Epidemiol. 2007, 36, 1111–1118. [Google Scholar] [CrossRef] [PubMed]
- Neufeld, L.M.; Haas, J.D.; Grajéda, R.; Martorell, R. Changes in maternal weight from the first to second trimester of pregnancy are associated with fetal growth and infant length at birth. Am. J. Clin. Nutr. 2004, 79, 646–652. [Google Scholar] [CrossRef] [PubMed]
- Sekiya, N.; Anai, T.; Matsubara, M.; Miyazaki, F. Maternal weight gain rate in the second trimester are associated with birth weight and length of gestation. Gynecol. Obs. Invest. 2007, 63, 45–48. [Google Scholar] [CrossRef] [PubMed]
- Shi, P.; Liu, A.; Yin, X. Association between gestational weight gain in women with gestational diabetes mellitus and adverse pregnancy outcomes: A retrospective cohort study. BMC Pregnancy Childbirth 2021, 21, 508. [Google Scholar] [CrossRef] [PubMed]
- Komem, D.; Salman, L.; Krispin, E.; Arbib, N.; Bardin, R.; Wiznitzer, A.; Hadar, E. Gestational weight gain and weight loss among women with gestational diabetes mellitus. Diabetes Res Clin Pr. 2018, 141, 88–97. [Google Scholar] [CrossRef] [PubMed]
- HAPO Study Cooperative Research Group; Metzger, B.E.; Lowe, L.P.; Dyer, A.R.; Trimble, E.R.; Chaovarindr, U.; Coustan, D.R.; Hadden, D.R.; McCance, D.R.; Hod, M.; et al. Hyperglycemia and adverse pregnancy outcomes. N. Engl. J. Med. 2008, 358, 1991–2002. [Google Scholar] [CrossRef] [Green Version]
- Zhou, Z.; Deng, C.; Xiang, X. Blood glucose related to pregnancy induced hypertension syndrome. Am. J. Transl. Res. 2021, 13, 5301–5307. [Google Scholar]
- Caughey, A.B.; Cahill, A.G.; Guise, J.-M.; Rouse, D.J. Safe prevention of the primary cesarean delivery. Am. J. Obstet. Gynecol. 2014, 210, 179–193. [Google Scholar] [CrossRef]
- Begum, T.; Rahman, A.; Nababan, H.; Hoque, D.M.E.; Khan, A.F.; Ali, T.; Anwar, I. Indications and determinants of caesarean section delivery: Evidence from a population-based study in Matlab, Bangladesh. PLoS ONE 2017, 12, e0188074. [Google Scholar] [CrossRef] [Green Version]
- Rafat, D.; Singh, S.; Nawab, T.; Khan, F.; Khan, A.U.; Khalid, S. Association of vaginal dysbiosis and gestational diabetes mellitus with adverse perinatal outcomes. Int. J. Gynaecol. Obs. 2021, 1–9. [Google Scholar] [CrossRef]
- Lukic, A.; Napoli, A.; Santino, I.; Bianchi, P.; Nobili, F.; Ciampittiello, G.; Nardone, M.R.; Santomauro, M.; Di Properzio, M.; Caserta, D. Cervicovaginal bacteria and fungi in pregnant diabetic and non-diabetic women: A multicenter observational cohort study. Eur. Rev. Med. Pharm. Sci. 2017, 21, 2303–2315. [Google Scholar]
- Haahr, T.; Clausen, T.D.; Thorsen, J.; Rasmussen, M.A.; Mortensen, M.S.; Lehtimäki, J.; Shah, S.A.; Hjelmsø, M.H.; Bønnelykke, K.; Chawes, B.L.; et al. Vaginal dysbiosis in pregnancy associates with risk of emergency caesarean section: A prospective cohort study. Clin. Microbiol. Infect. 2022, 28, 588–595. [Google Scholar] [CrossRef] [PubMed]
- Gou, B.-H.; Guan, H.-M.; Bi, Y.-X.; Ding, B.-J. Gestational diabetes: Weight gain during pregnancy and its relationship to pregnancy outcomes. Chin. Med. J. 2019, 132, 154. [Google Scholar] [CrossRef] [PubMed]
