
Effects of Walking as Physical Exercise on Functional Limitation through Pain in Patients with Fibromyalgia—How Does Catastrophic Thinking Contribute?

Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Instruments
2.3. Data Analysis
3. Results
3.1. Sample Characteristics
3.2. Descriptive Analysis and Correlations
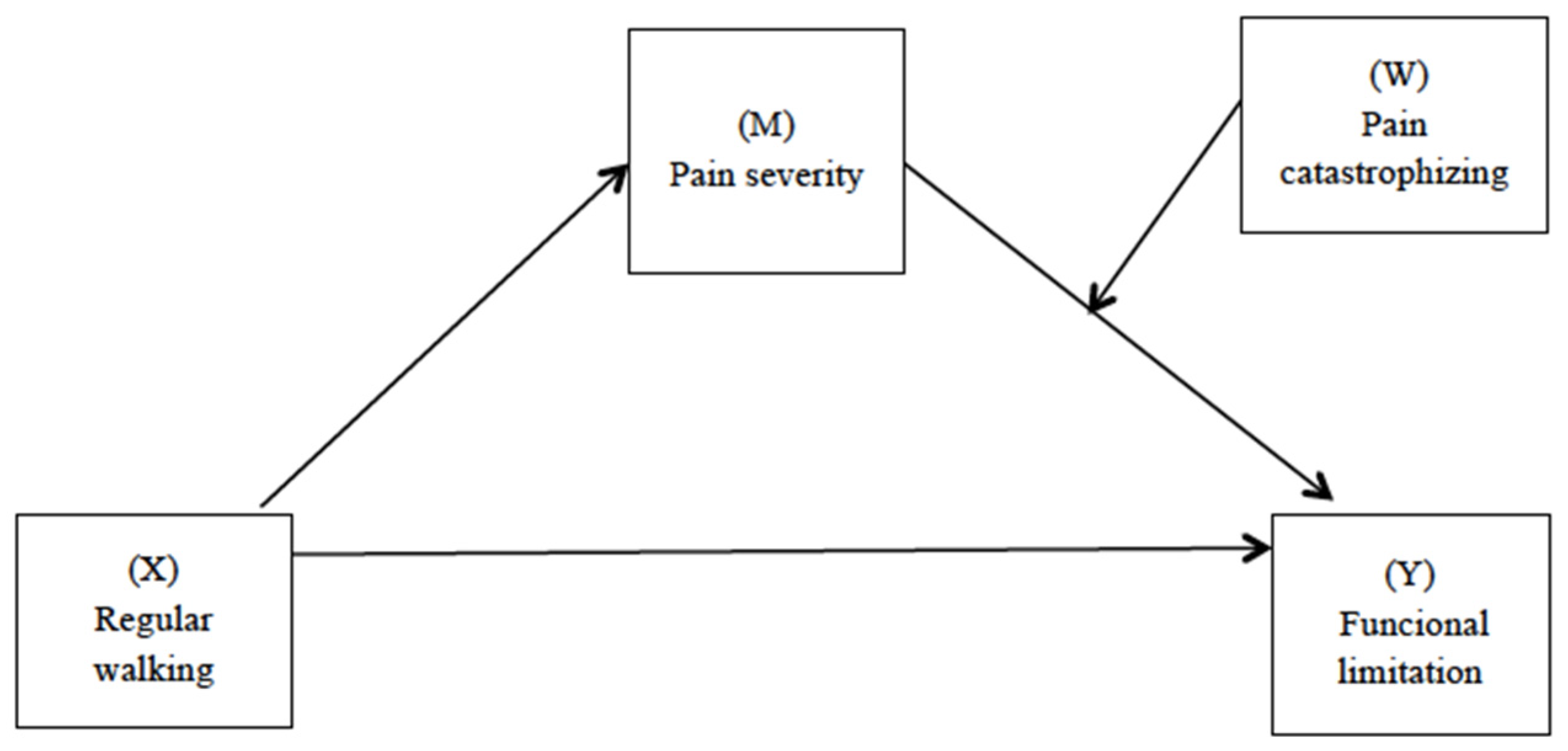
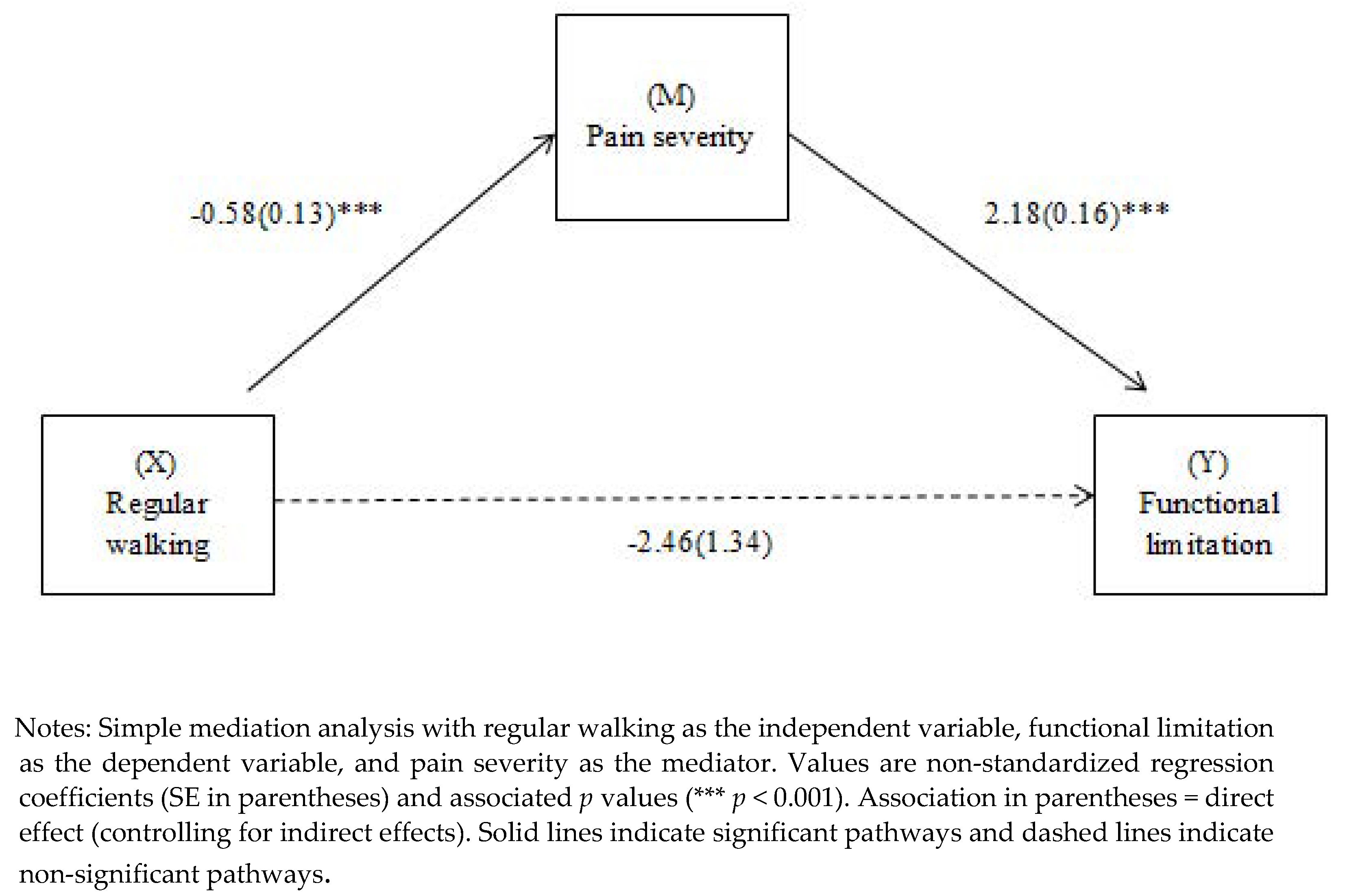
3.3. Mediation Model of the Relationship between Regular Walking and Functional Limitation with Pain Intensity as a Mediator
3.4. Moderate Mediation Model
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- O’Connor, S.R.; Tully, M.A.; Ryan, B.; Bleakley, C.M.; Baxter, G.D.; Bradley, J.M.; McDonough, S.M. Walking Exercise for Chronic Musculoskeletal Pain: Systematic Review and Meta-Analysis. Arch. Phys. Med. Rehabil. 2015, 96, 724–734.e3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kayo, A.H.; Peccin, M.S.; Sanches, C.M.; Trevisani, V.F.M. Effectiveness of physical activity in reducing pain in patients with fibromyalgia: A blinded randomized clinical trial. Rheumatol. Int. 2012, 32, 2285–2292. [Google Scholar] [CrossRef] [PubMed]
- Rooks, D.S. Group Exercise, Education, and Combination Self-management in Women With Fibromyalgia: A Randomized Trial. Arch. Intern. Med. 2007, 167, 2192. [Google Scholar] [CrossRef] [PubMed]
- Gusi, N.; Parraca, J.; Adsuar, J.; Olivares, P. Physical exercise and Fibromyalgia. In Physical Exercise Guidelines for People with Fibromyalgia; Penacho, A., Rivera, J., Pastor, M.A., Gusi, N., Eds.; Asociación de Divulgación de Fibromialgia: Vitoria, Spain, 2009; pp. 39–56. Available online: https://www.fibro.info/guiaejercicios.pdf (accessed on 15 November 2022).
- Terrier, P.; Praz, C.; Le Carré, J.; Vuistiner, P.; Léger, B.; Luthi, F. Influencing walking behavior can increase the physical activity of patients with chronic pain hospitalized for multidisciplinary rehabilitation: An observational study. BMC Musculoskelet. Disord. 2019, 20, 188. [Google Scholar] [CrossRef] [Green Version]
- Santos, E.; Campos, M.A.; Párraga-Montilla, J.A.; Aragón-Vela, J.; Latorre-Román, P.A. Effects of a functional training program in patients with fibromyalgia: A 9-year prospective longitudinal cohort study. Scand. J. Med. Sci. Sport. 2020, 30, 904–913. [Google Scholar] [CrossRef]
- Andrade, A.; Dominski, F.H.; Sieczkowska, S.M. What we already know about the effects of exercise in patients with fibromyalgia: An umbrella review. Semin. Arthritis Rheum. 2020, 50, 1465–1480. [Google Scholar] [CrossRef]
- Peñacoba, C.; Pastor, M.-Á.; López-Roig, S.; Velasco, L.; Lledo, A. Walking Beliefs in Women with Fibromyalgia: Clinical Profile and Impact on Walking Behavior. Clin. Nurs. Res. 2017, 26, 632–650. [Google Scholar] [CrossRef]
- Sanz-Baños, Y.; Pastor, M.-Á.; Velasco, L.; López-Roig, S.; Peñacoba, C.; Lledo, A.; Rodríguez, C. To walk or not to walk: Insights from a qualitative description study with women suffering from fibromyalgia. Rheumatol. Int. 2016, 36, 1135–1143. [Google Scholar] [CrossRef]
- Sanz-Baños, Y.; Pastor-Mira, M.-Á.; Lledó, A.; López-Roig, S.; Peñacoba, C.; Sánchez-Meca, J. Do women with fibromyalgia adhere to walking for exercise programs to improve their health? Systematic review and meta-analysis. Disabil. Rehabil. 2018, 40, 2475–2487. [Google Scholar] [CrossRef]
- López-Roig, S.; Pastor, M.A.; Peñacoba, C.; Lledó, A.; Sanz, Y.; Velasco, F. Prevalence and predictors of unsupervised walking and physical activity in a community population of women with fibromyalgia. Rheumatol. Int. 2016, 36, 1127–1133. [Google Scholar] [CrossRef]
- Lami, M.J.; Martínez, M.P.; Miró, E.; Sánchez, A.I.; Guzmán, M.A. Catastrophizing, Acceptance, and Coping as Mediators between Pain and Emotional Distress and Disability in Fibromyalgia. J. Clin. Psychol. Med. Settings 2018, 25, 80–92. [Google Scholar] [CrossRef] [PubMed]
- Catala, P.; Lopez-Roig, S.; Ecija, C.; Suso-Ribera, C.; Peñacoba Puente, C. Why do some people with severe chronic pain adhere to walking prescriptions whilst others won’t? A cross-sectional study exploring clinical and psychosocial predictors in women with fibromyalgia. Rheumatol. Int. 2021, 41, 1479–1484. [Google Scholar] [CrossRef] [PubMed]
- Yim, Y.-R.; Lee, K.-E.; Park, D.-J.; Kim, S.-H.; Nah, S.-S.; Lee, J.H.; Kim, S.-K.; Lee, Y.-A.; Hong, S.-J.; Kim, H.-S.; et al. Identifying fibromyalgia subgroups using cluster analysis: Relationships with clinical variables. Eur. J. Pain 2017, 21, 374–384. [Google Scholar] [CrossRef] [PubMed]
- Jobski, K.; Luque Ramos, A.; Albrecht, K.; Hoffmann, F. Pain, depressive symptoms and medication in German patients with rheumatoid arthritis-results from the linking patient-reported outcomes with claims data for health services research in rheumatology (PROCLAIR) study. Pharmacoepidemiol. Drug Saf. 2017, 26, 766–774. [Google Scholar] [CrossRef]