- Xie, X.; Liu, J.; Pujol, I.; López, A.; Martínez, M.J.; García-Patterson, A.; Adelantado, J.M.; Ginovart, G.; Corcoy, R. Inadequate weight gain according to the institute of medicine 2009 guidelines in women with gestational diabetes: Frequency, clinical predictors, and the association with pregnancy outcomes. J. Clin. Med. 2020, 9, 3343. [Google Scholar] [CrossRef]
- Mastella, L.S.; Weinert, L.S.; Gnielka, V.; Hirakata, V.N.; Oppermann, M.L.R.; Silveiro, S.P.; Reichelt, A.J. Influence of maternal weight gain on birth weight: A gestational diabetes cohort. Arch. Endocrinol. Metab. 2018, 62, 55–63. [Google Scholar] [CrossRef]
- Bogdanet, D.; Mustafa, M.; Khattak, A.; O’Shea, P.M.; Dunne, F.P. Atlantic DIP: Is Weight gain less than that recommended by IOM safe in obese women with gestational diabetes mellitus? Int. J. Obes. 2021, 45, 1044–1051. [Google Scholar] [CrossRef]
- Li, Y.; Zhang, Q.; Xu, F.; Wang, Y. Restricted gestational weight gain in overweight/obese women with gestational diabetes mellitus and pregnancy outcomes. Clin. Exp. Obstet. Gynecol. 2019, 46, 763–769. [Google Scholar] [CrossRef]
- Lima Ferreira, J.; Voss, G.; Dória, M.; Sá Couto, A.; Príncipe, R.M. Benefit of insufficient gestational weight gain in obese women with gestational diabetes mellitus: A multicenter study in portugal. Diabetes Metab. Syndr. 2021, 15, 419–424. [Google Scholar] [CrossRef]
- Park, J.E.; Park, S.; Daily, J.W.; Kim, S.-H. Low gestational weight gain improves infant and maternal pregnancy outcomes in overweight and obese Korean women with gestational diabetes mellitus. Gynecol. Endocrinol. 2011, 27, 775–781. [Google Scholar] [CrossRef]
- Kee, C.C.; Lim, K.H.; Sumarni, M.G.; Teh, C.H.; Chan, Y.Y.; Nuur Hafizah, M.I.; Cheah, Y.K.; Tee, E.O.; Ahmad Faudzi, Y.; Amal Nasir, M. Validity of self-reported weight and height: A cross-sectional study among Malaysian adolescents. BMC Med. Res. Methodol. 2017, 17, 85. [Google Scholar] [CrossRef] [Green Version]
- Luo, J.; Thomson, C.A.; Hendryx, M.; Tinker, L.F.; Manson, J.E.; Li, Y.; Nelson, D.A.; Vitolins, M.Z.; Seguin, R.A.; Eaton, C.B.; et al. Accuracy of self-reported weight in the women’s health initiative. Public Health Nutr. 2019, 22, 1019–1028. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Without GDM (n = 9115) | With GDM (n = 3013) | p Value a | |
|---|---|---|---|
| Maternal age, year | 36.0 (35.0–38.0) | 37.0 (36.0–39.0) | <0.001 |
| <35 | 1966 (21.6) | 312 (10.4) | <0.001 |
| ≥35 and <40 | 5829 (63.9) | 2047 (67.9) | |
| ≥40 | 1320 (14.5) | 654 (21.7) | |
| Han ethnicity | 8780 (96.3) | 2911 (96.6) | 0.459 |
| Multipara | 5296 (58.1) | 1754 (58.2) | 0.913 |
| Conception by ART | 1254 (13.8) | 590 (19.6) | <0.001 |
| Smoking b | 142 (1.6) | 42 (1.4) | 0.523 |
| Pre-pregnancy BMI, kg/m2 | 21.8 ± 2.8 | 22.8 ± 3.0 | <0.001 |
| Total GWG, kg | 13.5 ± 5.0 | 11.4 ± 5.1 | <0.001 |
| GWGR, kg/week | |||
| Total | 0.35 ± 0.13 | 0.30 ± 0.13 | <0.001 |
| First trimester c | 0.14 ± 0.17 | 0.15 ± 0.16 | 0.004 |
| Second trimester c | 0.43 ± 0.19 | 0.38 ± 0.19 | <0.001 |
| Third trimester c | 0.48 ± 0.32 | 0.35 ± 0.32 | <0.001 |
| Birth weight, g | 3262.0 ± 482.0 | 3231.0 ± 511.0 | 0.002 |
| Gestational age, week | 39.0 (38.3–39.9) | 38.6 (38.0–39.6) | <0.001 |
| Outcome | AOR (95% CI) | INTM (95% CI) | RERI (95% CI) | ||
|---|---|---|---|---|---|
| All Women (n = 12,128) | Without GDM (n = 9115) | With GDM (n = 3013) | |||
| SGA a | 0.75 (0.70–0.81) | 0.78 (0.71–0.85) | 0.70 (0.61–0.82) | 0.90 (0.77–1.05) | −0.09 (−0.21–0.02) |
| LGA b | 1.50 (1.40–1.60) | 1.41 (1.30–1.53) | 1.76 (1.54–2.00) | 1.24 (1.08–1.43) | 0.39 (0.13–0.65) |
| Preterm birth c | 1.07 (0.98–1.14) | 1.07 (0.99–1.16) | 1.08 (0.97–1.21) | 1.01 (0.89–1.14) | 0.03 (−0.14–0.20) |
| GWGR ≤ 0.44kg/week d | 0.87 (0.76–0.99) | 0.84 (0.71–0.99) | 0.90 (0.72–1.12) | 1.01 (0.78–1.31) | −0.01 (−0.23–0.20) |
| GWGR > 0.44kg/week e | 1.40 (1.24–1.57) | 1.42 (1.24–1.63) | 1.38 (1.09–1.75) | 0.95 (0.73–1.24) | 0.03 (−0.16–0.23) |
| Cesarean delivery f | 1.23 (1.18–1.28) | 1.21 (1.15–1.27) | 1.29 (1.17–1.41) | 1.10 (1.001–1.22) | 0.15 (0.01–0.29) |
| GHDs g | 1.32 (1.22–1.42) | 1.32 (1.20–1.45) | 1.29 (1.14–1.47) | 1.01 (0.88–1.18) | 0.15 (−0.11–0.42) |
| Outcome | Trimester | AOR (95% CI) | INTM (95% CI) | RERI (95% CI) | ||
|---|---|---|---|---|---|---|
| All Women (n = 9838) | Without GDM (n = 7227) | With GDM (n = 2611) | ||||
| LGA | First | 1.15 (1.07–1.24) | 1.15 (1.05–1.25) | 1.17 (1.01–1.35) | 1.05 (0.90–1.24) | 0.05 (−0.13–0.23) |
| Second | 1.50 (1.39–1.62) | 1.53 (1.40–1.67) | 1.43 (1.24–1.64) | 0.97 (0.83–1.13) | −0.05 (−0.28–0.19) | |
| Third | 1.20 (1.12–1.29) | 1.09 (1.002–1.19) | 1.52 (1.33–1.75) | 1.39 (1.19–1.62) | 0.46 (0.22–0.71) | |
| Cesarean delivery | First | 1.07 (1.02–1.13) | 1.08 (1.02–1.14) | 1.06 (1.001–1.14) | 0.98 (0.88–1.08) | −0.02 (−0.14–0.09) |
| Second | 1.22 (1.15–1.30) | 1.21 (1.13–1.30) | 1.24 (1.11–1.39) | 1.03 (0.91–1.18) | 0.04 (−0.13–0.20) | |
| Third | 1.18 (1.12–1.25) | 1.15 (1.08–1.22) | 1.28 (1.14–1.44) | 1.15 (1.01–1.31) | 0.19 (0.02–0.36) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cheng, Z.-H.; Wei, Y.-M.; Li, H.-T.; Yu, H.-Z.; Liu, J.-M.; Zhou, Y.-B. Gestational Diabetes Mellitus as an Effect Modifier of the Association of Gestational Weight Gain with Perinatal Outcomes: A Prospective Cohort Study in China. Int. J. Environ. Res. Public Health 2022, 19, 5615. https://doi.org/10.3390/ijerph19095615
Cheng Z-H, Wei Y-M, Li H-T, Yu H-Z, Liu J-M, Zhou Y-B. Gestational Diabetes Mellitus as an Effect Modifier of the Association of Gestational Weight Gain with Perinatal Outcomes: A Prospective Cohort Study in China. International Journal of Environmental Research and Public Health. 2022; 19(9):5615. https://doi.org/10.3390/ijerph19095615
Chicago/Turabian StyleCheng, Zhi-Hao, Yu-Mei Wei, Hong-Tian Li, Hong-Zhao Yu, Jian-Meng Liu, and Yu-Bo Zhou. 2022. "Gestational Diabetes Mellitus as an Effect Modifier of the Association of Gestational Weight Gain with Perinatal Outcomes: A Prospective Cohort Study in China" International Journal of Environmental Research and Public Health 19, no. 9: 5615. https://doi.org/10.3390/ijerph19095615
APA StyleCheng, Z. -H., Wei, Y. -M., Li, H. -T., Yu, H. -Z., Liu, J. -M., & Zhou, Y. -B. (2022). Gestational Diabetes Mellitus as an Effect Modifier of the Association of Gestational Weight Gain with Perinatal Outcomes: A Prospective Cohort Study in China. International Journal of Environmental Research and Public Health, 19(9), 5615. https://doi.org/10.3390/ijerph19095615