- Suso-Ribera, C.; Catalá, P.; Ecija, C.; Sanromán, L.; López-Gómez, I.; Pastor-Mira, Á.; Peñacoba-Puente, C. Exploring the contextual role of pain severity as a moderator of the relationship between activity patterns and the physical and mental functioning of women with fibromyalgia. Eur. J. Pain 2020, 25, 257–268. [Google Scholar] [CrossRef]
- Gellman, M.D.; Turner, J.R. Encyclopedia of Behavioral Medicine; Springer Science+Business Media: New York, NY, USA, 2013; ISBN 9781441910059. [Google Scholar]
- Galvez-Sánchez, C.M.; Reyes del Paso, G.A.; Duschek, S. Cognitive Impairments in Fibromyalgia Syndrome: Associations with Positive and Negative Affect, Alexithymia, Pain Catastrophizing and Self-Esteem. Front. Psychol. 2018, 9, 377. [Google Scholar] [CrossRef] [Green Version]
- Mork, P.J.; Vasseljen, O.; Nilsen, T.I.L. Association between physical exercise, body mass index, and risk of fibromyalgia: Longitudinal data from the Norwegian Nord-Trøndelag Health Study. Arthritis Care Res. 2010, 62, 611–617. [Google Scholar] [CrossRef]
- Ellingsen, D.-M.; Beissner, F.; Moher Alsady, T.; Lazaridou, A.; Paschali, M.; Berry, M.; Isaro, L.; Grahl, A.; Lee, J.; Wasan, A.D.; et al. A picture is worth a thousand words: Linking fibromyalgia pain widespreadness from digital pain drawings with pain catastrophizing and brain cross-network connectivity. Pain 2021, 162, 1352–1363. [Google Scholar] [CrossRef]
- Quartana, P.J.; Campbell, C.M.; Edwards, R.R. Pain catastrophizing: A critical review. Expert Rev. Neurother. 2009, 9, 745–758. [Google Scholar] [CrossRef]
- Van Damme, S.; Kindermans, H. A Self-Regulation Perspective on Avoidance and Persistence Behavior in Chronic Pain. Clin. J. Pain 2015, 31, 115–122. [Google Scholar] [CrossRef]
- Leeuw, M.; Goossens, M.E.; Linton, S.J.; Crombez, G.; Boersma, K.; Vlaeyen, J.W. The Fear-Avoidance Model of Musculoskeletal Pain: Current State of Scientific Evidence. J. Behav. Med 2006, 30, 77–94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arnow, B.A.; Blasey, C.M.; Constantino, M.J.; Robinson, R.; Hunkeler, E.; Lee, J.; Fireman, B.; Khaylis, A.; Feiner, L.; Hayward, C. Catastrophizing, depression and pain-related disability. Gen. Hosp. Psychiatry 2011, 33, 150–156. [Google Scholar] [CrossRef] [PubMed]
- Écija, C.; Luque-Reca, O.; Suso-Ribera, C.; Catala, P.; Peñacoba, C. Associations of Cognitive Fusion and Pain Catastrophizing with Fibromyalgia Impact through Fatigue, Pain Severity, and Depression: An Exploratory Study Using Structural Equation Modeling. J. Clin. Med. 2020, 9, 1763. [Google Scholar] [CrossRef] [PubMed]
- Peñacoba, C.; Pastor-Mira, M.Á.; Suso-Ribera, C.; Catalá, P.; Nardi-Rodríguez, A.; López-Roig, S. Activity Patterns and Functioning. A Contextual–Functional Approach to Pain Catastrophizing in Women with Fibromyalgia. Int. J. Environ. Res. Public Health 2021, 18, 5394. [Google Scholar] [CrossRef]
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.A.; Goldenberg, D.L.; Katz, R.S.; Mease, P.; Russell, A.S.; Russell, I.J.; Winfield, J.B.; Yunus, M.B. The American College of Rheumatology preliminary diagnostic criteria for fibromyalgia and measurement of symptom severity. Arthritis Care Res. 2010, 62, 600–610. [Google Scholar] [CrossRef] [Green Version]
- Busch, A.J.; Schachter, C.L.; Overend, T.J.; Peloso, P.M.; Barber, K.A. Exercise for fibromyalgia: A systematic review. J. Rheumatol. 2008, 35, 1130–1144. [Google Scholar]
- Cleeland, C.S.; Ryan, K.M. Pain assessment: Global use of the Brief Pain Inventory. Ann. Acad. Med. Singap. 1994, 23, 129–138. [Google Scholar]
- Jensen, M.P.; Turner, L.R.; Turner, J.A.; Romano, J.M. The use of multiple-item scales for pain intensity measurement in chronic pain patients. Pain 1996, 67, 35–40. [Google Scholar] [CrossRef]
- García Campayo, J.; Rodero, B.; Alda, M.; Sobradiel, N.; Montero, J.; Moreno, S. Validation of the Spanish version of the Pain Catastrophizing Scale in fibromyalgia. Med. Clin. 2008, 131, 487–492. [Google Scholar] [CrossRef]
- Salgueiro, M.; García-Leiva, J.M.; Ballesteros, J.; Hidalgo, J.; Molina, R.; Calandre, E.P. Validation of a Spanish version of the Revised Fibromyalgia Impact Questionnaire (FIQR). Health Qual. Life Outcomes 2013, 11, 132. [Google Scholar] [CrossRef] [Green Version]
- Herrero, M.J.; Blanch, J.; Peri, J.M.; De Pablo, J.; Pintor, L.; Bulbena, A. A validation study of the hospital anxiety and depression scale (HADS) in a Spanish population. Gen. Hosp. Psychiatry 2003, 25, 277–283. [Google Scholar] [CrossRef] [PubMed]
- IBM Corp. IBM SPSS Statistics for Windows, version 22.0; IBM Corp: New York, NY, USA, 2017. [Google Scholar]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis Second Edition A Regression-Based Approach; The Guilford Press: New York, NY, USA, 2017; ISBN 9781462534654. [Google Scholar]
- Latorre-Román, P.; Santos-Campos, M.; Heredia-Jimenez, J.; Delgado-Fernandez, M.; Soto-Hermoso, V. Analysis of the performance of women with fibromyalgia in the six-minute walk test and its relation with health and quality of life. J. Sport. Med. Phys. Fit. 2014, 54, 511–517. [Google Scholar]
- Mannerkorpi, K.; Nordeman, L.; Cider, Å.; Jonsson, G. Does moderate-to-high intensity Nordic walking improve functional capacity and pain in fibromyalgia? A prospective randomized controlled trial. Arthritis Res. Ther. 2010, 12, R189. [Google Scholar] [CrossRef] [PubMed]
- Ellingson, L.D.; Stegner, A.J.; Schwabacher, I.J.; Lindheimer, J.B.; Cook, D.B. Catastrophizing Interferes with Cognitive Modulation of Pain in Women with Fibromyalgia. Pain Med. 2018, 19, 2408–2422. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Varallo, G.; Scarpina, F.; Giusti, E.M.; Suso-Ribera, C.; Cattivelli, R.; Guerrini Usubini, A.; Capodaglio, P.; Castelnuovo, G. The Role of Pain Catastrophizing and Pain Acceptance in Performance-Based and Self-Reported Physical Functioning in Individuals with Fibromyalgia and Obesity. J. Pers. Med. 2021, 11, 810. [Google Scholar] [CrossRef]
- Galvez-Sánchez, C.M.; Montoro, C.I.; Duschek, S.; del Paso, G.A.R. Pain catastrophizing mediates the negative influence of pain and trait-anxiety on health-related quality of life in fibromyalgia. Qual. Life Res. 2020, 29, 1871–1881. [Google Scholar] [CrossRef]
- Montoro, C.I.; Galvez-Sánchez, C.M. The Mediating Role of Depression and Pain Catastrophizing in the Relationship between Functional Capacity and Pain Intensity in Patients with Fibromyalgia. Behav. Neurol. 2022, 2022, 9770047. [Google Scholar] [CrossRef]
- O’Dwyer, T.; Maguire, S.; Mockler, D.; Durcan, L.; Wilson, F. Behaviour change interventions targeting physical activity in adults with fibromyalgia: A systematic review. Rheumatol. Int. 2019, 39, 805–817. [Google Scholar] [CrossRef]
- Robinson, M.E.; Staud, R.; Price, D.D. Pain Measurement and Brain Activity: Will Neuroimages Replace Pain Ratings? J. Pain 2013, 14, 323–327. [Google Scholar] [CrossRef] [Green Version]
- Wideman, T.H.; Edwards, R.R.; Walton, D.M.; Martel, M.O.; Hudon, A.; Seminowicz, D.A. The Multimodal Assessment Model of Pain. Clin. J. Pain 2019, 35, 212–221. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Psychosocial Characteristics | Mean (SD) | Sample Range | 2. | 3. | 4. | 5. | 6. | 7. |
|---|---|---|---|---|---|---|---|---|
| 1. Pain severity | 7.05 (1.49) | 1–10 | 0.367 ** | 0.541 ** | 0.219 ** | 0.172 ** | 0.058 | −0.187 ** |
| 2. Pain catastrophizing | 30.20 (12.17) | 0–52 | 0.401 * | 0.497 ** | 0.188 ** | −0.052 | −0.191 ** | |
| 3. Functional limitation | 22.00 (6.27) | 0–30 | 0.255 ** | 0.212 ** | 0.096 * | −0.222 ** | ||
| 4. Axiety | 12.17 (3.69) | 4–21 | 0.113 * | −0.107 * | −0.159 ** | |||
| 5. Depression | 11.48 (4.15) | 1–21 | 0.107 | −0.073 | ||||
| 6. Age | 53.89 (9.25) | 19–78 | −0.062 | |||||
| 7. Regular walking, n (%) | ||||||||
| Yes | 312 (63.5) | . | . | |||||
| No | 179 (36.5) |
| R2 | F | p | Beta | t | p | |
|---|---|---|---|---|---|---|
| Model 1 | 0.59 | 66.91 | <0.001 | |||
| Regular walking | −2.46 | −1.83 | 0.067 | |||
| Pain severity | 2.54 | 7.10 | <0.001 | |||
| Pain catastrophizing | 0.28 | 3.36 | <0.001 | |||
| Pain catastrophizing × Pain severity | −0.02 | −2.10 | 0.033 | |||
| Anxiety (covariate) | 0.079 | 1.10 | 0.271 | |||
| Depression (covariate) | 0.130 | 2.29 | 0.021 | |||
| Age (covariate) | 0.032 | 1.29 | 0.195 |
| Pain Catastrophizing | Beta | SE | LL 95% CI | UL 95% CI |
|---|---|---|---|---|
| 1SD below the mean | −1.22 | 0.31 | −1.86 | −0.64 |
| Mean | −1.05 | 0.27 | −1.61 | −0.54 |
| 1SD above the mean | −0.87 | 0.25 | −1.41 | −0.42 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Catalá, P.; Peñacoba, C.; López-Roig, S.; Pastor-Mira, M.A. Effects of Walking as Physical Exercise on Functional Limitation through Pain in Patients with Fibromyalgia—How Does Catastrophic Thinking Contribute? Int. J. Environ. Res. Public Health 2023, 20, 190. https://doi.org/10.3390/ijerph20010190
Catalá P, Peñacoba C, López-Roig S, Pastor-Mira MA. Effects of Walking as Physical Exercise on Functional Limitation through Pain in Patients with Fibromyalgia—How Does Catastrophic Thinking Contribute? International Journal of Environmental Research and Public Health. 2023; 20(1):190. https://doi.org/10.3390/ijerph20010190
Chicago/Turabian StyleCatalá, Patricia, Cecilia Peñacoba, Sofía López-Roig, and María Angeles Pastor-Mira. 2023. "Effects of Walking as Physical Exercise on Functional Limitation through Pain in Patients with Fibromyalgia—How Does Catastrophic Thinking Contribute?" International Journal of Environmental Research and Public Health 20, no. 1: 190. https://doi.org/10.3390/ijerph20010190
APA StyleCatalá, P., Peñacoba, C., López-Roig, S., & Pastor-Mira, M. A. (2023). Effects of Walking as Physical Exercise on Functional Limitation through Pain in Patients with Fibromyalgia—How Does Catastrophic Thinking Contribute? International Journal of Environmental Research and Public Health, 20(1), 190. https://doi.org/10.3390/ijerph20010190